Liver function tests
38
Liver Function Tests Dr.laxman wagle
-
Upload
laxman-wagle -
Category
Health & Medicine
-
view
21 -
download
1
Transcript of Liver function tests

Liver Function Tests
Dr.laxman wagle

• Liver – the largest solid organ in human body• Weighing bet/n 1200 and 1500gm• Located in the upper quadrant of abdomen• Two sources of blood supply
– Hepatic artery from aorta supplies arterial blood rich in oxygen
– Portal veins shunt the venous outflow of the intestines and spleen-blood with less O2 but rich in nutrients to liver


• Liver is divided into thousands of lobules.• Each lobule composed of plates of hepatocytes
(liver cells) that radiates from central vein like spokes in a wheel.
• Hepatocytes continually form and secrete bile into canaliculi, which empty into terminal bile ducts.

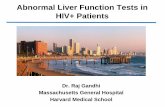
Basic structure of a liver lobule

Functions of liver
• Produces bilirubin a product of hemoglobin (Hgb) breakdown, excreted via bile ducts into intestinal tract for digestion.
• Major role in amino acid and carbohydrate metabolism.
• Produces many crucial proteins, including coagulation factors and albumin.

Functions of liver
• Most lipid and lipoprotien metabolism, including cholesterol synthesis occurs in liver which excretes into bile.
• Primary location for most drug and hormone metabolism hence in liver failure standard dosing of some medications lead to high serum concentration and toxicity.

Tests include:
a) Tests to assess liver synthetic capabilities
b) Tests to assess cholestatic disease and hepatocellular injury

Tests to assess liver synthetic capabilities
Used to assess functional capabilities of liver
Its synthetic products are measured [albumin, fibrinogen, prothrombin, hepatoglobin, transferin and other proteins]

Tests to assess liver synthetic capabilities
Most commonly used tests includeAlbuminProthrombin time
OccasionallyTotal proteinGlobulin (with albumin)Ammonia ( controversial)

Tests to assess liver synthetic capabilities
Albumin:Reference range: 3.5 to 5 gms/dl
liver Synthesizes albumin using AA derived from gut/breakdown of proteins
It Maintains plasma oncotic pressure.
It binds numerous hormones , anions, drugs and fatty acids

Tests to assess liver synthetic capabilities
Albumin:
Liver synthesise 12 gm /day if needed it can double the synthesis
Serum half life is20 days
Serum Albumin measurements are slow to fall after the onset of hepatic dysfunction due to long lifespan

Tests to assess liver synthetic capabilities
Albumin:
Complete cessation of albumin production results in only 25% decrease in serum concentrations after 8 days.
Albumin concentration remains unaltered in many liver disease when liver function is preserved.
if disease progress its synthetic capacity impaired[severe hepatitis, cirrhosis]

Tests to assess liver synthetic capabilities
Non hepatic causes: Hypoalbuminemia:Malnutrition, malabsorption, overhydration, nephrotic syndrome, protein losing enteropathy (through Gut), burns and chronic illness
At very low concentration (2-2.5gm/dl) patients can develop peripheral edema, ascities or pulmonary edema

Tests to assess liver synthetic capabilities
Non hepatic causes: Hyperalbuminemia:
Dehydration
Anabolic steroids
Does not cause any symptoms

Tests to assess liver synthetic capabilities
Globulin:
Reference range: 2 to 3gm/dl
Refers to total measurements of immunoglobulins (antibodies) in serum
Synthesised by B cell lymphocytes
Ig – IgA, IgD, IgE, IgG and IgM

Tests to assess liver synthetic capabilities
Causes:
Malabsorption
Protein losing enteropathy
Hepatocellular dysfunction does not lower globulin concentration (because some produced elsewhere) unless associated with malabsorption
Elevation of globulins is a sign of inflammation – may present in hepatitis

Tests to assess liver synthetic capabilities
Causes:
In chronic hepatitis - albumin decreases and globulin increases
In primary biliary cirrhosis – Increase in IgM
Alcoholic patients – increase IgA

Tests to assess liver synthetic capabilities
Non – hepatic causes: increases globulin
Chronic infections, chronic inflammatory states, multiple myeloma
In non hepatic condition – globulin increases than albumin concentration and thus G:A ratio will be >1 (normal – 0.6)

Tests to assess liver synthetic capabilities
Total protein:
Reference range: 5.5 to 9gm/dl
Refers to sum of albumin and globulin
Any symptoms increase either albumin/ globulin also increases total protein
Its value is limited if albumin and globulin results are already known

Tests to assess liver synthetic capabilities
Prothrombin time:
It is one of the coagulation factor
Liver synthesises SIX coagulation factors: I, II, V,
VII, IX and X
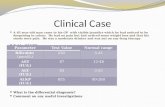
Normal range: 10 to 13 seconds
PT is not specific for liver disease

Tests to assess liver synthetic capabilities
Causes for prolongation of PT:
- inadequate vitamin K in the diet
- poor fat absorption
- poor / inadequate nutrition
- drugs – warfarin, salicylates, moxalactum, cefoperazone, tetracycline

Tests to assess liver synthetic capabilities
If PT remains prolonged despite parenteral vitamin K (10mg), it is considered a sign of substantial hepatic dysfunction
Treat the patient with vitamin K if no bleeding
If bleeding present, treat with fresh frozen plasma

Tests to assess cholestatic disease and hepatocellular injury
Liver disease:
Cholestatic
Hepatocellular damage
Mixed

Tests to assess cholestatic disease and hepatocellular injury
Cholestatic – primary interference with the metabolism or secretion of bilurubin from its initial production in hepatocytes to its secretion into duodenum.
Hepatocellular damage – damage to hepatocytes or inflammation of hepatocytes
Mixed type is due to: back pressureCholestatic hepatocellular damage swelling

Tests to assess cholestatic disease and hepatocellular injury
Elevation of liver enzymes are common findings in clinical practice
The significance of the elevation has to be assessed whether or not mild non-specific elevation (e.g., viral / drug / liver disease)

Tests to assess cholestatic disease and hepatocellular injury
Useful testsEnzymes Reference rangeALP 30 – 120 U/LGGT 0 - 30U/LAST 0 – 35 U/LALT 0 – 35 U/LLDH 110 – 220 U/L

Tests to assess cholestatic disease and hepatocellular injury
Useful testsReference rangeBilurubintotal 2 - 18 mmol/Ldirect (conjugated) 0 - 4 mmol/Lindirect (unconjugated) ?
Albumin 3.5 – 5.0 gms/dlGlobulin 2.0 – 3.0 gms/dlProthrombin time 10 – 13 seconds

Liver enzymes are most useful in differentiating hepatocellular damage from cholestasis
ALP extra-cellular GGT (present in cells lining biliary
canaliculi)
AST intra-cellular enzymes
ALT (present in cytosol of liver cells)
LDH

CHOLESTASIS
Intra-hepatic(obstruction in bile ducts within
liver)
Causes:– metastasis
Extra-hepatic(obstruction in bile ducts outside the
liver)
Causes:– gall stones– cancer of head of
pancreas– inflammation

• Jaundice is usually obvious to the eye• Confirmed by ALP and GGT• ALP & GGT Bone disorder (pagets disease, osteomalacia, 10, 20 malignancy of bone)
GGT (100-140 U/L) Chronic alcoholism
without any abnormality or in liver phenytoin

• If chronic alcoholism is associated with hepato-cellular damage, ALT increase along with GGT
• Chronic alcoholism can lead to fatty infiltration, alcoholic hepatitis and cirrhosis

Hepatocellular damage
• In hepatocellular damage, AST, ALT and LDH increases
• Both AST and ALT runs parallel
• Measure ALT as it is very specific to liver

Causes: Paracetamol overdose, ischemic / hypoxic hepatitis
Marked elevation of ALT and LDH, both of the same order (800-3000 U/L) The ratio of ALT / LD is 0. 8 - 1.2
Chronic alcoholism
chronic alcoholics with under lying disease when gives therapeutic dose of paracetamol, can sustain liver damage with the marked rise ALT/LDH as paracetamol toxicity
Viral hepatitis
- both ALT and LDH increases- ALT elevation is significantly > LDH- ALT/LDH ratio is 1.2-2.0

Rhabdomylosis
- LD level will be markedly elevated (800-20,000 U/L) than ALT
- ALT: LDH ratio is < 0. 8
- Due to muscle destruction CK level also increase (2,000 – 1,00,000 U/L)
- Increase CK does not occur in liver damage (liver does not contain CK)
Infections mono-nucleousis
Simultaneous increased level of ALP, GGT, LD and ALT between (200-600 U/L) occur.

Drugs involved in liver disorders
• Predominantly hepatocellular– Allopurinol, aspirin, cytotoxic, diclofenac, anti TB drugs,
methotrexate, paracetamol, phenytoin, propylthiouracil and quinidine
• Predominantly cholestasis- Augmentin, CBZ, chlorpromazine, chlorpropamide, flucloxacillin,
dicloxacillin, indomethacin, phenothiazines and tolbutamide
• Mixed– Methyldopa, halothane, norfloxacin, PAS, ranitidine, sulindac,
valproate co-trimaxozole


Thank you