Mini implant in orthodontics - canine and incisor retraction

ORIGINAL ARTICLE
Load system of segmental T-loops for canineretraction
Zeyang Xia,a Jie Chen,b Feifei Jiangc,c Shuning Li,c Rodrigo F. Viecilli,d and Sean Y. Liue
Hong Kong, China, Indianapolis, Ind, and New York, NY
aAssoAcadebProfety-PuOral FcPhDdue UdAssisUniveeAssisana UAll auPotenSuppoReprinDeparPurduIN 46Subm0889-Copyrhttp:/
548
Introduction: The orthodontic load system, especially ideal moment-to-force ratios, is the commonly useddesign parameter of segmental T-loops for canine retraction. However, the load system, including moment-to-force ratios, can be affected by the changes in canine angulations and interbracket distances. Wehypothesized that clinical changes in canine position and angulation during canine retraction will significantlyaffect the load system delivered to the tooth.Methods: The load systems of 2 T-loop groups, one for translationand the other for controlled tipping, from 9 bilateral canine retraction patients were made to the targeted valuesobtained from finite element analyses and validated. Each loop was tested on the correspondingmaxillary dentalcast obtained in the clinic. The casts were made before and after each treatment interval so that both initial andresidual load systems could be obtained. The pretreatment and posttreatment interbracket distances wererecorded for calculating interbracket distance changes. Results: As the interbracket distances decreased,the average retraction-force drop per interbracket distance reduction was 36 cN/mm, a 30% drop per 1 mm ofinterbracket distance decrease. The average antitipping-moment drops per interbracket distance reductionswere 0.02 N-mm per millimeter for controlled tipping and 1.4 N-mm per millimeter for translation, about 0.6%and 17% drops per 1 mm of interbracket decrease, respectively. Consequently, the average moment-to-forceratio increases per 1 mm of interbracket distance reduction were 1.24 mm per millimeter for controlled tippingand 6.34 mm per millimeter for translation. There was a significant residual load, which could continue tomove the tooth if the patient missed the next-scheduled appointment. Conclusions: Clinical changes in canineposition and angulation during canine retraction significantly affect the load system. The initial planned moment-to-force ratio needs to be lower to reach the expected average ideal value. Patients should be required to followthe office visit schedule closely to prevent negative effects because of significant moment-to-force ratiosincreases with time. (Am J Orthod Dentofacial Orthop 2013;144:548-56)
Segmental T-loops are used in maxillary canineretraction. The resulting orthodontic load (forceand moment) system on the canine is affected
ciate professor, Shenzhen Institutes of Advanced Technology, Chinesemy of Sciences and Chinese University of Hong Kong.ssor and chair, Department of Mechanical Engineering, Indiana Universi-rdue University, Indianapolis; professor, Department of Orthodontics andacial Genetics, Indiana University, Indianapolis.student, Department of Mechanical Engineering, Indiana University-Pur-niversity, Indianapolis.tant professor, Department of Orthodontics, College of Dentistry, New Yorkrsity, New York.tant professor, Department of Orthodontics and Oral Facial Genetics, Indi-niversity, Indianapolis.thors have completed and submitted the ICMJE Form for Disclosure oftial Conflicts of Interest, and none were reported.rted by the NIH/NIDCR under grant number 1R01DE018668.t requests to: Jie Chen, Department of Mechanical Engineering andtment of Orthodontics and Oral Facial Genetics, Indiana University-e University Indianapolis, 723 W Michigan St, SL260, Indianapolis,202; e-mail, [email protected], January 2013; revised and accepted, May 2013.5406/$36.00ight � 2013 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2013.05.007
by multiple factors, including changes in interbracketdistance and tooth angulations.1-3 However, thechanges in the clinical load system that occursimultaneously with canine movement have not beenquantified. Different load systems, especially smalldifferences in moment-to-force ratios (M/F), result indifferent tooth movement patterns: tipping or transla-tion.4,5 It is important to quantify the load changes forpredicting the treatment effects and preventingpotential side effects. We hypothesized that clinicalchanges in canine position and angulation duringcanine retraction will significantly affect the loadsystem delivered to the tooth.
An orthodontic load system is 3 dimensional (3D) andconsists of 3 force and 3 moment components. It is diffi-cult to measure the entire 3D orthodontic load systemclinically. Therefore, it has been investigated primarily inlaboratory settings by using archwires placed on dentalcasts6-8; numeric estimations, such as the Loopsimulation software (dHAL Software, Kifissia, Greece)9-12; or the finite element method.13,14 Viecilli12 simulated

Xia et al 549
the effect of changes of the canine position and angula-tion on the M/F. The study was 2-dimensional and basedon ideal rotation. Despite the clinically applicable infor-mation acquired, these studies were mostly conductedon ideal dentures, and the changes of the load systemsof individual patients during tooth movement have notbeen considered.
To better understand how the load system affectstooth movement clinically, the load components andtheir changes during clinical treatment need to be quan-tified. The objectives of this study were to monitor theclinical load systems on the canines undergoing retrac-tion and to quantify the effects of the movement patternon the load components.
MATERIAL AND METHODS
Customized segmental T-loops were designed andfabricated to retract the canines with tipping or transla-tion. Measurements of force and moment components,and the M/F, were made by using models obtainedfrom the patient at different times, with a custom-made orthodontic force tester. Interbracket distancesand the initial and residual load components beforeand after canine retraction were quantified to investigatechanges of the load system during canine retraction.
After approval by the institutional review board of In-diana University, 9 patients consented for this study. Theinclusion criteria were (1) need for extraction of bothmaxillary first premolars and (2) a possible indicationfor maxillary canine retraction during treatment. Theaverage age of these patients was about 21 years (range,14-47 years). The maxillary first premolars were ex-tracted, and the maxillary dental arch including the sec-ond molars was bracketed, leveled, and aligned withsequential archwires. Before canine retraction, a 0.0193 0.025-in stainless steel archwire was fully engagedin brackets with 0.022 3 0.028-in slots. The maxillarysecond premolar, first molar, and second molar werecoligated with a 0.010-in stainless steel wire, connectedwith a transpalatal arch to establish a posterior unit.
For each patient, the right and left canines wererandomly assigned to receive controlled tipping or trans-lation orthodontic tooth movements. To accomplishcontrolled tipping or translation, 2 segmental T-loops,made of 0.017 3 0.025-in TMA wire (Ormco, Glendora,Calif), were designed and fabricated to deliver differentM/F to retract the canines. The T-loops on both sideswere designed to deliver 124 cN of retraction force.15
The desired M/F for controlled tipping and translationwere calculated by using finite element models of thepatients, constructed based on cone-beam computedtomography. The maxillary image was taken before the
American Journal of Orthodontics and Dentofacial Orthoped
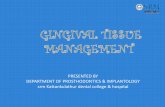
canine retraction using an i-CAT device (Imaging Sci-ences International, Hatfield, Pa) at the resolution of0.25-mm voxel size with a scanning time of 27 seconds.For each patient, the raw image data of the cone-beamcomputed tomography scan were processed usingMIMICS software (Materialise, Leuven, Belgium) tocreate a reconstructed digital model of the teeth, peri-odontal ligament, and maxillary bone complex. A finiteelement model was created from the digital model andthen imported into ANSYS software (Canonsburg, Pa)to compute the tooth displacement from an orthodonticload. The load consisted of the retraction force and acouple (moment), which were applied at the bracket(Fig 1). The resulting tooth displacement pattern wascalculated. The moment was then incrementallyincreased. The moment and force pairs that create trans-lation and controlled tipping were identified. The detailsof the modeling were reported previously.16 Mx/Fy wasused to control the distal tipping. The average desiredamounts of Mx/Fy of the 9 patients were 7.7 mm forcontrolled tipping and 10.4 mm for translation.
The interbracket distance was defined as the distancefrom the mesial aspect of the auxiliary tube of the firstmolar bracket to the distal aspect of the canine bracket.This was expected to decrease during canine retraction;with it, there would be more decrease in force thanmoment, resulting in an increase of the M/F. For thisreason, measures for initial M/F adjustment needed tobe conducted. The M/F increase in the retraction planeper 1 mm of interbracket distance reduction was esti-mated using the Loop simulation software. An approxi-mately 50% increase in the M/F was estimated per 1 mmof interbracket distance reduction from this analysis. Inthis study, each treatment period was defined as whena canine was retracted more than 1 mm, measured dur-ing each office visit. The interbracket distance changeswere expected to vary significantly because of variationsin treatment time periods caused by scheduling-relatedissues. Thus, the total increase of M/F could only beestimated; it was set at 70%. To be consistent, the calcu-lated M/F for translation was decreased by approxi-mately 35% (half of the estimated total M/F increase)to ensure that the average M/F during the treatmentperiod was close to the ideal value. The M/F for tippingwas further discounted to enhance the tipping effects. Inaddition, to prevent mesial out rotation caused by theretraction force, the desired antirotation moment fortranslating the tooth was also calculated with the samefinite element model. Mz/Fy was used to control thetooth rotation. To ensure that the average Mz/Fy wasclose to the desired value, the implemented initial Mz/Fy was reduced by approximately 35% on both caninesto compensate for the effects of interbracket distance
ics October 2013 � Vol 144 � Issue 4

Fig 1. The finite element model of a canine-periodontalligament-bone complex for estimating the M/F requiredto translate or tip the canine. A force, F, and a couple,C, were applied at the location of the tube on the bracket.The resulting tooth displacement was calculated. The Fand C pairs that produced translation and controlledtipping were selected.
550 Xia et al
reduction. However, the target Mz/Fy was difficult toachieve because it was primarily realized by adjustingthe first-order gable angles. Large gable angles wererequired in many patients; they caused the T-loop tointerfere with the cheek or gum. To prevent interference,only smaller gable angles could be used; they caused Mz
to be lower than the target value. The main focus of thisstudy was on translation and tipping. Control of Mz wasconsidered secondary and thus was allowed to becompromised in some subjects. Other load componentswere kept minimal when the T-loops were produced.
According to the desired load system, the T-loopswere bent to express the desired force and moment com-ponents. These components were calibrated experimen-tally on the corresponding dental casts. The casts wereprepared using the following protocol. Over the periodof canine retraction, the patients were seen every 5 to6 weeks. A decision was made on whether a treatmentinterval was completed. A treatment interval was defined
October 2013 � Vol 144 � Issue 4 American
when 1 canine moved more than 1 mm. Thus, multipleintervals might occur for each patient because allpatients in this study had more than 3 mm of spacebetween the canine and the second premolar. However,the number of intervals varied among the patientsbecause of the differences in tooth movement ratesand durations between office visits. When an intervalwas completed, an impression was made, the T-loopwas retrieved, and a new T-loop was designed andapplied. Then the next treatment interval began. Thecasts were made before and after each interval. At thebeginning of each treatment interval, each T-loop wasadjusted on the corresponding duplicate acrylic modelattached to a custom-made orthodontic force tester toensure delivering accurate loads.6 An impression of themaxillary dental arch was made by injecting light andmedium polyvinylsiloxane material (Examix NDS; GC,Tokyo, Japan) over the brackets, followed by an alginateimpression. Duplicate canine and first molar bracketswith tubes (Burstone; Ormco) were placed in the polyvi-nylsiloxane, and autopolymerizing acrylics (RepairMaterial; Dentsply, York, Pa) were packed into theimpression and allowed to cure. The acrylic model wasattached to the orthodontic force tester with 2 screws.The target teeth (canines) were attached to the load cellswith epoxy adhesive (Loctite E-120HP Hysol; Henkel,Rocky Hill, Conn) and then were completely separatedfrom the acrylic model, thus maintaining their originalpositions and orientations (Fig 2).
After we measured the initial interbracket distancesbetween the canine andmolar tubes of the acrylic model,we made a T-loop with the geometry shown in Figure 3.The size, shape, leg length, and dimensions of theT-loops were determined by considering their effectson the load system, as well as preventing interferenceswith the cheek and gum.2 The first-order and second-order gable bends were added symmetrically to theT-loops to bring the load components to the targets(Fig 4). The loop bending and adjustment process wasiterated until the desired force and moments were accu-rately expressed. The horizontal leg was bent on eachend of the T-loop to allow easy insertion into the tube.The method also ensured that the interbracket distancewas identical when transferred the orthodontic forcetester validated T-loop to the patient (Fig 5). The valida-tion was performed on the orthodontic force tester. T-loops were installed on the duplicate acrylic modelattached to the orthodontic force tester for testing forceand moment components. The orthodontic force testerwas designed to measure the orthodontic load systemat the canine bracket (Fig 2,A). Two load cells (Multiaxisforce/torque Nano17; ATI Industrial Automation, Apex,NC) were used to measure the 6 force and moment
Journal of Orthodontics and Dentofacial Orthopedics

Fig 3. The geometry and dimensions of the loops beforethe first- and second-order bends were added.
Fig 4. The fabricated T-loops.
Fig 5. A canine retraction patient with the T-loop on theleft side.
Fig 2. A, The laboratory setting for measuring the ortho-dontic load system on the canines. The setting includesan orthodontic force tester, a dental cast with brackets,and the T-loops. The coordinate systems on B, the leftside and C, the right side were defined at the centers ofthe canine brackets.
Xia et al 551
components applied at the canine brackets. The forcerange of each load cell was 0 to 20 N, with a 0.025-N res-olution, and the moment range was 0 to 100 N-mmwitha 0.003 N-mm resolution. A local coordinate system wasestablished on each left canine with the retraction direc-tion aligned with the load cell's positive y-axis, thebuccal direction with the positive x-axis, and thegingival direction with the positive z-axis (Fig 2, B).The local coordinate system on the right canine was
American Journal of Orthodontics and Dentofacial Orthoped
different from that of the left canine (Fig 2, A and B).In this study, the clinically expressed load systems wereof interest, and the side was not a controlled parameterbecause tipping or translation was randomly assigned toeach side. Thus, the clinically used coordinate system onthe left side was used to describe the results.
For each treatment interval, an acrylic model wasfabricated after each treatment period, and a newT-loop was bent for each canine and adjusted usingthe orthodontic force tester. The posttreatment inter-bracket distances were also recorded. The T-loops usedin the previous treatment were retrieved and installedon the posttreatment acrylic model to measure the resid-ual load system with the orthodontic force tester. TheT-loops retrieved were examined visually for signs ofpermanent deformation or other damage from removal.Damaged T-loops were excluded from this study. Conse-quently, both initial and residual load systems wererecorded.
Statistical analysis
Linear regressions were performed on the retractionforce, Fy, drop, antitipping moment, Mx, drop, and Mx/
ics October 2013 � Vol 144 � Issue 4

Table I. Results from the 10 tests to estimate errorsfrom T-loop installation and instrument
Test Fx (N) Fy (N) Fz (N) Tx (N-mm) Ty (N-mm) Tz (N-mm)1 �0.28 1.16 0.21 �6.95 �3.32 �5.102 �0.29 1.18 0.23 �6.93 �3.29 �4.883 �0.29 1.19 0.25 �6.81 �3.22 �4.774 �0.30 1.17 0.26 �6.70 �3.54 �4.635 �0.29 1.17 0.25 �6.80 �3.49 �4.676 �0.30 1.14 0.23 �6.92 �3.56 �4.647 �0.28 1.17 0.23 �6.86 �3.23 �4.908 �0.28 1.17 0.25 �6.70 �3.47 �4.709 �0.29 1.15 0.25 �6.78 �3.47 �4.71
10 �0.28 1.17 0.26 �6.66 �3.41 �4.74Mean �0.29 1.17 0.24 �6.81 �3.40 �4.77SD 0.01 0.01 0.02 0.10 0.12 0.15
T, Moment component.
552 Xia et al
Fy increase with respect to interbracket distancechanges. The initial and residual load systems werecompared using paired t tests. The force and momentdrops between the controlled tipping and translationgroups were compared using a t test. Significance wastested at the 95% confidence level.
To assess the errors from wire installation and instru-ment, a cast and a T-loop were used for a repeatabilitytest. The same T-loop was installed on the same cast10 times. The resulting load system corresponding toeach installation was measured. The means and standarddeviations were calculated.
RESULTS
The installation and instrument errors of the 6 loadcomponents are shown in Table I. The maximum stan-dard deviations for the key load components, Fy, Mx,and Mz, were only 1%, 1%, and 3%, respectively, mean-ing that the measurements were consistent.
Only 9 T-loops on the controlled tipping side and 11on the translation side passed the visual inspections. Theinitial interbracket distances in this study ranged from16.4 to 24.4 mm because of interpersonal difference orvariations in incremental tooth displacement. The inter-bracket distance decrease in each treatment intervalranged from 0.3 to 1.9 mm (average, 1.23 mm). Despitethe 1-mm canine movement criterion for the treatmentinterval, there were intervals with greater canine move-ments, causing larger interbracket distance decreases.The larger decrease was primarily due to prolongedtreatment intervals caused by missed appointments.The initial and residual load systems were measured(Table II). The load systems on both sides were expressedusing the same convention. The positive y-axis corre-sponded to the retraction (distal) direction, the positivex-axis represented the buccal direction, and the positivez-axis corresponded to the gingival direction. The posi-tive Mx tips the crown distally, the positive My tips thecrown lingually, and the positive Mz rotates the crowndistal in. Thus, negative Mx is the antitipping moment.The initial retraction force, Fy, was 124.4 6 3.3 cN. Onthe retraction plane, the initial antitipping moments,Mx, were �780 6 0.8 cN-mm for translation and�340 6 1.1 cN-mm for controlled tipping. Conse-quently, the initial Mx/Fy amounts were �6.3 6 0.8mm for translation and �2.8 6 0.9 mm for controlledtipping after we implemented the M/F discountsdescribed previously. The Mz/Fy was not reportedbecause Mz was compromised to prevent interferencewith the cheek and gum.
The load systems between the 2 groups werecompared first. Statistically, there was no significant
October 2013 � Vol 144 � Issue 4 American
difference in the force drops (P 5 0.4046), but therewas a significant difference (P 5 0.02037) in momentdrops between the controlled tipping and translationgroups. The retraction forces dropped to 58.5 6 20.6cN (residual force) on the controlled tipping side and55.6 6 26.6 cN on the translation side at the end ofeach treatment interval. The average initial antitippingmoment, Mx, drop on the controlled tipping side was140 6 130 cN-mm, which decreased to �200 cN-mm(residual moment); on the translation side, it was 2506 150 cN-mm, which dropped to�530 cN-mm. Conse-quently, the average Mx/Fy drop on the controlledtipping side was 1.1 6 2.3 mm; on the translationside, it was 4.0 6 3.6 mm. In the other directions, likethe retraction force, the initial load components werethe same; thus, the data of the 2 groups were combined.The buccolingual force, Fx, changed from �5.6 6 17.5cN (lingual) to 96 24.9 cN (buccal); the occlusogingivalforce, Fz, changed from 4.76 11.9 cN to 3.46 17.9 cN(intrusion); the antitipping moment, My, in the bucco-lingual direction, changed from 60 6 180 N-mm to 506 180 cN-mm (lingual tipping); and the antirotationmoment, Mz, changed from �580 6 190 cN-mm to�520 6 240 cN-mm (crown mesial in).
The retraction forces, Fy, were decreased as theinterbracket distance was reduced because of canineretraction. Figure 6 shows the interbracket distancereduction vs force drop of each loop. The linear regres-sions of force drop vs the interbracket distance changefor the 2 groups were estimated as Fy drop (cN) 535.3 1 26.7 3 interbracket distance reduction (mm)for controlled tipping, and Fy drop (cN) 5 14.9 1 44.93 interbracket distance reduction (mm) for translation.
The average amounts of retraction force drop per in-terbracket distance reduction were 26.7 cN/mm on thecontrolled tipping side and 44.9 cN/mm on the
Journal of Orthodontics and Dentofacial Orthopedics

Table II. Means and standard deviations of the load components on the controlled tipping (CT) side, the translation(TR) side, and both sides combined
Status Fx (cN) Fy (cN) Fz (cN) Mx (cN-mm) My (cN-mm) Mz (cN-mm) Mx/Fy (mm)Initial
CT Mean �1.22 123.00 2.67 �340 81 �519 �2.74SD 15.64 2.35 16.12 110 112 202 0.91
ResidualMean 9.11 57.33 6.22 �203 �3 �490 �3.81SD 31.70 22.56 19.80 120 157 211 2.62
InitialTR Mean �9.09 125.55 6.36 �779 043 �629 �6.22
SD 18.90 3.67 7.34 81 218 166 0.78Residual
Mean 8.91 52.09 1.00 �522 86 �551 �11.11SD 19.31 24.68 16.80 157 195 274 3.61
InitialCombined Mean �5.55 124.40 4.70 �582 60 �580 �4.66
SD 17.53 3.33 11.89 242 175 187 1.95Residual
Mean 9.00 54.45 3.35 �379 46 �524 �7.83SD 24.89 23.28 17.91 213 180 243 4.86
A
B
Fig 6. Interbracket distance decrease vs force drop ofeach loop: A, on the controlled tipping (CT) side; B, onthe translation (TR) side.
Xia et al 553
translation side, meaning that after 1 mm of interbracketdistance decrease, the retraction force has dropped by20% on the tipping side and by 36% on the translationside from the initial values (P\0.0001). The coefficients
American Journal of Orthodontics and Dentofacial Orthoped
of determination (R2) were 0.3714 and 0.5575. This co-efficient is between 0 and 1; the higher the value, thestronger the correlation.
Similarly, the antitipping moment, Mx, was alsoreduced with decreasing interbracket distances (Fig 7).The linear regressions of antimoment drops vs inter-bracket distance reductions were expressed as Mx drop(cN-mm)5 1341 2.13 interbracket distance reduction(mm) for controlled tipping, and Mx drop (cN-mm) 572 1 144 3 interbracket distance reduction (mm) fortranslation.
The coefficients of determination were R2 5 0 forcontrolled tipping and 0.1899 for translation. Theaverage antitipping moment drops per 1 mm of inter-bracket distance decrease were about 2 cN-mm per milli-meter for controlled tipping and 144 cN-mm permillimeter for translation, an 18% drop per 1 mm ofinterbracket distance decrease.
In contrast, the Mx/Fy ratio increased with the reduc-tion in interbracket distance (Fig 8). The linear regres-sions of antimoment drop vs interbracket distancereduction were expressed as Mx/Fy increase (mm) 5�0.35 1 1.25 3 interbracket distance reduction (mm)for controlled tipping, and Mx/Fy increase (mm) 5�3.33 1 6.34 3 interbracket distance reduction (mm)for translation.
The coefficients of determination were R2 5 0.063and 0.4836, respectively. The average M/F increasesper interbracket distance decrease were 1.25 mm permillimeter for controlled tipping and 6.34 mm per milli-meter for translation.
ics October 2013 � Vol 144 � Issue 4

A
B
Fig 7. Interbracket distance decrease vs moment drop ofeach loop:A, on the controlled tipping (CT) side;B, on thetranslation (TR) side.
A
B
Fig 8. Interbracket decrease vs M/F increase of eachloop: A, on the controlled tipping (CT) side; B, on thetranslation (TR) side.
554 Xia et al
DISCUSSION
In this clinical study, we quantified the orthodonticload system of a T-loop segmental wire for canineretraction and its residual load system as a function ofinterbracket distance reduction from canine movement.Our in-vitro “transfer” method, simulating the clinicalcondition, provides the best estimates at present onthe clinical load systems because it preserves the bound-ary conditions that occur in the clinic; these are thedominating factors affecting accuracy.6 The effects ofa bracket's translation and rotation in all 3 directionswere considered; this has never been done before.Although these results are limited to this type ofT-loop, they have a broader implication because theyexpress changes that could occur with loops with dimen-sions and activations calibrated to deliver similar loadsystems.17
The load systems on the canines were controlled andquantified, with the same retraction force and differentantitipping moments in the retraction plane for eithercontrolled tipping or translation. There were no signifi-cant differences in retraction force, Fy, drop vs inter-bracket distance decrease between the controlledtipping and the translation groups. Thus, the Fy data
October 2013 � Vol 144 � Issue 4 American
were combined for further analyses. The average retrac-tion force drop per interbracket distance decrease was36 cN/mm, a 30% drop per 1 mm of interbracket dis-tance decrease (P \0.0001). The antitipping moment,Mx, drop vs the interbracket distance decrease wassignificantly different between the 2 groups, most likelybecause the initial moments were different. The rate ofMx drop per interbracket distance change was higherfor translation than for controlled tipping. Translationrequires a higher moment, which indicates that the Mx
drop depends on the initial moment level. The higherthe initial moment, the faster it drops. When the initialmoment is low, there is a negligible moment drop (Fig 7).
Canine retraction causes both retraction force, Fy,and antitipping moment, Mx, to drop (Figs 6 and 7). In-terbracket distance is directly related to canine retractionbut is not the only dominant factor affecting the forceand moment drops. The coefficient of determinationof regression analysis on interbracket distance reductionvs force drop indicated some relationship between inter-bracket distance and force drop. The coefficient of deter-mination indicated the amount of variability in forcedrop explained by the interbracket distance decrease.
Journal of Orthodontics and Dentofacial Orthopedics

Xia et al 555
The coefficient of determination for moment drop vsinterbracket distance decrease on the translation sidewas only 0.1899, meaning that interbracket distancedecrease explains only 18% of the variability in momentdrop. Theoretically, if the displacement only occurs inthe retraction plane and there is no bracket angulationchange due to tipping, the M/F change should have littlevariation, and the coefficient of determination shouldbe high. However, in the clinic, the canine moves in 3 di-mensions; this causes the bracket to rotate about all 3axes. Consequently, other factors, such as bracket angu-lation, also contribute to the moment change, whichcreates the significant scattering of the data shown inFigure 7.
In this clinical study, there were large initial and re-sidual out-of-retraction-plane load components, suchas Fx, My, and Mz, shown in Table I; these might initiateout-of-retraction-plane displacements and affect finaltooth positions, including bracket angulations. Theseinitial out-of-retraction-plane load components aredifficult to eliminate for T-loop designs. The values arenot trivial and thus need to be considered. To under-stand their effects on the load component drops, the 6components of clinical displacement should be furtherstudied.
Ideally, the load drops are expressed with the 3Dtooth displacement, which includes angulation changesmeasured from the tooth's tipping and rotation. This en-sures that coupling effects of angulation changes in 3directions are considered; this reflects the clinical reality.Previous studies measured 2-dimensional distal tippingangles from radiography and input the angles into com-puter models to calculate the residual load.18,19 Theresidual load was under ideal boundary conditions,and the effects of angulations in the other 2 directionswere not included. Although the results were moreconsistent, they might not accurately represent realityand did not reflect interpersonal variations. Thus, theresults can be used only qualitatively. These issueswere addressed in this study. However, the 3Ddisplacement components are hard to measureclinically and difficult to present. Only interbracketdistance is directly measurable clinically; thus, it wasused in this study.
Our results showed that as the canine retracted,both retraction force and antitipping momentdecreased at different rates. The load drop was signif-icant (30% reduction per 1 mm of interbracket dis-tance loss) and faster than the antitipping moment(0.6% and 18% reductions per 1 mm of interbracketdistance loss for controlled tipping and translation,respectively). These differential drops between loadand antitipping moment increase the M/F. Our results
American Journal of Orthodontics and Dentofacial Orthoped
support previous findings that the antitippingmoment, Mx, is less affected by the interbracket dis-tance change than the retraction force, although theincreasing rate is different because of different T-loop designs.17 The tooth displacement pattern relieson the M/F. When a T-loop designed for translationis used, prolonged treatment caused by missed ap-pointments will continue to increase the M/F, meaningthat a relatively stronger antitipping moment than isneeded for translation is applied. If this reaches a crit-ical level, it can cause canine crown tipping in themesial direction. Unless this is a desired tooth move-ment, the patient should be strongly advised to keepthe scheduled office visits and have the T-loopadjusted close to the scheduled time. On the otherhand, if a higher antitipping moment is needed butis not achievable clinically, having longer intervals be-tween visits might achieve the desired M/F for transla-tion as long as the residual retraction force is stilleffective.
Current theory requires that certain M/F to bemaintained to either translate or tip the canine, de-pending on the treatment strategy. This is difficult toachieve for a segmental T-loop because the M/Fchanges as the tooth moves. Our results show the levelof changes, which are significant enough to make aclinical impact. To ensure that the average M/F is closeto the desired value, the initial M/F should be reduceddepending on the expected tooth displacement in eachtreatment period. If the expected tooth displacement is1 mm, then the initial M/F for translation should beabout 3 mm less than the expected value becausethe M/F drop is about 6 mm per 1 mm of interbracketdistance reduction. The greater the expected toothmovement, the greater the M/F reduction that isneeded.
The initial retraction force should not be too low. It iscommonly accepted that there is an effective force levelfor moving a tooth, although there is no consensus onthe actual level. An initial force less than 36 cN woulddrop below zero when the canine retracts more than 1mm; this would have no retraction effect. On the otherhand, if the initial load is as high as 124 cN, as in ourcase, the retraction force would still be greater thanthe effective force level after the predetermined treat-ment period; thus, the tooth would still move if thepatient misses appointments. This force combined withthe slower dropped antitipping moment would causeM/F to increase and exceed the value for translation,causing tipping in the protraction direction, a side effectto avoid. Therefore, clinicians might want to considerthis when determining the initial force level and sched-uling the office visits.
ics October 2013 � Vol 144 � Issue 4

556 Xia et al
CONCLUSIONS
A 3D approach to calibration of customizedsegmental T-loops with desired loadings and measure-ments of the change of loadings was developed and vali-dated in a canine retraction clinical study. The followingconclusions were made.
1. Clinical changes in canine position during canineretraction can significantly affect the load systemdelivered to the tooth.
2. In canine retraction, the retraction force decreasesfaster than the antitipping moment; this results inan M/F increase.
3. Out-of-retraction-plane load components exist andchange, and they will affect out-of-retraction-planemovement.
4. The initial M/F needs to be lower than the targetedvalue to reach the expected effect. The reductioncan be approximately half of the expected M/Fincrease during the treatment interval.
5. The initial force needs to be higher to ensure thatthe residual force is effective during the treatmentperiod. The value depends on the force dropcorresponding to the level of expected toothmovement.
REFERENCES
1. Burstone C. The segmented arch approach to space closure. AmJ Orthod 1982;82:361-78.
2. Burstone C, Koenig H. Optimizing anterior and canine retraction.Am J Orthod 1976;70:1-19.
3. Proffit W. Contemporary orthodontics. St Louis: Mosby; 2000. p.340-61.
4. Burstone CJ, Pryputniewicz RJ. Holographic determination ofcenters of rotation produced by orthodontic forces. Am J Orthod1980;77:396-409.
October 2013 � Vol 144 � Issue 4 American
5. Gjessing P. Controlled retraction of maxillary incisors. Am J OrthodDentofacial Orthop 1992;101:120-31.
6. Chen J, Isikbay SC, Brizendine EJ. Quantification of three-dimensional orthodontic force systems of T-loop archwires. AngleOrthod 2010;80:754-8.
7. Gajda S, Chen J. Comparison of three-dimensional orthodonticload systems of different commercial archwires for space closure.Angle Orthod 2012;82:333-9.
8. Katona T, Le Y, Chen J. The effects of first- and second-order gablebends on forces and moments generated by triangular loops. AmJ Orthod Dentofacial Orthop 2006;129:54-9.
9. Halazonetis D. Design and test orthodontic loops using yourcomputer. Am J Orthod Dentofacial Orthop 1997;111:346-8.
10. Martins R, Buschang P, Martins L, Gandini LJ. Optimizing thedesign of preactivated titanium T-loop springs with Loop soft-ware. Am J Orthod Dentofacial Orthop 2008;134:161-6.
11. Raboud D, Faulkner M, Lipsett A, Haberstock D. Three dimensionaleffects in retraction appliance design. Am J Orthod DentofacialOrthop 1997;112:378-92.
12. Viecilli R. Self-corrective T-loop design for differential spaceclosure. Am J Orthod Dentofacial Orthop 2006;129:48-53.
13. Coimbra ME, Penedo ND, de Gouvea JP, Elias C, de SouzaAr�ujo MT, Coelho PG. Mechanical testing and finite element anal-ysis of orthodontic teardrop loop. Am J Orthod Dentofacial Orthop2008;188.e9-13.
14. Haskell B, Spencer W, Day M. Auxiliary springs in continuous archtreatment: part 1. An analytical study employing thefinite-elementmethod. Am J Orthod Dentofacial Orthop 1990;98:387-97.
15. Viecilli RF, Katona TR, Chen J, Hartsfield JK Jr, Roberts WE. Ortho-donticmechanotransduction and the role of the P2X7 receptor. AmJOrthod Dentofacial Orthop 2009;135:694.e1-16:discussion, 694-5.
16. Meyer BN, Chen J, Katona TR. Does the center of resistance dependon the direction of tooth movement? Am J Orthod DentofacialOrthop 2010;137:354-61.
17. Chen J, MarkhamDL, Katona TR. Effects of T-loop geometry on itsforces and moments. Angle Orthod 2000;70:48-51.
18. Kuhlberg AJ, Priebe D. Testing force systems and biomechanics—measured tooth movements from differential moment closingloops. Angle Orthod 2003;73:270-80.
19. Martins RP, Buschang PH, Gandini LG Jr. Group A T-loop fordifferential moment mechanics: an implant study. Am J OrthodDentofacial Orthop 2009;135:182-9.
Journal of Orthodontics and Dentofacial Orthopedics