Liver diseases yakrut vikara
45
Liver diseases- Yakrut Vikara Dr. Prathamesh V. Karpe
-
Upload
prathamesh-karpe -
Category
Education
-
view
81 -
download
2
Transcript of Liver diseases yakrut vikara
- 1. Liver diseases- Yakrut Vikara Dr. Prathamesh V. Karpe
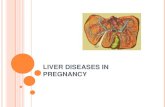
- 2. Anatomy and physiology A Liver B Hepatic vein C Hepatic artery D Portal vein E Common bile duct F Stomach G Cystic duct H Gallbladder
- 3. Anatomy- 1) 2 anatomical lobe with separate blood supply, bile-duct & venous drainage. 2) Dual blood supply- 80% PV and 20% H.Artery 3) Liver regenrates fully after partial ressection. 4) Ressection is based on anatomical lines to preserve Max. functioning of the liver.
- 4. Physiology 1) Maintaining core body temperature. 2) pH balance and correction of lactic acidosis. 3) Synthesis of clotting factors. 4) Glucose metabolism, Glycolysis, gluconeogenesis. 5) Urea, Bilirubin formation from protein catabolism. 6) Drug & Hormone metabolism and excretion. 7) Removal of gut endotoxins & Foreign antigen.
- 5. Normal LFTs 1 Blirubin 5 7 mol /L 2 Alkaline phosphatase (ALP) 35 130 IU/L 3 Alanine transaminase (ALT) 5 40 IU / L 4 Asparate transaminase (AST) 5 40 IU / L 5 Gamma-Glutamyl transpeptidase 10 48 IU / L 6 Albumin 35-50 g/L 7 Prothrombin time (PT) 12 16 secs
- 6. ALT and AST Enzymes, found in Hepatocytes Released when liver cells damaged ALT is specific for liver injury AST (SGOT) is also found in skeletal and cardiac muscle
- 7. Transaminitis: < 5 x normal ALT predominant Chronic Hep B / C Acute A-E, EBV, CMV Steatosis / Steatohep Hemochromatosis Medications / Toxins Autoimmune Hepatitis Alpha-1-antitrypsin Wilsons Disease Celiac Disease AST predominant Alcohol-related liver dz Steatosis/ Steatohep Cirrhosis Non-hepatic source Hemolysis Myopathy Thyroid disease Strenuous exercise
- 8. Severe AST & ALT Elev: >15x Acute Viral Hepatitis does not predict outcome Bili > 20 poor prognosis Ischemic Hepatitis hypotension sepsis hemorrhage MI Autoimmune Hepatitis Wilsons Disease Acute bile duct obstr Hepatic Artery ligation Budd-Chiari Syndrome Medications / Toxins acetaminophen CCl4
- 9. ALKALINE PHOSPHATASE Found in hepatocytes that line the bile canaliculi Level is raised in Biliary obstruction (causes stretch of the bile canaliculi) BUT also found in BONE and PLACENTA GGT is also found in bile canaliculi and therefore can be used in conjunction with Alk Phos for predicting liver origin BUT GGT can be raised by many drugs including Alcohol and therefore non specific
- 10. BILIRUBIN Water insoluble product of heme metabolism Taken up by liver and conjugated to become water soluble so it can be excreted in bile and into bowel. Patient looks Jaundiced if bilirubin >2.5 If patient is vomiting GREEN, then they have bowel obstruction below the level of the Ampulla of Vater.
- 11. WHAT IS THE DEAL WITH DIRECT AND INDIRECT BILIRUBIN? Prehepatic disease (eg hemolysis) causes high bilirubin which is non conjugated ie. Indirect fraction higher Hepatic disease causes increased conjugated and unconjugated bilirubin Post hepatic disease eg. Gallstones have increased conjugated (direct) bilirubin and lead to dark urine and pale stool.
- 12. PROTHROMBIN TIME/INR Measure of the Vitamin K dependent clotting factors ie. II, VII, IX and X. The liver is involved in activating Vitamin K. Therefore in liver damage, these clotting factors cannot be produced. Before you believe that prolonged INR is due to liver disease just make sure the patient has adequate Vitamin K by giving 10mg sc. Giving Vitamin K has no effect on INR if patient has impaired synthetic function.
- 13. ALBUMIN Albumin has a half life of 21 days, so the drop that occurs with hepatic dysfunction does not occur acutely That said, acute illness can cause albumin to drop rapidly a process thought to be due to cytokines increasing the rate of albumin metabolism HOWEVER, dont forget that low albumin also occurs in NEPHROTIC syndrome, so always check the urine for protein.
- 14. TYPICAL PATTERNS HEPATOCELLULAR Increased transaminases Viral Hepatitis Drugs/alcohol Autoimmune NASH Hemochromatosis CHOLESTATIC Increased Alk Phos and Bilirubin Also may cause increased transaminases Gallstones Primary Biliary Cirrhosis Sclerosing Cholangitis Pancreatic C/a
- 15. Acute liver failure Causes :- 1) Viral hepatitis (A,B,C,D,E) 2) Drugs- halothane, isoniazid, rifambicin, antidepressant, NSAIDs, valporic acid, paracetomol over dose (>1000mg/day). 3) Mushroom poisoning. 4) Shock and multi-organ failure 5) Acute Budd-chiari syndrome 6) Wilsons disease 7) Fatty liver of Pregnancy
- 16. Clinical features Early stage- no objective sign, severe liver dysfunction Onset of clinical jaundice + neurological signs(hepatic encephalopathy)- drowsiness, confusion, coma
- 17. Treatment 1) Fluid balance and electrolytes 2) Acid base balance and blood glucose monitoring 3) Nutrition 4) Renal function (hemofiltration) 5) Respiratory support ( ventillation) 6) Monitering and treatment of cerebral oedema 7) Treat bacterial and fungal infection 8) Liver transplant
- 18. Chronic liver disease Lethargy and weakness Jaundice (inability to metabolise bilirubin) Hyperdynamic circulation with High cardiac output, large pulse volume, low BP, flushed warmed extremities Fever- due to inflammation and cytokinin released from the diseased liver or bacterial infection. Skin changes spider naevi, palmar erythema, white nails Endocrinological hypogonadism and gynaecomastia. Hepatic encaphalopathy- mental derrangement- memory impairement, confusion, personality changes, altered speech pattern, slow slurred speech, flapping tremors (Asterixis). Abdominal distention due to ascitis Protein catabolism- coagulation defect, skin bruising
- 19. Portal hypertension Causes 1)Prehepatic- PV abnormality before entering into liver, ex- portal vein thrombosis, splenic vein thrombosis, congenital atresia. 2) Intrahepatic- liver cirrhosis, malignancy of liver, polycystic liver (in the liver causes) 3) Post hepatic- above liver causes- Right sided heart failure, Budd chiari syndrome
- 20. Liver cirrhosis Alcohol is commonest cause Viral hepatitis (B and C commonly) Injury- alcohol, virus (B&C), prolonged cholestasis Autoimmune (lupoid hepatitis) Metabolic disorders- hemochromatosis, wilsons disease, - antitrypsin deficiency.
- 21. 4 Stages Liver cell necrosis Inflammatory cell infiltate Fibrosis Nodular regeneration which may be macronodular (alcohol), micronodular (viral) or mixed
- 22. What is portal HTN? Portal pressure above 5 mm Hg 8-10mm Hg pressure is required to stimulate porto-systemic collaterisation Collateral network through coronary vein & short azygous vein leads to Oesophageal and gastric varices. Recanalised umbilical vein from the left portal vein to the epigastric venous system- Caput medusae Retroperitoneal collateral network- hemorrhoidal veins- hemerrhoids.
- 23. volume of Portal vein flow is regulated indirectly by vasoconstriction and vasodilatation of the splanchic Arterial bed. Hepatic arterioles responds to catecholamines & sympathetic N. stimulation thus Hep. Art flow is directly regulated. In decreased Portal flow, hepatic blood flow is kept near to normal as possible by hepatic Arterial autoregulatory or buffer response.
- 24. cf Non-specific complaints Weight loss Malaise, weakness Past H/o alcoholism- chronic Complicated biliary disease Exposure to hepato-toxins
- 25. signs signs advanced signs 1. Spider angiomas 2. Palmar erythema 1) ascitis 3. Testicular atrophy 2) jaundice 4. Gynaecomastia 3) palpation of firm irregular liver edge 5. Palpable spleen 4) liver flap tremors *Accompanied by Anaemia,leukopenia,thrombocytopenia
- 26. Investigations 1. Anaemia- hemmorhage, nutritional deficiency, hemolysis, bone marrow depression, alcholism. 2. Platlet count 3mg/100ml 9. Hepatitis serology B&C 10. Hep A causes acute liver disease 11. HCC secondary to Hep B and C 12. HCC elevated Alpha feto protein level 13. CT abdomen 14. Sr. Electrolytes hypo NA,K, Metabolic Alkalosis
- 27. Metabolic disorders secondary to hypoaldosteronism, Diarrhoea and recurrent emesis. Conversion of NH3cl to NH3+ cerebraltoxincrosses blood brain barrier encaphalopathy- coma Liver biopsy Hepatic veinous wedge pressure assessment USG Doppler USG
- 28. Pharmacotherapy Betablockers- propanolol Betablockers+long acting nitrates(isosorbide 5-mononitrate) more effective than variceal ligation and alone betablockers.
- 29. Acute bleeding BT minimum 6 units Ballon tamponade Endoscopic band ligation Scleronizing agent injection Drugs- sphlenchic vasoconstrictor- somatostatin 250g iv bolus followed by continuous infusion 250g/hr 2-4 days Octreotide- 50g iv bolus, 25-50g/hr continuos infusion 2-4 days Combination of endoscopic procedure and octreotide injection is more effective
- 30. Vasopressin- 20 IU for 20 mins followed by 0.2-0.4 IU/min, used with Nitroglycerin- 40g/min and then titrted to achieve BP control. Adverse effect of vasopressin 1)MI 2) limb/mesenteric ischemia 3)Arrythemia
- 31. Terlipressin, Somatostatin,Octreotide are safer option and more effective. Vit.K injection 10mg IV IV olloid solution till BT is done TIPS Shunting
- 32. Yakrutodar /pittodar - / / // (../)
- 33. S/ // ../
- 34. - / // ../
- 35. - / // ../
- 36. / / // ../
- 37. / // ../ // ../
- 38. General features / / // ../
- 39. chikitsa repeatedly virechana madhura gana dravya siddha ghrita snehan and virechan with shyama,triphala,trivrutta siddha ghrita. Aasthapan basti and anuvasan basti- nyagrodhadi gana kashaya after mixing with adequate quantity of honey, sugar and ghrita. Upanaha prepared from payasa should be applied on abdomen Diet- Vidarigandhadi siddha payasa
- 40. Plihodara & yakrutodara Rx After performing snehan-swedan, patient is made to eat curd-rice and after consuming food siravedh is performed from left kurpar sandhi (elbow), medial side vein should be punctured. Massage gently on phliha to let more blood out. Yakrutodar- right kurpar sandhi Agnikarma- daha with shara after flexing left wrist joint, the vein which is heading towards the thumb.
- 41. After samyak shodhan- samudrashukti kshar with milk is given. Hingu + sarjikshar with milk internally Palash kshar and yavakshar together with milk Palashapushpa ksharodak with yavakshar. Parijatak+kekshuraka(talamkhana)+apamarga kshar Shobhanjana kwatha with taila, pipplai, saindhav and chitrak Putikaranja kshar mixed with kanji and vid-lavana and pipplai in large quantity. Shatpala ghrita Varangak kshara Yakrutphlihari loha