Liver lift: A simple suture technique for liver retraction during laparoscopic gastric surgery
3
Journal of Surgical Oncology 2007;95:83–85 HOW I DO IT Liver Lift: A Simple Suture Technique for Liver Retraction During Laparoscopic Gastric Surgery JUN HO LEE, MD, KEUN WON RYU, MD,* YOUNG WOO DOH, MD, JA SEONG BAE, MD, YOUNG WOO KIM, MD, AND JAE-MOON BAE, MD Gastric Cancer Branch, National Cancer Center, Goyang, Korea KEY WORDS: gastric cancer; laparoscope; liver retraction INTRODUCTION Minimally invasive, laparoscopically assisted surgery remains a popular surgical practice [1–3]. This approach offers important advantages versus open surgery, that is, reduced intraoperative blood loss, reduced post-operative pain, accelerated recovery, an earlier return to a normal bowel function with earlier oral intake resumption, and early discharge from hospital [4,5]. Although the issue is actively debated, laparoscopic gastrectomy for gastric cancer is becoming increasingly popular, and the laparoscopic approach is proving to be an acceptable alternative to open surgery for colon cancer [1]. One of the technical problems of laparoscopic gastrectomy in obese patients is a thickened fat-laden falciform ligament that hangs down and obscures the field of vision. Thus, laparoscopic surgeons have devised a falciform lift method, which helpfully exposes the hepatoduodenal ligament [6]. However, liver retraction is essential for full visualization of the gastrohepatic ligament near the esophageal hiatus and lesser curvature of stomach during laparoscopic gas- trectomy [7]. We attempted liver lift using a straight needle. This method not only eliminates the abdominal wounding required for another trocar, but also frees an assistant’s hand. In this article, we describe an effective method of liver lift that enables dissection of lymph node stations 1, 3, and 5 during laparoscopic gastric cancer surgery. OPERATIVE TECHNIQUE The early gastric cancer patients included in this study were staged using the following techniques: esophagogastroduodenoscopy, double contrast study of the upper gastrointestine, endoscopic ultrasonography, and contrast-enhanced computed tomography (CT) of the abdomen and pelvis. Transcutaneous ultrasonography was not routinely performed. Laparoscopic-assisted distal gastrectomy (LADG) and laparoscopic-assisted total gastrectomy (LATG) was performed under general anesthesia, as previously described [8]. With a patient lying supine on the table. A 11-mm sized skin incision was made in the supraumbilical or infraumbilical region. After CO 2 pneumoperitoneum was obtained using an open techni- que, an 11-mm trocar was inserted, and used as a camera port. Laparoscopic staging included inspection of the peritoneum, diaphragm, and liver capsule (Fig. 1a). The pelvis was inspected in the Trendelenberg position. Four other trocars were inserted through the abdominal wall, one in the left upper quadrant (5-mm sized trocar; as an assistant’s working port), one in the left lower quadrant (5-mm sized trocar; also as an assistant’s working port), one in the right upper quadrant (5-mm sized trocar; operator’s working port), and one in right lower quadrant (12-mm sized trocar; operator’s working port). A 5-cm long straight needle with a 75-cm long polyprolene thread attached to its proximal end (Prolen 2-0 1 , Ethicon, Somerville, NJ) was inserted at the left side of the xiphoid process, and directed to the patient’s left. The needle was grasped from inside, pulled into the abdominal cavity, and then punctured the left lateral segment of the liver at 1 cm removed from the liver margin. It was then rotated around the falciform ligament, and pushed out of the abdomen through a *Correspondence to: Keun Won Ryu, MD, Gastric Cancer Branch, National Cancer Center, 411-764 809 Madu 1-dong Ilsandong-gu Goyang-si, Gyeonggi-do Korea. Fax: 82-31-920-0069. E-mail: [email protected] Received 26 April 2006; Accepted 22 May 2006 DOI 10.1002/jso.20611 Published online in Wiley InterScience (www.interscience.wiley.com). ß 2006 Wiley-Liss, Inc.
-
Upload
jun-ho-lee -
Category
Documents
-
view
218 -
download
4
Transcript of Liver lift: A simple suture technique for liver retraction during laparoscopic gastric surgery

Journal of Surgical Oncology 2007;95:83–85
HOW I DO IT
Liver Lift: A Simple Suture Technique for LiverRetraction During Laparoscopic Gastric Surgery
JUN HO LEE, MD, KEUN WON RYU, MD,* YOUNG WOO DOH, MD, JA SEONG BAE, MD,YOUNG WOO KIM, MD, AND JAE-MOON BAE, MD
Gastric Cancer Branch, National Cancer Center, Goyang, Korea
KEY WORDS: gastric cancer; laparoscope; liver retraction
INTRODUCTION
Minimally invasive, laparoscopically assisted surgeryremains a popular surgical practice [1–3]. This approachoffers important advantages versus open surgery, that is,reduced intraoperative blood loss, reduced post-operativepain, accelerated recovery, an earlier return to a normalbowel function with earlier oral intake resumption, andearly discharge from hospital [4,5].
Although the issue is actively debated, laparoscopicgastrectomy for gastric cancer is becoming increasinglypopular, and the laparoscopic approach is proving to bean acceptable alternative to open surgery for colon cancer[1]. One of the technical problems of laparoscopicgastrectomy in obese patients is a thickened fat-ladenfalciform ligament that hangs down and obscures thefield of vision. Thus, laparoscopic surgeons havedevised a falciform lift method, which helpfullyexposes the hepatoduodenal ligament [6]. However, liverretraction is essential for full visualization of thegastrohepatic ligament near the esophageal hiatus andlesser curvature of stomach during laparoscopic gas-trectomy [7].
We attempted liver lift using a straight needle. Thismethod not only eliminates the abdominal woundingrequired for another trocar, but also frees an assistant’shand. In this article, we describe an effective method ofliver lift that enables dissection of lymph node stations 1,3, and 5 during laparoscopic gastric cancer surgery.
OPERATIVE TECHNIQUE
The early gastric cancer patients included in thisstudy were staged using the following techniques:esophagogastroduodenoscopy, double contrast study ofthe upper gastrointestine, endoscopic ultrasonography,
and contrast-enhanced computed tomography (CT) of theabdomen and pelvis. Transcutaneous ultrasonographywas not routinely performed.
Laparoscopic-assisted distal gastrectomy (LADG) andlaparoscopic-assisted total gastrectomy (LATG) wasperformed under general anesthesia, as previouslydescribed [8]. With a patient lying supine on the table.A 11-mm sized skin incision was made in thesupraumbilical or infraumbilical region. After CO2
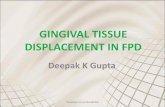
pneumoperitoneum was obtained using an open techni-que, an 11-mm trocar was inserted, and used as a cameraport. Laparoscopic staging included inspection of theperitoneum, diaphragm, and liver capsule (Fig. 1a). Thepelvis was inspected in the Trendelenberg position. Fourother trocars were inserted through the abdominal wall,one in the left upper quadrant (5-mm sized trocar; as anassistant’s working port), one in the left lower quadrant(5-mm sized trocar; also as an assistant’s working port),one in the right upper quadrant (5-mm sized trocar;operator’s working port), and one in right lower quadrant(12-mm sized trocar; operator’s working port).
A 5-cm long straight needle with a 75-cm longpolyprolene thread attached to its proximal end (Prolen2-01, Ethicon, Somerville, NJ) was inserted at the leftside of the xiphoid process, and directed to the patient’sleft. The needle was grasped from inside, pulled into theabdominal cavity, and then punctured the left lateralsegment of the liver at 1 cm removed from the livermargin. It was then rotated around the falciformligament, and pushed out of the abdomen through a
*Correspondence to: Keun Won Ryu, MD, Gastric Cancer Branch, NationalCancer Center, 411-764 809 Madu 1-dong Ilsandong-gu Goyang-si,Gyeonggi-do Korea. Fax: 82-31-920-0069. E-mail: [email protected]
Received 26 April 2006; Accepted 22 May 2006
DOI 10.1002/jso.20611
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2006 Wiley-Liss, Inc.

point adjacent to the right border of its attachment to theanterior abdominal wall, near the xiphoid process. Toprevent potential laceration of the liver by the thread, a freegauge was placed between the liver and thread (Fig. 1b).Both ends of the thread were then pulled and tied.
RESULTS
Five patients with early gastric cancer underwent theliver lift method during LADG and one patient underwentLATG. The patient’s characteristics are described inTable I. Median patient age was 66 years (range 51–76 years); five were male and one female. Median bodymass index of male patients was 23.5 kg/m2 (range 20.3–29.1 kg/m2). Body mass index of the female patient was32.3 kg/m2.
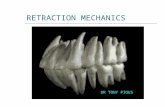
Livers were adequately retracted using the describedstraight needle method and hepatoduodenal and gastro-hepatic ligaments were fully exposed in all five casesfrom the porta hepatis to the esophageal hiatus (Fig. 2).Surgical fields were improved when stomachs werepulled down and leftward with a grasper. No patientneeded an additional trocar for liver retraction to obtain afield of vision along the lesser curvature. Two straightneedles were required in one patient with a BMI of 32.3;one for liver retraction and the other for falciformligament retraction.
The median number of retrieved lymph nodes was 22.5(range 10–32), and lymph node station 1, 3, or 5 were notmissed. The median operating time was 275 min (range227–318 min). Liver retraction took less than 10 min.
Pre-operative aspartate aminotransferase (AST) levelswere within normal limits (<40 IU/L) except in onepatient with 71 IU/L because of a fatty liver. The levelswere not significantly changed on post-operative day 7 inall six patients.
DISCUSSION
Liver lift using a straight needle can be safelyperformed in gastric cancer patients, especially in the
Journal of Surgical Oncology DOI 10.1002/jso
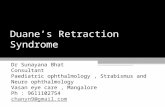
Fig. 1. a: Picture showing status before a liver lift. The gastrohepaticligament was not exposed. b: Picture showing status after liver liftusing a straight needle. Free gauze was placed between the liver andthe thread to prevent potential liver injury. [Color figure can be viewedin the online issue, available at www.interscience.wiley.com.]
TABLE I. Characteristics of Patients
Patients Age Sex BMI Operation Op. timea TNM stage Retrieved LNsbLiver profile
(pre-operativec)
Liver profile
(POD#7d)
1 76 Male 21.2 LADG 227 Ia 28 77/23/7e 59/18/9
2 51 Male 29.1 LADG 315 II 10 78/71/80 117/70/84
3 64 Male 23.1 LADG 245 Ib 20 109/19/14 158/21/12
4 62 Male 23.9 LADG 262 Ia 20 60/20/13 64/20/15
5 69 Male 20.3 LATG 318 Ia 32 81/16/10 58/16/17
6 76 Female 32.3 LADG 282 Ia 25 120/23/18 107/27/20
aOperating time (min).bLymph nodes.cPre-operative.dPost-operative day.eAlkaline phosphatase (IU/L)/aspartate aminotransferase (IU/L)/alanine aminotransferase (IU/L).
84 Lee et al.

obese, with minimal injury. In addition, it is an effectivemeans of exposing the hepatoduodenal ligament, gastro-hepatic ligament, and esophageal hiatus.
Falciform lift is a simple method and in some cases, itallows an elevation of the left lobe of the liver. However,approaches to the lesser curvature and the esophagealhiatus for laparoscopic gastrectomy or laparoscopicfundoplication require another method [7]. To retractthe left lobe of the liver, some surgeons use alaparoscopic retractor or 10-mm wide metacrylic rod[7], and these methods require an additional port and anextra assisting hand. However, the liver lift method usinga straight needle described in this study needs noadditional port or extra assistance, thus minimizingwounding and reducing the surgeon’s workload. Inaddition, upward retraction can be easily enhanced byincreasing thread tension or adding another liverpuncture.
No complication related to this procedure wasexperienced. The liver margin contains no major bile
duct or vessels and the retraction force applied did notdamage the liver during the procedure [9]. Therefore,liver puncture in this region appears to be safe much likethe liver wedge biopsy technique [10]. Moreover, ifbleeding should occur, it can be easily controlled byelectrocoagulation.
The devised technique simply and efficiently facili-tated access to lymph node station 1, 3, and 5, and wellsubstitutes conventional retraction methods thatrequire laparoscopic retractors and therefore anotherport. This technique may be helpful not only inlaparoscopic gastrectomy, but also in approaches to theesophageal hiatus during, for example, laparoscopicfundoplication.
REFERENCES
1. Clinical Outcomes of Surgical Therapy Study Group: Acomparison of laparoscopically assisted and open colectomy forcolon cancer. N Engl J Med 2004;350:2050–2059.
2. Eltabbakh GH, Shamonki MI, Moody JM, et al.: Laparoscopy asthe primary modality for the treatment of women withendometrial carcinoma. Cancer 2001;91:378–387.
3. Kercher KW, Heniford BT, Matthews BD, et al.: Laparoscopicversus open nephrectomy in 210 consecutive patients: Outcomes,cost, and changes in practice patterns. Surg Endosc 2003;17:1889–1895.
4. Adachi Y, Suematsu T, Shiraishi N, et al.: Quality of life afterlaparoscopy-assisted Billroth I gastrectomy. Ann Surg 1999;229:49–54.
5. Braga M, Vignali A, Zuliani W, et al.: Laparoscopic versus opencolorectal surgery: Cost-benefit analysis in a single-centerrandomized trial. Ann Surg 2005;242:890–895.
6. Nathanson LK, Cuschieri A: The falciform lift: A simple methodfor retraction of the falciform ligament during laparoscopiccholecystectomy. Surg Endosc 1990;4:186.
7. Hashmonai M, Kopelman D: Sling retraction of the falciformligament to ameliorate exposure in laparoscopic upper abdominalsurgery. Surg Laparosc Endosc 1996;6:71–72.
8. Kim YW, Bae JM, Lee JH, et al.: The role of hand-assistedlaparoscopic distal gastrectomy for distal gastric cancer. SurgEndosc 2005;19:29–33.
9. Townsend CM, Beauchamp RD, Evers BM, et al.: Textbookof surgery, 17th ed. Philadelphia: Elsevier Sounders; 2004.pp 1515–1525.
10. Bulut O, Bora S, Safak T: A simple technique for wedge biopsy ofthe liver. Surg Gynecol Obstet 1987;165:167.
Journal of Surgical Oncology DOI 10.1002/jso
Fig. 2. Picture showing exposures of the stomach lesser curvatureand esophageal hiatus. The gastrohepatic ligament, hepatoduodenalligament, and esophageal hiatus were well visualized after liver liftingand pulling the stomach down and leftwards. [Color figure can beviewed in the online issue, available at www.interscience.wiley.com.]
Liver Lift During Laparoscopic Gastric Surgery 85