Local Anesthetics 5

of 117
Transcript of Local Anesthetics 5
-
8/14/2019 Local Anesthetics 5
1/117
Local Anesthetics
-
8/14/2019 Local Anesthetics 5
2/117
2
General principles
Chemistry.
Esters-Procaine
-Chloroprocaine-Tetratcaine
-Cocaine
Metabolism-Hydrolysis by pseudo-
cholinesterase enzyme
Amides-Lidocaine
-Mepivacaine-Bupivacaine
-Etidocaine
-Prilocaine
-Ropivacaine
Metabolism-Liver
-
8/14/2019 Local Anesthetics 5
3/117
3
General principles
B.Mechanism of action 1.Local anesthetics block nerve conduction
2. Local anesthetics interact directly with
specific receptors on Na+ channel3. Physiochemical properties
High lipid solubilityprotein binding
pKa
Lower pH of the drug solution
4.Differential blockade of nerve fibers5. Sequence of clinical anesthesia.
6. Pathophysiologic factors .
-
8/14/2019 Local Anesthetics 5
4/117
4
Clinical uses of local anesthetics
The drugs in common use are
lignocaine, bupivacaine and prilocaine,
their characteristics are shown in Table.The choice of drug depends on the
speed of onset and duration of action
required. Epinephrine (adrenaline)
prolongs the latter.
-
8/14/2019 Local Anesthetics 5
5/117
5
Characteristics of local anaesthetic drugs
7
2
8
3
2
4
13
14
13
Lignocaine
Bupivacaine
Prilocaine
With
epinephrine
(mg/kg)
Plain
(mg/kg)
Duration
(h)
Agent
Maximum dose
-
8/14/2019 Local Anesthetics 5
6/117
6
Local anaesthetic drugs have serious side
effects if given in excess, or inadvertently released
into the circulation. Toxicity is manifested in avariety of ways ranging from mild excitation to
serious neurological and fatal cardiac sequelae.
-
8/14/2019 Local Anesthetics 5
7/117 7
Symptoms and signs of local anaesthetic toxicity
Anxiety Restlessness
Nausea
Tinnitus Circumoral tingling
Tremor
Tachypnoea
Clonic convulsions Arrhythmias
ventricular fibrillation
asystole
-
8/14/2019 Local Anesthetics 5
8/117 8
Recommendations for the safe use ofepinephrine in local anaesthetic solutions No hypoxia
No hypercapnia
Caution with arrhythmogenic volatile agents,for example, halothane
Concentration of 1:200,000
Dose
-
8/14/2019 Local Anesthetics 5
9/117 9
Requirements before starting regional
anaesthesia Informed consent
Vascular access Resuscitation drugs and equipment
Sterility of anaesthetist
Sterility of operative site
No contraindications to procedure Correct dosage of local anaesthetic drug
-
8/14/2019 Local Anesthetics 5
10/117 10
Epidural Spinal and Caudalanaesthesia
-
8/14/2019 Local Anesthetics 5
11/117 11
General considerations
A.Preoperative assessmentB. The area where the block is to be administered
should be examined
C. A history of abnormal bleeding
and a review of the patient's medicationsD. Patients should be given a detailed explanation
E. patients should receive appropriate monitoring
and have an intravenous (IV) line in place
-
8/14/2019 Local Anesthetics 5
12/117 12
Segmental level required for surgery
A knowledge of the sensory, motor, and autonomic
distribution of spinal nerves will help the anesthetist
determine the correct segmental level required for a
particular operation and help anticipate the potentialphysiologic effects of producing a block to that level.
illustrates the dermatomal distribution of the spinal
nerves.
-
8/14/2019 Local Anesthetics 5
13/117
13
Segmental level required for surgery
Key Dermatomes & Levels-C1-C2: Oops
-C3,4,5: Keep the diaphragm
alive
-T1-T4: Cardioaccelerator
-T4: Nipple line
-T6: Xyphoid process
-T10: Umbilicus-S2,3,4: Keep the penis
off the floor
-
8/14/2019 Local Anesthetics 5
14/117
14
-
8/14/2019 Local Anesthetics 5
15/117
15
A. Absolute1.Patient refusal.
2.Localized infection at skin puncture site.
3.Generalized sepsis (e.g., septicemia, bacteremia).
4.Coagulopathy.5.Increased intracranial pressure.
B. Relative
1.Localized infection peripheral to regional technique site
2.Hypovolemia.3.Central nervous system disease.
4.Chronic back pain.
Contraindications to peridural anesthesia
-
8/14/2019 Local Anesthetics 5
16/117
16
Section 1 Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
17/117
17
Epidural anesthesiais achieved by introduction of anesthetics into
the epidural space.
-
8/14/2019 Local Anesthetics 5
18/117
18
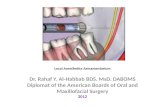
Anatomy
The epidural space runs from the base of the skullto the bottom of the sacrum at the sacrococcygeal
membrane. The spinal cord, cerebrospinal fluid
and meninges are enclosed within it .
-
8/14/2019 Local Anesthetics 5
19/117
19
The spinal cord becomes the cauda equina at
the level of L2 in an adult and the cerebrospinal
fluid stops at the level of S2. The epidural space
is 36mm wide and is defined posteriorly by the
ligamentum flavum, the ante-rior surfaces of the
vertebral laminae, and the articular processes.
Anteriorly it is related to the posterior
longitudinal ligament and laterally is bounded bythe intervertebral foramenae and the pedicles.
Anatomy
33 Vertebra (inc 4 coccygeal)
Curvature(
L1 and S2 (end of cord/dura)
Angle of spinal processes
-
8/14/2019 Local Anesthetics 5
20/117
-
8/14/2019 Local Anesthetics 5
21/117
21
Anatomy
This is an accurate, and evencolorful representation of
the Epidural space in
relation to other structures
present in the vertebral area
-
8/14/2019 Local Anesthetics 5
22/117
22
Anatomy
The view from above
looking down, gives
an interesting perspective
on the planes traversed with
the epidural needle
-
8/14/2019 Local Anesthetics 5
23/117
23
Epidural anesthesia technique--Preparation
Obtain an epidural anesthesia kit
Check the contents of the kit for the
following items
-Skin local
-Test dose
-16-18g Husted or Touhy needle
-Glass syringe-Epidural catheter with adapter for
injection
-Various needles for local, seeker,
etc.
-
8/14/2019 Local Anesthetics 5
24/117
24
-
8/14/2019 Local Anesthetics 5
25/117
25
Epidural anesthesia techniquePositioning Sitting vs. lateral decubitis
-Most beginners do better sitting
-ALL patients should be on the monitor before starting
Encourage the patient to extrude their lower back
-Use yourself as an example
- Push your back out toward me, arched like a mad
cat
- pretend you are the worlds largest boiled shrimpThis will open up the interspace, help ID your landmarks, and
improve your chances
-
8/14/2019 Local Anesthetics 5
26/117
26
-
8/14/2019 Local Anesthetics 5
27/117
27
Epidural anesthesia technique
Approach
1.Midline easier
2.Paramedian
when there is narrowing of the
interspace or difficulty in flexion of
the spine
Paramedian Approach:
Larger Aperture
Better feel
-
8/14/2019 Local Anesthetics 5
28/117
28
Epidural anesthesia
Epidural anesthesia technique Preparation of the skin is done in a circular motion
from the center out to the periphery
Use all 3 scrub brushes
Place eye drape centered over your target You can use either the end of your pen or your
fingernail to make an indentation in the back to find
your target more readily
-
8/14/2019 Local Anesthetics 5
29/117
29
Epidural Anesthesia
Epidural anesthesia technique Skin wheal is accomplished with plain lidocaine
Be fairly generous
Seeker needle is placed and more local injected on
removal Some people like to use an 18g needle to break the
skin, followed by the epidural needle into the same
hole
This is because the epidural needle is not sharp andsignificant pressure may be required to break the skin
with it
-
8/14/2019 Local Anesthetics 5
30/117
30
Epidural Anesthesia
Epidural anesthesia technique The needle is inserted using landmarks and position
identical to that used in spinal anesthesia
Advance the needle and go through the supraspinous
ligament (feels gritty) and seat it in the intraspinousligament
Now the needle should not droop when you let go
Remove the stylet at that time and place your glass
syringe tightly onto the hub of the needle
-
8/14/2019 Local Anesthetics 5
31/117
31
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
32/117
32
Epidural Anesthesia
Epidural anesthesia technique Loss of resistance technique
Some people use saline
Some use air
Some wet the barrel with saline and use air Some use a combination of air and saline
Advance the needle 1mm at a time, then ballot the
syringe
-
8/14/2019 Local Anesthetics 5
33/117
33
Epidural Anesthesia
Epidural anesthesia technique Loss of resistance technique
Maintain contact with the skin with your nondominanthand
You will notice the resistance increase when you enter
the ligamentum flavum This is not always the case in OB
Continue to advance until air/saline injects with ease
Injecting saline may help tent the dura and makecatheter placement easier
If fluid rushes back at you when you disconnect thesyringe, it is probably CSF
-
8/14/2019 Local Anesthetics 5
34/117
34
Epidural Technique(Loss of Resistance Technique)
Hand-position
Note depth
Air or Saline debate
Catheter 3-5 cm in space (should go easily)
-
8/14/2019 Local Anesthetics 5
35/117
35
Air vs Saline LOR Technique
-
8/14/2019 Local Anesthetics 5
36/117
36
Hanging drop technique
Consider forCervicalEpidurals (thinepidural
space) Prone or
sitting
-
8/14/2019 Local Anesthetics 5
37/117
37
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
38/117
38
Epidural Anesthesia
Epidural anesthesia technique If you think you may have wet tapped the patient, butare not sure, or if you aspirate fluid from your catheter,you can test it using glucose test strips
The catheter has a large mark on it to signify the end
of the needle You advance the catheter 2.5 to 4cm
Hold the catheter as you remove the needle
When the catheter is visible at the skin, grasp it there
and pull the needle the rest of the way off
-
8/14/2019 Local Anesthetics 5
39/117
39
Epidural Anesthesia
Epidural anesthesia technique Place the catheter injection adapter onto the catheter
Push the end of the catheter into the adapter and
screw it closed
Give it a gentle tug to ensure it is seated and clamped Tape the catheter in the manner. The techniques
vary greatly
-
8/14/2019 Local Anesthetics 5
40/117
40
Epidural Anesthesia
Epidural anesthesia technique Using sterile technique, draw up your test dose
Aspirate the catheter to ensure you do not see fluid or
blood
Inject 3ml of test dose (pt.should be on the monitor) If catheter is intravenous, you should notice a 20%
increase in B/P and Heart rate, due to the 15ug
epinephrine
If the catheter is subarachnoid, you should notice a
sympathectomy and partial sensory/motor block ensure
-
8/14/2019 Local Anesthetics 5
41/117
41
-
8/14/2019 Local Anesthetics 5
42/117
42
Epidural Anesthesia
Epidural anesthesia technique The rule of thumb is 0.5-1.5ml of local per segment
of block desired
3-5ml of local every 3 minutes until level desired is
reached Slow dosing decreases the untoward sympathectomy
complications
Baricity is not a factorin the epidural space,
because there is no other fluid normally present
-
8/14/2019 Local Anesthetics 5
43/117
43
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
44/117
44
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
45/117
45
Epidural Anesthesia
Epidural anesthesia technique Place the patient in the position of comfort if laboring
For non labor patients, do not position them for
surgery until you are sure you have an adequate
block Gravity matters! It will influence the direction and
spread of the block, so consider its implications
during your dosing regimen
-
8/14/2019 Local Anesthetics 5
46/117
46
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
47/117
47
Epidural Anesthesia
Combined spinal/epidural technique Spinal anesthetic followed by epidural infusion
Combines rapid onset with sustained analgesia
May be used for surgery/post op pain management
May be used for labor/delivery
Access epidural space
Spinal needle fits through the lumen of the epidural
Epidural needle is special must have back eye
-
8/14/2019 Local Anesthetics 5
48/117
48
Epidural anesthesia
Undocumented concern
exists that some of the
epidural injection canmigrate subarachnoid,
causing an increased
level of block
-
8/14/2019 Local Anesthetics 5
49/117
49
Epidural Anesthesia
Immediate complications of epidurals Sympathetic nervous system disruption
(sympathectomy)
Severe hypotension (pre-ganglionic sympathetic block)
Peripheral vasodilation Venous pooling
Reduction in venous return
High block may result in anesthetizing cardiac
accelerators (T1-T4), with resulting slowed heartrate
called the Bainbridge Reflex
-
8/14/2019 Local Anesthetics 5
50/117
50
Epidural Anesthesia
Immediate complications of epidurals Perioperative hypotension
Rapid position changes
Skeletal muscle tone loss
Decreased venous return Reflex surgical stimulation
Low volume status
Preoperative medications
Concurrent medical problems
-
8/14/2019 Local Anesthetics 5
51/117
51
Epidural Anesthesia
Immediate complications of epidurals Perioperative management of hypotension
Non glucose containing crystalloid solutions
5mL/kg bolus
Elevated heart rate phenylephrine (if no
contraindications)
Decreased heart rate ephedrine (if no
contraindications)
Risk of mortality increases the longer hypotension
persists
Be careful using trendelenburg position, especially
when you are using a hyperbaric spinal or high volume
epidural
E id l A h i
-
8/14/2019 Local Anesthetics 5
52/117
52
Epidural Anesthesia
Immediate complications of epidurals Hypertension
Rare, but does happen
Anxiety
Pain Vasopressors
Consider vasodilators, narcotics, anxioulytics
Always consider discomfort in the places that are NOT
anesthetized.
E id l A th i
-
8/14/2019 Local Anesthetics 5
53/117
53
Epidural Anesthesia
Immediate complications of epidurals Hypoxia and/or hypercarbia
High level of block can be insidious
Remember C3,4,5 keeps the diaphragm alive
Once your level of blockead has exceeded C3, phrenicnerve paralysis will ensue
Perception of intercostal nerves and abdominal
excursion is lost at the level of T2-4
Intercostal nerves account for 20% of tidal breathing
some of our patients dont tolerate that well!
E id l A th i
-
8/14/2019 Local Anesthetics 5
54/117
54
Epidural Anesthesia
Immediate complications of epidurals Hypoxia and/or hypercarbia
Anxiety due to inability to sense tidal breathing may
occur
Increased doses of sedatives and/or narcotics cancompound your problem
Hypoventilation increases with decreasing level of
consciousness
With intercostal nerve paralysis, cough becomes
ineffective
May lead to inability to protect the airway
E id l A th i
-
8/14/2019 Local Anesthetics 5
55/117
55
Epidural Anesthesia
Total spinal/epidural Can lead to acute pulmonary collapse Treated symptomatically
Intubation required
Will loose consciousness Will be severely hypotensive, requiring vasopressor
infusion
Unopposed parasympathetic system leads tobradycardia and vomiting
E id l A th i
-
8/14/2019 Local Anesthetics 5
56/117
56
Epidural Anesthesia
Immediate complications of epidurals Nausea and/or vomiting
Parasympathetically mediated
Always rule out neurological hypoxia as the first cause
Factors that increase neurological hypoxia: ETOH (ethyl alcohol )
Obesity
Prone position
Apprehension
High level of blockade
E id l A th i
-
8/14/2019 Local Anesthetics 5
57/117
57
Epidural Anesthesia
Immediate complications of epidurals Intravascular injection
You can neverover test dose a catheter
You should re-test dose if it has been 4 hours since
placement or last bolus IV lidocaine leads to neurologic symptoms, such as
ringing in the ears, metallic taste in mouth, numbness
and/or tingling around the mouth
Epinephrine 15ug should be enough to cause
hypertension, palpitations, anxiety, tachycardia
E id l A th i
-
8/14/2019 Local Anesthetics 5
58/117
58
Epidural Anesthesia
Immediate complications of epidurals Intravascular injection
ALWAYS aspirate your catheter before you inject
EVERY time
Positive blood aspiration requires immediate removaland/or replacement of catheter
Positive CSF aspiration is problematic- use blood
glucose strip to test if unsure, or CSF will precipitate
when mixed with thiopental (not as accurate)
E id l A th i
-
8/14/2019 Local Anesthetics 5
59/117
59
Epidural Anesthesia
Immediate complications of epidurals Subarachnoid injection
Immediate change in sensorium
Anxiety
Dyspnea Immediate intubation and vasopressor support are
crucial to survival
Discontinue the catheter
Call for help!
E id l A th i
-
8/14/2019 Local Anesthetics 5
60/117
60
Epidural Anesthesia
Delayed complications of epidurals Post dural puncture headache (PDPH)
Can occur after either obvious or occult dural puncture
CSF leaks chronically out of the hole in the dura
Decreased amount of available CSF in Subarachnoidspace
Medulla and brainstem sag into foramen magnum
Resulting stretching of the meninges and pulling on the
tentorium cause the headache
E id l A th i
-
8/14/2019 Local Anesthetics 5
61/117
61
Epidural Anesthesia
Delayed complications of epidurals Post dural puncture headache (PDPH)
Headaches most common in parturients, as they
already have a decreased CSF production and
engorged epidural veins
The proposed causes are related to
Needle type and size
Direction of the bevel
Number of punctures
Patient position
Epid ral Anesthesia
-
8/14/2019 Local Anesthetics 5
62/117
62
Epidural Anesthesia
Delayed complications of epidurals Post dural puncture headache (PDPH)
Incidence decreases with age
More common in women than men
Patient expectations have been correlated with
incidence
Symptoms include:
Increased pain with upright position
Frontal/occipital headache
Stiff neck and shoulders
Nausea and/or vomiting
Vertigo( )
Blurred vision
Epidural anesthesia
-
8/14/2019 Local Anesthetics 5
63/117
63
Epidural anesthesia
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
64/117
64
Epidural Anesthesia
Delayed complications of epidurals Post dural puncture headache (PDPH)
Conservative treatment is always attempted first
Bed rest
Vigorous hydration (if tolerated) Use of sedatives and opioids
Abdominal binder for ambulation
Caffeine and niacin
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
65/117
65
Epidural Anesthesia
Delayed complications of epidurals Post dural puncture headache (PDPH)
Definitive treatment is epidural blood patch
Epidural space is accessed using sterile technique
30cc of blood drawn from dependent antecubital ofpatient
Blood is slowly injected into epidural needle until the
patient complains of pressure in the back
Pt. Placed supine flat in bed for 2 hours
Severe backache (you artificially induced one heck of abruise!) almost always follows (tx with ice, analgesics)
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
66/117
66
Epidural Anesthesia
Delayed complications of epidurals Low back pain
Many patients will complain of backache after epiduralremoved
Traumatic procedure with large needle
Consider if patient positioning during surgery couldhave exacerbated symptoms
Were there multiple attempts/punctures?
Prolonged labor?
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
67/117
67
Epidural Anesthesia
Delayed complications of epidurals Urinary retention
Common in labor
Most places place foley after epidural in place
Sympathetic blockade allows for parasympatheticoverride
Bladder distention may occur with fluid bolus
Full bladder can impede fetal decent
Narcotics can exacerbate urinary retention Allow attempt to void, if possible
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
68/117
68
Epidural Anesthesia
Delayed complications of epidurals Infection Septic meningitis
Aseptic meningitis
Adhesive arachnoiditis Intraneural injection
Injection of wrong medications
Undiagnosed neurological disease
Epidural Anesthesia
-
8/14/2019 Local Anesthetics 5
69/117
69
Epidural Anesthesia
Technical difficulties in epidurals Broken needles
Most common cause is burying the needle
Broken or sheared catheters
NEVER pull a catheter back through the insertion needle
ALWAYS chart that the tip of the catheter was intact whenyou removed it
Visually inspect all catheters before inserting them
Glass from broken vials in the epidural space
Break away from the tray and use a 4X4
Use filter needles Do not core the bottom of the vial when drawing from it
-
8/14/2019 Local Anesthetics 5
70/117
70
-
8/14/2019 Local Anesthetics 5
71/117
71
-
8/14/2019 Local Anesthetics 5
72/117
72
-
8/14/2019 Local Anesthetics 5
73/117
73
-
8/14/2019 Local Anesthetics 5
74/117
74
-
8/14/2019 Local Anesthetics 5
75/117
75
-
8/14/2019 Local Anesthetics 5
76/117
76
-
8/14/2019 Local Anesthetics 5
77/117
77
-
8/14/2019 Local Anesthetics 5
78/117
78
-
8/14/2019 Local Anesthetics 5
79/117
79
-
8/14/2019 Local Anesthetics 5
80/117
80
-
8/14/2019 Local Anesthetics 5
81/117
81
-
8/14/2019 Local Anesthetics 5
82/117
82
-
8/14/2019 Local Anesthetics 5
83/117
83
-
8/14/2019 Local Anesthetics 5
84/117
84
-
8/14/2019 Local Anesthetics 5
85/117
85
-
8/14/2019 Local Anesthetics 5
86/117
86
Section 2 Spinal anesthesia
-
8/14/2019 Local Anesthetics 5
87/117
87
Spinal anesthesiainvolves the administration of local anesthetic into
the subarachnoid space.
Anatomy
-
8/14/2019 Local Anesthetics 5
88/117
88
y
1.The spinal canal extends from the foramen magnumto the sacral hiatus.
2.Three interlaminar ligaments bind the vertebral
processes together:
supraspinous ligamentinterspinous ligament
ligamentum flavum
3. The spinal cord extends the length of the vertebral canal
during fetal life, ends at about L-3 at birth, and moves
progressively cephalad to reach the adult position near
L-1 by 2 years of age.
Anatomy
-
8/14/2019 Local Anesthetics 5
89/117
89
4. The spinal cord is invested in three meninges:
The pia mater.
The dura mater.
The arachnoid .
5. The subarachnoid space lies between the pia
mater and the arachnoid and extends from the
attachment of the dura at S-2 to the cerebralventricles above. The space contains the spinal
cord, nerves, cerebrospinal fluid (CSF), and
blood vessels that supply the cord.
y
Physiology
-
8/14/2019 Local Anesthetics 5
90/117
90
Physiology
1.Neural blockade. Smaller C fibers conveying autonomicimpulses are more easily blocked than the larger sensory
and motor fibers.
2. Cardiovascular. Hypotension is directly proportional to
the degree ofsympathetic blockade produced.3. Respiratory. Low spinal anesthesia has no effect on
ventilation. With ascending height of the block into the
thoracic area, there is a progressive ascending intercostal
muscle paralysis.
Physiology
-
8/14/2019 Local Anesthetics 5
91/117
91
4.Visceral effects
Bladder.
Intestine.
5. Renal blood flow is maintained, except
with severe hypotension.
6. Neuroendocrine.
7. Thermoregulation.
y gy
Technique
-
8/14/2019 Local Anesthetics 5
92/117
92
q
1.Spinal needle.
Technique
-
8/14/2019 Local Anesthetics 5
93/117
93
2.Patient position.
q
a.lateral position .
b.sitting position
c.prone position
Technique
-
8/14/2019 Local Anesthetics 5
94/117
94
3.Procedure
a.The L2-3, L3-4, or L4-5 interspaces are commonly
used for spinal anesthesia.
b. Disinfect a large area of skin with an appropriate
antiseptic solution.
c. Check the stylet for correct fit within the needle.
d. Raise a skin wheal with 1% lidocaine and a 25-gauge
needle at the spinal puncture site.
q
Technique
-
8/14/2019 Local Anesthetics 5
95/117
95
e. Approaches1.Midline.
2.Paramedian.
3.Needle placement.
5.Administration of anesthetic.
4.Remove the stylet
Technique
-
8/14/2019 Local Anesthetics 5
96/117
96
f. Closely monitor (every 60 to 90 seconds)
blood pressure, pulse, and respiratory function
for 10 to 15 minutes. Determine the ascending
anesthetic level by noting the response to gentlepinprick or a cold alcohol swab. Stabilization
of the local anesthetic level takes about 20 minutes.
Determinants of level of spinal blockade
-
8/14/2019 Local Anesthetics 5
97/117
97
p
1.Drug dose.
2. Drug volume.
3. Turbulence of CSF.
4. Baricity of local anesthetic solution.5. Increased intraabdominal pressure.
6. Spinal curvatures.
Complications
-
8/14/2019 Local Anesthetics 5
98/117
98
p
1.Hypotension
2. Bradycardia3. Paresthesias.
4. Bloody tap.
5. Dyspnea
6. Apnea7. Nausea and vomiting
8. Postdural puncture headache
9. Backache.
10. Urinary retention.
11. Neurologic impairment
12. Infection
-
8/14/2019 Local Anesthetics 5
99/117
99
Epidural techniques are more difficult to master,
so knowledge of where your needle is is vital
Summary
-
8/14/2019 Local Anesthetics 5
100/117
100
Midline Approach
-Skin
-Subcutaneous tissue
-Supraspinous ligament
-Interspinous ligament- Ligamentum flavum
-Epidural space
- Dura mater
-Arachnoid materParamedian or Lateral Approach
-Same as midline excluding supraspinous
& interspinous ligaments
-
8/14/2019 Local Anesthetics 5
101/117
101
Section 3 Caudal anesthesia (Learn by yourself)
References(video)
-
8/14/2019 Local Anesthetics 5
102/117
102
http://v.blog.sohu.com/u/vw/318279
http://v.blog.sohu.com/u/vw/289724
http://v.blog.sohu.com/u/vw/877237
http://v.blog.sohu.com/u/vw/1627820
( )
http://v.blog.sohu.com/u/vw/318279http://v.blog.sohu.com/u/vw/289724http://v.blog.sohu.com/u/vw/877237http://v.blog.sohu.com/u/vw/1627820http://v.blog.sohu.com/u/vw/1627820http://v.blog.sohu.com/u/vw/877237http://v.blog.sohu.com/u/vw/289724http://v.blog.sohu.com/u/vw/318279 -
8/14/2019 Local Anesthetics 5
103/117
Peripheral nervesare classified according to size and function
-
8/14/2019 Local Anesthetics 5
104/117
104
-
8/14/2019 Local Anesthetics 5
105/117
105
a. Sympathetic block with peripheral vasodilation
and skin temperature elevation.
b. Loss of pain and temperature sensation.c. Loss of proprioception.
d. Loss of touch and pressure sensation.
e. Motor paralysis.
Neural blockade of peripheral nerves
usually progresses in the following order:
Pathophysiologic factors
-
8/14/2019 Local Anesthetics 5
106/117
106
p y g
a. A decrease in cardiac outputreduces the volume of distribution and plasma clearance
of local anesthetics, increasing plasma concentration and
the potential for toxicity.
b. Severe hepatic diseasemay prolong the durationof action of amino amides.
c.Renal diseasehas minimal effect.d. Patients withreduced cholinesterase activity
(newborns and pregnant patients) and patients withatypical
cholinesterasemay have an increased potential for toxicity.
e.Fetal acidosismay result in greater transplacental transferand trapping of local anesthetics from mother to her fetus and
thus may have an increased potential for fetal toxicity.
Spine Landmarks/Positions
(Fetal Sitting Prone)
-
8/14/2019 Local Anesthetics 5
107/117
107
(Fetal, Sitting, Prone)
-
8/14/2019 Local Anesthetics 5
108/117
108
Sitting Position
Advantages:Advantages:
Ease of placementEase of placement
Disadvantages:Disadvantages:
VasovagalVasovagalOnset w/ hypo orOnset w/ hypo or
hyperbarichyperbaric
SedationSedation
-
8/14/2019 Local Anesthetics 5
109/117
109
Landmarks
L1 End of cordL1 End of cord
S2 End of duraS2 End of dura
-
8/14/2019 Local Anesthetics 5
110/117
110
-
8/14/2019 Local Anesthetics 5
111/117
111
Reverse Trendelenburg Position
-
8/14/2019 Local Anesthetics 5
112/117
112
steep Trendelenburg position
-
8/14/2019 Local Anesthetics 5
113/117
113
-
8/14/2019 Local Anesthetics 5
114/117
114
-
8/14/2019 Local Anesthetics 5
115/117
115
-
8/14/2019 Local Anesthetics 5
116/117
116
-
8/14/2019 Local Anesthetics 5
117/117