Live pulmonary endoscopy Interstitial and pleural diseases · 2015-09-18 · 26–30 September 2015...
96
ERS International Congress Amsterdam 26–30 September 2015 Live pulmonary endoscopy Interstitial and pleural diseases Thank you for viewing this document. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author. ©2015 by the author Tuesday, 29 September 2015 10:45 – 12:45 Room Auditorium RAI
Transcript of Live pulmonary endoscopy Interstitial and pleural diseases · 2015-09-18 · 26–30 September 2015...

ERS International Congress Amsterdam
26–30 September 2015
Live pulmonary endoscopy
Interstitial and pleural diseases
Thank you for viewing this document.
We would like to remind you that this material is the
property of the author. It is provided to you by the ERS
for your personal use only, as submitted by the author.
©2015 by the author
Tuesday, 29 September 2015
10:45 – 12:45
Room Auditorium RAI

You can access an electronic copy of these educational materials here:
http://www.ers-education.org/2015LE_ILD
To access the educational materials on your tablet or smartphone please find below a list of apps to
access, annotate, store and share pdf documents.
Apple iOS
Adobe Reader - FREE - http://bit.ly/1sTSxn3
With the Adobe Reader app you can highlight, strikethrough, underline, draw (freehand), comment
(sticky notes) and add text to pdf documents using the typewriter tool. It can also be used to fill out
forms and electronically sign documents.
Mendeley - FREE - http://apple.co/1D8sVZo
Mendeley is a free reference manager and PDF reader with which you can make your own searchable
library, read and annotate your PDFs, collaborate with others in private groups, and sync your library
across all your devices.
Notability - €3.99 - http://apple.co/1D8tnqE
Notability uses CloudServices to import and automatically backup your PDF files and allows you to
annotate and organise them (incl. special features such as adding a video file). On iPad, you can
bookmark pages of a note, filter a PDF by annotated pages, or search your note for a keyword.
Android
Adobe Reader - FREE - http://bit.ly/1deKmcL
The Android version of Adobe Reader lets you view, annotate, comment, fill out, electronically sign
and share documents. It has all of the same features as the iOS app like freehand drawing,
highlighting, underlining, etc.
iAnnotate PDF - FREE - http://bit.ly/1OMQR63
You can open multiple PDFs using tabs, highlight the text and make comments via handwriting or
typewriter tools. iAnnotate PDF also supports Box OneCloud, which allows you to import and export
files directly from/to Box.
ezPDF Reader - €3.60 - http://bit.ly/1kdxZfT
With the ezPDF Reader you can add text in text boxes and sticky notes; highlight, underline, or
strikethrough texts or add freehand drawings. Add memo and append images, change colour /
thickness, resize and move them around as you like.

Live pulmonary endoscopy
Interstitial and pleural diseases
AIMS: Interstitial lung diseases constitute a significant part of the workload of pulmonologists.
Sarcoidosis is the most prevalent interstitial lung disease and tissue confirmation is often needed.
Novel endoscopic techniques that yield peripheral lung tissue are available. The techniques that will
be demonstrated are bronchoscopy with BAL, cryobiopsies, EBUS, and EUS (B). Malignant and
infectious/inflammatory diseases are often associated with pleural diseases. Thoracoscopy is the
standard technique for diagnosing pleural diseases. The techniques that will be demonstrated are
flexible and rigid thoracoscopy.
CHAIRS: V. Poletti (Forli, Italy), N. M. Rahman (Oxford, United Kingdom)
SESSION PROGRAMME
10:45 Opening lecture: Endoscopy for sarcoidosis and ILD
V. Poletti (Forli, Italy)
Patient advocate (AMC)
E. van der Heijden (Nijmegen, Netherlands), O. Schuurbiers (Nijmegen, Netherlands)
Bronchoscopy, BAL, and cryobiopsy
J. Hetzel (Dusslingen, Germany), J. Daniels (Amsterdam, Netherlands)
EBUS-TBNA
R. Trisolini (Bologna, Italy) S. Gasparini (Ancona, AN, Italy)
EUS-B
M. Oki (Nagoya, Japan), J. Annema (Amsterdam, Netherlands)
Rigid thoracoscopy
J. Janssen (Nijmegen, Netherlands), M. Froudarakis (Alexandroupolis, Greece)
Flexible thoracoscopy
A. Rozman (Golnik, Slovenia), M. Munavvar (Preston, United Kingdom)
12:20 Interstitial and pleural diseases: live procedure question and answer session
V. Poletti (Forli, Italy), N. Rahman (Oxford, United Kingdom)
12:30 Concluding lecture: Role of thoracoscopy in pleural diseases
N. Rahman (Oxford, United Kingdom)
BOOKLET CONTENTS PAGE
Endoscopy for sarcoidosis and ILD 4
Thoracoscopy in Pleural Disease 42
Additional resources 84
Cryobiopsy increases the diagnostic yield of endobronchial biopsy: a multicentre trial 85
ATS/ERS/WASOG statement on sarcoidosis 91
Faculty disclosures 94
Faculty contact information 95

Endoscopy for sarcoidosis and ILD
Prof. Venerino Poletti
Department of Diseases of the Thorax
Ospedale G.B. Morgagni
Via Carlo Forlanini 34
47100 Forlì
ITALY
4

ENDOSCOPY FOR SARCOIDOSIS AND ILD
Venerino Poletti
Department of Diseases of the Thorax
Ospedale GB Morgagni, Forlì (I)
Department of Respiratory Diseases & Allergology
Aarhus University Hospital (DK)
5

Conflict of interest disclosure I have no, real or perceived, direct or indirect conflicts of interest that relate to
this presentation.
Affiliation / financial interest Nature of conflict / commercial company name
Tobacco-industry and tobacco corporate affiliate relatedconflict of interest
Grants/research support (to myself, my institution or department):
Roche, Boehringer Ing, Novartis, Chiesi
Honoraria or consultation fees: Roche, Boehringer Ing
Participation in a company sponsored bureau:
Stock shareholder:
Spouse/partner:
Other support or other potential conflict of interest:
This event is accredited for CME credits by EBAP and speakers are required to disclose their potential conflict of interest going back 3 years prior to this presentation. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgment. It remains for audience members to determine whether the speaker’s interests or relationships may influence the presentation.Drug or device advertisement is strictly forbidden.
6

INTRODUCTION
AIMS
• Aim 1
The best logic (and centered patient) approach to reach a
« morphological diagnosis »
• Aim 2
Knowledge of the complications using different approaches
• Aim 3
Skillness in organizing an Endoscopy Unit ables to meet all the
problems encountered using invasive procedures
7

• Pre-test probability (Thomas Byas)
• All guidelines recognize that their “one size fits all” recommendations may
not apply to individual patients. Increased attention is now being paid to
understand how best to adjust group-level clinical evidence of treatment
harms and benefits to account for the absolute level of risks faced by
subgroups and even individual patients, using, for example,
validated clinical risk scores.
8

ENDOSCOPY FOR SARCOIDOSIS/LDS
BAL
Bronchial Biopsy
Transbronchial lung biopsy
Conventional TBNA
EBUS/EUS
Cryo-TBB
9

Diagnostic Invasive Procedures in
Diffuse Infiltrative Lung Diseases
Respiration 2004;71:107–119 109
Alcian-negative material in alveolar lipoproteinosis, reac-
tive type II pneumocytes collected in pseudopapillae
around amorphous extracellular material in diffuse alveo-
lar damage (table1; fig. 1). The detection of bacteria or
viruses or fungi often after having used more sophisti-
cated microbiological investigations is not per se diagnos-
tic of pneumonia. In these cases the distinction between
pneumonia or colonization is based on the radiologic
aspects and the clinical background [19, 21].
Nonspecific findings in BAL fluid may be used as an
adjunct to diagnosis together with an extensive clinical
and roentgenological investigation (table2) [10, 22–24].
In drug- or radiation-related toxicity besides hyperplastic/
dysplastic changes of type II pneumocytes and negative
microbiological investigations, any type of alveolitis has
been described in BAL fluid. However, morphologically
activated CD8+ cells indicating a hypersensitivity reac-
tion are the most frequent and suggestive occurrence. Cel-
lular interstitial pneumonitis as clinicopathological mani-
festation of GVHD in the lungs may be inferred on the
basis of negative pertinent microbiological investigations
and CD8+ cell lymphocytosis in BAL fluid [24–26].
Application of deep sedation and use of the laryngeal
mask appear to be a safe and effective alternative to intu-
bation for accomplishing fiberoptic bronchoscopy with
BAL in patients (adults and children) with suspected
pneumonia and severe hypoxemia [27–29]. Protected
brushing or lavage has a lower diagnostic yield and speci-
ficity because they do not allow to correlate microbiologi-
cal data with the cytological profile detectable in the respi-
ratory airways and brushing is associated with a higher
incidence of side effects [19]. HRCT patterns that have
been shown to predict a high diagnostic yield of BAL pro-
cedure are [10, 18, 23, 26]: alveolar and/or ground-glass
opacities (nonspecific patterns observed more frequently
in infections, drug-induced toxicity, organizing pneumo-
nia, alveolar hemorrhage and diffuse alveolar damage),
‘tree in bud pattern’ (more typically observed in bron-
chiolitis and peribronchiolitis of infectious cause, i.e.
tuberculosis, lobular pneumonitis), nodular or reticulo-
nodular pattern with a perilymphatic distribution (typi-
cally observed in lymphomatous infiltration and carcino-
matous lymphangitis), and escavated nodules (usually of
infectious nature) [24, 30]. A conclusive diagnosis is not
obtained in the minority by BAL fluid analysis. In these
cases transbonchial lung biopsy or even open lung biopsy
has to be considered.
Transbronchial lung biopsy (TBB) is a procedure
where pneumothorax is a not very frequent morbidity and
significant bleeding a more dangerous and frequent side
Table 1. Diagnoses feasible on the basis of BAL findings in immuno-
compromised patients
P. carinii pneumonia
Mycobacteriosis
Legionellosis
Viral pneumonitis (intranuclear and intracytoplasmic inclusions)
Diffuse alveolar damage (reactive type II pneumocytes and
amorphous extracellular material)
Alveolar proteinosis
Eosinophilic pneumonia
Alveolar hemorrhage
Epithelial neoplastic cells
Lymphoid atypical cells (cytological or phenotypical aspects)
Myeloid cells
Table 2. Diagnoses feasible on the basis of BAL findings in immuno-
competent patients
Dust exposure (asbestos bodies, silica)
Alveolar proteinosis
Lipoid pneumonia
Chronic eosinophilic pneumonia
Acute eosinophilic pneumonia
Diffuse alveolar damage
Alveolar hemorrhage
Langerhans cell histiocytosis
Bronchoalveolar cell carcinoma
Carcinomatous lymphangitis
Hematogenous metastases
Low-grade B cell lymphoma, MALT type
Microlithiasis
Gaucher and Niemann-Pick cells
Intracytoplasmic inclusions in Hermansky-Pudlak disease
effect (seen however in ! 3% of cases) [31]. In cases in
which a TBB is deemed necessary and is feasible (absence
of significant coagulopathy, platelet 150,000) broncho-
scopic procedures should be performed under general
anesthesia through a rigid bronchoscope or an oro- or
nasotracheal tube under fluoroscopic control in order to
better control ventilation and bleeding [32]. In this way
the bioptic forceps are not passed through the operating
channel of the fiberoptic bronchoscope and therefore, the
samples, frequently larger than the tip of the forceps, are
not crushed (fig. 2). Combined BAL and TBB may also
be performed safely in mechanically ventilated patients
[33].
Nonspecific pathological changes are common in TBB
specimens in these patients but if they are interpreted in
Dow
nlo
ade
d b
y:
Sta
tsb
iblio
teket
149
.126
.75.1
- 7
/28/2
01
5 1
:20
:44 P
M
Diagnostic Invasive Procedures in
Diffuse Infiltrative Lung Diseases
Respiration 2004;71:107–119 109
Alcian-negative material in alveolar lipoproteinosis, reac-
tive type II pneumocytes collected in pseudopapillae
around amorphous extracellular material in diffuse alveo-
lar damage (table1; fig. 1). The detection of bacteria or
viruses or fungi often after having used more sophisti-
cated microbiological investigations is not per se diagnos-
tic of pneumonia. In these cases the distinction between
pneumonia or colonization is based on the radiologic
aspects and the clinical background [19, 21].
Nonspecific findings in BAL fluid may be used as an
adjunct to diagnosis together with an extensive clinical
and roentgenological investigation (table2) [10, 22–24].
In drug- or radiation-related toxicity besides hyperplastic/
dysplastic changes of type II pneumocytes and negative
microbiological investigations, any type of alveolitis has
been described in BAL fluid. However, morphologically
activated CD8+ cells indicating a hypersensitivity reac-
tion are the most frequent and suggestive occurrence. Cel-
lular interstitial pneumonitis as clinicopathological mani-
festation of GVHD in the lungs may be inferred on the
basis of negative pertinent microbiological investigations
and CD8+ cell lymphocytosis in BAL fluid [24–26].
Application of deep sedation and use of the laryngeal
mask appear to be a safe and effective alternative to intu-
bation for accomplishing fiberoptic bronchoscopy with
BAL in patients (adults and children) with suspected
pneumonia and severe hypoxemia [27–29]. Protected
brushing or lavage has a lower diagnostic yield and speci-
ficity because they do not allow to correlate microbiologi-
cal data with the cytological profile detectable in the respi-
ratory airways and brushing is associated with a higher
incidence of side effects [19]. HRCT patterns that have
been shown to predict a high diagnostic yield of BAL pro-
cedure are [10, 18, 23, 26]: alveolar and/or ground-glass
opacities (nonspecific patterns observed more frequently
in infections, drug-induced toxicity, organizing pneumo-
nia, alveolar hemorrhage and diffuse alveolar damage),
‘tree in bud pattern’ (more typically observed in bron-
chiolitis and peribronchiolitis of infectious cause, i.e.
tuberculosis, lobular pneumonitis), nodular or reticulo-
nodular pattern with a perilymphatic distribution (typi-
cally observed in lymphomatous infiltration and carcino-
matous lymphangitis), and escavated nodules (usually of
infectious nature) [24, 30]. A conclusive diagnosis is not
obtained in the minority by BAL fluid analysis. In these
cases transbonchial lung biopsy or even open lung biopsy
has to be considered.
Transbronchial lung biopsy (TBB) is a procedure
where pneumothorax is a not very frequent morbidity and
significant bleeding a more dangerous and frequent side
Table 1. Diagnoses feasible on the basis of BAL findings in immuno-
compromised patients
P. carinii pneumonia
Mycobacteriosis
Legionellosis
Viral pneumonitis (intranuclear and intracytoplasmic inclusions)
Diffuse alveolar damage (reactive type II pneumocytes and
amorphous extracellular material)
Alveolar proteinosis
Eosinophilic pneumonia
Alveolar hemorrhage
Epithelial neoplastic cells
Lymphoid atypical cells (cytological or phenotypical aspects)
Myeloid cells
Table 2. Diagnoses feasible on the basis of BAL findings in immuno-
competent patients
Dust exposure (asbestos bodies, silica)
Alveolar proteinosis
Lipoid pneumonia
Chronic eosinophilic pneumonia
Acute eosinophilic pneumonia
Diffuse alveolar damage
Alveolar hemorrhage
Langerhans cell histiocytosis
Bronchoalveolar cell carcinoma
Carcinomatous lymphangitis
Hematogenous metastases
Low-grade B cell lymphoma, MALT type
Microlithiasis
Gaucher and Niemann-Pick cells
Intracytoplasmic inclusions in Hermansky-Pudlak disease
effect (seen however in ! 3% of cases) [31]. In cases in
which a TBB is deemed necessary and is feasible (absence
of significant coagulopathy, platelet 150,000) broncho-
scopic procedures should be performed under general
anesthesia through a rigid bronchoscope or an oro- or
nasotracheal tube under fluoroscopic control in order to
better control ventilation and bleeding [32]. In this way
the bioptic forceps are not passed through the operating
channel of the fiberoptic bronchoscope and therefore, the
samples, frequently larger than the tip of the forceps, are
not crushed (fig. 2). Combined BAL and TBB may also
be performed safely in mechanically ventilated patients
[33].
Nonspecific pathological changes are common in TBB
specimens in these patients but if they are interpreted in
Dow
nlo
ade
d b
y:
Sta
tsb
iblio
teke
t
149
.126.7
5.1
- 7
/28
/201
5 1
:20:4
4 P
M
114 Respiration 2004;71:107–119 Poletti/Chilosi/Olivieri
Table 3. Disease with nonspecific but characteristic BAL profile
Disease Features
Sarcoidosis Increased CD4/CD8 ratioa
Hypersensitivity pneumonitis Increased total cell count, lymphocytosis, mast cells,
plasma cells, decreased CVD4/CD8 ratiob
Organizing pneumonia Lymphocytosis, scattered neutrophils and eosinophils,
plasma cells, decreased CD4/CD8 ratiob
Nonspecific interstitial pneumonitis (cellular variant) Lymphocytosis (decreased CD4/CD8 ratio)
Respiratory bronchiolitis-ILD/desquamative interstitial
pneumonitis
Increased total cell count, brown macrophages, slight
increase of neutrophils
Giant cell interstitial pneumonitis Multinucleated giant cell, ‘cannibalistic’ figures
Bacterial pneumonia Neutrophils, apoptotic nuclei, intracytoplasmic micro-
organisms
ILD = Interstitial lung disease.a CD4/CD8 ratio may also be increased in berylliosis, tuberculosis, asbestosis, Crohn’s disease, rheumatoid
arthritis.b The differential diagnosis between hypersensitivity pneumonitis and organizing pneumonitis is often not feasible
on the basis of BAL features only.
From the morphological point of view the pattern called
nonspecific interstitial pneumonia (NSIP), cellular vari-
ant is quite characteristic (maintenance of pulmonary
architecture, interstitial thickening due to mononuclear
cell infiltration, cuboidal type II metaplasia) but it is clini-
cally nonspecific being observed in cases of collagen vas-
cular disease (inflammatory myositis in particular), in
patients with drug-related toxicity, in GVHD-related lung
damage, and, in a minority of cases, it is of unknown
cause (idiopathic NSIP) [56]. Surgical lung biopsy is con-
sidered the best way to obtain enough tissue to demon-
strate this pattern. However, generous TBB may provide
good specimens for a morphological diagnosis. This
pathological diagnosis is acceptable in specific clinical set-
tings (polymyositis-dermatomyositis-related interstitial
lung disease, drug toxicity) but it might also be of clinical
value in cases of unknown etiology [57]. RB is at last easi-
ly recognizable in TBB specimens and nowadays the utili-
ty of surgical lung biopsy in the diagnosis of RB-associat-
ed interstitial lung disease is disputable and probably ethi-
cally not advisable.
The role of the number of specimens obtained and of
the size of the forceps used has not been evaluated in
detail in the literature. Descombes et al. [54] reviewed the
histological and clinical data of 530 consecutive TBBs
performed in 516 immunocompetent patients, having
either a chronic diffuse lung infiltrate, a localized periph-
eral lung lesion or hilar adenopathies. The authors have
shown that there is a direct correlation between the num-
ber of samples obtained per TBB and the overall diagnos-
tic yield (i.e. 38% with one to three tissue fragments vs.
69% with six to ten, p ! 0.01). They recommend that at
least five to six specimens per TBB should be taken, the
optimal number of specimens to optimize the diagnostic
yield being, however, seven to ten. Curley et al. [58]
reported that larger biopsy specimens were more likely to
contain diagnostic tissue (r = 0.29, p = 0.001). Cup forceps
retrieved smaller pieces of tissue (p = 0.007) and were less
likely to obtain diagnostic tissue (p = 0.06). Specimens
that floated were no more likely to be diagnostic or abnor-
mal than specimens that sank (p ! 0.05). Loube et al. [59]
prospectively compared the diagnostic yield of transbron-
chial biopsies using large and small forceps (cup sizes, 3 !
2 ! 0.9 vs. 2 ! 1.5 ! 0.6 mm, respectively). Large for-
ceps obtained significantly more tissue than did small for-
ceps [20 of 27 patients (74%) vs. 5 of 27 patients (19%),
p ! 0.005]. Also, large forceps obtained significantly more
alveolar tissue than did small forceps [16 of 22 patients
(73%) vs. 6 of 22 patients (27%), p ! 0.05, with no alveo-
lar tissue obtained in 5 patients]. If larger forceps are not
withdrawn through the operative channel, crash artifacts
may also be avoided. Becker et al. [60] and Casoni et al.
Dow
nlo
ade
d b
y:
Sta
tsb
iblio
teke
t
149.1
26.7
5.1
- 7
/28
/201
5 1
:20:4
4 P
M
Respiration 2004
10

– TBB forceps reach the alveolar structures through bronchi/bronchioles
They sample mostly the centrilobular zones
11

12

Yield of TBB
• Interstit. lung disease 60-80 %
• Sarcoidosis up to 90%
• Solitary nodule < 2 cm low
• Solitary nodule 2-4 cm 50-60 %
• Solitary nodule > 4 cm ca 80%
13

ERJ 2012
HRCT features may predict bronchial/TBB diagnostic yield in sarcoidosis/ILDs
14

UIP in TBB: Results
Tomassetti S et al, 2012
15

E
B
U
S
E
U
S
16

6
SpleenLeft adrenalglandKidney
Liver
5
17

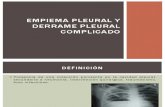
JAMA 2013
Trisolini R, 2015. Endobronchial ultrasound-guided transbronchial
needle aspiration for diagnosis of sarcoidosis in clinically unselected
study populations
The median prevalence of sarcoidosis was 15%. EBUS-TBNA had a pooled
diagnostic yieldof 0.79 (standard deviation, 0.24), a pooled sensitivity
of 0.84 (95% confidence interval (CI), 0.79–0.88) and a pooled specificity of
1.00 (95% CI, 0.99–1.00). 18

C
E
L
L
B
L
O
C
K
S
L
I
D
E
19

Plit ML 2013
Cancellieri A 2013
Sarcoidal Granulomas in Cytology Specimens
Respiration 2013;85:244–251 247
0.522); p = 0.071], and are significantly more likely to have giant cells (59 vs. 38%; p = 0.005).
We did not find any significant correlation between any of the morphologic parameters of the granuloma de-scribed above and the needle size used ( table 3 ) or the patients’ age (data not shown).
Discussion
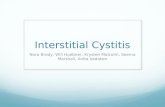
The main finding of the present study is that the mor-phologic characteristics of granulomas allow them to be easily and reliably identified on the cytological material obtained with TBNA. Sarcoidal granulomas ( fig. 1 a–d)
appear as tiny ‘nodules’ consisting of a tight aggregate of epithelioid histiocytes. These nodules, which are easily appreciated even at low power, are well defined, round or elliptical in shape, and have a regular contour in most cases. Their background is usually clean, with only a mi-nority of cases showing a hemorrhagic background. A necrotic, ‘dirty’ background was the only morphologic finding which proved specific enough to suggest a tuber-cular etiology of the granulomatous inf lammation over a sarcoidal one in the present series, as already observed by Fritscher-Ravens et al. [14, 25] in two studies aimed at as-sessing the role of EUS-NA in sarcoidosis and tuberculo-sis. It should be kept in mind, however, that the presence of a necrotic background is useful only when present, as
a b
c d
Fig. 1. TBNA cytological smears obtained from mediastinal sar-coidal lymph nodes. a Granulomas appear as well-defined nod-ules, ‘popping out’ of the slide (arrows). The background shows numerous lymphocytes and absence of necrotic debris or exudate. May-Grünwald-Giemsa. ! 40. b A granuloma at a higher magni-fication shows a regular contour, with a tight aggregation of epi-
thelioid histiocytes, with many having twisted nuclei. Papanico-laou. ! 400. c A multinucleated giant cell (arrow) is visible at the edge of an elliptical granuloma. May-Grünwald-Giemsa. ! 200. d Strands of fibrosis (arrows), along with several granulomas. Pa-panicolaou. ! 40.
Co
lor vers
ion
availab
le o
nlin
e
Do
wnlo
aded
by:
87
.21.2
45.2
09
- 5
/17/2
01
5 3
:47:2
7 P
M
Fax +41 61 306 12 34E-Mail [email protected]
Interventional Pulmonology
Respiration 2013;85:244–251
DOI: 10.1159/000345386
Sarcoidal Granulomas in Cytological Specimens from Intrathoracic Adenopathy: Morphologic Characteristics and Radiographic Correlations
Alessandra Cancellieri b Kevin O. Leslie a Carmine Tinelli d Marco Patelli c
Rocco Trisolini c
a Department of Laboratory Medicine and Pathology, Mayo Clinic Arizona, Scottsdale, Ariz. , USA;
b Anatomic Pathology Unit and c Thoracic Endoscopy and Pulmonology Unit, Maggiore Hospital, Bologna , and
d Clinical Epidemiology and Biometry Service, IRCCS Policlinico San Matteo, Pavia , Italy
ments lacked necrotic debris or exudate. The density [me-
dian (IQR) number of granulomas per slide: 6.85 (3.66–11) vs.
5.25 (2.5–8), p = 0.073] and size [median (IQR) largest diam-
eter: 0.51 (0.319–0.733) vs. 0.398 (0.318–0.522), p = 0.071]
tended to be larger in stage I than in stage II sarcoidosis. A
necrotic background was common in the tuberculosis co-
hort studied (79 vs. 0%, p ! 0.0001). Conclusions: Granulo-
mas can be reliably identified on TBNA cytological material
once their characteristic cytomorphology is delineated. A
higher density of granulomas in lymphadenopathy of stage
I sarcoidosis patients could partly explain the higher success
rate constantly obtained by TBNA and EBUS-TBNA in this
stage of the disease. A necrotic background suggests a tu-
bercular etiology of the granulomas over a sarcoidal one, in
the appropriate clinical set ting.
Copyright © 2012 S. Karger AG, Basel
Introduction
Sarcoidosis is a multisystem disorder whose diagnosis is one of exclusion and is thought to be more accurate if the clinical and radiological suspicion is corroborated by the demonstration of nonnecrotizing granulomatous in-f lammation in at least one involved organ [1, 2] .
Key Words
Cytology Granuloma Lymphadenopathy Sarcoidosis
Transbronchial needle aspiration Endobronchial
ultrasound-guided transbronchial needle aspiration
Tuberculosis
Abstract
Background: Clinical experience and literature data suggest
that the ability of pathologists to identify granulomas in cy-
tological specimens from intrathoracic lymphadenopathy
varies considerably and may negatively influence the yield
of transbronchial needle aspiration (TBNA), both conven-
tional and ultrasound-guided (EBUS-TBNA). Objectives: To
describe the cytomorphology of sarcoidal granulomas on
TBNA cytology specimens and to analyze the presence of as-
sociations between the cytological characteristics of granu-
lomas and the radiographic stage of sarcoidosis. Methods:
TBNA cytological specimens from 123 sarcoidosis patients
and 14 tuberculosis patients (control population) were re-
viewed independently by two pathologists blinded to the
clinical-radiological details. Results: Sarcoidal granulomas
were small [median (IQR) largest diameter: 0.478 (0.318–
0.701) mm] and well-formed, round or elliptical in shape, and
almost invariably had a regular contour. Background ele-
Received: August 18, 2012
Accepted after revision: October 22, 2012
Published online: December 29, 2012
Rocco Trisolini, MD Thoracic Endoscopy and Pulmonology Unit, Maggiore Hospital Largo B. Nigrisoli 2 IT–40133 Bologna (Italy) E-Mail rocco.trisolini @ ausl.bologna.it
© 2012 S. Karger AG, Basel0025–7931/13/0853–0244$38.00/0
Accessible online at:www.karger.com/res
Do
wnlo
ad
ed b
y:
87
.21.2
45
.209
- 5
/17
/2015
3:4
7:2
7 P
M
ROSE
sensitivity 87.8%
specificity 91%
PPV 97.7%
20

Diagnosis and Subt yping of De Novo andRelapsed Mediast inal Lym phom as byEndobronchial Ult rasound Needle Aspirat ion
Mufaddal T. Moonim1, Ronan Breen2, Paul A. Fields3, and George Sant is4
1Department of Cellular Pathology, 2Department of Respiratory Medicine, and 3Division of Haemato-oncology, Guy’s and St Thomas’ NHS
Foundation Trust, London, United Kingdom; and 4Division of Asthma, Allergy and Lung Biology, King’s College London, London, United Kingdom
Rationale: The current management of lymphoma requires accurate
diagnosis and subtyping of de novo lymphoma and of relapsed or
refractory lymphoma in known cases. The role of endobronchial
ultrasound-guided transbronchial needle aspirat ion (EBUS-TBNA)
in the clinical management of lymphomas is unclear.
Objectives: To invest igate the use of EBUS-TBNA in the diagnosis of
de novo and relapsed mediast inal lymphomas.
Methods: A total of 2,256 consecut ive pat ients who underwent
EBUS-TBNA in a tertiary center between February 2008 and April
2013 were prospectively evaluated. The diagnost ic accuracy and clini-
cal use of EBUS-TBNA in 100 cases of de novo or suspected relapsed
mediastinal lymphoma was investigated by comparing EBUS-TBNA
diagnosis with the final diagnosis.
Measurements and Main Results: De novo mediast inal lymphoma was
correct ly diagnosed by EBUS-TBNA in 45 (88%) of 51 and relapsed
lymphoma in 15 (100%) of 15 lymphoma cases. EBUS-TBNA accu-
rately established a diagnosis other than lymphoma in 32 (97%) of
33 pat ients with suspected lymphoma relapse. Sensit ivity, specific-
ity, posit ive predict ive value, negat ive predict ive value, and accu-
racy of EBUS-TBNA in the diagnosis of mediast inal lymphoma were
89%,97%, 98%, 83%, and 91%, respectively. Sensit ivity of EBUS-TBNA
in subtyping lymphomas into high-grade non-Hodgkin lymphoma,
low-grade non-Hodgkin lymphoma, and Hodgkin lymphoma was
90%, 100%, and 79%, respectively. EBUS-TBNA diagnosis was ade-
quate for clinical management in 84 (84%) of 100 cases.
Conclusions: Mult imodality evaluat ion of EBUS-TBNA can be success-
ful in the diagnosis of de novo mediast inal lymphomas and is ideally
suited in dist inguishing lymphoma relapse from alternat ive pathol-
ogies; it is least sensit ive in subtyping Hodgkin lymphoma.
Keywords: lymphoma; fine-needle aspiration; cytology; endobronchial
ultrasound
Lymphomas account for 20% of primary mediastinal tumors inadultsand involvement of mediastinum by systemic lymphoma is
common (1). The diagnosis and classification of lymphoma no
longer relies on pure morphologic characteristics of tissue speci-mens. The World Health Organization recommends the use ofa mixture of diagnostic modalities (cytomorphology, immuno-
phenotype, cytogenetics, and molecular features) for accuratesubclassification (2). A s a consequence, fine-needle aspiration
cytology (FNA C) has received attention as an alternative tohistology on excisional or core biopsies, which represent the
gold standard for lymphoma diagnosis (3–8). The developmentof endobronchial ultrasound (EBUS), which allows ultrasound-
guided aspiration of mediastinal and pulmonary lymph nodes
and masses (EBUS transbronchial needle aspiration [TBNA ]),offers the opportunity to incorporate FNA C to the diagnosis
and management of mediastinal lymphoid neoplasms, whichhad hitherto required sampling by more invasive techniques,
such as mediastinoscopy, mediastinotomy, or surgical thoraco-scopy. A lthough there is support for the use of EBUS-TBNA in
lung cancer (9–12) and in the evaluation of isolated mediastinallymphadenopathy (13), there is limited information of its value
in the diagnosis and management of lymphoma (14–18). Theability of FNA C in general (5) and EBUS-TBNA specifically
(14, 18) to correctly diagnose and subtype lymphoma has beenquestioned. In this study we investigated the accuracy of diag-nosis and subtyping of mediastinal lymphoma by multimodality
evaluation of EBUS-TBNA and assessed its role in the investi-gation of suspected lymphoma relapse.
METHODS
A ll patients who underwent EBUS-TBNA in a tertiary center between
February 2008 and A pril 2013 were prospectively evaluated to assessthe
diagnostic accuracy and clinical use of EBUS-TBNA in casesof denovo
and suspected relapsed mediastinal lymphoma.
EBUS-TBNA was performed by two consultant pulmonologists as
previously described (19–21). The size, nodal station, and number of
aspirates for each node sampled were recorded in real-time. A biomed-
ical scientist prepared EBUS-derived aspirates for rapid on-site morpho-
logic evaluation of air-dried smears by a consultant cytopathologist, who
provided real-time assessment of the aspirates and allowed triage of cell
suspensions for diagnostic tests(Figure 1) (19–21). The same cytopathologist
(Received in original form March 10, 2013; accepted in final form August 26, 2013)
Supported in part by the Department of Health via the National Institutes of
Health Research comprehensive Biomedical Research Centre award to Guy’s
and St Thomas’ National Health Service Foundation Trust in partnership with
King’s College London (G.S.).
Author Contributions: Conception and design, G.S. and M.T.M. Analysis and in-
terpretation, M.T.M., R.B., P.A.F., and G.S. Endobronchial ultrasound was per-
formed by G.S. and R.B., M .T.M . reviewed all pathology. Draft ing the
manuscript, G.S. Contribution to final manuscript, M.T.M., R.B., P.A.F., and G.S.
Correspondence and requests for reprints should be addressed to George Santis,
M.D., Division of Asthma, Allergy and Lung Biology, King’s College London, 5th
Floor Tower Wing, Guy’s Hospital Campus, London SE1 9RT, UK. E-mail: george.
This article has an online supplement, which isaccessible from this issue’s table of
contents at www.atsjournals.org
Am J Respir Crit Care Med Vol 188, Iss. 10, pp 1216–1223, Nov 15, 2013
Copyright ª 2013 by the American Thoracic Society
Originally Published in Press as DOI: 10.1164/ rccm.201303-0462OC on September 18, 2013
Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY
Scient ific Knowledge on the Subject
The role of endobronchial ultrasound transbronchial needleaspiration in lymphoma diagnosis and management has not
been established.
What This Study Adds to the Field
This study demonstrates that this minimally invasive tech-nique can be used in the diagnosis and management ofmediastinal lymphoma, thereby obviating the need for
more invasive surgical biopsies.
AJRCCM, 2013
21

E-Mail [email protected]
Review
Respiration 2014;87:343–351
DOI: 10.1159/000357066
Complication Rate of Endosonography (Endobronchial and Endoscopic Ultrasound): A Systematic Review
M.B. von Bartheld a A. van Breda a J.T. Annema a, b
a Department of Pulmonology, Leiden University Medical Center, Leiden , and b Department of Pulmonology,
Amsterdam Medical Center, Amsterdam , The Netherlands
(0.14%) and 35 AE (0.22%) were reported. No mortality was
observed. SAE were more frequent in patients investigated
with EUS (0.30%) than in those investigated with EBUS
(0.05%). Infectious SAE were most prevalent (0.07%) and pre-
dominantly occurred in patients with cystic lesions and sar-
coidosis. In lung cancer patients, complications were rare.
Discussion: Endosonography for intrathoracic nodal assess-
ment seems safe for lung cancer patients and mortality has
not been reported. For cystic lesions and sarcoidosis, there
may be a small, but nonnegligible risk of infectious compli-
cations. The true incidence of SAE might be higher as accu-
rate documentation of complications is missing in most
studies. © 2014 S. Karger AG, Basel
Introduction
In patients with lung cancer, endosonography is the method of choice for intrathoracic nodal staging ac-cording to current guidelines [1, 2] . Additionally, it seems the diagnostic method of choice for the assess-ment of sarcoidosis [3, 4] . Several – mainly infectious (mediastinitis/abscess formation) – severe adverse events (SAE) have been reported in the literature raising
Key Words
Adverse events · Complication rate · Cysts · Endobronchial
ultrasonography · Endoscopic ultrasonography ·
Fine needle aspiration · Mediastinum · Sarcoidosis ·
Transbronchial needle aspiration · Ultrasound
Abstract
Background: Endosonography [endoscopic ultrasound
(EUS)-guided fine needle aspiration and endobronchial ul-
trasound (EBUS)-guided transbronchial needle aspiration] is
increasingly used for lung cancer staging and the assess-
ment of sarcoidosis. Serious adverse events (SAE) have been
reported in case reports, but the true incidence of complica-
tions is yet unknown. Objectives: To assess the rate of SAE
related to endosonography and to investigate associated
risk factors. Materials and Methods: PubMed, EMBASE and
Cochrane libraries were searched for eligible references up
to April 2012 and these included studies reporting on linear
EUS or EBUS for the analysis of mediastinal/hilar nodal or
central intrapulmonary lesions. Case series describing com-
plications were excluded. Reported complications were clas-
sified into SAE or minor adverse events (AE). Results: 190
studies met the inclusion criteria. Information on follow-up
was missing in half of the studies. In 16,181 patients, 23 SAE
Received: August 19, 2013
Accepted after revision: October 24, 2013
Published online: January 16, 2014
J.T. Annema, MD, PhD Department of Pulmonology, Academic Medical Center, University of Amsterdam PO Box 22700 NL–1100 DE Amsterdam (The Netherlands) E-Mail j.t.annema @ amc.nl
© 2014 S. Karger AG, Basel0025–7931/14/0874–0343$39.50/0
www.karger.com/res
Dow
nlo
ade
d b
y:
87.2
1.2
45.2
09 -
5/1
6/2
015 3
:37
:10 P
M
2014
16,181 pts
*Serious adverse events 23 (0.14%)
EUS 0.30%
EBUS 0.05%
*Infectious SAE were most prevalent (0.07%) and
pre- dominantly occurred in patients with cystic lesions
and
sarcoidosis
*Mortality 0
22

Li K, Jiaang S. A randomized controlled study of conventional TBNA
versus EBUS-TBNA for diagnosis of suspected stage I and II sarcoidosis.
Li K1, Jiang S.
The overall diagnostic yield of EBUS-TBNA for stage I and II sarcoidosis
was higher than TBNA.
However, conventional TBNA has very high diagnostic yield,similar to
EBUS-TBNA, if
*the lymph nodes located on the 4th and 7th group
*the shortest diameter was greater than 15 mm.
23

TRANSBRONCHIAL CRYOBIOPSY
• Poletti V, Respirology 2014• Babiak A, Respiration 2009
24

25

TRANSBRONCHIAL CRYOBIOPSY IN DLD:
DIAGNOSTIC YIELD
AUTHOR (year) Mean specimen area Diagnostic yield (%) UIP (%)
Babiak A (2009) 5.82 mm2 95 (39/41) 37
Pajares V (2010) 9.5 mm2 50 (5/10) 0
Kropski JA (2013) 64.2 mm2 76 (19/25) 28
Yarmus L (2013) 10 mm2 NA 0
Frutcher O (2013) 9 mm2 100 (15/15) 0
Frutcher O (2013) 10 mm2 100 (40/40) 0
Fruchter O (2014) 9 mm2 68 (51/75) 9
Pajares V (2014) 14.7 mm2 74.4 (29/39) 18
Casoni G-Poletti V (2014)
39 mm2 86 (63/73) 64
Poletti V (2014) NA 80 (141/176) 34
NA= not available26

PlosOne- 2014
27

INCLUSION CRITERIA
• Patients had to be at least 18 years old,
• Forced vital capacity (FVC) > 50% of predicted normal value
• Diffusing capacity for carbon monoxide (DLco) >30% of predicted
normal value
• Pulmonary systolic arterial pressure estimated by
echocardiography< 40 mmHg
EXCLUSION CRITERIA
• Coagulopathy (Plts<70,000x109/L, INR>1,5)
• FEV1<0.8 L
• Bullous disease
• Hemodynamic instability
• Severe hypoxemia (PaO2< 55 mmHg on room air)
28

Cryobiopsy: UIP with high confidence
29

INTEROBSERVER AGREEMENT for the presence of honeycombing features (Kappa )
0.64 (95% CI 0.42-0.86)
INTEROBSERVER AGREEMENT for the presence of fibroblast foci features (Kappa)
0.50 (95% CI 0.30-0.70)
INTEROBSERVER AGREEMENT for the presence of patchy fibrosis. features (Kappa)
0.59 (95% CI 0.40-0.78)
INTEROBSERVER AGREEMENT FOR
PATHOLOGIC FEATURES OF UIP
30

Cryo-TBB/UIP
hsp27
Sandwich
foci
Tubb3
CK5
31

CLINICAL ROLE OF
CRYO-TBB
32

2008 2009 2010 2011 2012 2013 Total
New IPF diagnoses 36 27 26 55 40 52 236
N % N % N % N % N % N % NAge: median
(Range)Y
CRYO 0 0% 0 0% 0 0% 22 40% 18 45% 24 46% 64 62 (33-78)
SLB 15 42% 8 30% 7 27% 3 5% 3 8% 7 13% 43 57 (42-74)
Cases with
cryoTBB+SLB 0 0 0 0 2 4 6
Bioptic approach to “IPF Patients”: from SLB to Cryo TBB
Biopsy confirmed IPF
SLB 42% in 2008
13% in 2013
33

TRANSBRONCHIAL FORCEPS VS.
CRYOBIOPSY
34

Tomassetti S, et al. Submitted35

AuthorsArea
(mm2)UIP (%) PNX (%) Pleura (%)
Poletti V (2014) Nr 34 23 Nr
Pajares V [2014] 15 18 8 Nr
Fruchter O [2014] 9 9 3 Nr
Casoni GL-Poletti V [2014] 39 64 (75) 27 33
Yarmus L [2013] 10 0 6 0
Kropski JA [2013] 64 32 0 Nr
Babiak A [2009] 15 Nr 8 Nr
Nr: not reported
PNX: RATE & WHY?
36

The incidence of pneumothorax might be linked
to:
•Biopsies </= 1 cm from the pleura
•UIP pattern/HRCT fibrotic score
•Bronchoscopist’s skillness
•Dimensions/number of samples (??)
37

Author Year OT-Tube RB L Mask No Int GA+JV GA/DS LA Bronchialblocker
Cryoprobesize
Freezingtime
Babiak 2009 x x N 2.4 4
Pajares 2010 x x N 2.4 3
Griff 2011 x x x x
Kropski 2013 x x 1.9 4
Yarmus 2013 X (10) X (11) x x Y 1.8 3
Frutcher 2013 x x N 2.4 4
Frutcher 2013 x x N 2,4 4
Frutcher 2014 x x N 2.4 4
Sastre 2014 x x Y 2.4
Casoni 2014 x x Y 2.4 5/6
Pajares 2014 x x Y 2.4 3/4
Poletti 2014 x x Y 2.4 5/6
Griff 2014 x X x x N 1.9 3/5
Gershman 2015 x x N 2.4 4
Hagmeyer 2015 x x x N 2.4 4/5
HernandezGonzalez
2015 X X Y 1.9 3/4 38

NEED TO STANDARDIZE THE PROCEDURE
Poletti V, Hetzel J, submitted
Flexible bronchoscope with no intubation
Orotracheal tube
Rigid tracheoscope
Fogarty balloon (or other balloons)
Cryoprobe 2.4 vs 1.9
Bioptic sites/distance from the pleura/freezing time 39

CRYO-TBB IS A VALID COMPETITOR OF SURGICAL LUNG BIOPSY IN ILDS40

TAKE HOME MESSAGE
*BAL : may be considered an ancillary
diagnostic tool
*Conventional B/TBB: mainly useful
in “perilymphatic” and peribronchial
disease (as documented by HRCT)
*EBUS/EUS:the diagnostic yield
for stage I and II sarcoidosis is high
*Cryo-TBB: a novel lung bioptic
procedure useful in “fibrotic”
parenchymal disease
*Cryo-TBB a valid surrogate
of surgical lung biopsy
41

Thoracoscopy in Pleural Disease
Dr Najib Rahman
Oxford Centre for Respiratory Medicine
Churchill Hospital
Old Road
Headington
Oxford OX3 7LJ
UNITED KINGDOM
42

Oxford
Pleural
Unit
Najib M Rahman
Consultant and Senior Lecturer
Oxford Centre for Respiratory Medicine
University of Oxford
ERS Live Pulmonary Endoscopy
Thoracoscopy in Pleural Disease
43

Oxford
Pleural
Unit
I have no real or perceived conflicts of interest that relate to this presentation:
This event is accredited for CME credits by EBAP and EACCME and speakers are required to disclose their potential conflict of interest. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for audience members to determine whether the speaker’s interests, or relationships may influence the presentation. The ERS does not view the existence of these interests or commitments as necessarily implying bias or decreasing the value of the speaker’s presentation. Drug or device advertisement is forbidden.
44

Oxford
Pleural
Unit Overview
• Indications for thoracoscopy
• Specific conditions:
– Malignant effusion
– Tuberculosis
• Thoracoscopy as a therapeutic tool
• Practical aspects
45

Oxford
Pleural
Unit Malignant Pleural Effusion
• Estimated 300,00 patients per year (UK + US)
• Extra 100,000 cases of cancer per year by 2025
• Mesothelioma projected to increase until 2020:
• >90% develop malignant effusion
• 65,000 projected to die of mesothelioma in
the UK between 20001 and 2050
• Will become prominent problem in the
developing world
• Average District General in the UK will see
around 250 cases per year
46

Oxford
Pleural
Unit
Predicted mesothelioma deaths
in British men
Incidence of mesothelioma
increasing
– 1% of all male deaths
in 1940’s cohort
Lancet - Peto47

Oxford
Pleural
Unit Thoracoscopy: Indications
1. Assessment of cytology negative exudate:• Malignant pleural effusion
• Tuberculosis
• Inflammatory / fibrotic
2. Talc pleurodesis for malignant effusion control
3. Talc pleurodesis for other effusion control (CCF, chylothorax)
4. Staging
5. Less common:• Secondary pneumothorax
• Empyema management
48

Oxford
Pleural
Unit
Indications for Thoracoscopy
1. Suspected malignant effusion
49

Patient referred with undiagnosed pleural effusion (no recent diagnosis of malignancy)
Large effusion (>30% hemithorax)?
Diagnostic fluid sample (image guidance if needed)
tests as in BTS diagnostic guideline
Pleural exudate by Lights criteria?No
Seek and treat cause of transudate
Yes
NoSeek and treat cause of small effusion
If performance status 2 or better,
consider image image-guided biopsy
Pleural cytology positive for malignancy? Yes
Consider whether pleural histology
is needed for diagnostic clarity
Yes
Treat appropriately
No
Yes
Performance status 2 or better?
coagulation normal? No
Treat appropriately
No
Yes
Consider referral
for thoracoscopy
Treat appropriately
Perform CT scan
50

Oxford
Pleural
Unit The diagnostic pathway
Cytology• 60% sensitivity overall
• Substantially worse (22%) in mesothelioma
• ? Second attempt
Cytology positive cases• “Malignant cells” • Further confirmation needed in some circumstances• E.g.:
• Mesothelioma• Breast• Lymphoma• EGFR status
51

Oxford
Pleural
Unit “Tissue is the issue”
Cytology negative exudate – diagnostic options:• “Closed” (Abram’s, Cope)
• Image guided
• Local anaesthetic thoracoscopy
• VATs / Thoracotomy
Size of biopsy may matter:• Different biology of pleural metastasis to
primary cancer1,2
• Altered survival in breast1 and lung2
1Schwarz et al, ERJ 20042Wu et al, ERJ, 2008
52

Oxford
Pleural
Unit ? Place for Abram’s
biopsy
18F Tru-cut biopsy needle Abram’s biopsy needle
53

Oxford
Pleural
Unit Abram’s for suspected
malignant effusion
Versus CT guided biopsy• Randomised evidence suggests Abrams should
not be used
Versus thoracoscopy:• No direct comparisons
• Problems with Abrams:
• Distribution of disease
• Safety
54

Oxford
Pleural
Unit Malignant effusion
Abram’s Diagnostic Yield:• ~60%
Thoracoscopy Diagnostic Yield1:• 22 studies
• 1494 patients
• Diagnostic rate = 93.3%
• 95% CI = 92 to 95
1BTS thoracoscopy guidelines, Thorax 201055

56

Oxford
Pleural
Unit Malignant effusion
“Stop messing about”• Thoracoscopy versus surgical biopsy?
57

58

59

Oxford
Pleural
Unit Malignant effusion
- summary
Thoracoscopy for diagnosis• Likely to be equivalent to VATs for diagnosis
of malignant pleural disease
• Higher diagnostic yield than Abram’s
• No direct comparison to CT guided available (and no point)
Added benefits:• Simultaneous drainage and poudrage in
single procedure
60

Normal
Inflammation
Pleural Plaques
61

Parietal and visceral
malignancy
Gross Parietal
Malignancy
62

Oxford
Pleural
Unit
Indications for Thoracoscopy
2. Tuberculosis
63

Oxford
Pleural
Unit Pleural TB
Pathology• Diffuse pleural process
• Widespread even distribution from apex to diaphragm
• Therefore unguided pleural biopsy likely to have high diagnostic yield
Abram’s therefore as good?
64

Oxford
Pleural
Unit Abram’s versus thoracoscopy
Diacon et al• 51 patients with undiagnosed exudative effusion
• Investigated with:• CXR
• sputum AFB smear
• Pleural fluid (biochem / cytol / micro)
42/51 (82%) had TB• High prevalence TB area (Cape Town S.A.)
• bronchial wash
• fluid microbiology
• Abram’s biopsy, histology
• Medical thoracoscopyDiacon et al. Eur Respir J 2003
65

Oxford
Pleural
Unit Abram’s versus thoracoscopy
Histology and AFB stain
• Thoracoscopy:• True positive 42/42 pts (100%)
• Sensitivity 100%
• Specificity 100%
• NPV 100%
• Abrams:• True positive 28/42 pts (67%)
• Sensitivity 67%
• Specificity 100%
• NPV 39% p = 0.02 c2
Immediate results:
67% vs 100%
66

Oxford
Pleural
Unit Abram’s versus thoracoscopy
Histology and AFB stain + CULTURE
• Thoracoscopy:• True positive 42/42 pts (100%)
• Sensitivity 100%
• Specificity 100%
• NPV 100%
• Abrams:• True positive 33/42 pts (79%)
• Sensitivity 79%
• Specificity 100%
• NPV 50% p = 0.05 c2
Delayed results:
79% vs 100%
67

Oxford
Pleural
Unit TB effusion
Thoracoscopy Diagnostic Yield1:• 5 studies
• 4 in low prevalence areas for TB:
• Thoracoscopy diagnostic rate = 93.3%
• 1 high prevalence area:
• Thoracoscopy diagnostic rate = 100%
1BTS thoracoscopy guidelines, Thorax 201068

Oxford
Pleural
Unit TB pleural effusion
Suspected TB pleuritis:• Good diagnostic yield (80%) with Abram’s
• Case control study shows thoracoscopy to have a
higher diagnostic yield
• Use of Abram’s will:
• Delay diagnosis in ~40%
• Miss diagnosis in ~20%
69

TB PleuritisNormal
70

Oxford
Pleural
Unit
Thoracoscopy as a therapeutic
procedure
71

Oxford
Pleural
Unit Talc poudrage
Poudrage for MPE:• 10 studies
• 645 patients
• Overall efficacy at 1 month = 84.6%
• 95% CI = 82 to 87
Slurry versus poudrage for MPE• Cochrane review in favour of poudrage
• RR of non recurrence = 1.19 (95% CI 1.04 to 1.36)
• Single RCT – equivalent to slurry
• ? Some subgroup signals
72

Oxford
Pleural
Unit
Safety
73

Oxford
Pleural
UnitThoracoscopy
safety
Safety and complications• 47 studies
• 4163 procedures
Complications Rate 95% CI Num / Denom
Major 2.7% 2.2 to 3.2 113/4163
Minor 7.0% 5.9 to 8.3 147/2105
Mortality 0.40% 0.2 to 0.7 20/4163
Major complications: Death / empyema / haemorrhage / tract tumour growth / bp fistula / post op
pneumothorax /air leak / pneumonia
Minor complications: sc emphsyema / minor haemorrhage / site infection / hypotension during
procedure / raised temperature / AF74

Oxford
Pleural
UnitThoracoscopy
safety
Safety and complications• 47 studies
• 4163 procedures
Complications Rate 95% CI Num / Denom
Major 2.7% 2.2 to 3.2 113/4163
Minor 7.0% 5.9 to 8.3 147/2105
Mortality 0.40% 0.2 to 0.7 20/4163
Mortality
(diagnostic alone)0.0%
0.0 to 0.15 0/2421
Major complications: Death / empyema / haemorrhage / tract tumour growth / bp fistula / post op
pneumothorax /air leak / pneumonia
Minor complications: sc emphsyema / minor haemorrhage / site infection / hypotension during
procedure / raised temperature / AF75

Oxford
Pleural
Unit
Practical aspects
76

Oxford
Pleural
Unit Patient Selection
“Inclusions”• Radiologically confirmed pleural effusion
• Reasonable prognosis
• Tissue diagnosis will change management
• Able to tolerate sedation and position
“Exclusions”• Intractable cough
• Significant hypercapnia
• Lung adherent to chest wall throughout hemithorax
• Gross obesity
77

Oxford
Pleural
Unit Practical issues - OPD
Fitness for the examination:• If hypoxic, assess CO2
• Severely breathless at rest (unless very large
effusion)
Absence of bleeding diathesis:• Platelet count
• PT / APTT
• Anticoagulants
78

Oxford
Pleural
Unit Available Thoracoscopes
7mm 50o:• Excellent view of hemithorax
• “Periscope” view
• >7mm initial incision
5mm 0o:• Direct view of hemithorax
• Smaller pictures
• Useful for single port biopsy technique
2mm 0o
• “Needle Scope”
• Driven directly in to pleural space with “Verres” needle
• Very small view
Semi-rigid scope
79

Oxford
Pleural
Unit Biopsy techniques
Two port:• Good visulisation of hemithorax
• Permits adhesion division
• Permits “palpation” of pleural surface
• Requires second entry in to thorax
Single Port:• Single entry
• More simple
• Less access / flexibility within hemithorax
80

Singe PortTwo portl
81

Oxford
Pleural
Unit
Conducted when:• Macroscopic evidence of malignancy
• Probable malignancy in older age group
Technique:• Post biopsies, before drain insertion
• 4g sterile talc (graded)
• Dry powder insufflation
• Ensure other port open / catheter does not entirely fill port (risk of tension)
Talc Poudrage
82

Oxford
Pleural
Unit Summary
Thoracoscopy • High diagnostic yield in pleural effusion
• Permits diagnosis / drainage / therapy in a
single procedure
• Safe
• Increasing need for the technique
• Essential part of a specialist service
83

Additional course resources
Readings, guidelines and E-learning resources
1. Rozman A, Camlek L, Marc-Malovrh M, Triller N, Kern I., Rigid versus semi-rigid thoracoscopy
for the diagnosis of pleural disease: a randomized pilot study, Respirology. 2013 May; 18(4):704-
10. doi: 10.1111/resp.12066.
2. Rozman A, Camlek L, Kern I, Malovrh MM., Semirigid thoracoscopy: an effective method for
diagnosing pleural malignancies, Radiol Oncol. 2014 Jan 22; 48(1):67-71. doi: 10.2478/raon-
2013-0068. eCollection 2014
3. Rozman A, Camlek L, Marc Malovrh M, Kern I, Schönfeld N., Feasibility and safety of parietal
pleural cryobiopsy during semi-rigid thoracoscopy, Clin Respir J. 2014 Dec 16. doi:
10.1111/crj.12256
4. von Bartheld MB1 Dekkers OM, Szlubowski A, Eberhardt R, Herth FJ, in 't Veen JC, de Jong
YP, van der Heijden EH, Tournoy KG, Claussen M, van den Blink B, Shah PL, Zoumot Z,
Clementsen P, Porsbjerg C, Mauad T, Bernardi FD, van Zwet EW, Rabe KF, Annema JT.,
Endosonography vs conventional bronchoscopy for the diagnosis of sarcoidosis: the
GRANULOMA randomized clinical trial, JAMA. 2013 Jun 19; 309(23):2457-64. doi:
10.1001/jama.2013.5823
5. Cancellieri A, Leslie KO, Tinelli C, Patelli M, Trisolini R., Sarcoidal granulomas in cytological
specimens from intrathoracic adenopathy: morphologic characteristics and radiographic
correlations, Respiration. 2013; 85(3):244-51. doi: 10.1159/000345386. Epub 2012 Dec 29
84

Cryobiopsy increases the diagnostic yield
of endobronchial biopsy: a multicentre trialJ. Hetzel, R. Eberhardt, F.J.F. Herth, C. Petermann, G. Reichle, L. Freitag,I. Dobbertin, K.J. Franke, F. Stanzel, T. Beyer, P. Moller, P. Fritz, G. Ott,P.A. Schnabel, H. Kastendieck, W. Lang, A.T. Morresi-Hauf, M.N. Szyrach,R. Muche, P.L. Shah, A. Babiak and M. Hetzel
ABSTRACT: Forceps, brushes or needles are currently the standard tools used during flexible
bronchoscopy when diagnosing endobronchial malignancies. The new biopsy technique of
cryobiopsy appears to provide better diagnostic samples. The aim of this study was to evaluate
cryobiopsy over conventional endobronchial sampling.
A total of 600 patients in eight centres with suspected endobronchial tumours were included in
a prospective, randomised, single-blinded multicentre study. Patients were randomised to either
sampling using forceps or the cryoprobe. After obtaining biopsy samples, a blinded histological
evaluation was performed. According to the definitive clinical diagnosis, the diagnostic yield for
malignancy was evaluated by a Chi-squared test.
A total of 593 patients were randomised, of whom 563 had a final diagnosis of cancer. 281
patients were randomised to receive endobronchial biopsies using forceps and 282 had
biopsies performed using a flexible cryoprobe. A definitive diagnosis was achieved in 85.1% of
patients randomised to conventional forceps biopsy and 95.0% of patients who underwent
cryobiopsy (p,0.001). Importantly, there was no difference in the incidence of significant
bleeding.
Endobronchial cryobiopsy is a safe technique with superior diagnostic yield in comparison with
conventional forceps biopsy.
KEYWORDS: Cryobiopsy, diagnostic yield, endobronchial biopsy, forceps, multicentre, tumour
Flexible bronchoscopy is the diagnostic toolof choice to diagnose endobronchial malig-nancies. It allows inspection and biopsy of
any endobronchial abnormalities under direct vision.Pathology samples can be harvested by usingvarious techniques, e.g. forceps, brushing or wash-ing. Flexible bronchoscopy and the associated tissuesampling techniques are the most widespreadprocedures in the diagnosis of central lung cancer.Even though the specimens are obtained underdirect vision, there is a significant failure rate, which,therefore, requires repeated bronchoscopies. Con-current application of different sampling techniquesat bronchoscopy has been shown to improve theyield [1–3].
The major drawback of the forceps biopsytechnique is the relatively small amount of tissueobtained, which is determined by the size of theforceps. Additionally, mechanical compressionor crush artefacts from the instrument tip cause
alterations of the tissue samples, which affect thequality of the histological analysis [4].
A biopsy tool of choice should provide a safetechnique that is capable of obtaining large biopsysamples without causing any morphological altera-tion to the tissue samples, thereby lowering the rateof additional sampling techniques needed, or eventhe need for repeated bronchoscopies. It should alsoenable sampling from areas of the endobronchial treethat may be difficult to access. The flexible cryoprobeappears to have most of these characteristics.
Successful removal of endobronchial tumourfrom the central airways by using flexible cryo-probes has been previously demonstrated [4, 5].Tissue samples from cryorecanalisation weredemonstrated to be of a high quality and muchlarger than conventional biopsy samples [4].
The aim of this multicentre study was to evaluatethe diagnostic yield and safety of cryobiopsy in
AFFILIATIONS
Author affiliation details can be found
in the Acknowledgements section.
CORRESPONDENCE
J. Hetzel
Dept of Internal Medicine II
University of Tuebingen
Otfried-Mueller str. 10
72076 Tuebingen
Germany
E-mail: [email protected]
tuebingen.de
Received:
Feb 21 2011
Accepted after revision:
July 08 2011
First published online:
Aug 18 2011
European Respiratory Journal
Print ISSN 0903-1936
Online ISSN 1399-3003For editorial comments see page 513.
EUROPEAN RESPIRATORY JOURNAL VOLUME 39 NUMBER 3 685
Eur Respir J 2012; 39: 685–690
DOI: 10.1183/09031936.00033011
Copyright�ERS 2012
c
85

comparison with conventional forceps biopsy for samplingendobronchial lesions suspicious for malignancy.
MATERIALS AND METHODSThis study was a prospective, randomised, single-blinded,controlled, multicentre study. The primary goal of the studywas to assess the diagnostic yield of cryobiopsies in comparisonwith forceps biopsies. The gold standard was the final patho-logical diagnosis and takes into consideration any otherdiagnostic investigations that were performed. Secondary end-points of the study were to assess the duration of the biopsyprocedure, the number of samples taken, the level of difficulty inpositioning the probe and the amount of bleeding.
Inclusion criteria were: suspected endobronchial lesion based onclinical signs and radiological images; age .18 yrs; and signedinformed consent.
Patients with a bleeding diathesis or who were on anticoagulantsor who had oxygen saturation ,90% (under delivery of oxygen atf2 L?min-1), or severe underlying cardiac disease (unstableangina pectoris, myocardial infarction in the past month ordecompensated heart failure) were excluded.
The corresponding ethics committees and the institutional reviewboard at the University of Ulm, Ulm, Germany, approved thestudy protocol.
BronchoscopyWritten informed consent for participation in the study and fordata protection was obtained before bronchoscopy. The protocolallowed the bronchoscopy to be performed either by the flexibleor rigid technique. However, all patients who underwent flexiblebronchoscopy were required to be intubated with an endotra-cheal tube in order to provide a secure airway and also to enablecryobiopsies to be performed. Where rigid bronchoscopy wasutilised, the actual biopsy was performed using the flexiblebronchoscope inserted through the rigid tube. General anaes-thesia for rigid bronchoscopy, as well as sedation for flexiblebronchoscopy, was performed according to each centre’sstandards. Standard patient monitoring comprised continuousO2 saturation and ECG monitoring with repeated blood pressuremeasurements.
The patients were randomised only after a suspicious lesionrequiring a biopsy was identified at bronchoscopy, providing theyhad been enrolled into the study and had signed a consent form.A stratified block randomisation into forceps or cryobiopsy groupwas performed, giving the information by using consecutivenumbered envelopes for randomisation at each study site.
Tissue samplingDepending on randomisation, either cryobiopsy or forcepsbiopsy was performed. With cryobiopsy, the cryoprobe wasplaced onto the suspicious lesions, and the freezing cycle wasthen initiated causing the tissue to attach to the probe tip [4–6].The duration of the freezing cycle was dependent on the tissuecharacteristics and was judged by the operator according tothe size of the frozen tissue formed. Freezing for ,2–3 s wasconsidered as sufficient for most of the biopsies. Whilst stillfrozen, the cryoprobe was retracted together with the broncho-scope to extract a biopsy sample. The frozen biopsy was then
released from the probe by thawing in a water bath and placed informalin.
The number of biopsies needed per protocol was left to thebronchoscopist’s discretion with a suggested maximum limit offour samples. The actual number of biopsies and their localisationwere documented, as well as any significant bleeding or othercomplications. Tumour growth was classified into exophytic orsubmucosal. Duration of the biopsy procedure, and type andamount of medication were documented. Additionally, thedifficulty of positioning the biopsy instrument on the lesionwas rated to be easy, moderate or difficult.
HistologyThe biopsy samples were fixed in neutral 10% buffered formalin,embedded in paraffin and cut into 4-mm sections followed bystaining with haematoxylin and eosin. The samples wereanalysed and assessed by one pathologist in each centreaccording to common standards describing malignancy and itsentity. The pathologist was blinded from the biopsy techniquethat had been used. To allow an exact classification, additionalstainings and immunohistochemistry were allowed.
StatisticsAll data were analysed by descriptive methods. For categoricalvariables, absolute and relative frequencies, and for continuousvariables mean¡SD, are given, whereby the primary andsecondary end-points are presented separately for both groups.
The biopsy technique utilised was regarded as successful whenhistological confirmation of the diagnosis was achieved at theinitial bronchoscopy and matched the final diagnosis. Ifadditional tests, e.g. further bronchoscopies, surgery, etc., wereneeded to establish the diagnosis, the biopsy was regarded asnondiagnostic. Diagnostic yield was calculated for each biopsytechnique as the number of diagnostic procedures divided bynumber of nondiagnostic procedures plus the number ofdiagnostic procedures. An explorative test of the diagnostic yieldof the two biopsy techniques was performed in a small number ofpatients before statistical planning of this trial. On the basis ofthese data, the study was powered at 90% for a level ofsignificance of p50.05. A group size of 278 patients wascalculated and, assuming possible dropouts, a group size of 300patients was proposed.
The primary confirmatory comparison of diagnostic rate betweenthe two techniques was evaluated by a two-tailed Chi-squaredtests with a 5% level of significance.
All additional secondary assessments were investigated using therespective tests for parallel-group designed studies (Chi-squaredtest and Mann–Whitney rank tests). The respective levels ofsignificance in this exploratory analysis were set to 5%, and noadjustment for multiple testing was performed.
All adverse events were recorded and compared descriptively.Bleeding was defined according to the clinical interventionsrequired. Mild bleeding was defined as bleeding that wascontrolled by suctioning. Severe bleeding was regarded as theneed for additional intervention, e.g. instillation of ice-cold salineor a diluted vasoconstrictive drug, balloon tamponade, argonplasma coagulation (APC), conversion to rigid bronchoscopy ormechanical ventilation.
LUNG CANCER J. HETZEL ET AL.
686 VOLUME 39 NUMBER 3 EUROPEAN RESPIRATORY JOURNAL
86

RESULTSA total of 600 patients were randomised from June 2006 toOctober 2008 in eight centres in Germany. 593 of these patientswere included in the evaluation; five patients withdrew theirwritten consent and two patients were randomised twice.Malignant disease was diagnosed in 563 patients (fig. 1). 388patients had nonsmall cell lung cancer (NSCLC), 118 patientssmall cell lung cancer (SCLC) and 57 patients other malignantentities, including metastases (table 1 and fig. 1).
The demographic and baseline characteristics of the two groupswere similar (table 1). The patients were ,65 yrs of age with amale preponderance. There was no difference in the proportionof patients that were taking aspirin between the two groups (25versus 27 patients) or clopidogrel (one versus four patients).General anaesthesia was used in 134 patients in the forceps groupand 136 patients in the cryobiopsy group. For conscious sedation,propofol was used in 174 patients, 42 patients receivedmidazolam and 92 received a combination of both. In 15 patients,the intubation was performed exclusively under local anaesthe-sia. There was no difference in the rates of rigid bronchoscopyand flexible bronchoscopy (forceps group: rigid in 133 patientsand flexible in 164 patients; cryobiopsy group: rigid in 136patients and flexible in 160 patients). Different kinds of biopsyforceps were allowed according to the personal preferences ofeach centre or physician. These were standard biopsy forceps(with and without thorn) having claw diameters of 2.0 mm and2.6 mm, and crocodile forceps with claw diameters of 2.0 mmand 2.6 mm. Forceps with smaller claws (2.0 mm) were used in76 patients (25.6%) and the forceps with larger claws (2.6 mm) in219 patients (73.7%). In two cases, specification of the forceps wasnot documented. The diagnostic yield was not different inpatients who were diagnosed with the small forceps (2.0 mm;84.2%) or the large forceps (2.6 mm; 85.4%).
No difference in the coagulation parameters and thrombocytecount was found. There was no significant difference in thelocation of the lesion between the groups (p50.40; table 1).
Among patients with the diagnosis of a malignant disease, thediagnostic yield for cryobiopsy was 95.0% (268 out of 282patients) and 85.1% (239 out of 281 patients) for standard forceps.Comparison between groups revealed a significantly higherdiagnostic yield for cryobiopsy (p,0.001; table 2). Cryobiopsy
exceeded forceps biopsy significantly in the diagnosis of bothexophytic (97.3% versus 89.5%; p50.003) and submucosaltumours (90.9% versus 75.8%; p50.005) (table 2).
The final diagnosis could not be made with the instrumentpredefined by randomisation in 56 patients (42 of the forcepsbiopsy and 14 of the cryobiopsy patients). In these patients, thedefinitive diagnosis was obtained by many alternative proce-dures, including surgery as a final choice (table 3).
With respect to the bronchoscopy technique, the diagnostic yieldusing flexible bronchoscopy was significantly higher withcryobiopsy (95.2%) compared with forceps biopsy (82.2%)(p50.0001). When rigid bronchoscopy was used, there was atrend towards a higher diagnostic yield in the cryobiopsy group(94.6% versus 89.5%; p50.131).
In order to further demonstrate the added value of the cryobiopsytechnique with respect to the histopathological characteristics ofdifferent tumour entities, we performed a subgroup analysis for
57 other malignant disorders
118 SCLC
593 patients for evaluation
600 patients
7 patients dropped out
388 NSCLC
563 patients with malignant
disease
30 patients with no malignant disease
detectable
FIGURE 1. Patient distribution. NSCLC: nonsmall cell lung cancer; SCLC:
small cell lung cancer.
TABLE 1 Patient characteristics and distribution of thebiopsy sites for each biopsy technique
Forceps Cryoprobe p-value
Patient characteristics
Patients 297 296
Age yrs 65.3¡9.9 64.8¡10.3 0.55
Male 207 (69.6) 217 (73.4) 0.36
Body height cm 170.9¡8.5 170.2¡8.9 0.33
Body weight kg 74.3¡14.7 72.3¡15.0 0.10
Aspirin 100 mg?day-1 25 (8.42) 27 (9.12) 0.77
Clopidogrel 75 mg?day-1 1 (0.34) 4 (1.35) 0.22
General anaesthesia 134 (45.1) 136 (45.9) 0.87
Rigid bronchoscopy 133 (44.8) 136 (45.9) 0.80
PT % 95.1¡16.6 94.7¡16.2 0.77
PTT s 29.8¡4.6 29.5¡4.6 0.43
Thrombocyte count
6103 cells?mL-1
331.6¡130.9 331.0¡118.8 0.95
NSCLC 192 196 0.73
SCLC 62 56 0.61
Other malignant disease 27 30 0.68
Other disease 16 14 0.85
Distribution of the
biopsy sites
Trachea 18 16 0.40
Main bronchi 62 57
Lobe bronchi and
intermediate bronchus
156 175
Segmental bronchi 61 48
Lesions in patients
with malignancy
Exophytic 190 183 0.49
Submucosal 91 99
Data are presented as n, n (%) or mean¡SD, unless otherwise stated. None of
the values differed significantly between the two biopsy groups. PT:
prothrombin time; PTT: partial thromboplastin time; NSCLC: nonsmall cell lung
cancer; SCLC: small cell lung cancer.
J. HETZEL ET AL. LUNG CANCER
cEUROPEAN RESPIRATORY JOURNAL VOLUME 39 NUMBER 3 687
87

the two largest tumour entities in this collective: NSCLC andSCLC (table 4). The proportion of nondiagnostic results inpatients with NSCLC and SCLC was lower after cryobiopsythan after forceps biopsy: NSCLC, 5.5% (95% CI 2.8–9.6) versus11.8% (95% CI 7.6–17.2) and SCLC, 3.6% (95% CI 0.4–12.3) versus16.1% (95% CI 8.0–27.7) (table 4). The cryobiopsy group shows a
considerably smaller 95% confidence interval in comparison withthe forceps group regarding the nondiagnostic outcomes ofNSCLC and SCLC. This indicates that, cryobiopsy not only servesas a more sensitive but also as a more reliable tool than forcepsbiopsy for diagnosis.
No difference was found with respect to the time needed forbiopsy and subsequent bleeding control between the groups5.05¡4.54 versus 5.25¡4.20 min for cryobiopsy and forcepsbiopsy, respectively. The number of samples taken differed infavour of cryobiopsy (3.24¡1.16 versus 3.45¡0.95; p,0.001).Positioning judgement was not different between the groups,although there was a trend in favour of the cryobiopsy (p50.068,data not shown). There was significantly more bleeding in thecryobiopsy group compared with the forceps group (p50.009;table 5); however, the number of bleeding complications needingany intervention for bleeding control did not differ between thegroups (p50.90). APC was required in 13 patients from thecryobiopsy group compared with eight patients in the forcepsgroup. Tamponade was required in two patients in each group.All other episodes of bleeding were managed by instillation ofice-cold saline or vasoconstrictive drugs. No surgical interven-tions for bleeding control were needed and no fatal eventsoccurred.
DISCUSSIONThis is the first multicentre, prospective, randomised, single-blinded, controlled trial evaluating the novel cryobiopsy techni-que in comparison with our current standard technique usingforceps. We were able to demonstrate that a greater proportion ofpatients with an endobronchial lesion suspicious for malignancyhas a definite diagnosis when a cryobiopsy is performed (95%)
TABLE 2 Diagnostic and nondiagnostic biopsies for eachbiopsy technique in patients with maligancy
Forceps Cryoprobe p-value
Overall
Diagnostic 239 (85.1) 268 (95.0) ,0.001
Nondiagnostic 42 (14.9) 14 (5.0)
Exophytic tumour
Diagnostic 170 (89.5) 178 (97.3) 0.003
Nondiagnostic 20 (10.5) 5 (2.7)
Submucosal tumour
Diagnostic 69 (75.8) 90 (90.9) 0.005
Nondiagnostic 22 (24.2) 9 (9.1)
Data are presented as n (%), unless otherwise stated. Biopsies are shown in
relation to each biopsy group and subgroup analysis of exophytic and
submucosal tumours. Cryobiopsy was superior over forceps biopsy in the
diagnosis of exophytic and submucosal tumours.
TABLE 3 Procedures used to obtain the final malignantdiagnosis after nondiagnostic forceps biopsyand cryobiopsy
Forceps Cryoprobe
Subjects 42 14
Type of procedure for final diagnosis
Cryobiopsy 14 0
Forceps 14 3
Forceps + cytology 2 0
Forceps + catheter biopsy 0 1
Cervical lymph node biopsy 2 0
Catheter biopsy 0 1
Brush cytology 1 0
Cytology 2 0
Liver function 0 1
Transbronchial biopsy of a peripheral nodule 2 0
TBNA 0 2
Transcranial fine needle aspiration 1 0
Punch biopsy 0 2
Lymph node biopsy 0 1
Biopsy from stomach metastasis 0 2
Mediastinoscopy 1 0
Surgery 3 1
Data are presented as n. The procedures used to obtain the final diagnosis after
nondiagnostic procedures differed in the forceps biopsy and the cryobiopsy
group. There was no preferred second choice method. TBNA: transbronchial
needle aspiration.
TABLE 4 Numbers of nondiagnostic biopsies for eachbiopsy technique
Two most common
tumour types
Forceps Cryoprobe p-value
NSCLC
n/N 23/195 11/201 0.025
% (95% CI) 11.8 (7.6–17.2) 5.5 (2.8–9.6)
SCLC
n/N 10/62 2/56 0.024
% (95% CI) 16.1 (8.0–27.7) 3.6 (0.4–12.3)
NSCLC: nonsmall cell lung cancer; SCLC: small cell lung cancer.
TABLE 5 Biopsy-related bleeding for each biopsy group
Type of bleeding Forceps Cryoprobe p-value
None 91 (30.6) 59 (19.9) 0.009
Mild# 153 (51.5) 183 (61.8)
Severe" 53 (17.8) 54 (18.2)
Data are presented as n (%), unless otherwise stated. #: no intervention; ": at
least one intervention for bleeding control applied.
LUNG CANCER J. HETZEL ET AL.
688 VOLUME 39 NUMBER 3 EUROPEAN RESPIRATORY JOURNAL
88

rather than a traditional forceps biopsy (85.1%). With our currentstandard practice of forceps biopsy, the patients without aconclusive diagnosis (15%) would have required either a repeatbronchoscopy or an alternative procedure. This has both costimplications and the need for the additional invasive procedures,which increase the risk of adverse events in any individualpatient. This statement may be limited due to the secured airwayalso for flexible bronchoscopy, demanded by the protocol.Furthermore, the need for additional procedures would increaseany potential time delays to the patient’s treatment. Thediagnostic rate for cryobiopsy is the highest rate observed forany single sampling technique in bronchoscopy [7–9]. Evenwhere multiple sampling techniques (forceps, needles, brushingand washing) are utilised, the diagnostic yield reaches only 88%[2, 8, 10, 11]. The difference in our results is unlikely to be due to apoor yield in the standard forceps group, as its diagnostic rate issimilar to other published studies [7–9, 10]. However, superiorityof cryobiopsy becomes blurred when exclusively comparingbiopsies carried out using rigid intubation. Due to generalanaesthesia and a reduced breathing amplitude, positioning offorceps becomes easier, thus diminishing the benefit of cryo-biopsy. The overall superiority of cryobiopsies is most probablydue to the higher quality of the samples defined by their largersample size and low amount of biopsy-related tissue alterations,which has been shown in previous studies [4, 6, 12, 13]. Mostrecently, a single-centre analysis underlined this fact: the totalarea of each tissue section of the cryobiopsies had been describedto be twice as large as forceps biopsies, in addition to the higherquality of the cryobiopsies. This resulted in a significantly higherartefact-free area of each slide in the cryobiopsy group comparedwith the forceps group (9.6 versus 3.6 mm2). This is of increasingimportance in the treatment of lung cancer. Increasingly, drugsthat target specific genetic alterations in the tumour tissue arebeing utilised [14, 15] and, hence, a better quality of tissueobtained at biopsy might facilitate identification of moleculartargets for treatment.
Further advantages of the cryoprobe include the fact that biopsiescan be extracted even when the cryoprobe is positionedtangentially with an angle of 0u towards the tissue, whereas theforceps must be placed almost perpendicular to the tissue toobtain a good specimen. This is an important advantage,especially in a narrower lumen. Due to a concentric expansionof the freezing area starting from the tip of the cryoprobe andexpanding into the periphery, a larger surface area and, thereby,larger biopsies can be generated. The size can also be regulated bythe operator over the activation time: increasing the freezing timeincreases the biopsy size. Forceps biopsies are limited by the sizeof the forceps claws. These technical differences may also accountfor the significantly higher number of diagnostic biopsies, mostlyin submucosal (90.9% versus 75.8%; p50.005) but also inexophytic tumours (97.3% versus 89.5%; p50.003).
In addition, cryobiopsy could serve as a more sensitive and morereliable tool than forceps biopsy to diagnose both NSCLC andSCLC. We found that cryobiopsy was superior to forceps biopsyin the diagnosis of NSCLC (p50.025) and SCLC (p50.024)(table 4).
One histological characteristic of SCLC is the large amount ofnecrotic tissue present. As the size of the cryobiopsy specimenis larger, this may affect the diagnostic yield of cryobiopsy less
negatively than with forceps biopsy. A more detailedhistological evaluation, especially with respect to NSCLC andSCLC subtyping, will be the subject of further studies.
The safety profile for the two techniques was similar. Theadverse events, particularly bleeding, were quoted on the basisof interventions required. This is far more clinically relevantthan attempting to estimate the volume loss of the blood,which is notoriously difficult. There was a greater incidence ofmild bleeding with cryobiopsy, but no additional interventionswere required. This observation might be explained by the factthat, after retracting the bronchoscope for harvesting thebiopsy, there is a larger time period until bleeding controlcan be started, resulting in an accumulation of blood at thebiopsy site. This assumption is in line with the data of ananimal study, where no difference in bleeding times wasobserved between forceps biopsy and cryobiopsy, althoughlarger biopsies were extracted with the cryoprobe [16].
One limitation that might be argued is that only malignantdisease was included for calculation, for several reasons. First, thedegree of separation between a diagnostic and nondiagnosticresult is stronger than in benign disease. Secondly, in the settingof a multicentre study, it was important to have a standardiseddiagnostic process, which is defined best for malignancies.
A disadvantage of the cryobiopsy technique is that intubation ofthe patients is recommended. The tissue attached to the cryop-robe cannot be retracted through the instrument channel of thebronchoscope and, hence, requires removal of the cryoprobe andbronchoscope as a single unit. Under these circumstances, it isimportant to have a secure airway allowing rapid re-insertion ofthe bronchoscope to control any potential bleeding. This alsofacilitates additional suction if required and insertion oftamponade balloons if needed. However, we consider this to bea small additional step and most patients can tolerate anendotracheal tube without the need for additional sedation incomparison with a standard bronchoscopy. Our results clearlydemonstrate that there is no difference in the duration of the twoprocedures, or in the sedation or anaesthetic protocols.Furthermore, the procedure can be performed according to localpractice with either flexible bronchoscopy or in conjunction withrigid bronchoscopy.
In conclusion, endobronchial cryobiopsy is a safe technique witha higher diagnostic yield for the diagnosis of endobronchialmalignancies than forceps biopsy and might extend the numberof tools available to chest physicians for obtaining sufficientendobronchial tissue for a definitive diagnosis.
CLINICAL TRIALThis study is registered at www.controlled-trials.com with identifuernumber ISRCTN97376650.
STATEMENT OF INTERESTStatements of interest for J. Hetzel, M.N. Szyrach, P.L. Shah andM. Hetzel can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
ACKNOWLEDGEMENTSThe author’s affiliations are as follows. J. Hetzel: Dept of InternalMedicine II, University of Tuebingen, Tuebingen, Germany; R.Eberhardt and F.J.F. Herth: Dept of Pneumology and RespiratoryCare Medicine, Thoraxklinik at the University of Heidelberg,
J. HETZEL ET AL. LUNG CANCER
cEUROPEAN RESPIRATORY JOURNAL VOLUME 39 NUMBER 3 689
89

Heidelberg, Germany; C. Petermann: Dept of Lung and BronchialMedicine, Asklepios Clinic Harburg, Hamburg, Germany; G. Reichleand L. Freitag: Dept of Pulmonary Medicine and Thoracic Surgery,Lung Clinic of Hemer, Hemer, Germany; I. Dobbertin: Centre of
Pulmonary Medicine and Thoracic Surgery, Clinic Schillerhoehe,Gerlingen, Germany; K.J. Franke: Dept of Pulmonary Medicine andCritical Care Medicine, Helios Clinic Ambrock, University of Witten/
Herdecke, Hagen, Germany; F. Stanzel: Centre of Pulmonary Medicineand Thoracic Surgery, Asklepios Clinic Gauting GmbH, Munich,Germany; T. Beyer: Lung Clinic Ballenstedt/Harz GmbH, Ballenstedt,Germany; P. Moller: Institute of Pathology, University Clinic Ulm,
Ulm, Germany; P. Fritz and G. Ott: Dept of Pathology, Institute forClinical Pathology, Robert-Bosch Hospital, Stuttgart, Germany;P.A. Schnabel: Dept of General Pathology and Pathological Anatomy,Thoraxklinik Heidelberg, Heidelberg, Germany; H. Kastendieck: Dept
of Pathology, Asklepios Clinic Harburg, Hamburg, Germany; W. Lang:Institute of Pathology, Hannover, Germany; A.T. Morresi-Hauf:Institute of Pathology, Asklepios Clinic Gauting GmbH, Munich,Germany; M.N. Szyrach: ERBE Research, Tuebingen, Germany;
R. Muche: Institute of Biometry, University of Ulm, Ulm, Germany;P.L. Shah: Dept of Respiratory Medicine, Royal Brompton Hospital,London, UK; A. Babiak and M. Hetzel: Dept of Respiratory and Critical
Care Medicine, Red Cross Medical Centre, Stuttgart, Germany.
REFERENCES1 Dobler CC, Crawford AB. Bronchoscopic diagnosis of endoscop-
ically visible lung malignancies: should cytologic examinations beperformed routinely? Intern Med J 2009; 39: 806–811.
2 Lam B, Wong MP, Ooi C, et al. Diagnostic yield of bronchoscopicsampling methods in bronchial carcinoma. Respirology 2000; 5:
265–270.
3 Popp W, Rauscher H, Ritschka L, et al. Diagnostic sensitivity of
different techniques in the diagnosis of lung tumours with theflexible fiberoptic bronchoscope. Comparison of brush biopsy,imprint cytology of forceps biopsy, and histology of forceps
biopsy. Cancer 1991; 67: 72–75.
4 Hetzel J, Hetzel M, Hasel C, et al. Old meets modern: the use of
traditional cryoprobes in the age of molecular biology. Respiration.
2008; 76: 193–197.
5 Hetzel M, Hetzel J, Schumann C, et al. Cryorecanalization: a newapproach for the immediate management of acute airwayobstruction. J Thorac Cardiovasc Surg 2004; 127: 1427–1431.
6 Babiak A, Hetzel J, Krishna G, et al. Transbronchial cryobiopsy: anew tool for lung biopsies. Respiration 2009; 78: 203–208.
7 McLean AN, Semple PA, Franklin DH, et al. The Scottish multi-centre prospective study of bronchoscopy for bronchial carcinomaand suggested audit standards. Respir Med 1998; 92: 1110–1115.
8 Zavala DC. Diagnostic fiberoptic bronchoscopy: techniques andresults of biopsy in 600 patients. Chest 1975; 68: 12–19.
9 Gellert AR, Rudd RM, Sinha G, et al. Fibreoptic bronchoscopy:effect of multiple bronchial biopsies on diagnostic yield inbronchial carcinoma. Thorax 1982; 37: 684–687.
10 Rivera MP, Mehta AC. Initial diagnosis of lung cancer: ACCPevidence-based clinical practice guidelines (2nd edn). Chest 2007;132: Suppl. 3, 131S–148S.
11 Kacar N, Tuksavul F, Edipoglu O, et al. Effectiveness oftransbronchial needle aspiration in the diagnosis of exophyticendobronchial lesions and submucosal/peribronchial diseases ofthe lung. Lung Cancer 2005; 50: 221–226.
12 Franke KJ, Szyrach M, Nilius G, et al. Experimental study onbiopsy sampling using new flexible cryoprobes: influence ofactivation time, probe size, tissue consistency, and contactpressure of the probe on the size of the biopsy specimen. Lung
2009; 187: 253–259.13 Schumann C, Hetzel J, Babiak AJ, et al. Cryoprobe biopsy increases
the diagnostic yield in endobronchial tumour lesions. J ThoracCardiovasc Surg 2010; 140: 417–421.
14 Nicholson AG, Gonzalez D, Shah P, et al. Refining the diagnosisand EGFR status of non-small cell lung carcinoma in biopsy andcytologic material, using a panel of mucin staining, TTF-1,cytokeratin 5/6, and P63, and EGFR mutation analysis. J Thorac
Oncol 2010; 5: 436–441.15 Tiseo M, Rossi G, Capelletti M, et al. Predictors of gefitinib
outcomes in advanced non-small cell lung cancer (NSCLC): studyof a comprehensive panel of molecular markers. Lung Cancer 2010;67: 355–360.
16 Franke KJ, Theegarten D, Hann von Weyhern C, et al. Prospectivecontrolled animal study on biopsy sampling with new flexiblecryoprobes versus forceps: evaluation of biopsy size, histologicalquality and bleeding risk. Respiration 2010; 80: 127–132.
LUNG CANCER J. HETZEL ET AL.
690 VOLUME 39 NUMBER 3 EUROPEAN RESPIRATORY JOURNAL
90

EDITORIAL
ATS/ERS/WASOG statement on sarcoidosis
U. Costabel, G.W. Hunninghake, on behalf of the Sarcoidosis Statement Committee
The first international consensus statement on sar-coidosis is currently being copublished in the journals ofthe American Thoracic Society (ATS) and the WorldAssociation for Sarcoidosis and Other GranulomatousDisorders (WASOG) [1, 2]. This editorial wants to attractthe attention of the ERJ readers and European RespiratorySociety (ERS) members to this consensus report which isaimed at updating clinicians and scientists about newadvances related to sarcoidosis. It is hoped that the docu-ment will improve the care of patients with this disorderand trigger new studies to further elucidate the cause andpathogenesis of sarcoidosis. The panel members are ex-perts in the care of patients with sarcoidosis, and the levelof evidence for the recommendations made in this state-ment is largely that of expert opinion developed byconsensus. There is little supportive evidence from well-conducted randomized controlled trials.
The panel agreed on the following consensus of the stateof the art of the understanding of pathogenesis, diagnosis,and treatment of sarcoidosis:
What we know:N The clinical features and syndromesN How to make a diagnosisN That corticosteroids are an effective short-term therapyN The incidence and prevalence of the diseaseN That some genetic factors alter expression of the diseaseN The immunology characteristic of the initial onset of the
disease.What we would like to know:
N If there is a test to predict progressionN If corticosteroids alter the natural history of the diseaseN The optimal length of therapyN If there are less toxic therapies than corticosteroids or
cytotoxic agentsN How genetic factors alter expression of the diseaseN If genetic factors affect susceptibility to the diseaseN The mechanisms of lung injury and fibrosisN The mechanisms that result in persistent diseaseN The cause of sarcoidosis.
The panel was divided into groups responsible for writ-ing specific sections of the statement dealing with def-inition, history, epidemiology, aetiology and pathogenesis,pathology, clinical presentation and organ involvement,diagnostic approaches, natural history, and treatment ofsarcoidosis. The following is a summary of some of thesentinal statements of these sections.
The epidemiology of sarcoidosis remains problematicfor several reasons, including: 1) lack of a precise, con-sistent case definition; 2) variable methods of case ascer-tainment; 3) variability in disease presentation; 4) lack of
sensitive and specific diagnostic tests, resulting in under-recognition and misdiagnosis of the disease; and 5) thepaucity of systematic epidemiological investigations ofcause. The disease shows a consistent predilection for ad-ults <40 yrs of age, peaking in those aged 20±29 yrs. InScandinavian countries and in Japan, there is a second peakincidence in females >50 yrs of age. Significant hetero-geneity in prevalence, disease presentation and severityoccurs among different ethnic and racial groups. Severalstudies suggest that sarcoidosis in Afroamericans is moresevere, while Caucasians are more likely to present withasymptomatic disease. Overall mortality from sarcoidosisis 1±5%. Intriguing spatial clusters of illness have sug-gested person-to-person transmission or shared exposure toan environmental agent. Some studies have observed aseasonal clustering of sarcoidosis cases in winter and earlyspring. There are numerous reports of the familial clusteringof sarcoidosis. Human leukocyte antigen (HLA) analyses ofaffected families suggest that the mode of inheritance of riskfor sarcoidosis is to probably polygenic, with the mostcommon genotypes frequencies being class I HLA-A1 and-B8 and class II HLA-DR3. It is likely that geneticallypredisposed hosts are exposed to antigens that trigger anexaggerated cellular immune response leading to granulomaformation.
Although the aetiology of sarcoidosis remains un-known, there are three different lines of evidence sup-porting the idea that sarcoidosis results from exposure ofgenetically susceptible hosts to specific environmental ag-ents: 1) the aforementioned epidemiological studies; 2) theinflammatory response in sarcoidosis, with a pattern of cy-tokine production in the lungs that is most consistent with aTh1-type immune response triggered by an antigen; and 3)the implications of studies concerning the T-cell receptor(TCR) in patients with sarcoidosis. In regard to the role ofenvironmental agents, the list of possible causative agents
Correspondence: U. Costabel, Abt. Pneumologie/Allergologie, Ruhr-landklinik, TuÈschener Weg 40, D-45239 Essen, Germany, Fax: 492014334029.
Table 1. ± Examples of agents suggested to be involvedin the aetiology of sarcoidosis
Type of agent
Infectious Inorganic* Organic
Viruses (herpes, Epstein-Barr,retrovirus, coxsackie B virus,cytomegalovirus)
Aluminium Pine tree pollen
Borrelia burgdorferi Zirconium ClayPropionibacterium acnes TalcMycobacterium tuberculosisand other mycobacteria
Mycoplasma
*: beryllium, which causes berylliosis and not sarcoidosis, is notincluded.
Eur Respir J 1999; 14: 735±737Printed in UK ± all rights reserved
Copyright #ERS Journals Ltd 1999European Respiratory Journal
ISSN 0903-1936
91

has continuously expanded (table 1). The evidence for aninfective aetiology, particularly mycobacterial, is becom-ing more appealing. Unfortunately, even with the adventof molecular tools, such as the highly sensitive poly-merase chain reaction, the debate has not been resolved.Failure to demonstrate mycobacteria may depend oninsensitive methods, whereas positive findings may bedue to contamination. With respect to the T-cell receptorstudies, it is still unclear how helpful they will be in eli-citing the aetiology of sarcoidosis.
The immunological abnormalities of the early sarcoidreaction are well known and are characterized by the ac-cumulation of activated T-cells and macrophages at sites ofongoing inflammation, notably in the lung. However, nostudies have shown why lung disease persists in some pa-tients but not in others. In addition, no studies have shownhow persistent disease results in lung injury and fibrosis.Nevertheless, the immunological pattern of cells in the sar-coid infiltrate suggests that: 1) sarcoid granulomas areformed in response to a persistent and probably poorly de-gradable antigenic stimulus that induces a local Th1-typeT-cell mediated immune response with an oligoclonal pat-tern; and 2) as a consequence of their chronic stimulation,macrophages release mediators of inflammation, locallyleading to accumulation of Th1 cells at sites of ongoinginflammation and contributing to the development of thegranuloma structure.
The pathology section describes the morphology of sar-coid granulomas, the location and distribution of the lesion,and the major pathological differential diagnoses. Becauseimportant differential diagnoses are infectious diseases, theneed for microbiological studies and cultures continues,especially when the patient has fever or when there arenecrotic lesions in the biopsy specimens. Special stains foracid-fast bacilli and fungi are justified, especially whenthere are atypical features for sarcoidosis such as necrosis oran air-space predominance of granulomas.
The clinical presentation and organ involvement isreported in detail, with the lungs being affected in >90% ofpatients with sarcoidosis and the lymphoid system in aboutone-third. Clinical evidence of heart involvement is seen in~5%, liver granulomas in as many as 50±80% of liver bi-opsy specimens, cutaneous involvement in ~25%, and ocu-lar lesions in 11±83%. Neurosarcoidosis which is clinicallyrecognizable occurs in <10% of patients. Symptomaticmuscle and bone involvement is rare, whereas joint painsoccur in 25±39%. Special situations such as sarcoidosis inchildren, sarcoidosis in pregnancy, and sarcoidosis in theelderly are also considered.
The diagnosis of sarcoidosis needs a compatible clinicalpicture, histological demonstration of noncaseating gran-ulomas, and exclusion of other diseases capable of pro-ducing a similar histological or clinical picture. The diag-nostic work-up for patients with sarcoidosis should attemptto accomplish four goals: 1) provide histological con-firmation of the disease; 2) assess the extent and severity oforgan involvement; 3) assess whether the disease is stableor is likely to progress; and 4) determine whether therapywill benefit the patient. In the presence of a compatibleclinical picture, the first step is to choose the site for aproper biopsy. Transbronchial lung biopsy is the recom-mended procedure in most cases. Its diagnostic yield dep-ends largely on the experience of the operator, rangingfrom 40 to >90%. A careful examination of the patient maydisclose other possible sites for biopsy, such as skin, lip, orsuperficial lymph nodes. The problem of a patient withouthistology needs specific consideration. Some patients ref-
use biopsy and in others the pulmonary impairment is toosevere for a lung biopsy. Clinical and/or radiological fea-tures alone may be diagnostic for patients with Stage I(reliability of 98%) or Stage II (89%) disease, but are lessaccurate for patients with Stage III (52%) or Stage 0 (23%)disease. A patient who presents with a classic LoÈfgren'ssyndrome of fever, erythema nodosum, arthralgias, and bi-lateral hilar lymphadenopathy may not require biopsy proofif resolution of disease is rapid and spontaneous. In someinstances, bronchoalveolar lavage and studies on lympho-cyte subpopulations are helpful. The appearance of a Pan-da pattern combined with a Lambda pattern on a total body67Ga scan may support the diagnosis of sarcoidosis andobviate the need for an invasive diagnostic procedure. Amildly elevated angiotensin-converting enzyme is never di-agnostic because elevations may be seen in many diseases.
Once the diagnosis is established, an additional work-upis recommended for all patients (table 2). Lung computedtomography (CT) scans are only indicated for some pa-tients. The usual indications are as follows: 1) atypicalclinical and/or chest radiograph findings; 2) detection ofcomplications of the lung disease, such as bronchiectasis,aspergilloma, pulmonary fibrosis, traction emphysema, ora superimposed infection or malignancy; and 3) a normalchest radiograph but a clinical suspicion of the disease.Clinical activity is assessed on the basis of onset, wor-sening, or persistence of symptoms or signs directly rel-ated to sarcoidosis. A long list of markers of activity hasbeen suggested as potential diagnostic aids or indices of"activation". Some of these markers are consistent withthe ability of the disease to progress in one organ, but theyoften do not detect progress in other organs.
The natural history and prognosis of sarcoidosis arehighly variable, with a tendency of the disease to wax andwane, either spontaneously, or in response to therapy.Spontaneous remissions occur in nearly two-thirds of pa-tients, but the course is chronic or progressive in 10±30%.Serious extrapulmonary involvement (e.g. cardiac, centralnervous system, hepatic) occurs in 4±7% of patients withsarcoidosis at presentation; the incidence is higher as thedisease evolves. Fatalities occur in 1±5% of patients, typ-ically owing to progressive respiratory insufficiency orcentral nervous system or myocardial involvement. Severalclinical features have been associated with a chronic orprogressive course. Adverse prognostic factors include
Table 2. ± Recommended initial evaluation of patientswith sarcoidosis
Type of evaluation
1. History (occupational and environmental exposure,symptoms)
2. Physical examination3. Posteroanterior chest radiography4. Pulmonary function tests: spirometry and DL,CO
5. Peripheral blood counts: white blood cells, red bloodcells, platelets
6. Serum chemistries: calcium, liver enzymes (alanineaminotransferase, aspartate aminotransferase, alkalinephosphatase), creatinine, BUN
7. Urine analysis8. ECG9. Routine ophthalmologic examination10. Tuberculin skin test
DL,CO: diffusing capacity of the lung for CO; BUN: blood ureanitrogen; ECG: electrocardiogram.
736 U. COSTABEL ET AL.
92

lupus pernio, chronic uveitis, age at onset >40 yrs, chronichypercalcaemia, nephrocalcinosis, black race, progressivepulmonary sarcoidosis, nasal mucosal involvement, cysticbone lesions, neurosarcoidosis, myocardial involvement,and chronic respiratory insufficiency. Numerous studieshave affirmed the utility of chest radiographic "stage" as aprognostic guide. Spontaneous remissions occur in 55±90% of patients with Stage I disease, in 40±70% of thosewith Stage II disease, in 10±20% with Stage III disease,and in 0% with Stage IV disease.
Longitudinal surveillance of sarcoidosis should be mostintensive during the first 2 yrs after presentation, in order toassess prognosis and determine the need (if any) for ther-apy. For Stage I disease, initial follow-up every 6 months isusually adequate. More frequent evaluations (every 3±6months) are adviced for Stage II, III or IV sarcoidosis. Allpatients (irrespective of radiographic stage) should be mo-nitored for a minimum of 3 yrs after therapy is discon-tinued. Follow-up needs to be more vigilant amongpatients with corticosteroid-induced remissions, because ofthe high rate of relapses in this context.
The appropriate treatment of the disorder has not beenwell defined for all patients. The symptoms and/or findingsthat necessitate corticosteroid therapy remain controver-sial. In patients with mild disease, such as skin lesions,anterior uveitis or cough, topical steroid therapy may be allthat is necessary. In patients with systemic, symptomaticdisease, oral corticosteroids are often employed. Systemictherapy is clearly indicated for cardiac disease, neurolog-ical disease, eye disease not responding to topical therapy,and hypercalcaemia. The use of systemic therapy in pul-monary and other extrapulmonary disease is less clear cut,but most physicians feel that progressive symptomatic dis-ease should be treated. A patient with persistent pulmonaryinfiltrates or progressive loss of lung functions and nosymptoms may still require therapy. In patients requiringpersistent corticosteroid therapy, antimalarial agents andcytotoxic agents should be considered.
The optimal dose and duration of corticosteroids has notbeen studied in randomized, prospective trials. Dose andduration of therapy often must be individualized. For pul-monary sarcoidosis, the initial dosage is often 20±40 mg.day-1 prednisone or its equivalent on alternate days. Higherdoses may be necessary for cardiac or neurosarcoidosis.After 1±3 months, the patient should be evaluated forresponse. Patients failing to respond by 3 months areunlikely to respond to a more protracted course of therapy.At this point, other reasons for failure should be evaluated,such as presence of irreversible, fibrotic disease, noncom-
pliance, inadequate dosage, and intrinsic corticosteroidresistance. Among steroid responders, the dose is slowlytapered to 5±10 mg.day-1 or an every other day regimen.Treatment should be continued for a minimum of 12 mon-ths. Occasionally, a patient with minimal disease of recentonset may respond to therapy over a 3±6 month period.Patients with LoÈfgren's syndrome do not require therapywith corticosteroids, unless a nonsteroidal agent is not ef-fective. In some patients, recurrent relapses will occur andpatients may require long-term, low-dose therapy.
Several cytotoxic agents have been used to treat sar-coidosis. While these agents clearly are of value in selectedpatients, there are no studies that have clearly delineatedwhen these drugs should be used for therapy. On the basisof safety and efficacy, methotrexate and azathioprine arethe preferred agents for most patients. Cyclophosphamideshould be reserved for refractory cases (table 3).
In patients with fibrotic disease, bronchiectasis oftencomplicates the disease. These patients often require anti-biotic therapy. A particular complication of bronchiectasisin sarcoidosis is aspergilloma. Fatal haemoptysis has beennoted by many groups. The antifungal agent itraconazolehas been used but no clinical trials have demonstrated effi-cacy. Surgical resection and embolization of the bronchialarteries have been reported as helpful in selected cases.Patients with myalgias and fatigue and those with signi-ficant respiratory insufficiency may benefit from pulmon-ary rehabilitation. Hypoxaemia at rest or with exercise mayrequire supplemental oxygen therapy. Lung and other or-gan transplantation has been successfully performed forpatients with end-stage sarcoidosis.
In summary, the information presented in this statementprovides an update of the current knowledge on sarcoid-osis. It is hoped that this expert consensus will be of valuefor clinicians and scientists involved in the management ofpatients with sarcoidosis.
Committee Members: G.W. Hunninghake (Co-chairman); U. Costabel(Co-chairman); M. Ando; R. Baughman; J-F. Cordier, R. du Bois; A.Eklund; M. Kitaichi; J. Lynch; G. Rizzato; C. Rose; O. Selroos; G.Semenzato; O.P. Sharma.
References
1. ATS/ERS/WASOG Committee. Statement on Sarcoid-osis. Am J Respir Crit Care Med 1999; 160: 736±755.
2. ATS/ERS/WASOG Committee. Statement on Sarcoid-osis. Sarcoidosis Vasc Diffuse Lung Dis 1999; 16: 149±173.
Table 3. ± Alternative therapy for sarcoidosis
Drug
Methotrexate Azathioprine Cyclophosphamide HydroxychloroquineDosage 10±25 mg.week-1 50±200 mg.day-1 50±150 mg.day-1 orally, or 500±2000 mg
every 2 weeks intravenously200±400 mg.day-1
ToxicityNausea* 1 2 3 1Mucosilis* 2 1 1 0Haematologic* 1 2 3 0Teratogenicity* 2 1 3 0Carcinogenic* 0 1 3 0Other Liver, lung Bladder Retinal
*: scale: 0=none; 1=minimal, 2=occasional problem, 3=significant problem; it may be necessary to adjust the dosage or to use other agents.
737STATEMENTS ON SARCOIDOSIS
93

Faculty disclosures
Prof. Dr Jouke T. Annema’s institution educational endosonography related activities have been
supported by Hitachi, Pentax and COOK.
Dr Juergen Hetzel has received hororarium for workshops and presentations from Erbe
Medizintechnik GmbH, Germany and Superdimension/Covidien.
Prof. Venerino Poletti has received Grants/research support from Roche, Boehringer Ing, Novartis,
Chiesi, as well as honoraria or consultation fees from Roche and Boehringer Ing.
Dr Erik H.F.M. van der Heijden in the past 3 years has received unrestricted research grants,
speaker’s fees and travel expenditure from: Ankie Hak Foundation, Hitachi Medical, MediGlobe,
MSD-oncology, Pentax Medical Europe and Pfizer Oncology.
94

Faculty contact information
Prof. Dr Jouke T. Annema
Academic Medical Center
Meibergdreef 9
1105 AZ Amsterdam
NETHERLANDS
Dr Johannes M.A. Daniels
VUmc University Medical Center Amsterdam
De Boelelaan 1118
1081 HV Amsterdam
NETHERLANDS
Prof. Marios E. Froudarakis
Pneumonology
Medical School of Alexandroupolis
Democritus University of Thrace
Dragana
681 00 Alexandroupolis
GREECE
Prof. Stefano Gasparini
Polytechnic University of Marche Region
Pulmonary Diseases Unit
Azienda Ospedali Riuniti
Via Conca 71
60020 Ancona
ITALY
Dr Juergen Hetzel
Department of Internal Medicine
Division of Pulmonary Medicine
University of Tübingen
Geschwister-Scholl-Platz
72074 Tübingen
GERMANY
Dr Julius P. Janssen
Dept of Pulmonary Diseases B01
Canisius Wilhelmina Hospital
Post box 9015
6500 GS Nijmegen
NETHERLANDS
Dr Mohammed Munavvar
Lancashire Teaching Hospitals NHS Foundation
Trust
Royal Preston Hospital
Sharoe Green Lane
Fulwood
Preston PR2 9HT
UNITED KINGDOM
Dr Masahide Oki
Department of Respiratory Medicine
Nagoya Medical Center
4-1-1 Sannomaru, Naka Ward,
Aichi Prefecture 460-0001 Nagoya
JAPAN
Prof. Venerino Poletti
Department of Diseases of the Thorax
Ospedale G.B. Morgagni
Via Carlo Forlanini 34
47100 Forlì
ITALY
Dr Najib Rahman
Oxford Centre for Respiratory Medicine
Churchill Hospital
Old Road
Headington
Oxford OX3 7LJ
UNITED KINGDOM
Dr Ales Rozman
University Clinic Golnik
Golnik 36
4206 Golnik
SLOVENIA
Dr Erik H.F.M. van der Heijden
Department of Pulmonary Diseases – 614
Radboud University Medical Center
P.O. Box 9101
6500 HB Nijmegen
NETHERLANDS
95

Dr Olga C.J. Schuurbiers
Department of Pulmonary Diseases
Radboud University Medical Center
P.O. Box 9101
6500 HB Nijmegen
NETHERLANDS
Dr Rocco Trisolini
Policlinico S. Orsola-Malpighi
Via Albertoni 15
40138 Bologna
ITALY
96