Logan’s Community Maternal and Child Health Hubs: The ...
16
Design. Evaluate. Evolve. 1 Logan’s Community Maternal and Child Health Hubs: The contribution case for collective impact practice Since launching in 2018, the Community Maternal and Child Health Hubs (Maternity Hubs) have led to positive health and social outcomes for women and babies using the in-community Hubs. Outcomes include increased antenatal visits and care, and less birth interventions and complications. There is compelling evidence that without the collective impact practice of a mix of collaborating partners that a) the community co-designed Hubs, and b) the subsequent health outcomes for cohorts using the hubs, would not have happened. The Maternity Hubs aim to increase access and uptake of care during pregnancy and birth for Logan women and families experiencing vulnerability. They cater for Aboriginal and Torres Strait Islander women, Māori and Pacific Island women, young women under 18 years old, refugee and culturally diverse women, and women with significant social risk. Four community-located Maternity Hubs and a complex care services have been established in Logan since 2018. The Maternity Hubs provide culturally safe continuity of midwifery care for women and holistic, wrap around social service support. Women are offered their own midwife from the early stages of pregnancy to ensure continuity of care; a place to visit midwives in community, as opposed to larger central hospitals; and wrap around support via referrals to other services in community including emergency bill paying, housing, refugee settlement, and domestic and family violence support. Key Points • The Maternity Hubs have achieved a range of statistically significant perinatal outcomes compared to standard care in Logan (e.g. increased antenatal visits and vaccination rates, and less birth interventions such as caesarean section). • The effectiveness of the Hubs is credited to the continuity of midwifery care model and in-community location of care. These were a direct result of the inclusive community engagement and co-design with women– driven by the collective impact practice. • The contribution analysis showed that the Hubs, and subsequent outcomes, would not have happened without the collective impact practice. Collective impact practice underpinned the way partners worked together and navigated barriers and challenges. It was an enabling force and included strategic and “persistent” collective advocacy that led to funding and sustained momentum. • Many partners collaborated and contributed. Logan Together played a critical role in facilitating change and driving the collective impact agenda. The Backbone Team and Leadership Table contributed systems leadership and advocacy. “The Hubs are definitely the significant piece that really has changed lives…They certainly have changed the maternity landscape within Logan.” (Melanie McKenzie Director and Founder of Harrison’s Little Wings) “I think its directly related to the Hubs and the way they’ve been set up…. It’s the continuity of midwifery care and there is endless research around how that improves outcomes for vulnerable women and their babies” (Dr Belinda Maier, Queensland Nurses & Midwives’ Union) (Decision-makers could not ignore the collective advocacy)…Seeing us a collective, with such strength of community and consumer voice and evidence… and standing and leadership around midwifery… made it hard to not do.” (Professor Emeritus Jenny Gamble, Griffith University)
Transcript of Logan’s Community Maternal and Child Health Hubs: The ...

Design. Evaluate. Evolve. 1
Logan’s Community Maternal and Child Health Hubs:
The contribution case for collective impact practice
Since launching in 2018, the Community Maternal and Child Health Hubs (Maternity Hubs) have
led to positive health and social outcomes for women and babies using the in-community Hubs.
Outcomes include increased antenatal visits and care, and less birth interventions and
complications.
There is compelling evidence that without the collective impact practice of a mix of collaborating
partners that a) the community co-designed Hubs, and b) the subsequent health outcomes for
cohorts using the hubs, would not have happened.
The Maternity Hubs aim to increase access and uptake of care during pregnancy and birth for Logan
women and families experiencing vulnerability. They cater for Aboriginal and Torres Strait Islander
women, Māori and Pacific Island women, young women under 18 years old, refugee and culturally
diverse women, and women with significant social risk. Four community-located Maternity Hubs and a
complex care services have been established in Logan since 2018.
The Maternity Hubs provide culturally safe continuity of midwifery care for women and holistic, wrap
around social service support. Women are offered their own midwife from the early stages of pregnancy
to ensure continuity of care; a place to visit midwives in community, as opposed to larger central
hospitals; and wrap around support via referrals to other services in community including emergency bill
paying, housing, refugee settlement, and domestic and family violence support.
Key Points
• The Maternity Hubs have achieved a range of statistically significant perinatal outcomes compared to standard care in Logan (e.g. increased antenatal visits and vaccination rates, and less birth interventions such as caesarean section).
• The effectiveness of the Hubs is credited to the continuity of midwifery care model and in-community location of care. These were a direct result of the inclusive community engagement and co-design with women– driven by the collective impact practice.
• The contribution analysis showed that the Hubs, and subsequent outcomes, would not have happened without the collective impact practice. Collective impact practice underpinned the way partners worked together and navigated barriers and challenges. It was an enabling force and included strategic and “persistent” collective advocacy that led to funding and sustained momentum.
• Many partners collaborated and contributed. Logan Together played a critical role in facilitating change and driving the collective impact agenda. The Backbone Team and Leadership Table contributed systems leadership and advocacy.
“The Hubs are definitely the significant piece that really has changed lives…They certainly have changed the maternity landscape within Logan.” (Melanie McKenzie Director and Founder of Harrison’s Little Wings)
“I think its directly related to the Hubs and the way they’ve been set up…. It’s the continuity of midwifery care and there is endless research around how that improves outcomes for vulnerable women and their babies” (Dr Belinda Maier, Queensland Nurses & Midwives’ Union)
(Decision-makers could not ignore the collective advocacy)…Seeing us a collective, with such strength of community and consumer voice and evidence… and standing and leadership around midwifery… made it hard to not do.” (Professor Emeritus Jenny Gamble, Griffith University)

Design. Evaluate. Evolve. 2
About this report
This report summarises the findings of a rigorous Contribution Analysis commissioned by DSS and produced
by Clear Horizon. The methodology was designed to determine the extent that collective impact practice
contributed to the outcomes achieved via the Maternity Hubs and was informed by Mayne’s Contribution
Analysis.1 Clear Horizon conducted a desktop review of 30+ documents (including Queensland Health
evaluations and testimonies from women using the Hubs), and interviews and verification with 7 key
informants from the Oversight Committee, the Maternity Hubs and Hub host organisations.
Logan context prior to the Hubs
The City of Logan is a large and culturally diverse Local
Government Area (LGA).
Whilst a resourceful and resilient community, Logan LGA
faces several complex social and economic challenges
and there are many people in the community
experiencing vulnerability and disadvantage compared
to state averages. This is despite several decades of
significant federal and state government investment to
address social issues and entrenched disadvantage.
In the years prior to the Maternity Hubs there was
growing recognition that outcomes for mothers and
babies in Logan were poor compared to state averages and of the strong link between access to
antenatal care and the health outcomes for mothers and their babies. There are many reasons why
some women may not access these services, including lack of transport, eroded trust in the health
service, and cultural and social issues. The Metro South figures below show some areas where Logan
LGA was below state averages prior to the Maternity Hubs (2017).2
The story of setting up the Hubs
The Maternity Hubs concept had been an evolving conversation over many years and community and
service sector momentum for change was growing. Prior activities included long-term advocacy for
women by community and non-government organisations and the Midwifery Group Practice (MGP)
program in Logan Maternity Services from 2009-2012.3 MGP is where a small group of midwives care for a
woman during her pregnancy, labour and birth, and postpartum to ensure continuity of care.
1 Mayne, J. (2008). Contribution Analysis: An approach to exploring cause and effect, ILAC. 2 Data for antenatal appointments and birth weight are pre-2017, exact date range unspecified in original source. 3 This was a hospital-based program providing continuity of care to some women in Logan. It differed to the Maternity
Hubs model and did not have the key community-informed aspects identified by women during the deep engagement
process for the Maternity Hubs (such as in-community and culturally safe spaces and access to wrap around support).

Design. Evaluate. Evolve. 3
Logan Together, a large-scale collective impact initiative in the Logan region, formed in 2015. As part of
the start-up phase of Logan Together, community-wide consultations were undertaken with a focus on
improving outcomes for children aged 0-8 years. Logan Together marked a new era of cross-sector
commitment and structured collective impact practice for community-driven solutions for improving
outcomes for children 0-8 years (see box below for definition of collective impact).
Results from analysing available health data at the time, showed that each year between 500 and 600
women in Logan were accessing little or no care during their pregnancy, and many of those who were
seeking and receiving support were not receiving continuity of midwifery care. Women were mostly
accessing antenatal midwifery visits at the hospital, with some private midwifery, obstetrics and General
Practitioner shared care. At that time, the consultations revealed that services were regarded by some
women and staff as institution-centric, highly medicalised, authoritarian, limited in choices for women for
birthing and postnatal care, and not creating an environment that enabled the delivery of evidence-based
care. There were concerns that there was a lack of connection and care with the health service, lack of
trust, language and cultural barriers, and institutional racism. All of which are influential factors on
women’s choice to access care, or not access care.
Collective impact
Collective Impact is a community led movement for change, informed by broad and inclusive community and cross sector stakeholder engagement, which provides a framework and resources to focus on complex issues, people and place. For the Stronger Places, Stronger People initiative, the collective impact conditions reviewed for the contribution analysis are: 4
• A systems approach (not programmatic) drives systemic changes needed for long term outcomes.
• Inclusive community engagement where community is at the centre of the change process
• High leverage activities that can make the biggest difference are prioritised.
• Backbone, local leadership and governance that enable collective impact practice and collaboration.
• Shared aspiration and strategy bring mixed stakeholders to work together around a common goal.
• Strategic learning, data, and evidence (including community voice) is used for understanding, learning, decision-making, measurement, and evaluation.
As a result of frustrations with local health services and the locally identified issues around support for
women during pregnancy, Logan Together facilitated the formation (and ongoing running) of a project
group to lead further community consultations and co-design processes with Logan women to develop a
community-based service model. The project group had a mixed representatives including community
members, consumer advocates, service providers, academics, and government/ health and hospital
representatives.
The project group led extensive relationship brokerage, included community voice, utilised national and
international evidence, and ran engagement via forums, advocacy, and a co-design process with 500
women from diverse backgrounds and over 20 organisations to develop the model. The community
engagement utilised the established networks, relationships, and links to community of the Logan
Together partners. Co-design with the women was facilitated through Logan Together and partner
agencies, community organisations, as well as the Logan Mums and Bubs website and the Logan
Community Group Alliance/QLD Community Alliance. It was a lengthy and multifaceted process over 18
months from late 2015- 2016, involving meeting with women and mothers, community listening, and
4 These are adapted from ‘Collective Impact 3.0’ articulated by the Tamarack Institute (Cabaj, M., & Weaver, L. 2016.
Collective impact 3.0: An evolving framework for community change) that are used by Logan Together. Logan Together
also has ‘First Nations First’ as a condition. See Contribution Analysis Technical Report and Evidence for further detail on
how the models compare.

Design. Evaluate. Evolve. 4
more formalised co-design sessions. It involved understanding how women wanted their care delivered,
spiritually and culturally, and to work with them to design it.
The community consultations demonstrated that women wanted to receive care where there was cultural
and community connections, a sense of safety and wanted input into a community governance group to
ensure power in decision-making about how they wanted to receive health services.
Throughout 2016, the model was further refined, and the recommended relationship-based continuity of
midwifery care model became the basis of the Logan Community Maternal and Child Health Hubs.
Women were able to continue to offer their perspectives through co-design meetings, Talanoa Circles (a
traditional Pasifika approach for inclusive community conversations and dialogues), public events, a
survey through Logan Mums and Bubs, and community engagement through key organisations.
Governance structures were set up, including an external Logan Community Maternity and Child Health
Oversight Committee. On the committee were representatives from community groups, NGO’s,
consumers, Primary Health Network, Queensland Nurses and Midwives’ Union (QNMU), university and
internal stakeholders.
The way the core group and partners worked strongly reflected collective impact practice and in
particular had inclusive engagement and capacity building as central priorities so women, community
representatives and organisations could participate in the design, development and decision making.
This involved building community and organisational capacity, and helping develop a community-
controlled service system response to deliver the Hubs in community. These conditions weren’t in place
when the co-design process started. Growing the movement for change and the necessary capacity
required the core group to walk alongside community and with champions in hospital settings who were
prepared to advocate for change. Creating the conditions for the Hubs to be culturally safe for both
women and service/ system partners took dedicated trust building and intensive support.
Across 2015-17, Health Consumers QLD, consumers from a range of organisations, and Logan
Together used strategic and influential advocacy to draw political attention to the urgency of improving
child maternal health in Logan and the need for funding. This also involved capacity building to support
champions and advocates to engage with government and influence decision makers who could help
progress the work. The success of the collective advocacy, compared with previous attempts to get the
Hubs concept off the ground, was influenced by the extent of community engagement, the strategy to
rally cross-system support, and that those with a shared agenda become ‘one voice’ – that was made up
by many different voices in community and community agencies and networks. People were also
prepared to be disruptive to make a statement on the issues. At one point a public march was on the
cards if political support was not forthcoming, however was not needed for the campaign.
In late 2016, a joint model and costing was provided to Queensland government for 6 Maternity Hubs in
Logan, by Metro South Health and Logan Together on behalf of collaborating partners.
Queensland Government funding was secured in 2017 via the Logan Community Health Action Plan
commitment (prioritising maternal and child health, mental health, immunisations and multicultural and
refugee health), and via the Innovation Fund to upscale antenatal care using MGP. At the time the state
Health Minister Cameron Dick was the local member of Parliament, who was a champion for the Hubs
and local Logan resident.
While good progress had been achieved, there were also many challenges and turning points for the
collaboration during the co-design and proposal drafting process. Challenges included: facilitating a
process for mixed stakeholders to have shared conversations and ‘truth telling’ about women’s
experiences of hospital-based care at the time; stakeholders having divergent views about
‘interventionalist’ versus more socially focused solutions; initial resistance from within health services to
the proposed socially focused models of care and a ‘community controlled’ service; keeping the
community voice front and centre during the finalisation of the model and the governance structure; and
the need for re-engagement with Metro South Health executive team following staff changes.

Design. Evaluate. Evolve. 5
Resolving and progressing the Hubs initiative took considerable effort by several key partners. One of
the turning points that helped overcome some of the early challenges was when stakeholders put energy
into developing a program logic for an ‘ideal model’ which fostered shared ownership over a possible
solution. Momentum was also maintained through many intensive rounds of negotiation and dialogues
when challenges arose. This process, and the sometimes ‘hard conversations’, was convened and
supported by the Project Group, Logan Together, and Health Consumers QLD. Throughout the co-
design and establishment, a key tension was balancing the need for compromise between partners, to
achieve consensus, while ‘protecting’ the important core principles of the community-informed model.
Opening of the Hubs in Community
Logan’s first three Maternity Hubs were launched in 2018, with the complex care service and a fourth Hub in
2019. These were all implemented by Metro South Health. See map to the right showing the community-
based Maternity Hubs.
By mid-2020, the Maternity Hubs had scaled to support close to 1000 women, which is larger than the
target cohort for the known high-risk cohort (n=600) of birthing women. The midwifery workforce had
increased from 12 in 2019, to 33 by March 2020.
The aspiration of the Oversight Committee for the future is for the Maternity Hubs to cater for up to 50%
of all 3,500 public system births in the City of Logan by 2025 (noting the broader vision is that all women
in Logan have universal access to community-based continuity of midwifery care in the longer term).
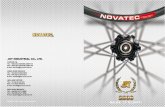
See Figure 1 for timeline of the Hubs journey. It covers milestones across the collective impact practice,
the pivots and challenges, the opening of Hubs and when changes started happening for target cohorts.
Many of the “changes in the system” in the timeline resulted from the collective impact practice. This is
expanded further in the next sections on outcomes and the contribution case for collective impact practice.

Design. Evaluate. Evolve. 6
Figure 1: Timeline of key events and milestones in the Maternity Hubs’ development and delivery

Design. Evaluate. Evolve. 7
What are the outcomes of the Maternity Hubs?
Outcomes for women and babies using the Hubs
The 2020 Evaluation Report compared women who received MGP and Hub care to women who received standard care (SC) at Logan Hospital.5 The overall results show that women in MGP were statistically significantly more likely to:
MGP SC
• Attend 5 or more antenatal appointments 97.7% 93.6%
• Undergo antenatal psychosocial screening 92.6% 86.6%
• Receive an influenza vaccine 65.6% 59.4%
• Have a spontaneous onset of labour 54.9% 44.3%
• Have a vaginal non-instrumental birth* 65.1% 59.0%
• Use non-pharmacological pain relief 54% 39.4%
• Exclusively breastfeed 74% 69%
And that women in MGP were significantly less likely to: MGP SC
• Require a caesarean section* 26% 30.2%
• Have a baby before 37 weeks gestation* 6.2% 8.9%
• Require Special Care Nursery (SCN) admission* 11.3% 14.9%
• Use epidural anaesthesia* 25.3% 29.8%
• Have an induction of labour 31.7% 38.5%
*These outcomes exclude data from the Complex Care MGP Service.
Health and social outcomes for women are resulting from referrals to support services through the Hubs
(e.g., to domestic violence, social isolation, mental health, and community connection supports).
Testimonies from women refer to wellbeing outcomes (beyond birthing and antenatal) for women and
families. Hubs are also improving culturally safe early and sustained engagement. The improvement in
the experience for culturally diverse women is important. Results show that the Hubs are more culturally
capable than standard care in Logan (2020 Evaluation report).
“It helped to have another Indigenous person guide me on my way. At hospital you don’t really
see many Indigenous people there.”
(Hub respondent from survey of women, 2020 Evaluation Report)
“The thing I liked best was my midwife communicated to me in language I could understand.”
(Hub respondent from survey of women, 2020 Evaluation Report)
5 2020 Evaluation Report (O’Connor, M., & Firmin, M. (2020). Community Maternity Hubs Model: Evaluation 30/10/2020. Queensland Health)

Design. Evaluate. Evolve. 8
“If women are in a continuity of care model such as ours, they also get access to many other
services. With our women, they can link into the Aboriginal and Torres Strait Islander medical
services and they can utilise the services there, such as their mental health and family
wellbeing services… these sorts of things can benefit women in keeping families together and
[providing] better outcomes in the maternity setting”
(Kyleigh Brown-Lolohea, Midwife, Jajumbora MGP, Logan Hospital/ Metro South Health)
(We are seeing these outcomes because) “we are embedded in the community. Women also
have ancillary and wrap around services… the synergies and relationships take a while… now
what’s happening at the three -nearly four year – mark is that sort of relationship connected-
ness that we have with child health and with family support and connected services with social
workers…. We’re getting people into services that will benefit them for a range of reasons.”
(Michelle O’Connor, MGP Midwifery Manager Logan Hospital)
While progress has been made, women using the service and key informants acknowledged that
entrenched systemic racism within institutions and services is an ongoing issue and needs continued
work. One response underway is investment in a scoping project and partnership building to explore how
the Hubs and hospital can support Birthing on Country/Birthing in Our Community in the future.
More broadly, there was evidence that the Hubs have contributed to system level changes in Logan. This
includes, yet is not limited to, the Hubs’ impact on the ‘maternity landscape’ and other early intervention
work in Logan, and that the Hubs’ are helping to connect women and families within the community.
“The hubs have significantly contributed to change and reform in the maternity space, and we
are seeing outcomes and results for the women and babies. The Hubs work built the platform
for really targeted early intervention work in Logan.”
(Matt Statham, Former Logan Together backbone employee)
“We are based in a deadly Kindy and they also have playgroups in the same centre… I am
engaging with women in a stronger together yarning circle, so bringing them into this safe
space, being culturally appropriate, culturally sensitive… and bringing women together. And
what I’ve seen happening is that they are developing these friendships and coming back into
this space.”
(Kyleigh Brown-Lolohea, Midwife, Jajumbora MGP, Logan Hospital/ Metro South Health)
Critical success factors about the Hubs and model
Women in the Hubs experience continuity of midwifery care within the community, which increases trust
and engagement in services, and improves observed outcomes for mothers and babies. There is strong
evidence that some of the unique features of the Hubs model and implementation (community-informed
elements of the local solution) are contributing to the Hubs’ effectiveness and outcomes.
Some of the evidenced critical success factors for the model include:
• women are at the centre of care
• it is a localised model of community health care
• it includes continuity of midwifery care via MGP
• it is creating culturally nurturing and connected spaces, including language diversity
• is overseen by a representative governance structure, and
• is making links between antenatal and general services.
At the core of the Maternity Hubs is ‘one known midwife’; evidence from evaluation reports and the wider
literature suggests that this increases trust in services by mothers, resulting in increased engagement in
services. It is likely that this is the primary mechanism for the outcomes experienced by the Maternity
Hubs. A survey of women using the Hubs found that 99% of 394 mothers who birthed through the
Maternity Hubs agreed that it was helpful to have the same midwife during their pregnancy.

Design. Evaluate. Evolve. 9
The following quotes are examples of positive testimonies provided by women using the Hubs.
“I’ve given birth through both the MGP hub model and mainstream, and so in my own
experience I can say that giving birth mainstream I felt isolated and experienced a lot more
anxiety. I definitely feel the hub model helps to reduce anxiety during pregnancy birth and
beyond.”
(Emily Ellis, Access Community Services)
“[My midwife] was a great help throughout everything. I feel having the same midwife is a
great comfort and felt less stressed.”
(Testimony from women using Hubs, 2020 Evaluation Report)
Other important factors included the growing trust from community; the integration being created
between birthing and general services; and that Maternity Hubs are demonstrating improved cultural
competency. Women are receiving care in a welcoming environment at a time of their choosing and the
power relations between health service provider and community member are more balanced.
“What is happening in Logan is this beautiful sort of synergy where women have started to
gain trust in this model. It’s in their community. It feels culturally safe. They’re happy to engage
and stay engaged after the six-week mark with all of the other services.”
(Michelle O’Connor, MGP Midwifery Manager Logan Hospital)
While the Maternity Hubs are established, key informants pointed
out that the Maternity Hubs model still must be ‘fought for’ – it is
not yet ‘business as usual’ and may be vulnerable if key advocates
and champions leave their posts. Members from the Oversight
Committee cited the need to “keep pushing” to ensure the model
continues. The areas for continued improvement identified during
the consultation with key informants included: involvement of First
Nations community and leaders, further increasing community
agency (generally), ongoing strategic learning, and working
together as long-term partners.

Design. Evaluate. Evolve. 10
Contribution analysis and the role of collective impact practice
Key Points:
• The effectiveness of the Hubs is credited to the model and in-community location of care. These essential elements were a direct result of the extensive community engagement and co-design with local women and stakeholders – driven by the collective impact practice.
• The contribution analysis findings demonstrate that without the collective impact practice the Hubs, and subsequent outcomes would not have happened.
• Inclusive engagement was a key factor for success in the Hubs story. It meant community preferences genuinely informed the model of care developed and in turn led to better service engagement and experiences.
• Over 20 partners collaborated in the set up of the Hubs, and all played unique and varying roles.
• Logan Together’s contribution was critical. The Logan Together Backbone Team and Cross Sector Leadership Group both played influential roles in bringing the framework for collective impact practice to the collaboration, and in driving a systems-wide engagement and advocacy that led to cross sector commitment and resourcing, without which the Hubs would not have been possible.
• When challenges arose, as is not unusual in new approaches and collaboration, Logan Together acted as a ‘container for change’ and convened both ‘front of house’ and ‘back stage’ conversations and resolution processes that helped sustain momentum for systems change.
“It is unlikely that the Hubs would have happened without collective impact…. We have been trying to tackle poor care at Logan for two decades!” (Professor Emeritus Jenny Gamble, Griffith University)
“Logan was able to provide what the women wanted and the service that they wanted for their maternity experience. And by creating that service that they wanted, it changes lives”. (Melanie McKenzie Director and Founder of Harrison’s Little Wings)
“There is absolutely no success without collectively working together...The whole MGP hub dynamic is really built on the success of listening to the community.” (Emily Ellis, Access Community Services)
“The Hubs now have an ability to support more than 1000 women. Almost perfect example of coming through some stormy seas at the beginning, bringing stakeholders together, getting the model up, the model is scaling to population scale, and of course, the actual health outcomes for women and babies are now moving very strongly in the right direction”. (Key informant, 2020)
The collaborating partners – the ‘whole’ is greater than the sum of the parts
Over 20 partners played significant and/or essential roles in the design and implementation of the
Maternity Hubs and together have made a collective impact. Several of the stakeholders interviewed
noted that the collective effort was greater than the sum of its parts.
Within the collective, some of the key contributing partners included:6
• Logan Community and Maternity Child Health Oversight Committee and original project group (made
up of representatives from a mix of the stakeholder groups below).
• Community members, families, consumer advocates, leaders and local groups.
• Logan Together collective impact initiative, including representatives from the movement, the
backbone team, and cross sector leadership group.
• Health services including Metro South Health, Logan Hospital, Child’s Health Queensland, Brisbane
South Primary Health Network
• Governments across three levels, including Queensland Health, and federal and local political support
• Host partner organisations: Aboriginal and Torres Strait Islander Community Health Service
(ATSICHS), Access Community Services, Village Connect, Benevolent Society.
• Wrap around support and local services.
• Organisations providing advocacy, academic and implementation support, including Griffith University,
Queensland Nurses and Midwives Union, and Health Consumers Queensland.
6 See Contribution Analysis Technical Report and Evidence for further detail and evidence on partner contributions.

Design. Evaluate. Evolve. 11
The role of Logan Together
Logan Together was a driver and facilitator of change (acting as a ‘container for change’) and played
several influential roles in the co-design and set-up of the Hubs. All key informants stated that Logan
Together was instrumental in the establishment of the Hubs and agreed that the co-designed Hubs
would not have been established otherwise.
Across myriad roles, Logan Together demonstrated leadership to change the system, brought its
collective impact framework to define the ‘way of working’ and community engagement, and drove
momentum. The collective impact practice of Logan Together was a key factor that differentiated the
results from previous attempts to evolve the Hubs concept and prior programmatic responses seeking to
affect maternity and birthing outcomes.
We had this momentum in the community, created through this shared, connected, visioning
process which the whole Logan Together Framework enabled through the coming together of
interested parties.”
(Professor Emeritus Jenny Gamble, Griffith University)
Logan Together also added strategic value through the advocacy, brokerage of power relations, capacity
building. Key informants described Logan Together as a ‘connector’, ‘facilitator’, ‘advocate’, ‘supporter’
and ‘incubator’, as well as convening difficult conversations and challenging partner dynamics so that
momentum was sustained.
“There was a lot of capacity built in government to work in a different way. The result has been
some pretty remarkable outcomes when it comes to improving antenatal engagement and
smoking cessation. That whole design element of working with community has paid off.”
(Matt Statham, Former Logan Together backbone employee)
“I've always thought of Logan Together as a hothouse incubating new ways and new ideas
and new perspectives on things. The contribution of Logan Together in putting the agenda of
investing in early years …(and their advocacy) for the sorts of changes that are required …
(Logan Together also made) a contribution for those little conversations about collaboration,
investment reform and outcomes focus. There are all sorts of little green shoots out there now,
that go to the sorts of changes that need to happen, that if Logan Together did not exist
wouldn’t be there.” (Key informant, 2020)
“Collective change is a huge part of what the (Logan Together) movement is about, bringing a
number of organisations together to not duplicate the work and just to find these ways that
everybody can be actually working aligned together, rather than in silos… like the Maternity
Hubs have.” (Key informant, 2020)
The Logan Together Cross Sector Leadership Table was able to leverage their system-wide networks
for advocacy and provided governance and support of the Hubs as a strategic high leverage project.
They played a critical role in developing and endorsing the joint funding proposal with Metro South
Health which led to essential funding. They prioritised Logan Together resources in supporting the
Backbone Team to drive the on-the-ground collective impact practice and helped in navigating some of
the challenges and continued issues around the Hubs’ governance, the service model, and
implementation.
The Backbone Team and leaders within the team played a catalytic and strategic leadership role and
scaffolded the initiation, co-design and implementation. In the early phases it was the Backbone Team
that initiated the community engagement process, established the project group, and strongly led the co-
design process. The Team designed engagement to be ‘in-community’ to make it inclusive and worked
one on one where needed to help build capacity of community members and partnering community
organisations to participate. In one case, this involved the development of a community-controlled
service organisation with the Māori and Pasifika community to deliver the Hub.

Design. Evaluate. Evolve. 12
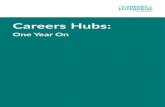
Figure 2: Significant and essential contributing partners in the collective impact practice and development of the Maternity Hubs

Design. Evaluate. Evolve. 13
The Backbone Team were able to fill a data gap in the maternal and child health field and provide
analysis for building a compelling, evidence -informed case for change. While the Maternity Hubs
concept and momentum existed, and community already had the assets to move to Maternity Hubs, the
Team helped draw attention and commitment by government and power brokers (including generated
contextual data that highlighted Logan issues and opportunities in new ways). For example, Logan
Together’s State of Logan’s Children and Families Report and local hospital data influenced the
Queensland Health Logan Community Health Action Plan 2017 (CHAP) in which $10M was committed
to improve the health and wellbeing of the Logan community.
The impact of collective impact practice
The effectiveness of the Hubs via the model and in-community location of care, is a direct result of the
extensive community engagement and co-design with local women and stakeholders – driven by the
collective impact practice. Without the collective impact practice, the Hubs and subsequent outcomes
would not have happened.
The contribution analysis verified a strong ‘chain of contribution’ between the collective impact practice in
building the conditions and systems changes that enabled the co-design and set up of the Hubs service
model, and in turn had strong causal links to Hubs’ outcomes. Some key lines of contribution included:
• The existing foundations and growing momentum for change were important starting conditions
that shaped the Maternity Hubs’ getting off the ground– partly from consumer advocates in
Logan but also from other groups such as the Queensland Community Alliance.
• Inclusive community engagement, with data and evidence collected and presented in new ways,
allowed stakeholders to understand the problem and become ‘of one voice’ with shared aspirations
during the co-design phase. This strengthened collective advocacy for a model that would suit
community needs, resulting in new resourcing to deliver the Maternity Hubs in the community.
• The Maternity Hubs are a high-leverage activity that takes a systems approach which has
fostered trust by users.
• The model is supported by a backbone team and local leadership and governance through the
Oversight Committee. The committee provides a space for continued collective advocacy and
strategic learning, which has changed mindsets and collective practice. Logan Together
Backbone Team and Leadership Table played crucial roles in driving collective practice and in
the Hubs development.
• Inclusive community engagement has contributed to community agency and strengthened
strategic learning.
• Women in the Hubs experience continuity of care within the community, which increases trust
and engagement in services, and improves observed outcomes for mothers and babies.
The contribution analysis revealed while all of the collective impact conditions were evidenced as playing
a contributing role, the conditions having the most influence on outcomes were:
• Inclusive community engagement
• Strategic and persistent collective advocacy
• Dedicated working groups to provide strategic oversight and enabling support (Hub project
group, governance via the Oversight Committee, Logan Together as a ‘container for change’).

Design. Evaluate. Evolve. 14
What collective impact practice looked like in the Logan context
The collective impact conditions as seen in Logan through the Hubs process are described below.
1. The Systems approach underpinning the collective impact practice had a strong influence on the
co-designed model with its holistic, wrap around social service support and place-based approach to
care. It shaped the set-up of cross sector structures, sustained participation, alignment, and
increased points for leverage across and beyond the health system. It also influenced shifts in the
service system from hierarchical to being more adaptive and flexible and helped reduce duplication.
2. Inclusive community engagement not only influenced the resultant Hub model and in-community
locations, it also strengthened many of the other collective impact conditions and amplified the
impact of activities such as the collective advocacy to secure political commitment and funding. It
influenced the extent of community agency and strategic learning, and included capacity building.
“There was a lot of energy from the start of the project, in terms of the amount of community engagement and the amount of interest from government for progressing this work… Part of the process was also about building community capacity and leadership to find and support the people who had the passion to drive it.” (Matt Statham, Former Logan Together backbone employee)
3. High leverage activities: The naming and prioritising of the Maternity Hubs project as a high-
leverage activity in the region, and the focus given to it by Logan Together Leadership Table
selecting it as one of their first strategic projects, was important for ensuring that there was the drive
and resources to invest in developing the model.
4. Backbone, local leadership and governance through the Oversight Committee provided a space
for continued collective advocacy and strategic learning, and was driven by cross sector
representation. This was important as it offered a way for community to be involved in the
governance model which had not happened before in other care models. The enabling support and
governance drove the ‘relentless’ and ‘persistent’ push for cross sector engagement and influenced
policy commitment, attracted investment, and improved coherence of strategy for better outcomes for
children and women in target cohorts.
5. Shared aspiration and strategy as the movement around the Hubs got going meant collaborating
partners started to commit to shared strategic objectives in new ways and started to behave and
allocate their resources accordingly. At the beginning of the process, it was reported that there was
not a shared aspiration by everyone. However, those with a shared aspiration created ‘one voice’ for
collective advocacy.
6. Strategic learning, data, and evidence use happened at the scale of individual practitioners,
governance bodies, and for organisations and services. This helped the collective to articulate the
community health data, needs and opportunities in new ways, which in turn influenced stakeholder
and community engagement. There are also ongoing learning and feedback loops that happen via
informal and formal processes: One key informant commented, “It’s not just checking in with your
consumers, it’s also making sure that you are regularly connected with your partners”.
“I’m involved in the MGP Hub operational group with Metro South Health, the other Hubs and
Logan Together. This has been a really great opportunity to come together and discuss great
outcomes but also challenges and barriers we see through our hubs. Together we have been
able to come up with a collective consensus on how we might be able to reduce those
barriers.”
(Emily Ellis, Access Community Services)

Design. Evaluate. Evolve. 15
Conclusion
Figure 3 shows a detailed theory of change for the Hubs based on the contribution analysis. It models
how change is happening and is expected to happen in the future. The application of collective impact
practice in delivering outcomes is a relevant and timely demonstration of how place-based and
community-led action achieves outcomes that would not have otherwise been possible.
Collective impact practice was essential for building the enabling conditions for the Hubs’ development
and implementation, and has been pivotal as the Hubs have continued to evolve, adapt, and be scaled.
Investing in building the collective impact conditions has directly contributed to the outcomes realised for
women and babies at the Hubs. It also contributed to other important changes for Logan organisations
and community (including wellbeing and other less tangible systems changes).
The contribution of the Hubs to population level changes is an area to monitor over the coming years as
the timeframe and scale for outcomes to be realised at this level increases. As well as tracking perinatal
outcomes, it will be valuable to monitor the broader outcomes the Hubs are achieving, including those
achieved via the wrap around services – which are expected to extend the impact of the Hubs further for
communities and families.
We respect and acknowledge the Traditional Custodians of the Logan City area, including the Yugambeh and Yuggera language speaking people. We would like to thank the many people that have contributed to the analysis and we extend appreciation to all of the key informants. We acknowledge the dedicated efforts of the Logan Together Backbone Team, the members of the Logan Community Maternal and Child Health Oversight Committee who participated in sharing their insights and accounts, and DSS input. The report was produced by Clear Horizon, led by Dr Ellise Barkley and team.
Interested in finding out more? See Contribution Analysis Technical Report and Evidence (separate document).

Design. Evaluate. Evolve. 16
Figure 3: Detailed Theory of Change for the Maternity Hubs
The work to create the Logan Together Hubs and the results of this work have been mapped below to the Stronger Places, Stronger People Theory of Change. The
contribution chain and the causal links evidenced align strongly with how change is expected to happen in the Stronger Places, Stronger People theory of change. Below the
dotted line are the outcomes in the Hubs’ sphere of influence.