Liver function test
71
GUIDED BY : DR. C. GADKARI MAM PRESENTED BY : DR. ANURAG GIRI
-
Upload
anurag-giri -
Category
Documents
-
view
180 -
download
3
Transcript of Liver function test

GUIDED BY : DR. C. GADKARI MAMPRESENTED BY : DR. ANURAG GIRI
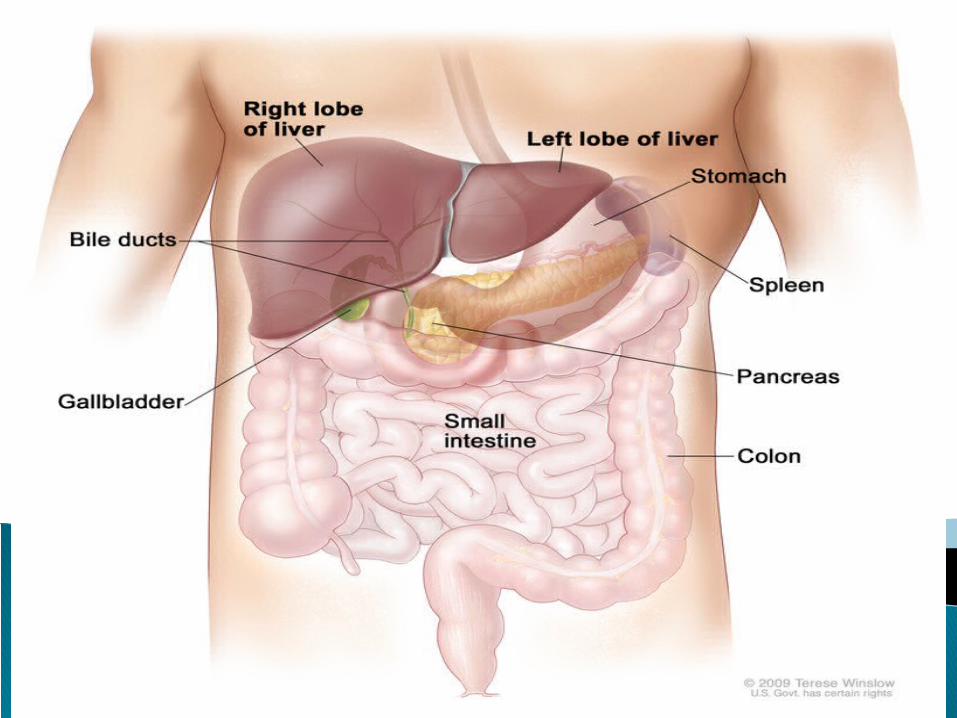

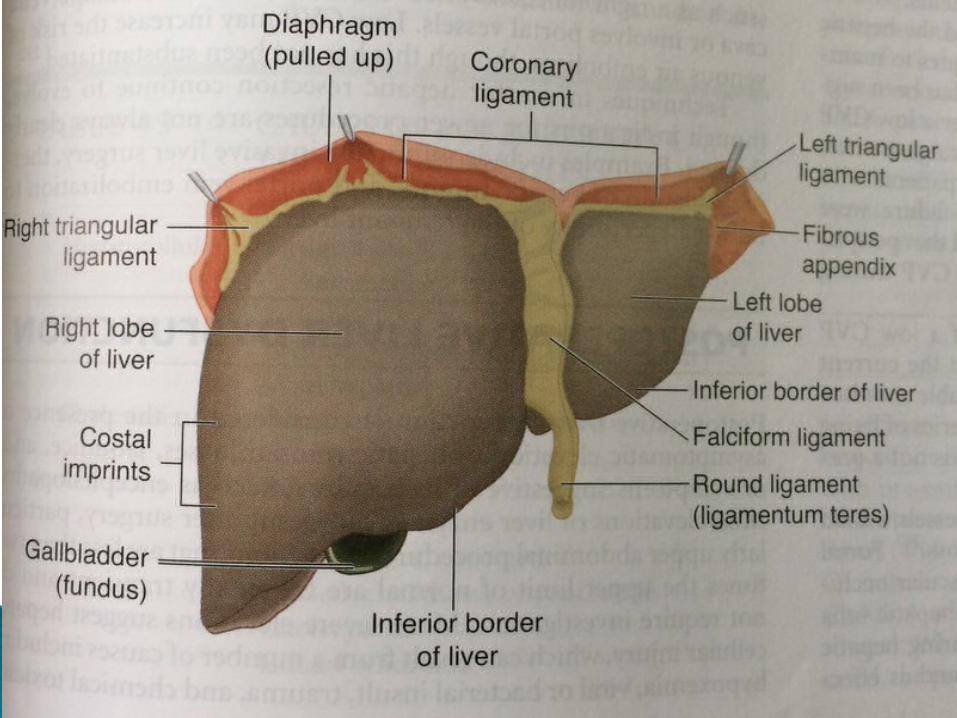
Located in rt upper quadrant of the abdomen under right lower rib cage and projects for a variable extent into left upper quadrant
Held in place by ligamentous attachment to the diphram, peritonium ,great vessles and upper GI track.
Rt lobe further divided into: 1. CAUDATE POSTERIOR SURFACE
2. QUADRATE INFERIOR SURFACELiver is divided into 8 segments
Largest internal organ and body’s metabolic headquarter
Wt. 1.5kg (2%)of total body weight of adult
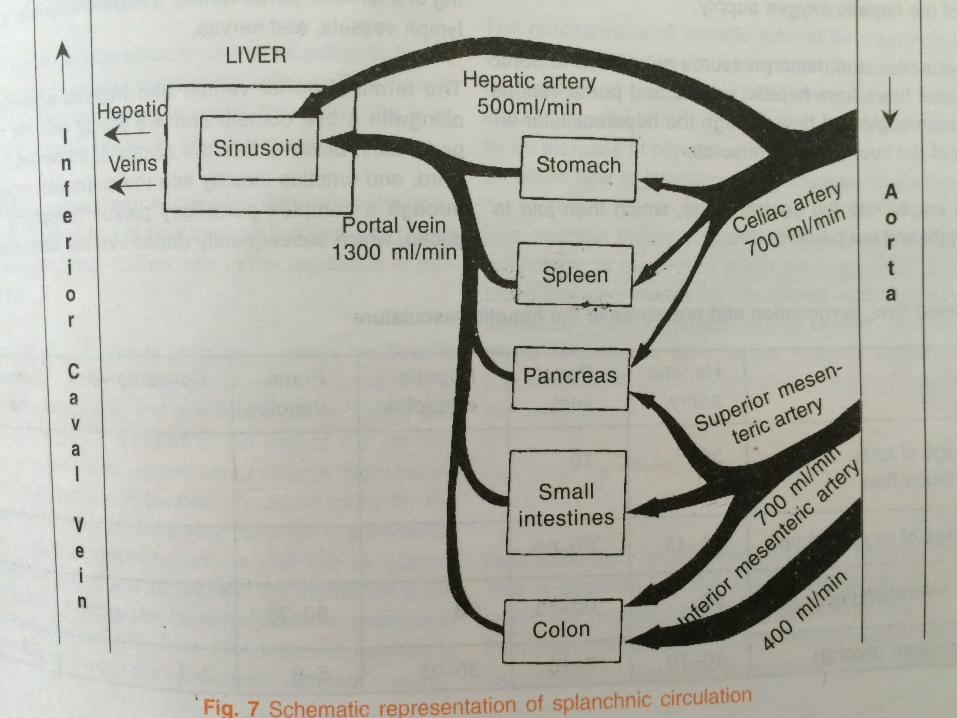
Liver receives 25% of cardiac output via dual supply (portal vein and hepatic artery)
Portal vein drains blood from GI track and supply 75% of liver inflow (1L/min)
Hepatic artery supply 25% Due to high O2 contents in hepatic artery each vessel
supply 50% of hepatic O2 Portal vein have low vascular resistance (8-10mm/hg) Hepatic venous pressure is 0 mm/hg

Functional unit Is lobule (1x2mm). 50,000-1,00,000
Lobule consists of plates of hepatocytes located in a radial distribution about a central vein
Efferent blood supply from portal vein and hepatic arterey enters at periphery of lobule
Bile formed in the hepatocytes flows into canaliculi (located between plates of hepatocytes) and drains to the bile duct
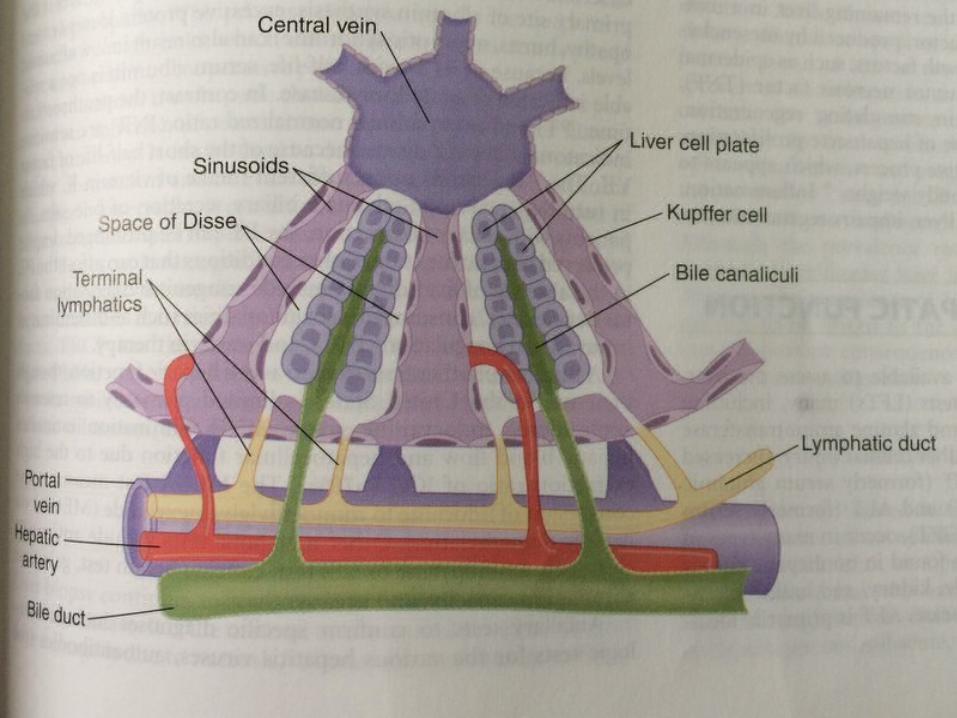
The large pores in the endothelium lining are sinusoids lined by two types of cell : typical endothelial cells and large kupffer cells(reticulo endothelial) capable of pagocytizing bacteria and other foreign matter in the blood. Allow plasma and its protein to move into the tissue space surrounding hepatocytes (space of dissc) This fluid drains into the lymphatic system
Microcirculation of liver lobule ZONE 1: PERIPORTEL : Receive O2 rich blood
from portal vein and hepatic artery. ZONE 2: MEDIOLOBULAR : As blood moves
through sinusoid it passes from zone 2 to zone 3. ZONE 3: CENTRILOBULAR : Poor in O2
Sympathetic innervation from T3 to T11 controls resistance in hepatic venules
When injured hepatocytes turns into fibrous tissue blood flow is impeded and causes portal hypertension
When portal venous flow is reduced the hepatic atrery can increase flow by 100% to maintain hepatic O2 supply.This relation between two vesseles is hepatic artrial buffer response
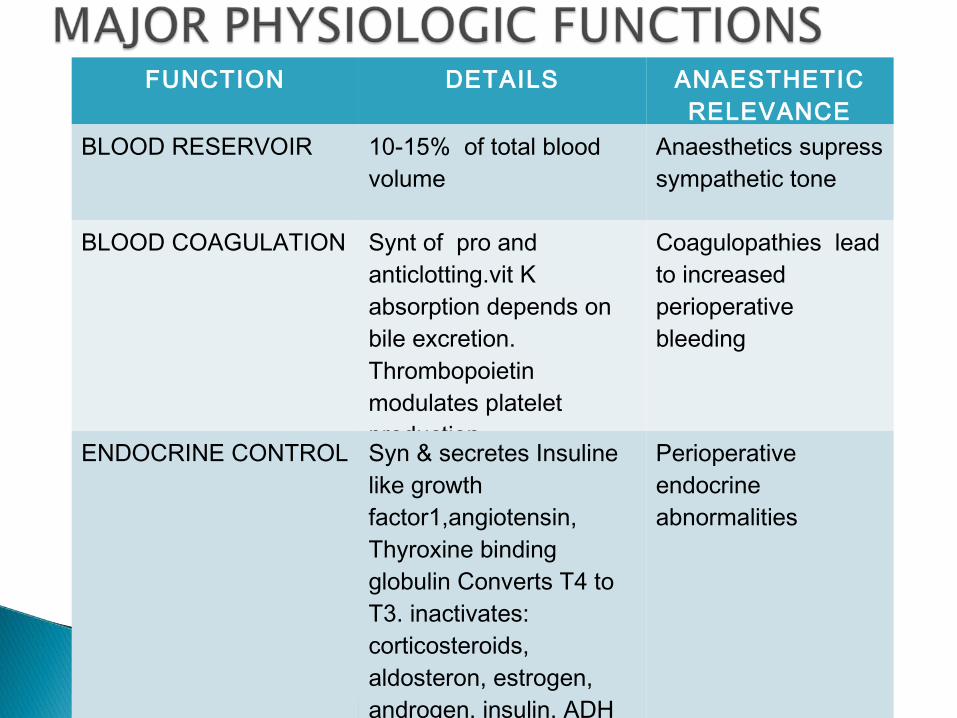
FUNCTION DETAILS ANAESTHETIC RELEVANCE
BLOOD RESERVOIR 10-15% of total blood volume
Anaesthetics supress sympathetic tone
BLOOD COAGULATION Synt of pro and anticlotting.vit K absorption depends on bile excretion. Thrombopoietin modulates platelet production
Coagulopathies lead to increased perioperative bleeding
ENDOCRINE CONTROL Syn & secretes Insuline like growth factor1,angiotensin, Thyroxine binding globulin Converts T4 to T3. inactivates: corticosteroids, aldosteron, estrogen, androgen, insulin, ADH
Perioperative endocrine abnormalities

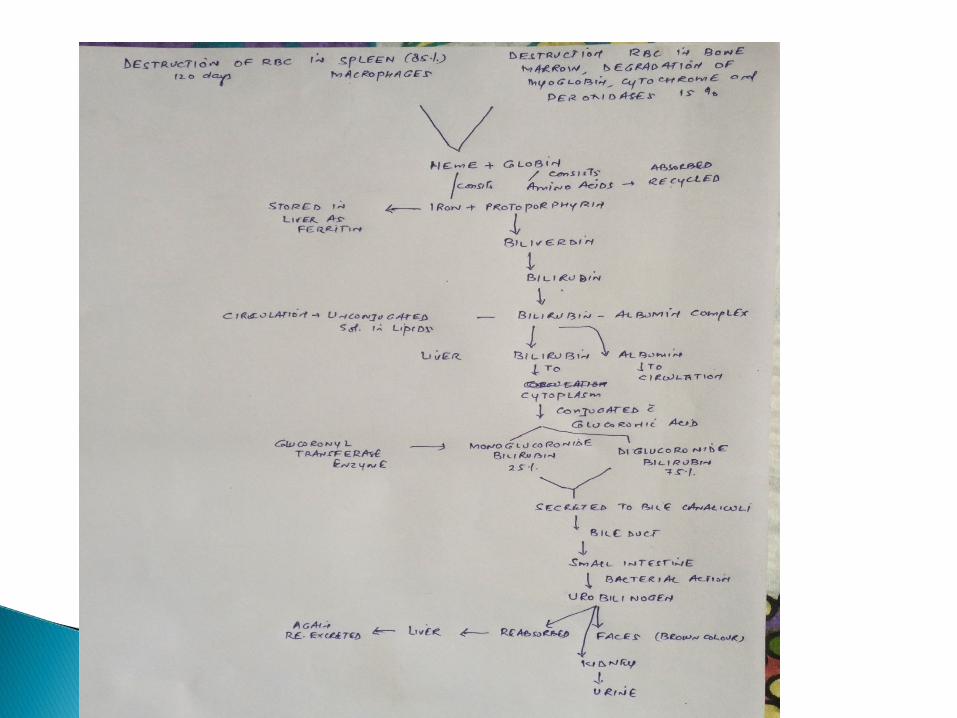
BILIRUBIN EXCRETION
Absorbs bil irubin from blood,conjugates and excretes.synthesizes haptoglobin and scavenges Hb
Lipid metabolism Fatty acid synthesis, cholesterol and lipoprotein metabolism
Abnormal cellular function, affect pharmacokinetic and dynamics of anaesthetic agents.
Amino acid metabolism Protein and aminoacid metabolism and urea production
Elevated level and encephalopathy
Immunologic modulation Largest reticuloendothelial organ. Filters out toxins, bacteria and debris. Hepatic macrophages,Tcells and Kupffer cells triggers systemic inflammatory response
Immunocompromise susceptible to perioperative infection and sepsis.

Liver can store 1L of blood and release blood in circulation at low blood volume
Liver stores vit.B12 (1yr supply) vit.D (3mnth supply) vit.A (10mnth supply) Iron transported via apoferrin and stored as ferritin
(blood iron buffer

Energy production and storage of nutrients absorbed from GI track
Glucose buffering function : Store glucose as glycogen convert carbohydrate (fructose and glactose) to glucose
Synthesise glucose from amino acid and triglicerides (gluconeogenesis)
Synthesise fat cholesterol phospholipids and lipo proteins
Metabolise fat,convert fatty acid to acetyl coenzyme A (COA) is excellent source of energy
Cholestrol synthesized is converted to bile salt and secreted to bile,rest is distributed to body to form cellular membrane and other vital structure
Protein metabolism synthesize all plasma protein except gama globolins (which are formed in plasma cell)
Forms 15-50gms protein/day Albumin is the major protein synthesized and
responsible for plasma oncotic pressure
Blood clotting factors Synthesize in liver except factor III (tissue
thromboplastin), factor IV (calcium) and factor VIII (von willbrand)
Vit K is required for synthesis of factor II (prothombin),factor VII , IX , X
Produce around 500ml of bile daily and store in gall bladder in concentrated form 35-50ml
The fat in food in the duodeneum causes release of choleystokenin hormone from duodenel mucose that stimulate gall bladder contraction
Bile contains bile salt,bilirubin and cholestrol. It dissolves fat to absorb into GI track and bile salt
returns to liver by portal vein
Liver has unique ability to regenerate It restores itself after injury or partial hepatectomy Hepatocytes growth factor produced by
mesenchymal cells in the liver Other growth factor are epidermal growth factor,
interlukin-6,cytokines ,tumor necrosis factors

Hepatocellular-like viral hepatitis features of liver injury & inflammation predominate
Cholestatic(obstructive)-gall stones,biliary cirrhosis ,features of inhibition of bile flow predominate
Mixed -both feature are presents
Etiologic diagnosis Estimation of disease sevearity (grading) Estimation of disease stage
Family history – jaundice, anaemia, splenectomy, cholecystectomy,gall stones
Occupation in detail Environmental factor – contacts with rats (weils
diseases), exposures to toxins Travel to other countary Alcohol intake Conact with jaundice patients BT, plasma transfusion ,tattoing, dental treatment
Drug history – narcotics, estrogens Indigestion or pain in rt upper quadrant
A patient of liver dysfunction presents with following complaints:
• Pain in abdomen-the rt. quadrant region• Abdominal distension• Pruritus• Anorexia• Nausea and vomiting• Wt. loss • Fever• Fatigue• Haematemesis• Malaena• Dark coloured urine (yellowish discolouration)• White colour stool • Oliguria
Jaundice Hepatomegaly Spider Naevi Splenomegaly Scratch Marks Ascites Palmer Erythema
Dilated Abdominal Veins
Peripheral Oedema Finger Clubbing Testicular Atrophy Bruising Gynaecomastia Confusion/Coma
Jaundice in sclera or in skin Pallar –sign of anaemia(hemolysis) Gynecomastia , testicular atrophy (cirrhosis) Skin exam- ecchymosis due to prothombin
defficiency, purpura due to thrombocytopenia,spidor angiomas found around face neck shoulder forearm
In chronic cholestatic – scratch marks , finger clubbing
Slight deterioration of the intellact &minimal personality changes may suggest hepatocellular disease
Ascitis Dilatation of periumblical veins Size of liver Tender gall bladder (murphy sign) Auscultation – venous hum over dilated collatral
veins radiating from umblicus called caput medusac
Typical battary of blood test used for initial assesment of liver disease
.Serum alanine aminotranferase (ALT) 5-42u/l
.Serum aspartate aminotransferase (AST) 5-40u/l
.Alkaline phosphatase
Children 25-350 u/l Adult males 25-120 u/l Adult females 25-90 u/l
.Direct (conjugated 0-0.2mg/dl)
. Total bilirubin (0.3 -1.0 mg/dl) .Albumin 3.5-5.0 gm/dl .Prothrombin time 11-15 secs .Gamma glutamyl transpeptidase (GTT) male-upto 40u/l female-upto 25u/l .Hepatitis serology to define types of viral hepatitis

.autoimmune markers to diagnose primary biliary cirrhosis (anti mitochondrial antibody AMA)
Selerosing cholongitis(peripheral antineutrophil cytoplasmic antibody P-ANCA)
Autoimmune hepatitis (antinuclear ,smooth muscle, liver kidney microsomal antibody)
Serum bilirubin: Bilirubin is a break down product of the porphyrin ring of heme containing protein found in two fraction1. Conjugated(direct) : water soluble and can be excreted by kidneys. Upto 30% of total bilirubin. Increased due to liver or billiary tree disease.2. Un- conjugated: Insoluble in water and bound to albumin in blood.Increased due to haemolatic disorder
Urine bilirubin: unconjugated bilirubin always bind with albumin so it is not filtered by kidneys only conjugated bilirubin is found in urine
A urine dipstick test is done for urine conjugated bilirubin
Ammonia is produced in the body during protein metabolism liver ditoxifies it and convert to ureaThere is a poor corelation of blood ammonia and hepatic function as striated muscles also detoxifies ammoniaAmmonia can be elevated in severe portal htn
1. Enzymes reflects the damage to hepatocytes: AST is found in liver,cardiac muscle, skeletol
muscle,kidney,brain,lungs,leucocytes and erythrocytes in decreasing order of concentration.
ALT is found primarily in liver These enzymes released in blood in increased
amount when liver cells are damaged resulting increase in permiability of cell membrane.
There is a poor corelation between degree of liver cell damaged and level of enzymes
Level upto 300u/l are non-specific and may be found in any type of liver disorder
Level upto more than 1000u/l are specific and extensive hepatocellular injury may present
In most acute hepatocellular disorder the ALT is higher than or equal to AST
A ratio of AST:ALT 3:1 is suggestive of ALD
The AST/ALT ratio is helpful in distinguishing between alcohol induced hepatitis and viral hepatitis.
Alcohol tends to damage hepatocyte mitochondria thus causing rise in AST usually greater than twice the ALT.
ALT activity is low in patients with alcohol induced liver disease as these have deficiencies of pyridoxal-5- phosphate, a vitamin necessary for the function of ALT.
A decrease in AST/ALT <1 ratio is more consistent with a diagnosis of viral hepatitis.
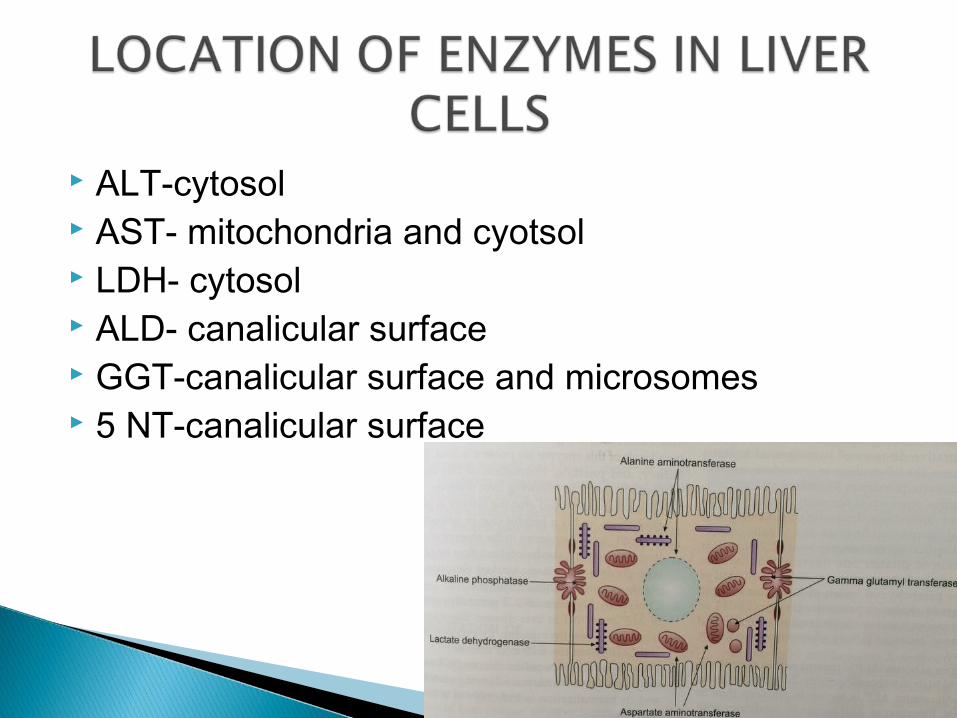
ALT-cytosol AST- mitochondria and cyotsol LDH- cytosol ALD- canalicular surface GGT-canalicular surface and microsomes 5 NT-canalicular surface
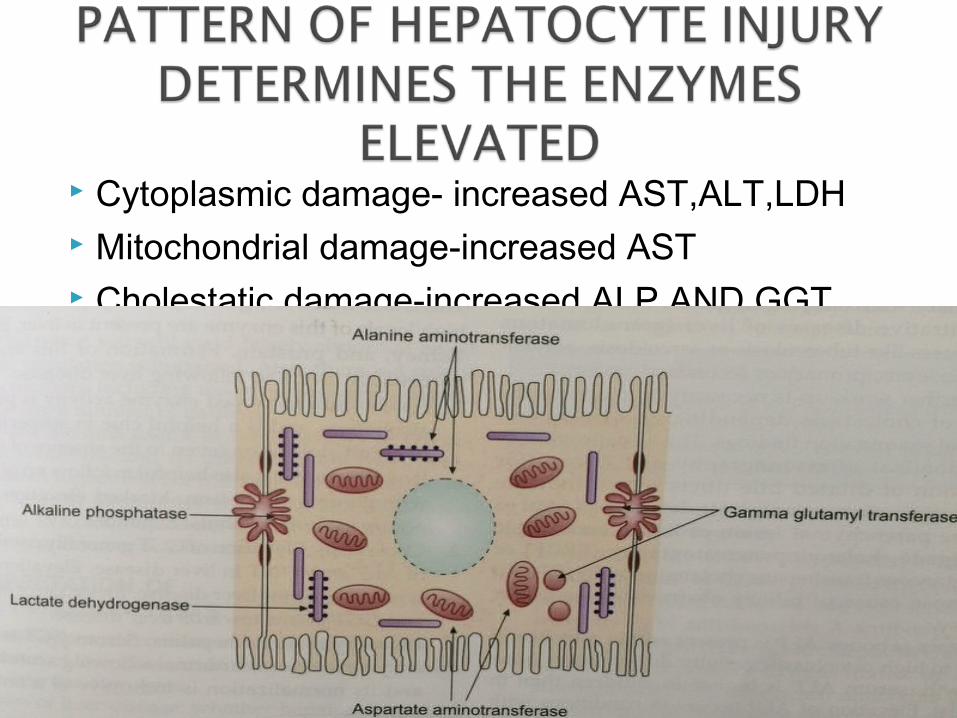
Cytoplasmic damage- increased AST,ALT,LDH Mitochondrial damage-increased AST Cholestatic damage-increased ALP AND GGT
1.SERUM ALBUMIN: exclusively synthesized by hepatocytes,long half life 15-20 days, poor indicator for acute of chronic hepatic dysfunction
Minimal changes seen in viral hepatitis, drug related hepatotoxicity and obstructed jaundice.
Hypo albuminemia is commom in cirrhosis

2. SERUM GLOBULIN: Group of protein made up of gamma globulin(immuno globulin).
Produced by B lymphocytes and alpha and beta globulin produced in hepatocytes
Gama globulin increased in chronic liver disease
Except factor VIII all blood coagulation factors are made in liver hepatocytes
Measurement of clotting factor is accurate measure of hepetic synthetic function
Serum prothrombine time measures factor II,V,VII and X
PT may be increased in vit.K deficiency PT more than 5 secs. Is poor prognostic sign in
hepatic disease
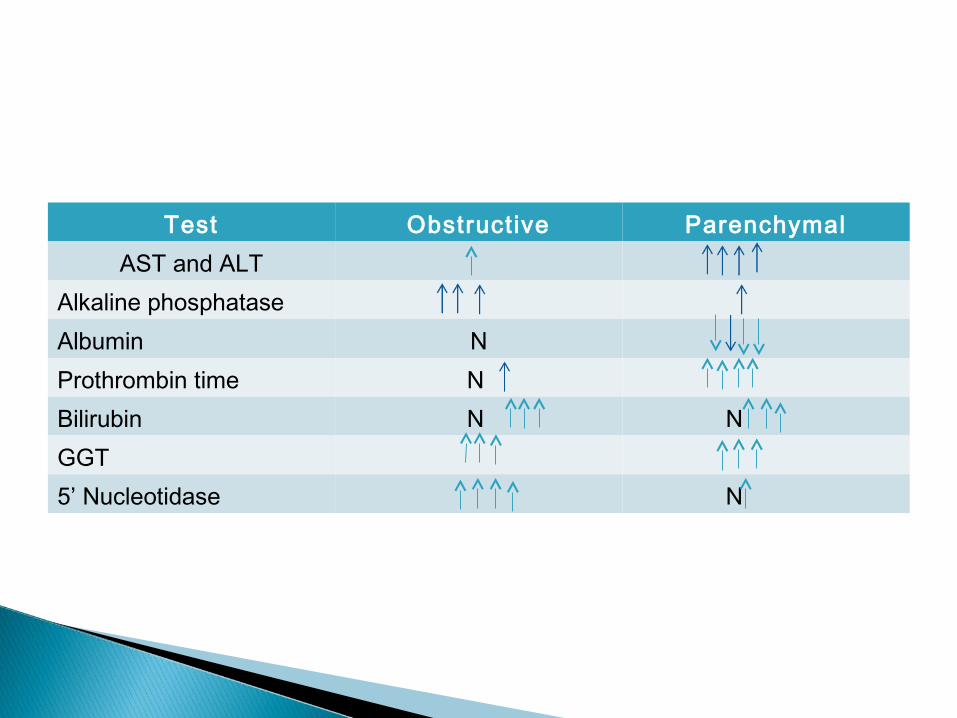
Test Obstructive ParenchymalAST and ALT
Alkaline phosphataseAlbumin NProthrombin time N Bilirubin N N GGT5’ Nucleotidase N
Xray- limited role detects calcified & gas containg lesions
Barium studies of GIT-In suspected cases of portal HTN to determine esophagogastric varices.-enlargement of lt. lobe of liver(due to tumour, abscess or cirrhosis) may displace the barium filled stomach laterally and anteriorly.-tumours of the head of pancreas may produce displacement or irregularity of 2nd part of duodenum.
USG whole abdomen-to know the size and shape of liver and spleen.-in biliary obstruction, to determine the size of bile ducts, presence of gall stones, presence of mass in the head of pancreas.-in detecting mass lesions such as tumours, cysts or liver abscess.
CT- Abdomen & MRI-in diagnosis of mass lesions in liver or pancreas.-in differentiating intrahepatic fluid collections such as cysts, abscesses and haematomas.-to obtain excellent image of pancreas,liver and spleen.
Magnetic resonance cholengiopancreatiography (MRCP) for visualization of billary tree
Endoscopic retrograde cholengiopancreatiography (ERCP)-allows for biopsy,direct visualisation of the ampulla and common bile duct having some therapeutic options like sphincterotomy,stone extraction,placement of nasobillary catheter and biliary stents
Percutaneous transhepatic cholangiography (THC) – Percutaneous injection of contrast into bile duct under fluoroscopic guidance can determine sight and cause of billary obstruction
Paul Ehrich performed first percutaneous liver biopsy in 1883 in Germany.
TYPES 1. Percutaneous liver biopsy a) blind liver biopsy b) guided liver biopsy c) plugged liver biopsy 2. Transvenous(trans jugular liver biopsy) 3. Laproscopic liver biopsy
Acute hepatitis of unknown cause Chronic liver disease a)to define cause b) grading of inflammatory activity c) staging of chronic hepatitis c and chronic hepatitis b d) monitor response to therapy Diagnosis of metabolic liver disorder Diagnosis and grading of alchoholic liver disease
Staging of advanced cases of primary billiary cirrhosis
Investigation of persistant abnormal and unexplained LFT
Investigation of PUO Diagnosis of focal hepatic lesion Histologic monitoring following liver
transplantation
Unco-operative patient Extrahepatic biliary obstruction Bleeding diathesis or abnormal coagulation profile Tense ascites Hydatid cyst of liver Suspected hemangioma or other vascular tumor Amyloidosis
French word jaune means yellow or icterus, yellow discoloration of skin, sclera and mucous membrane
Clinically evident when serum bilirubin>2.0 mg/dl
Main type of bilirubin increased in plasma Unconjugated>85%of total causes are hemolysis,resorption of large
hematoma,ineffective erythopoiesis,physiological jaundice of new born ,
Conjugated >50%of total causes are: hepatitis cirrhosis,
cholestasis,drugs(anabolic steroids, oral contraceptis) ,toxins
Mixed(conjugated+unconjugated) Conjugated bilirubin is 25-50% of total, viral or
alchohlic hepatitis
Hemolytic Hepatocellular Obstructive
Pre-hepatic: Excessive formation of bilirubin exceeding the capacity of the liver to conjugate it for excretion. The type of bilirubin increased is unconjugated.Urobilinogen is increased in urine and feces
Hepatic: Unconjugated, conjugated or both are increased.
Un conjugated: 1)Defective uptake of bilirubin by liver cell from blood (gilbert’s syndrome). 2) Defective conjugation of bilirubin
Conjugated hyperbilirubenemia: 1)Hepatocellular disease : AST and ALT are raised
2) Intrahepatic cholestasis a) Impairment of secretion of bilirubin from
hepatocyte into biliary canaliculi b) Obstruction of bile flow in canaliculi by
swollen hepatocytes. c) Damage to intrahepatic canaliculi 3) Post hepatic jaundice called as obstructive
surgical or extrahepatic cholestatic

Child-Turcotte Pugh classification is a universally used method developed in 1964.
Total score=15(minimum=3) Grades= A,B,C Grade A(score of 5-6)-low risk with 5% mortality. Grade B(score of 7-9)-moderate risk with 10% mortality. Grade C(score of >10)-high risk with >50% mortality.NB: grade C indicates decompensated cirrhosis.
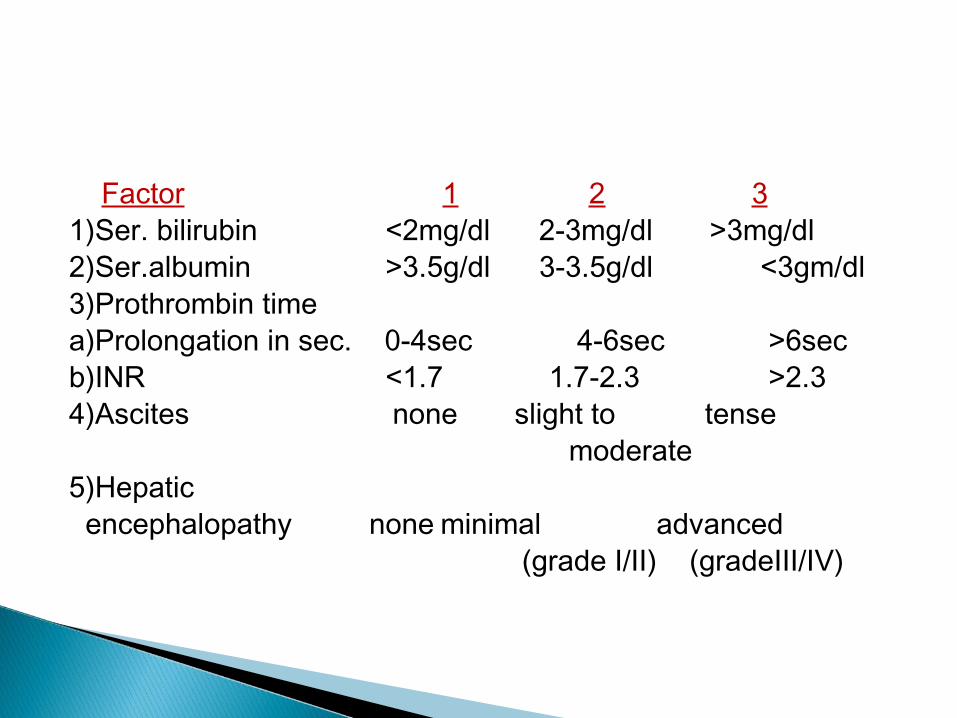
Factor 1 2 31)Ser. bilirubin <2mg/dl 2-3mg/dl >3mg/dl2)Ser.albumin >3.5g/dl 3-3.5g/dl <3gm/dl3)Prothrombin timea)Prolongation in sec. 0-4sec 4-6sec >6sec b)INR <1.7 1.7-2.3 >2.34)Ascites none slight to tense
moderate5)Hepatic encephalopathy none minimal advanced
(grade I/II) (gradeIII/IV)
Model for end stage liver disease(MELD) is another system to assess the severity of liver disease which was developed at Mayo clinic to assess 3 month outcomes of patients undergoing TIPS(transjugular intrahepatic portosystemic shunt procedure).
Calculation is done by MELD Score:=(0.957xlog e[serum creatinine(mg/dl)]+0.378 x log e[total serum bilirubin(mg/dl)]+1.120 x log e[INR]) x10
Minimum for all value=1 Maximum value for creatinine=4
A day prior to surgery, the anaesthetist should meet the patient and relatives and explain about the risk factors of surgery.
Any expected post-operative ventilatory support monitoring and about possible post-operative complications should be explained to patient and relatives.
Consent Availability of appropriate blood and blood
products and suitable post-operative facilities to be checked.
Anti-anxiety medication is prescribed a night prior to surgery in a guarded dose as there is reduced ability of the liver to metabolize the drug.
Patient to be kept NBM a night prior to surgery but during this period IVF(crystalloids) in a rate of 1-2ml/kg/hr is to be given as these patient who are having jaundice and with hepatorenal syndrome are at increase risk of renal damage if they become dehydrated or hypotensive as a result of pre-op fast as these concentrates toxins in the filtrate.
Dextrose containing fluids is a better choice to give when the patient is NBM as these pt. of hepatic dysfunction are more prone for hypoglycemia.(Liver acts as a glucostat i.e. maintains blood sugar level by glycogenesis and stopping glycogenolysis when there is increased blood sugar in blood and viceversa when there is decrease blood sugar).
The pre-operative risk factors associated with increase post-operative mortality includes-
1)Serum albumin <3gm/dl2)Presence of infection3)WBC >10,000 cells/cubic mm4)Treatment with more than 2 antibiotics.5)Prothrombin time >1.5 sec over control.6)Serum bilirubin >50µmol./litre(2.92mg/dl)7)Presence of ascites8)Malnutriion9)Emergency surgery

Regional anaesthesia is preferred in peripheral surgeries if there is no clotting abnormalities.
Guidelines: 1)Prothrombin time not greater than 2.5sec. above the
lab. control2)Platelet count >50,000/mm33)Bleeding time not greater than 12 min. If bleeding/clotting variables are within these
measurements epidural, spinal and regional block anaesthesia can be employed.
For abdominal surgeries/ pt. with obvious coagulopathy, regional anaesthesia is contraindicated.
Premedication-lorazepam(25-50 mck/kg)+ ranitidine
Induction – thiopentone (3-5 mg/kg) Intubation-succinylcholine (1-2 mg/kg) and low
pressure cuffed oral tracheal tube Maintenance-fentanyl 1 mck/kg, isoflurane,O2,
N2O/air,ippv+peep(aim for paco2 3.5-4.6 pka) Drug infusion- atracurium 0.5 mg/kg per hr Venous access – peripheral cannulae Arterial line-central venous line (two) one for
monitoring one for drug infusion Urinary catheter – for urine output