Line diagrams - skull base 360 - part 2
92
Dr.B.D.CHAURASIA - Great anatomist of india whose books inspired me to take up surgical field . Simplified the anatomy with line diagrams . Line diagrams - Skull base 360°- Part 2 28-12-2016 6.24 pm
-
Upload
murali-chand-nallamothu -
Category
Education
-
view
39 -
download
1
Transcript of Line diagrams - skull base 360 - part 2
Dr.B.D.CHAURASIA - Great anatomist of india whose books inspired me to take up surgical field . Simplified the anatomy with line diagrams .
Line diagrams - Skull base 360°- Part 2
28-12-2016 6.24 pm
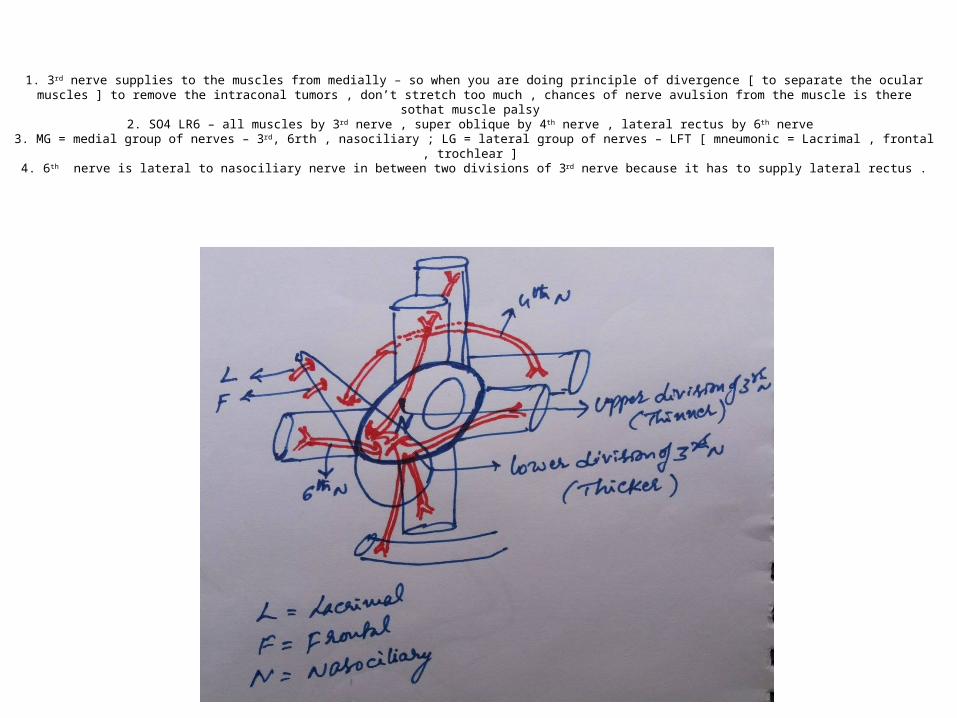
1. 3rd nerve supplies to the muscles from medially – so when you are doing principle of divergence [ to separate the ocular muscles ] to remove the intraconal tumors , don’t stretch too much , chances of nerve avulsion from the muscle is there sothat muscle palsy
2. SO4 LR6 – all muscles by 3rd nerve , super oblique by 4th nerve , lateral rectus by 6th nerve 3. MG = medial group of nerves – 3rd, 6rth , nasociliary ; LG = lateral group of nerves – LFT [ mneumonic = Lacrimal , frontal , trochlear ]
4. 6th nerve is lateral to nasociliary nerve in between two divisions of 3rd nerve because it has to supply lateral rectus .
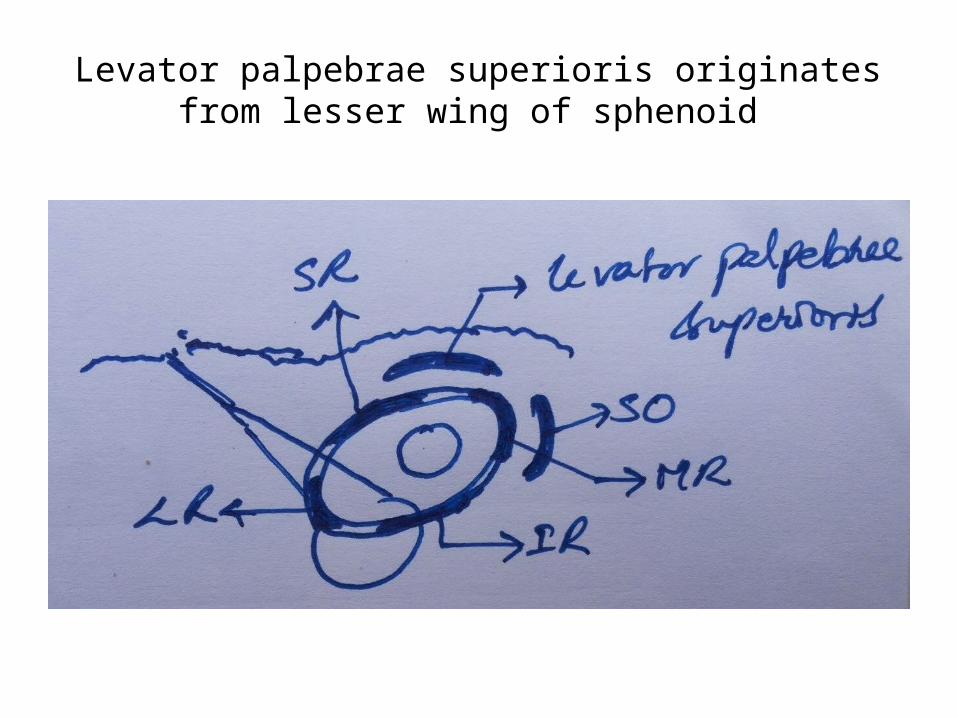
Levator palpebrae superioris originates from lesser wing of sphenoid
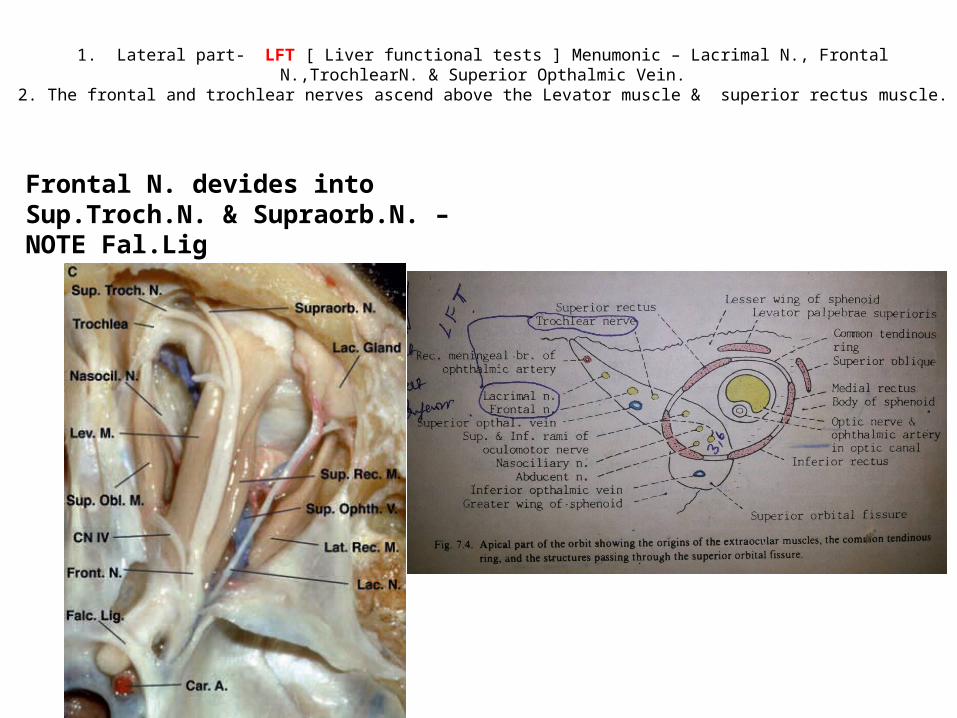
1. Lateral part- LFT [ Liver functional tests ] Menumonic – Lacrimal N., Frontal N.,TrochlearN. & Superior Opthalmic Vein.
2. The frontal and trochlear nerves ascend above the Levator muscle & superior rectus muscle.
Frontal N. devides into Sup.Troch.N. & Supraorb.N. – NOTE Fal.Lig
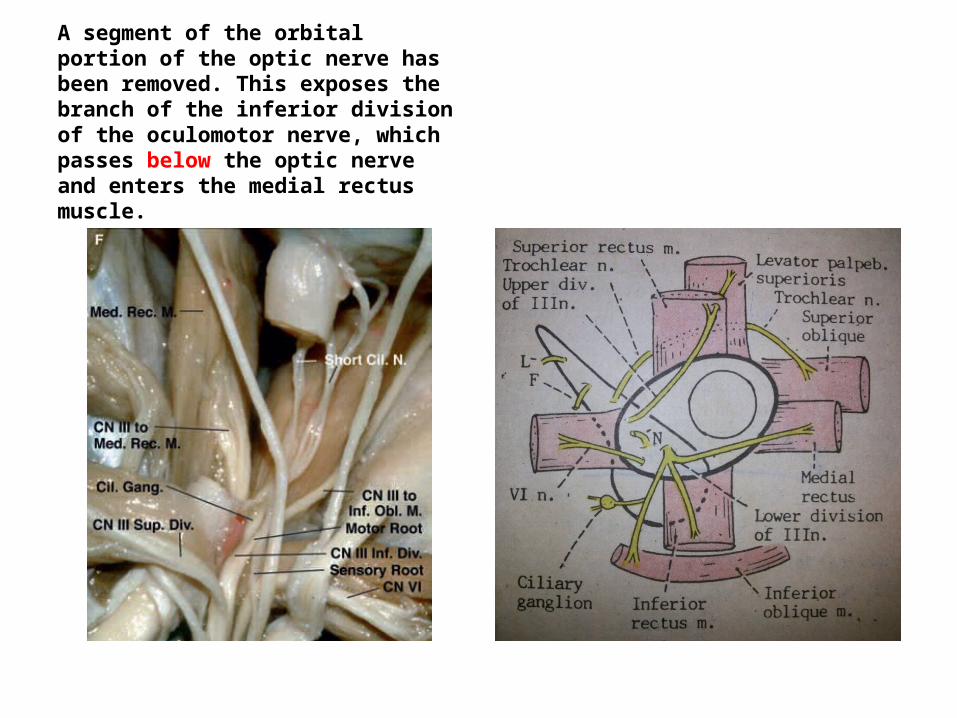
A segment of the orbital portion of the optic nerve has been removed. This exposes the branch of the inferior division of the oculomotor nerve, which passes below the optic nerve and enters the medial rectus muscle.
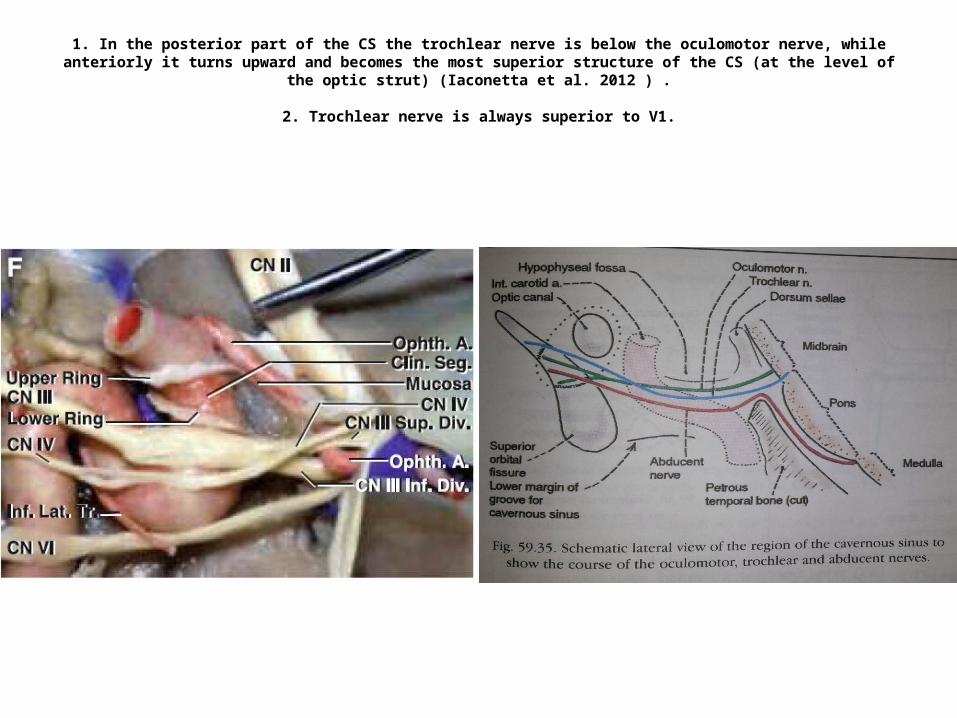
1. In the posterior part of the CS the trochlear nerve is below the oculomotor nerve, while anteriorly it turns upward and becomes the most superior structure of the CS (at the level of the optic strut) (Iaconetta et al. 2012 ) .
2. Trochlear nerve is always superior to V1.
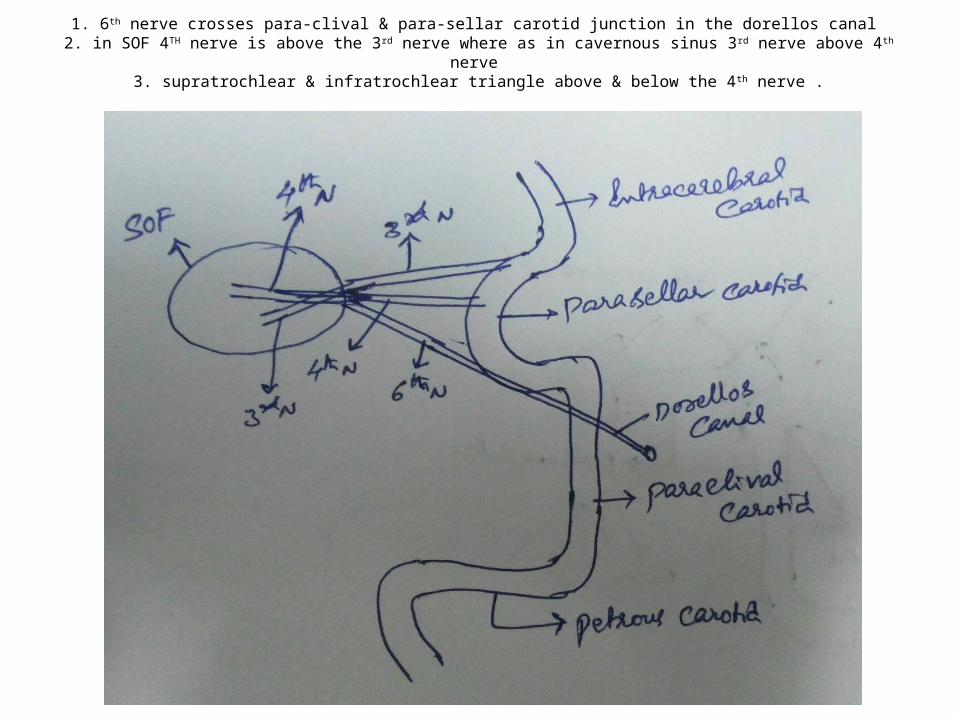
1. 6th nerve crosses para-clival & para-sellar carotid junction in the dorellos canal 2. in SOF 4TH nerve is above the 3rd nerve where as in cavernous sinus 3rd nerve above 4th nerve
3. supratrochlear & infratrochlear triangle above & below the 4th nerve .
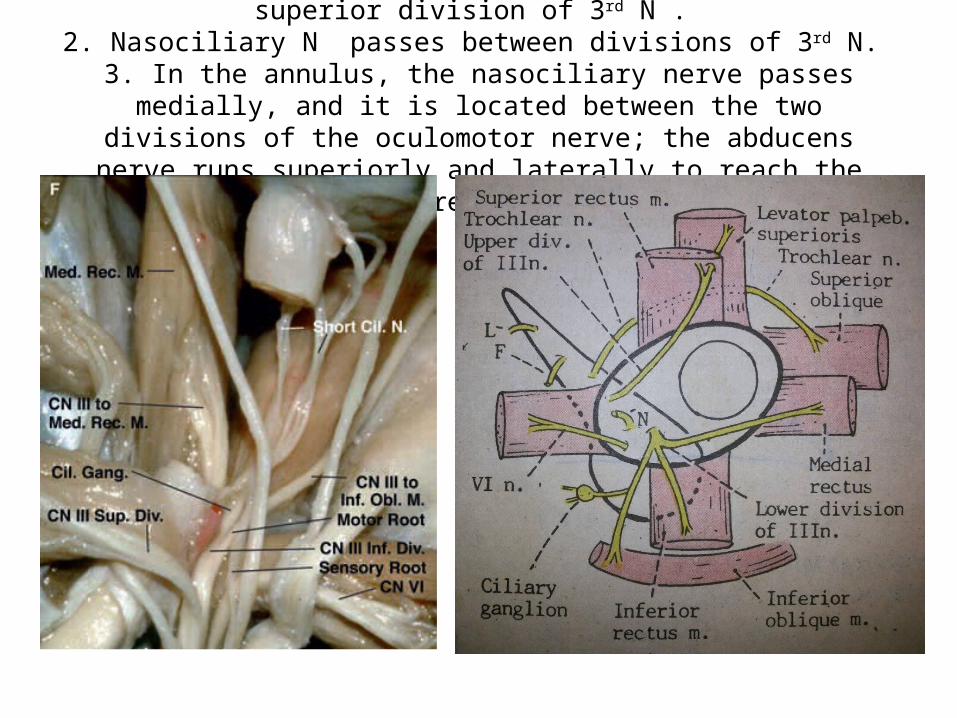
1. Thicker inferior division of 3rd N. & thinner superior division of 3rd N . 2. Nasociliary N passes between divisions of 3rd N.
3. In the annulus, the nasociliary nerve passes medially, and it is located between the two divisions of the oculomotor nerve; the abducens nerve runs
superiorly and laterally to reach the lateral rectus muscle.
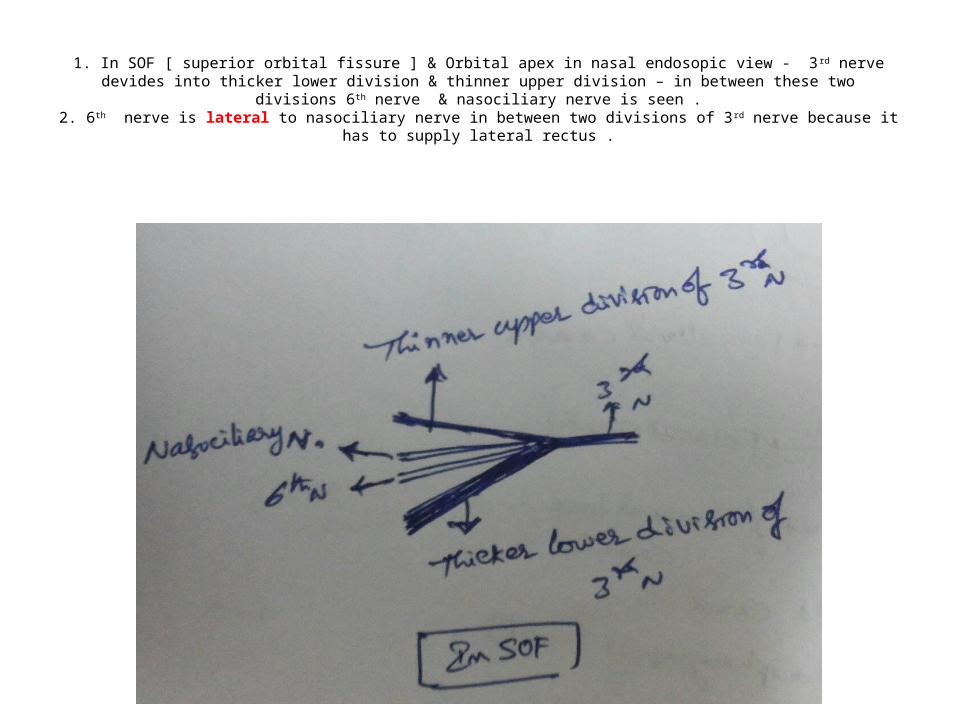
1. In SOF [ superior orbital fissure ] & Orbital apex in nasal endosopic view - 3rd nerve devides into thicker lower division & thinner upper division – in between these two divisions 6th nerve & nasociliary nerve is seen .
2. 6th nerve is lateral to nasociliary nerve in between two divisions of 3rd nerve because it has to supply lateral rectus .
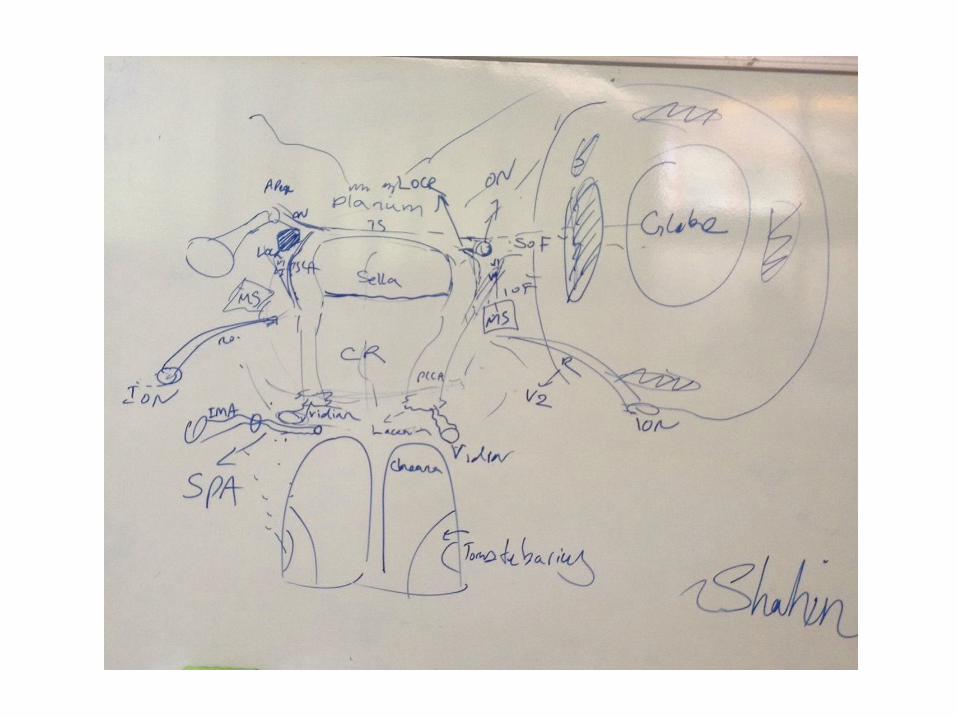
M-OCR
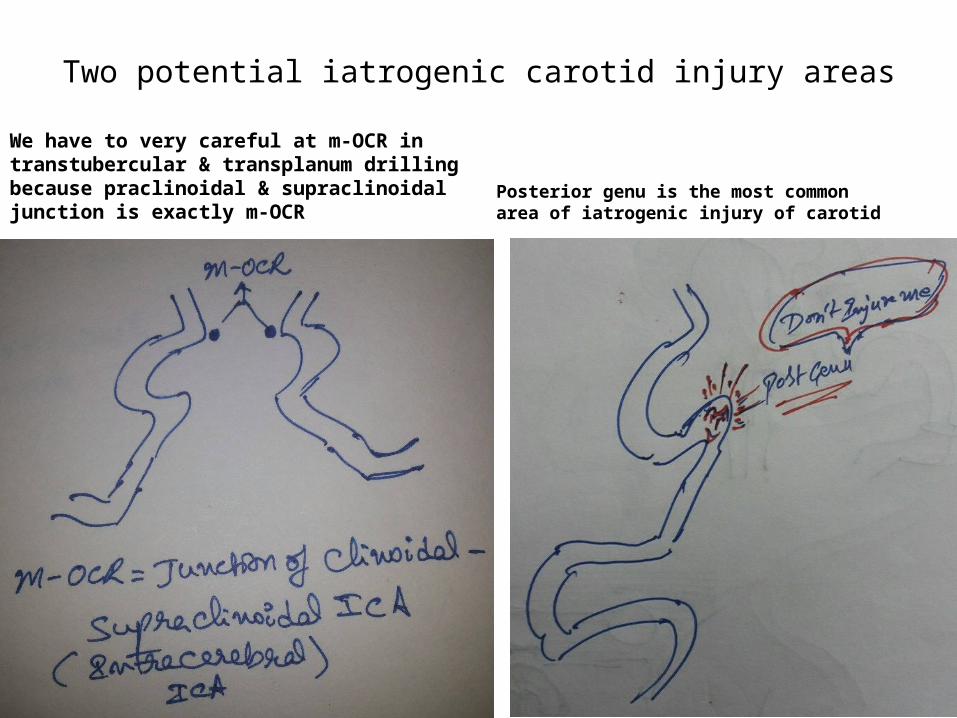
Two potential iatrogenic carotid injury areas
We have to very careful at m-OCR in transtubercular & transplanum drilling because praclinoidal & supraclinoidal junction is exactly m-OCR
Posterior genu is the most common area of iatrogenic injury of carotid
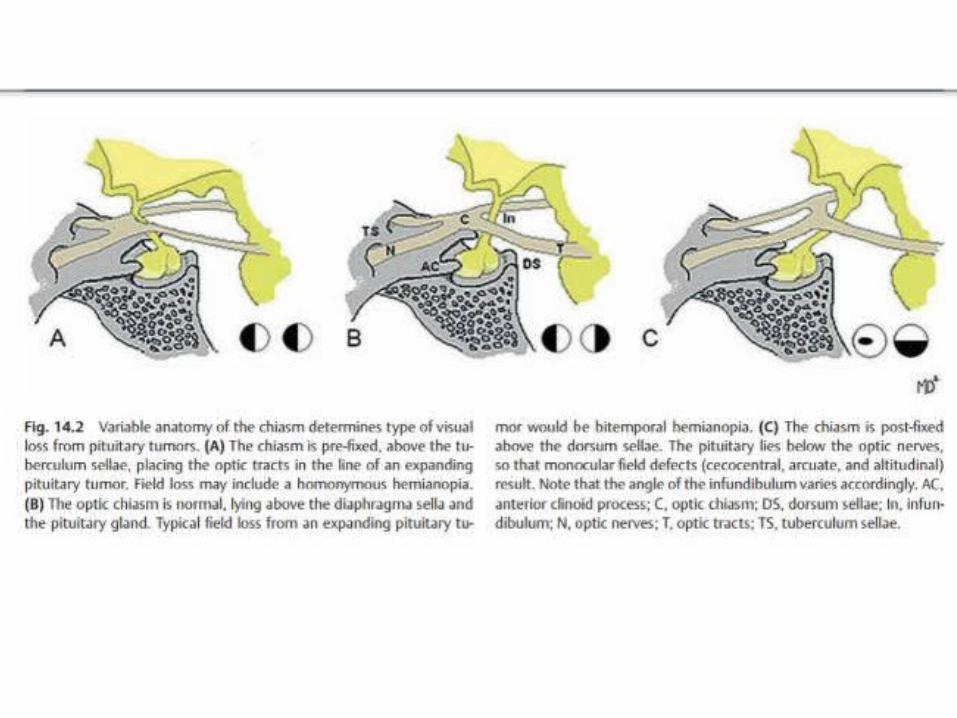
The optic chiasm is referred to as prefixed when it is located above the tuberculum sellae and as a postfixed chiasm when it is situated superior
to the dorsum sellae
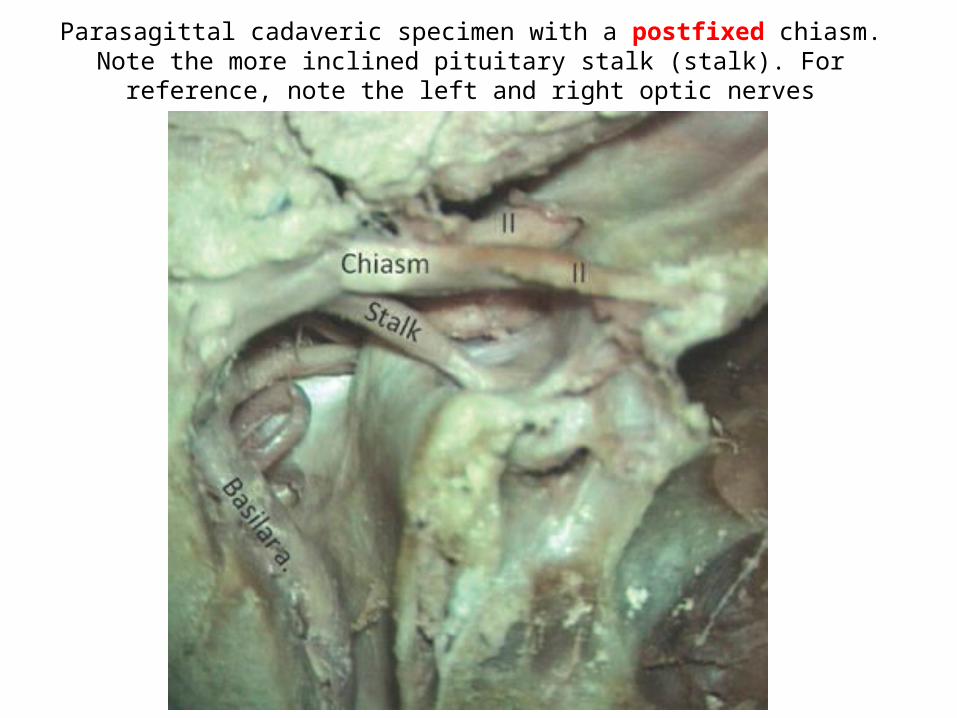
Parasagittal cadaveric specimen with a postfixed chiasm. Note the more inclined pituitary stalk (stalk). For reference, note the left and right optic
nerves
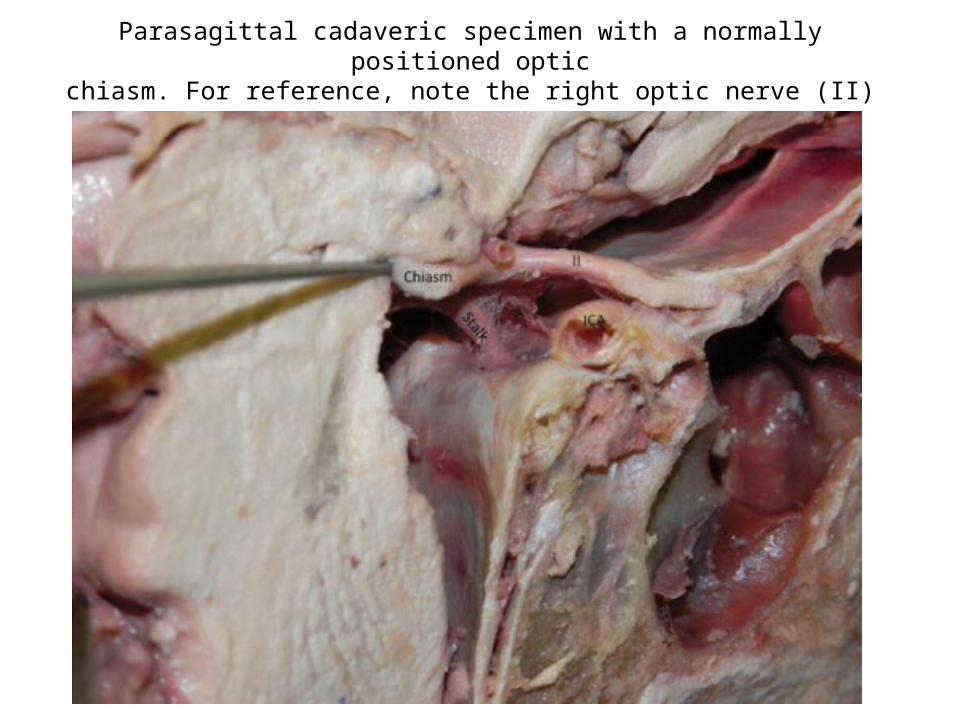
Parasagittal cadaveric specimen with a normally positioned opticchiasm. For reference, note the right optic nerve (II)
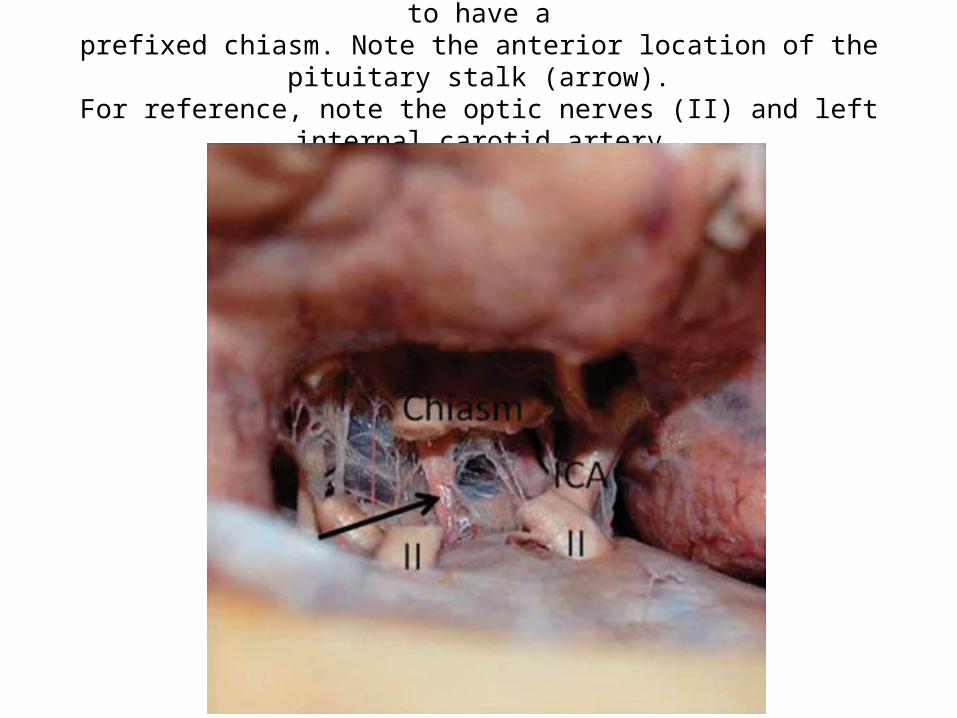
Subfrontal cadaveric dissection in a specimen found to have aprefixed chiasm. Note the anterior location of the pituitary stalk (arrow).
For reference, note the optic nerves (II) and left internal carotid artery(ICA)
Opthalmic artery
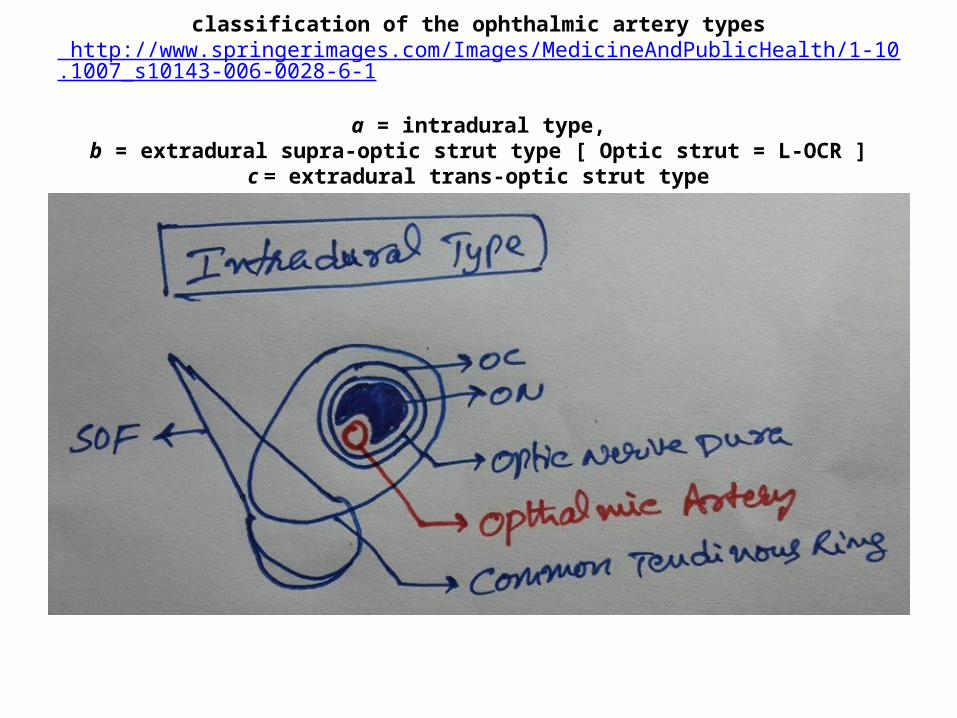
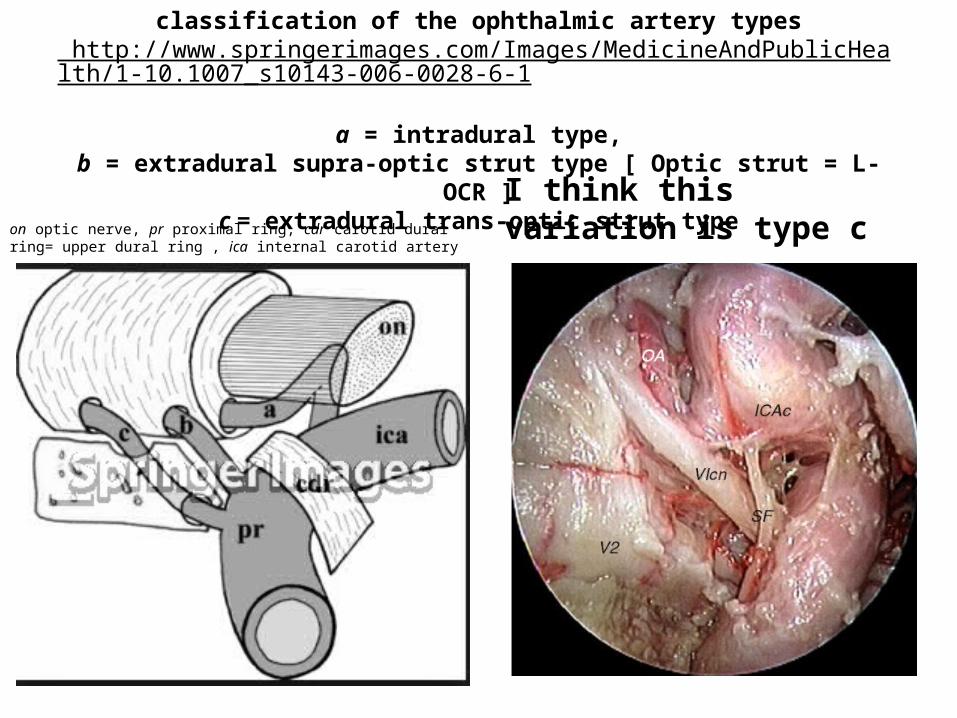
classification of the ophthalmic artery types http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s10143-006-0028-6-1
a = intradural type,
b = extradural supra-optic strut type [ Optic strut = L-OCR ]c = extradural trans-optic strut type
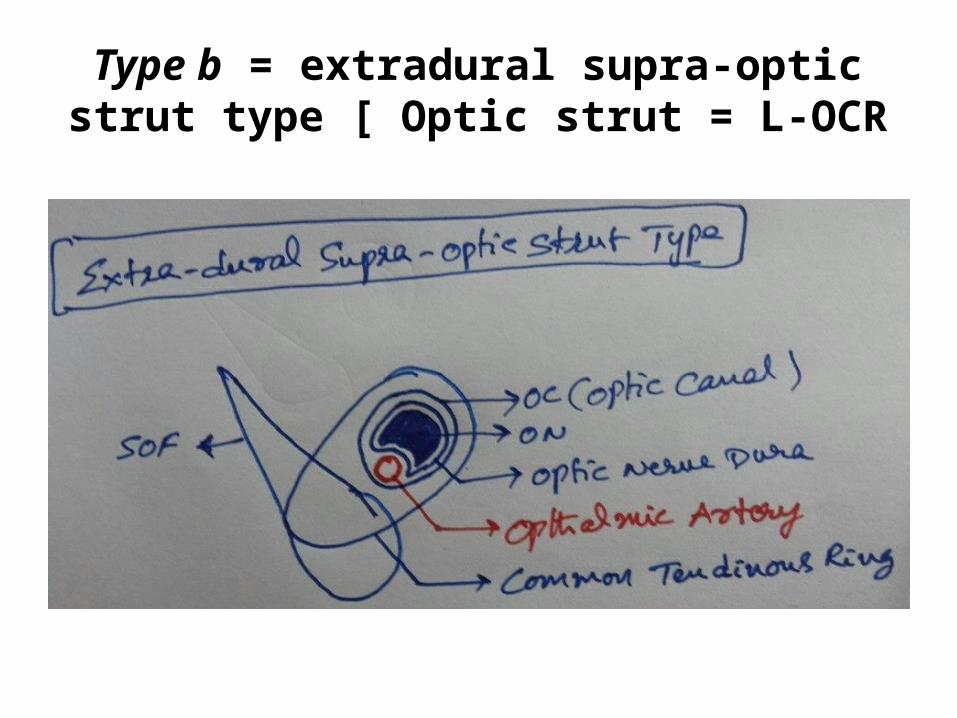
Type b = extradural supra-optic strut type [ Optic strut = L-OCR
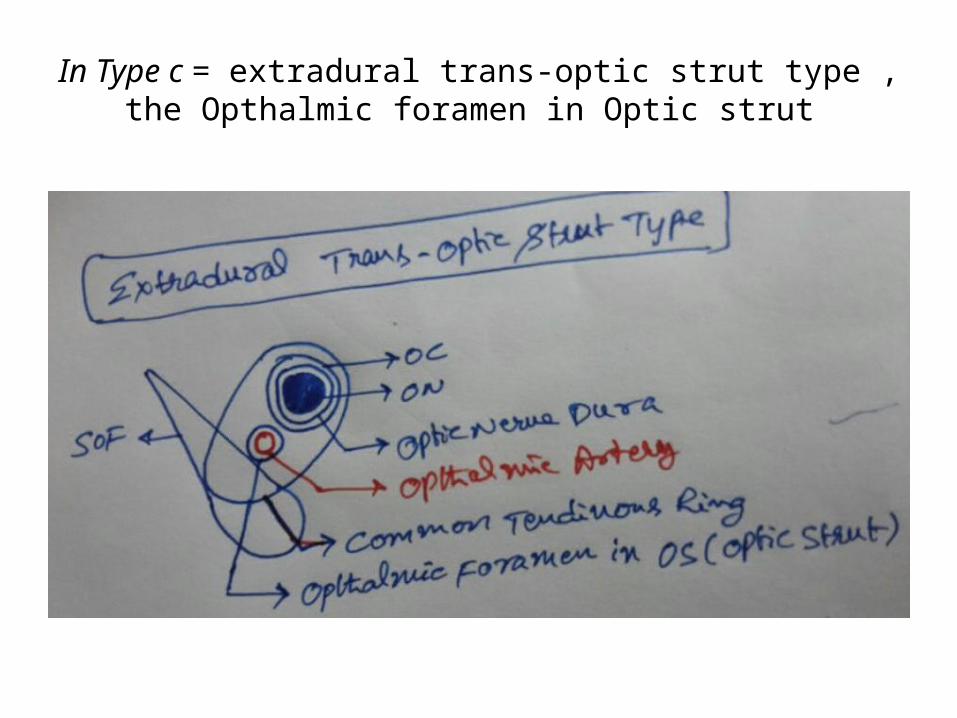
In Type c = extradural trans-optic strut type , the Opthalmic foramen in Optic strut
classification of the ophthalmic artery types http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s10143-006-0028-6-1
a = intradural type,
b = extradural supra-optic strut type [ Optic strut = L-OCR ]c = extradural trans-optic strut typeon optic nerve, pr proximal ring, cdr carotid dural
ring= upper dural ring , ica internal carotid artery I think this variation is type c
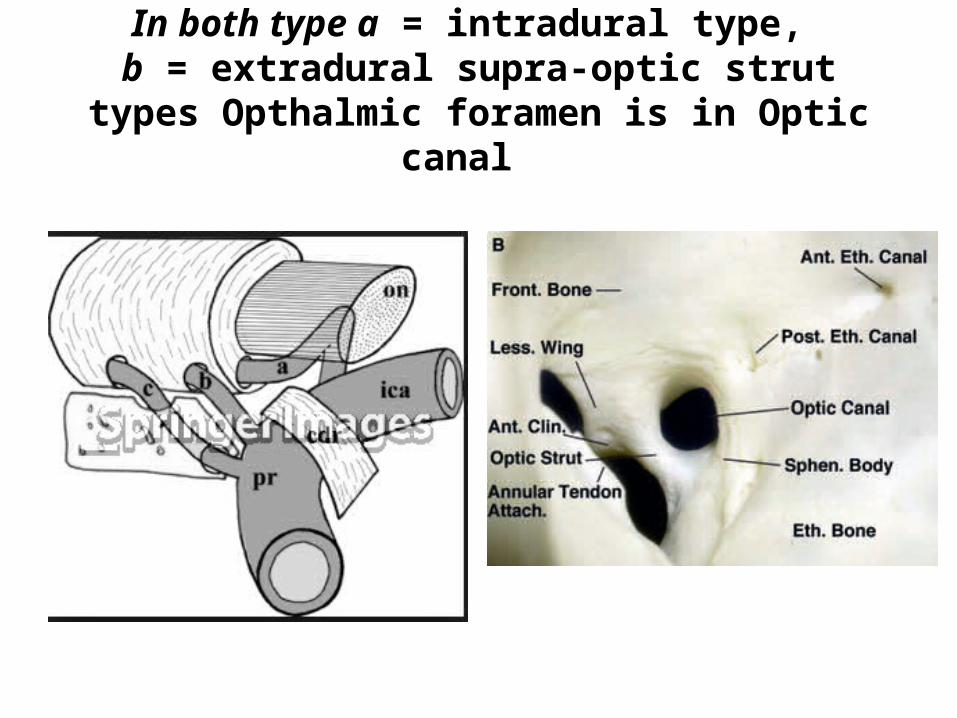
In both type a = intradural type, b = extradural supra-optic strut types Opthalmic
foramen is in Optic canal
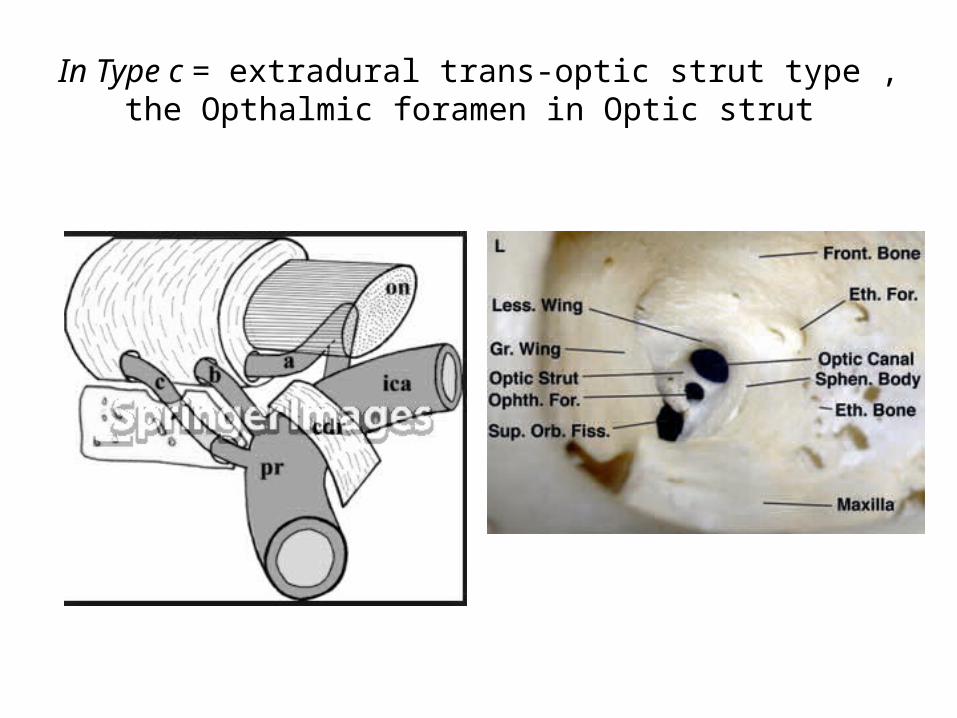
In Type c = extradural trans-optic strut type , the Opthalmic foramen in Optic strut
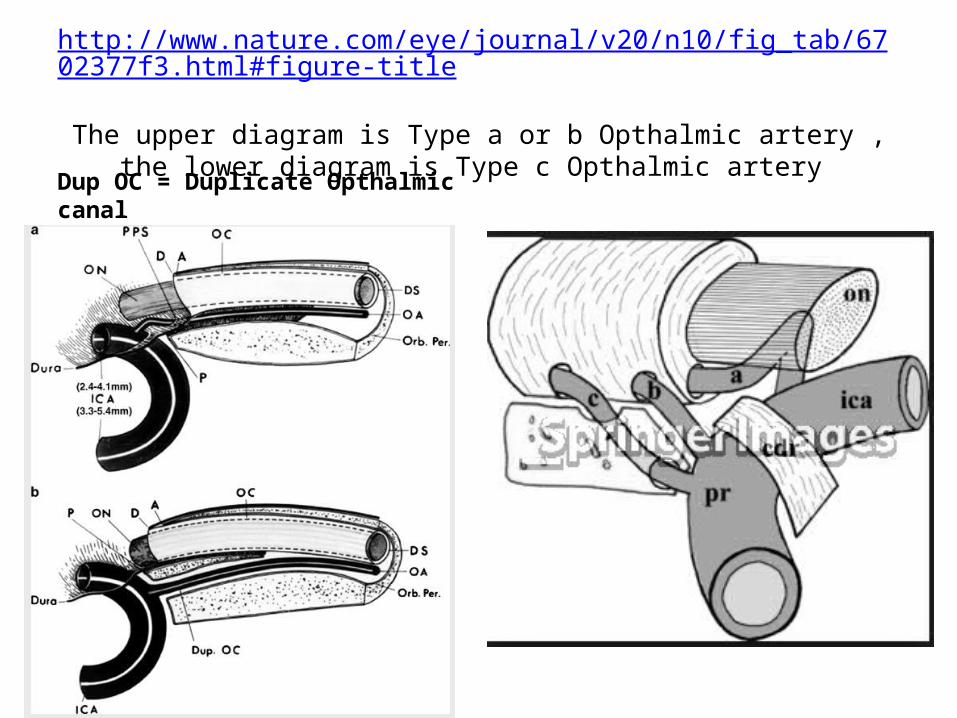
http://www.nature.com/eye/journal/v20/n10/fig_tab/6702377f3.html#figure-title
The upper diagram is Type a or b Opthalmic artery , the lower diagram is Type c Opthalmic artery
Dup OC = Duplicate Opthalmic canal
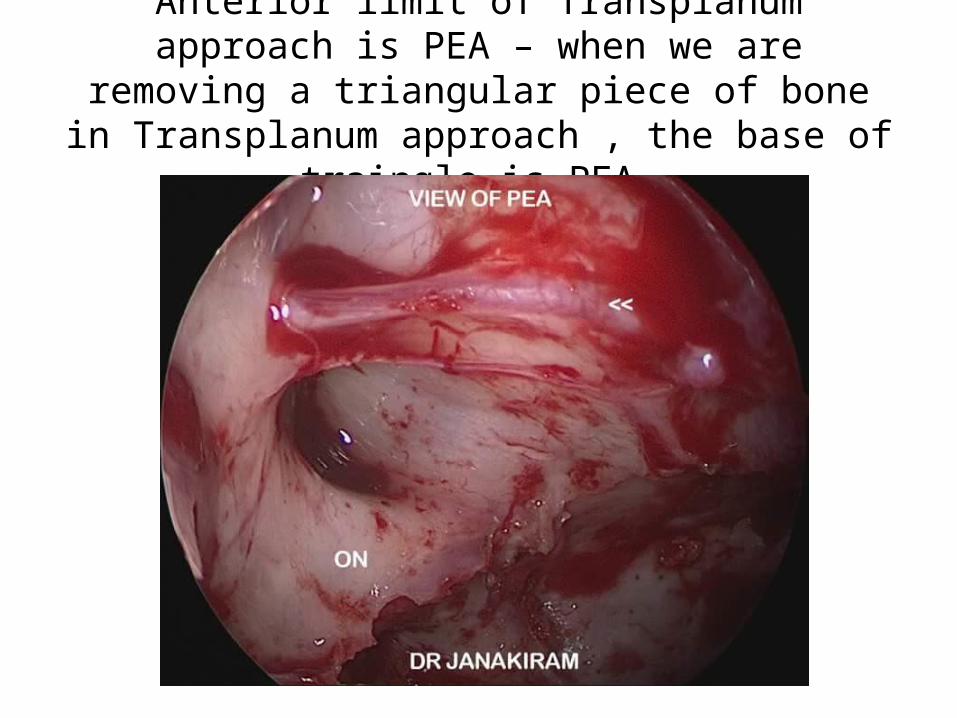
Anterior limit of Transplanum approach is PEA – when we are removing a triangular piece of bone in
Transplanum approach , the base of traingle is PEA
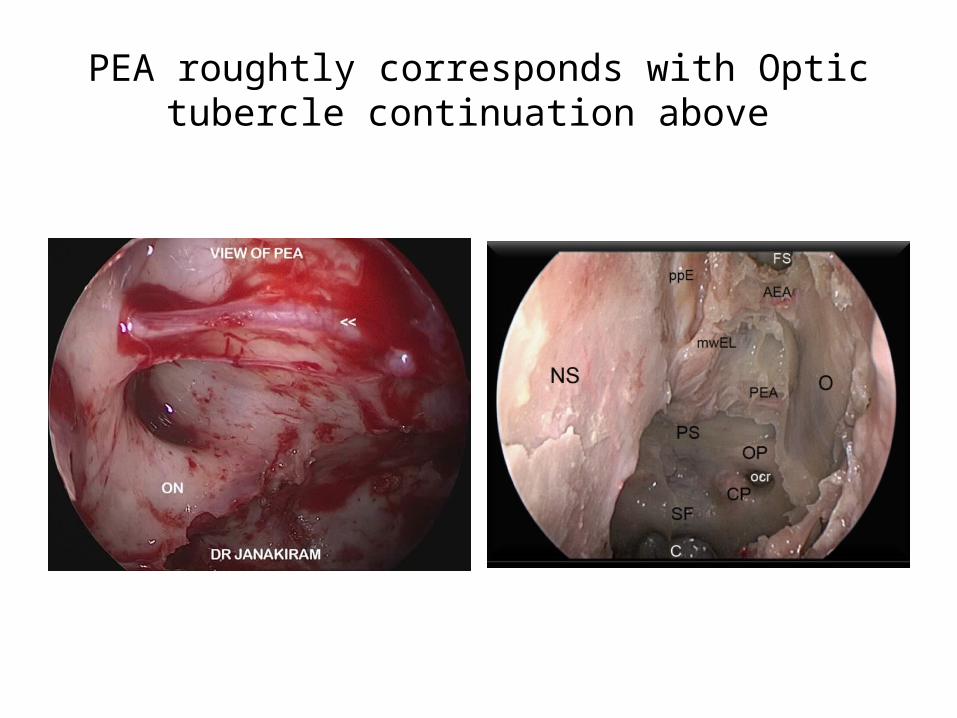
PEA roughtly corresponds with Optic tubercle continuation above
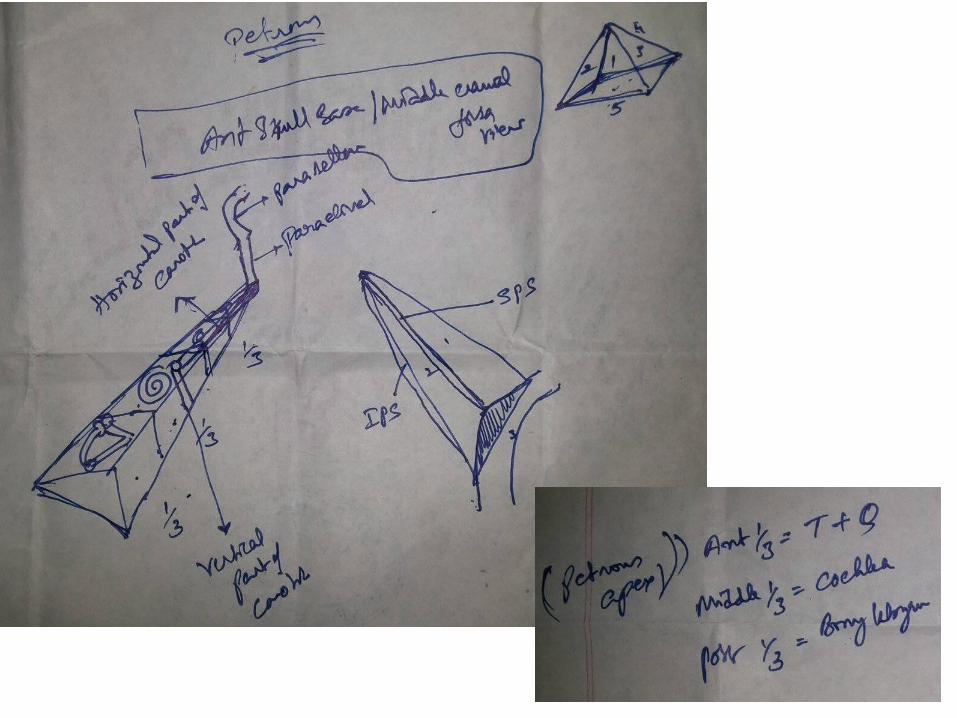
Petrous apex
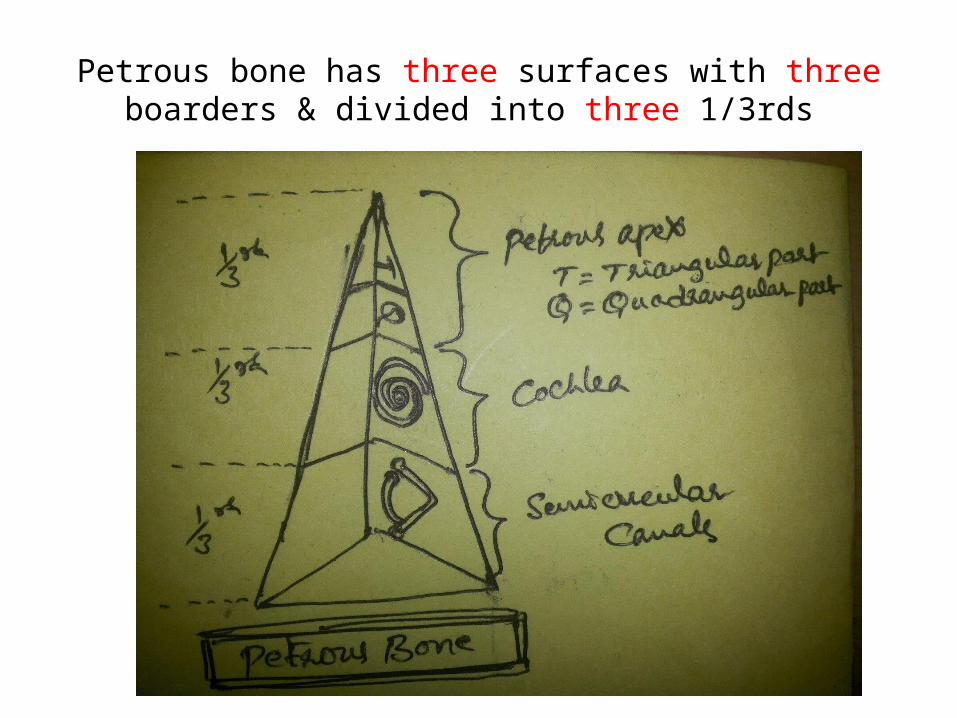
Petrous bone has three surfaces with three boarders & divided into three 1/3rds
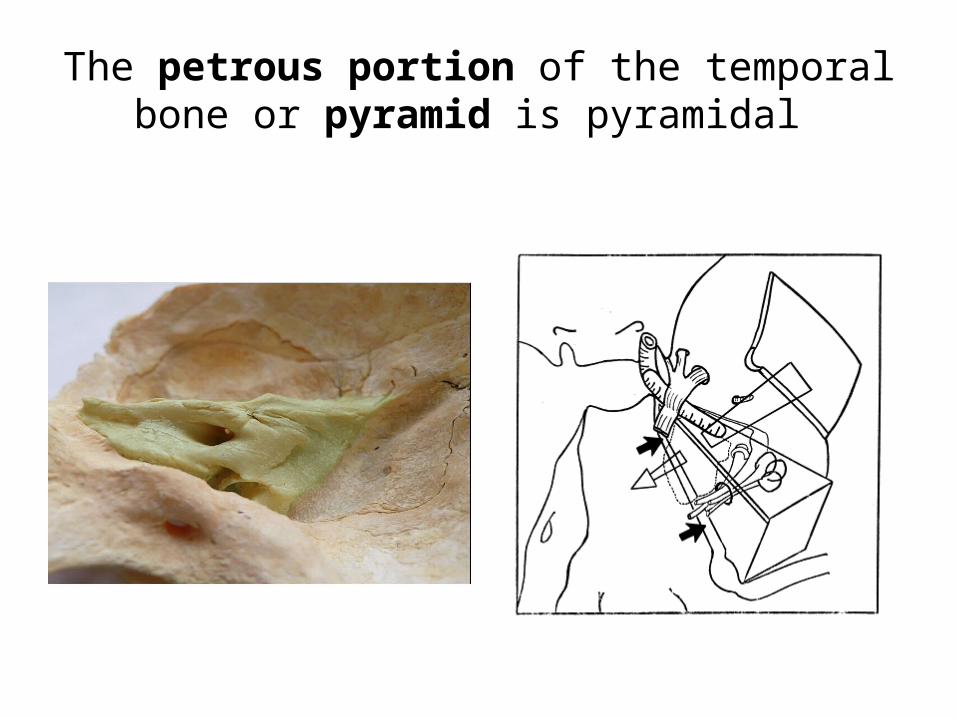
The petrous portion of the temporal bone or pyramid is pyramidal
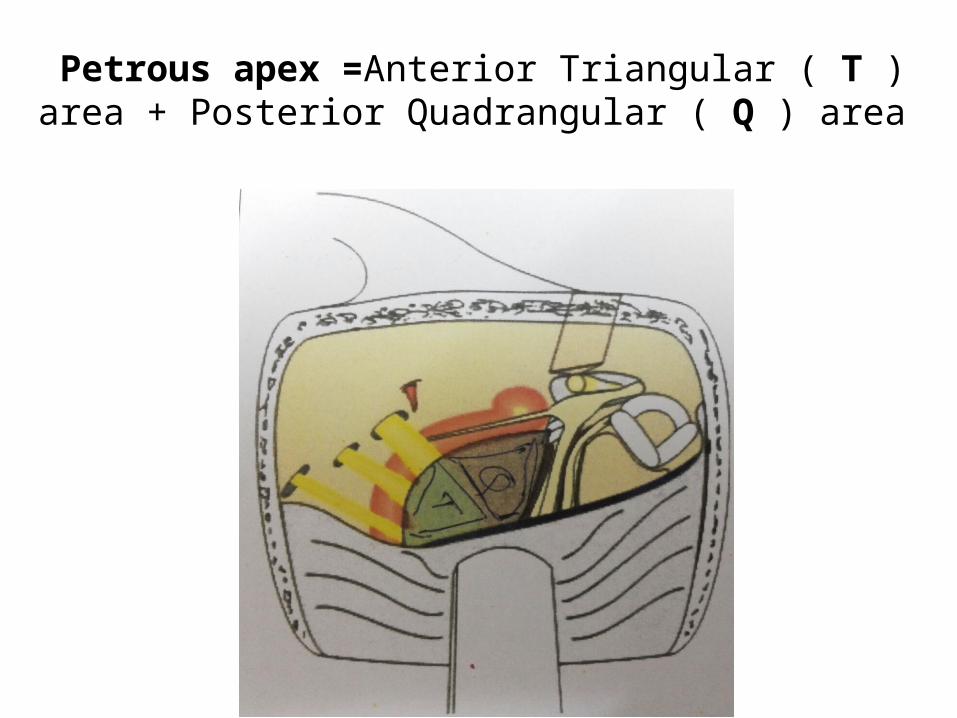
Petrous apex =Anterior Triangular ( T ) area + Posterior Quadrangular ( Q ) area
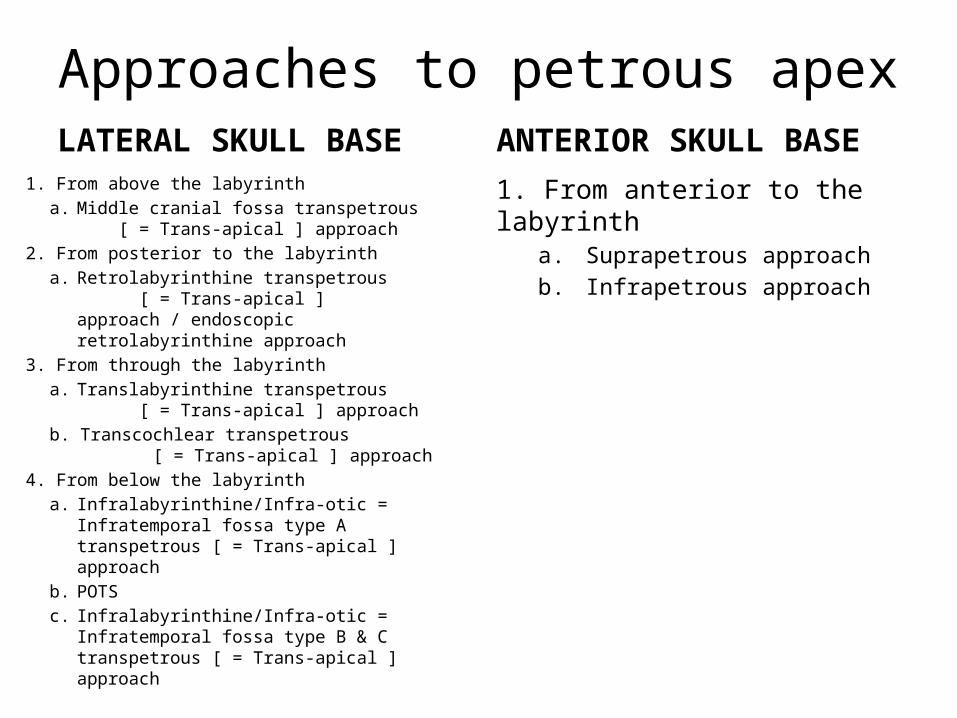
Approaches to petrous apex LATERAL SKULL BASE
1. From above the labyrinth a. Middle cranial fossa transpetrous [ =
Trans-apical ] approach 2. From posterior to the labyrinth
a. Retrolabyrinthine transpetrous [ = Trans-apical ] approach / endoscopic retrolabyrinthine approach
3. From through the labyrintha. Translabyrinthine transpetrous [ =
Trans-apical ] approach b. Transcochlear transpetrous [ =
Trans-apical ] approach4. From below the labyrinth
a. Infralabyrinthine/Infra-otic = Infratemporal fossa type A transpetrous [ = Trans-apical ] approach
b. POTSc. Infralabyrinthine/Infra-otic =
Infratemporal fossa type B & C transpetrous [ = Trans-apical ] approach
ANTERIOR SKULL BASE1. From anterior to the labyrinth
a. Suprapetrous approachb. Infrapetrous approach

Lateral skull base view
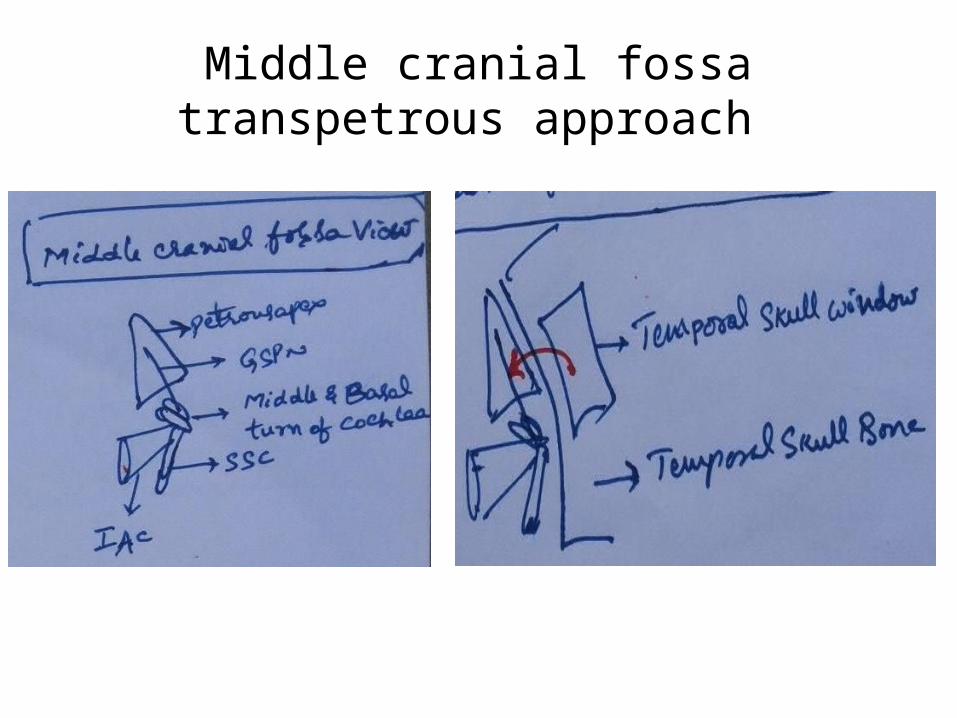
Middle cranial fossa transpetrous approach
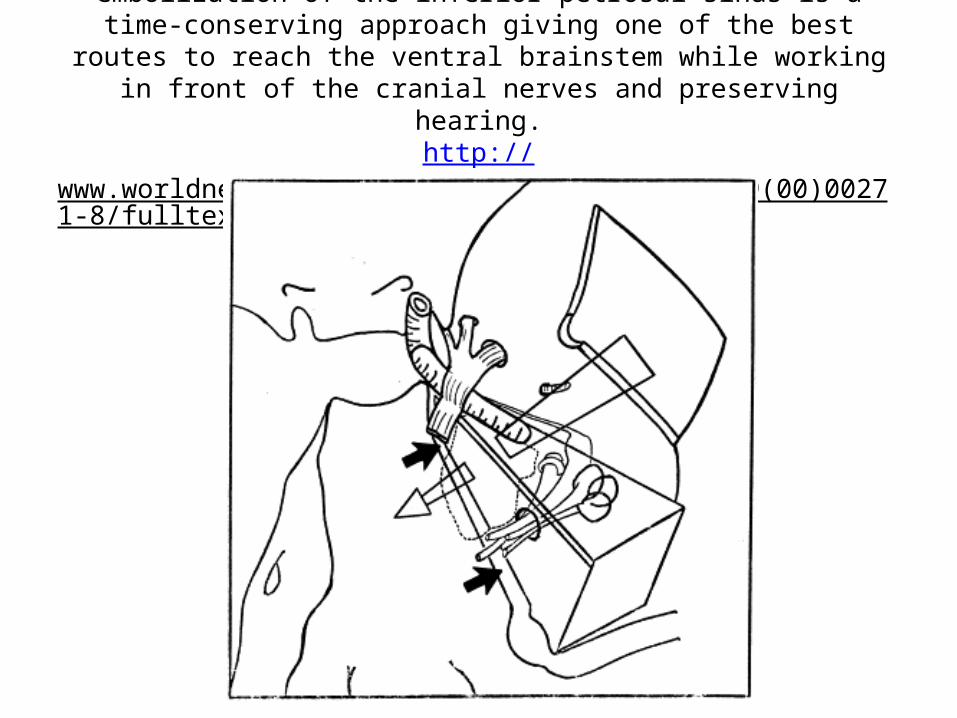
the anterior petrosectomy with preoperative embolization of the inferior petrosal sinus is a time-conserving approach giving one of the best routes to reach the ventral brainstem while working in front of the cranial nerves and
preserving hearing.http://www.worldneurosurgery.org/article/S0090-3019(00)00271-8/fulltext
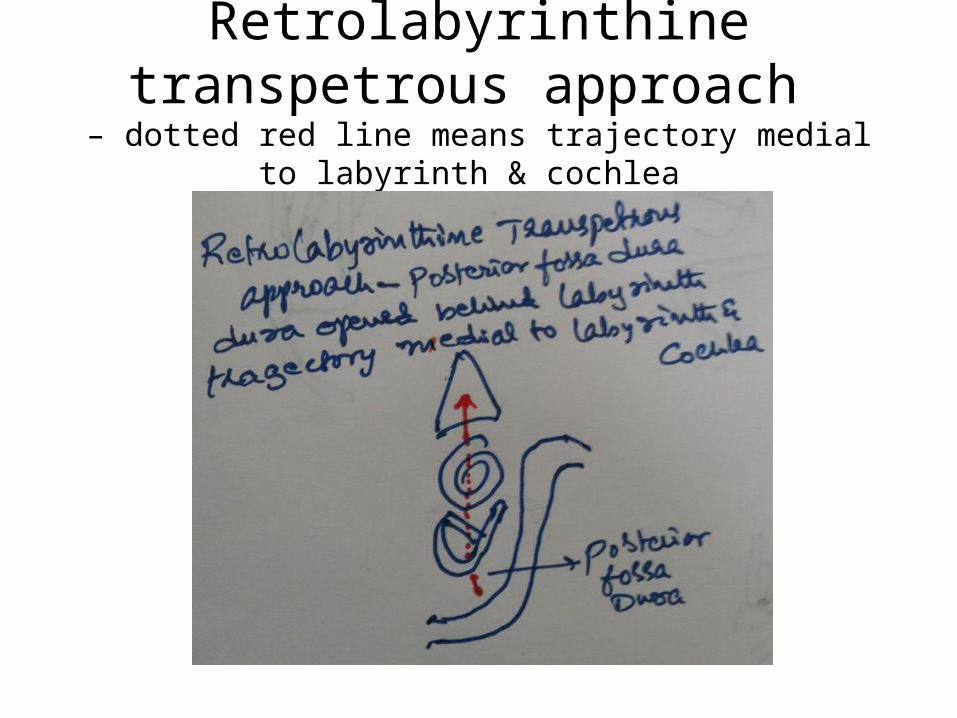
Retrolabyrinthine transpetrous approach
– dotted red line means trajectory medial to labyrinth & cochlea
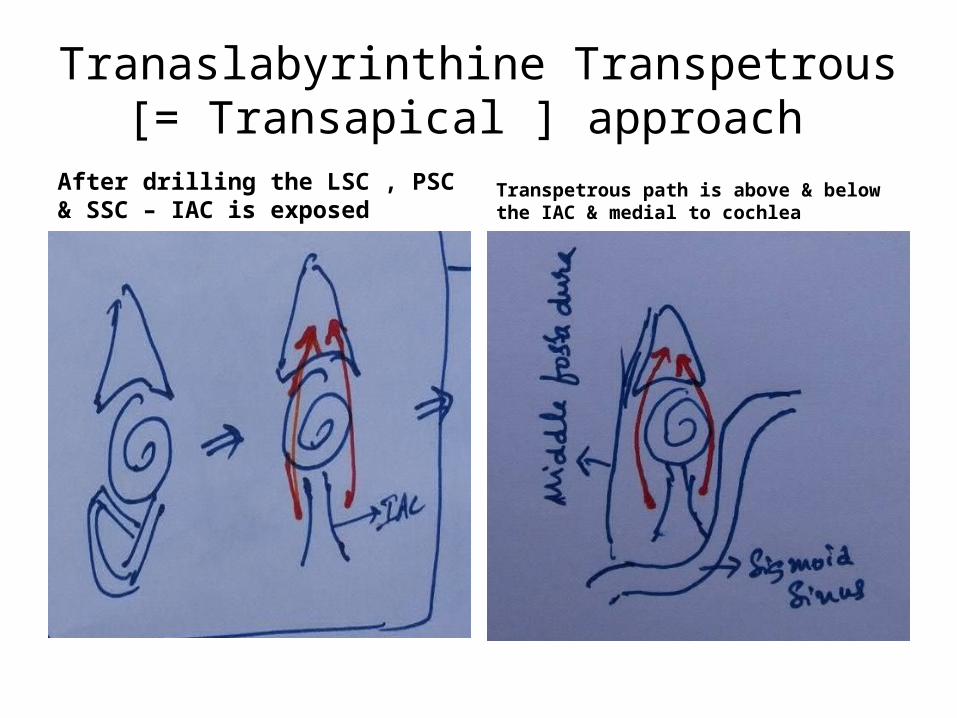
Tranaslabyrinthine Transpetrous [= Transapical ] approach
After drilling the LSC , PSC & SSC – IAC is exposed
Transpetrous path is above & below the IAC & medial to cochlea
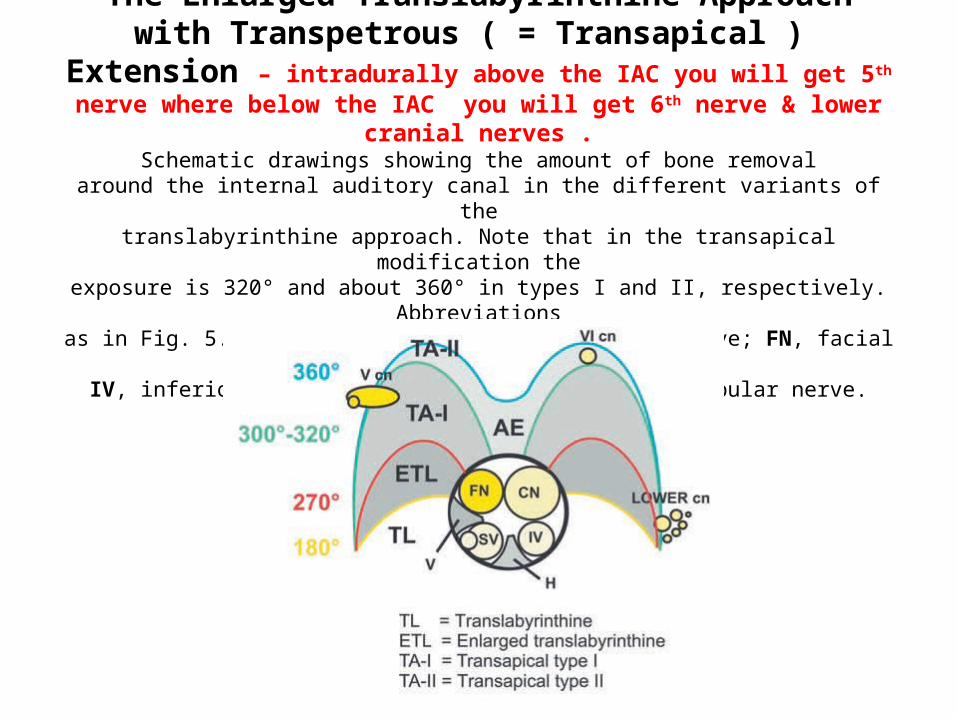
The Enlarged Translabyrinthine Approach with Transpetrous ( = Transapical ) Extension – intradurally above the IAC you will get 5th nerve
where below the IAC you will get 6th nerve & lower cranial nerves .Schematic drawings showing the amount of bone removal
around the internal auditory canal in the different variants of thetranslabyrinthine approach. Note that in the transapical modification the
exposure is 320° and about 360° in types I and II, respectively. Abbreviationsas in Fig. 5.1. cn, cranial nerve; CN, cochlear nerve; FN, facial nerve;
IV, inferior vestibular nerve; SV, superior vestibular nerve.
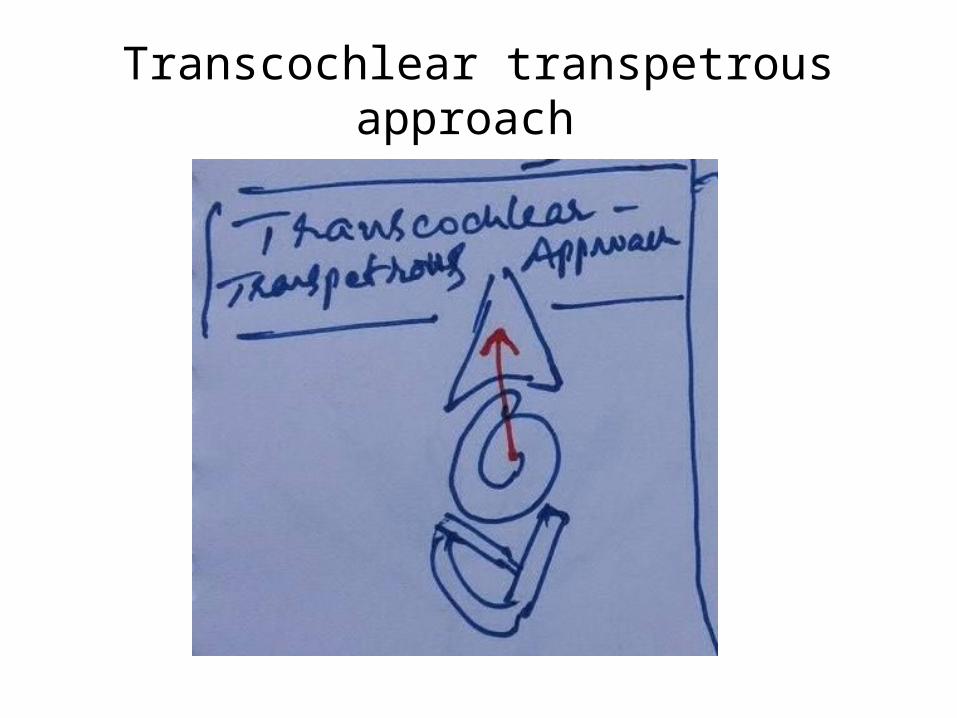
Transcochlear transpetrous approach
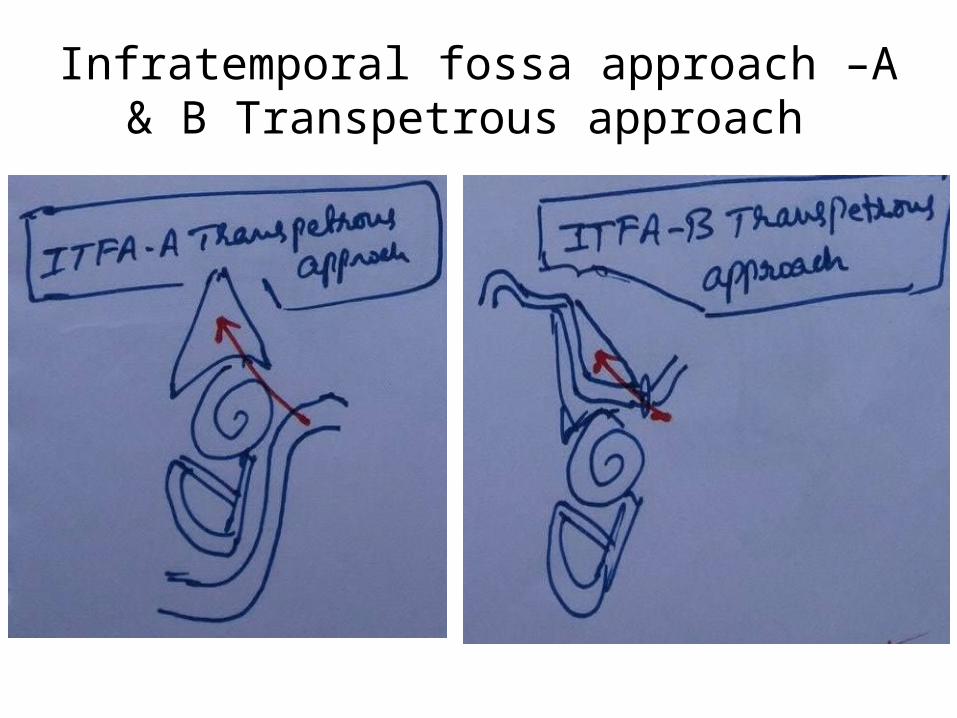
Infratemporal fossa approach –A & B Transpetrous approach
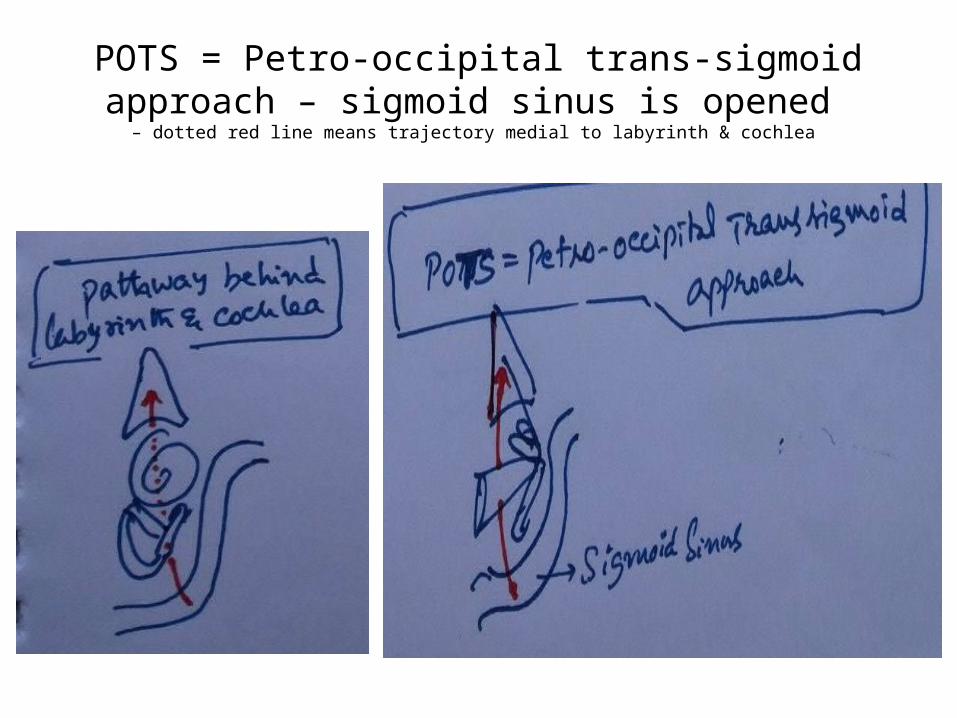
POTS = Petro-occipital trans-sigmoid approach – sigmoid sinus is opened
– dotted red line means trajectory medial to labyrinth & cochlea
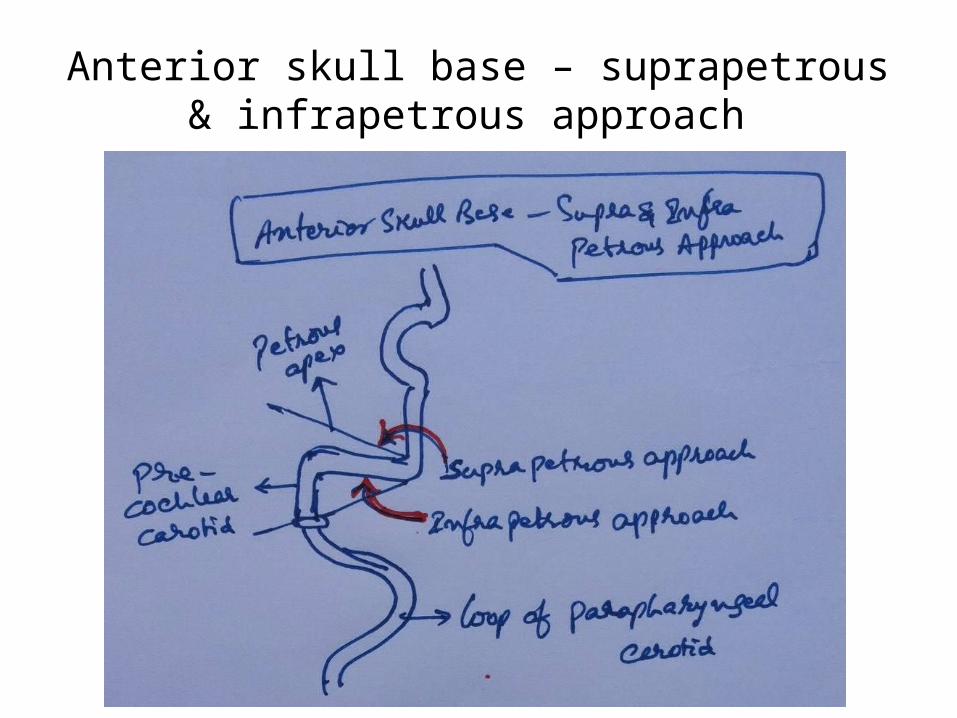
Anterior skull base – suprapetrous & infrapetrous approach
CP angle
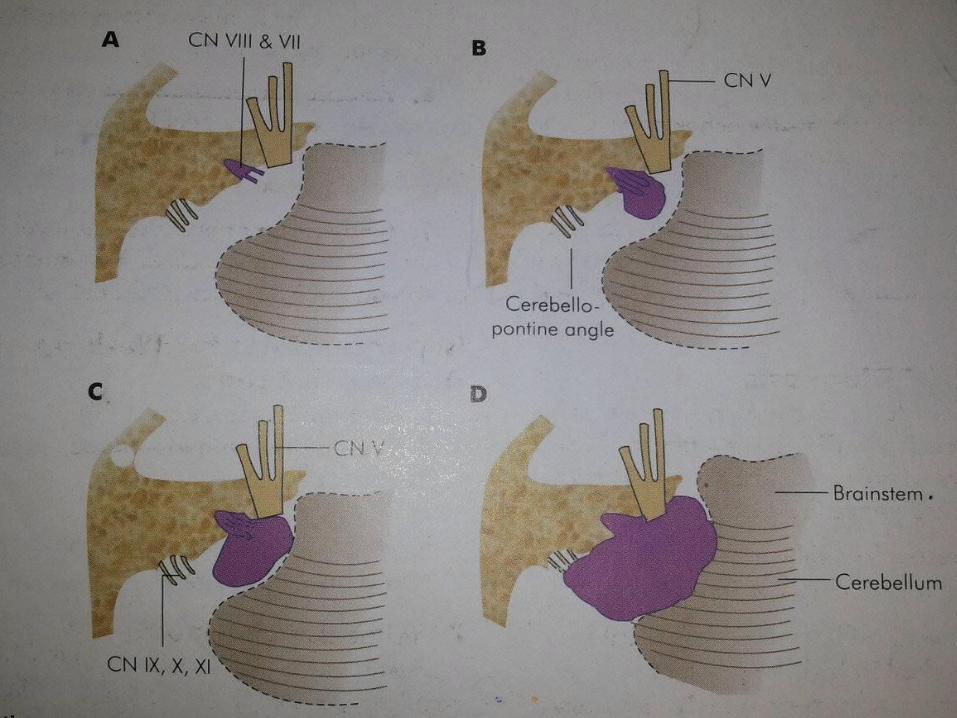
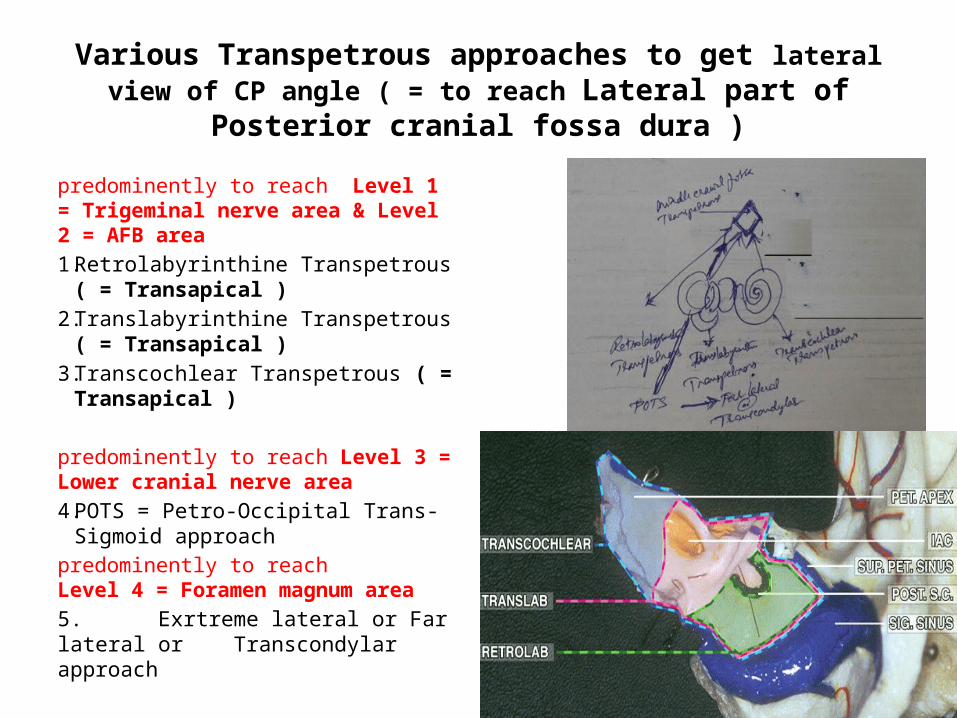
Various Transpetrous approaches to get lateral view of CP angle ( = to reach Lateral part of Posterior cranial fossa dura )
predominently to reach Level 1 = Trigeminal nerve area & Level 2 = AFB area1. Retrolabyrinthine Transpetrous ( =
Transapical )2. Translabyrinthine Transpetrous ( =
Transapical )3. Transcochlear Transpetrous ( =
Transapical )
predominently to reach Level 3 = Lower cranial nerve area4. POTS = Petro-Occipital Trans-Sigmoid
approach predominently to reach Level 4 = Foramen magnum area5. Exrtreme lateral or Far lateral or Transcondylar approach
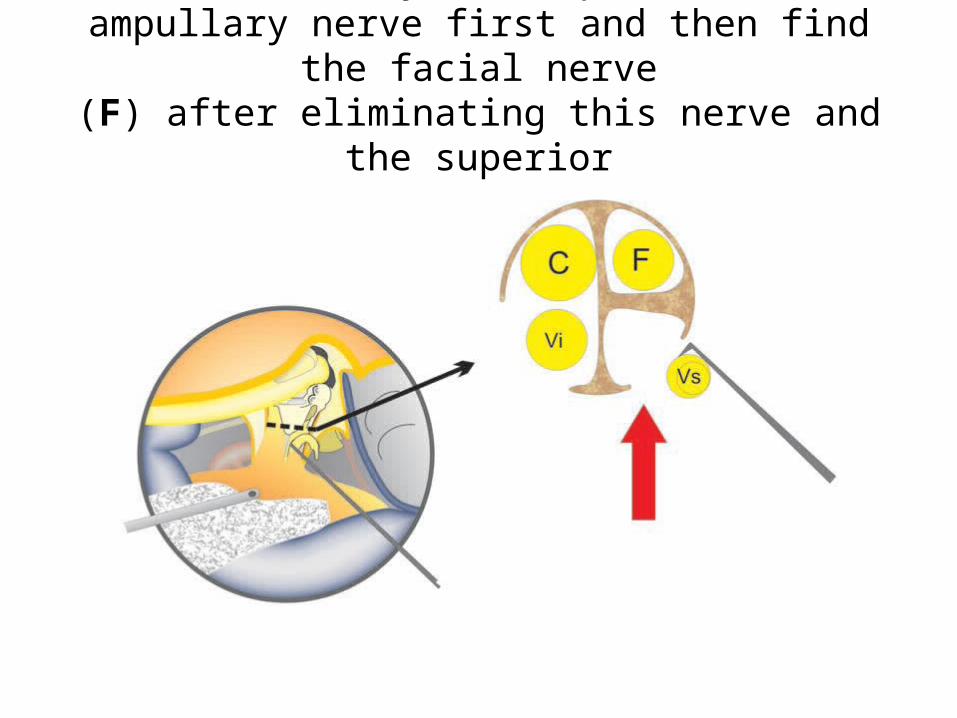
identify the superiorampullary nerve first and then find the facial nerve
(F) after eliminating this nerve and the superiorvestibular nerve (Vs).

The Enlarged Translabyrinthine Approach with Transpetrous ( = Transapical ) Extension – intradurally above the IAC you will get 5th nerve
where below the IAC you will get 6th nerve & lower cranial nerves .Schematic drawings showing the amount of bone removal
around the internal auditory canal in the different variants of thetranslabyrinthine approach. Note that in the transapical modification the
exposure is 320° and about 360° in types I and II, respectively. Abbreviationsas in Fig. 5.1. cn, cranial nerve; CN, cochlear nerve; FN, facial nerve;
IV, inferior vestibular nerve; SV, superior vestibular nerve.

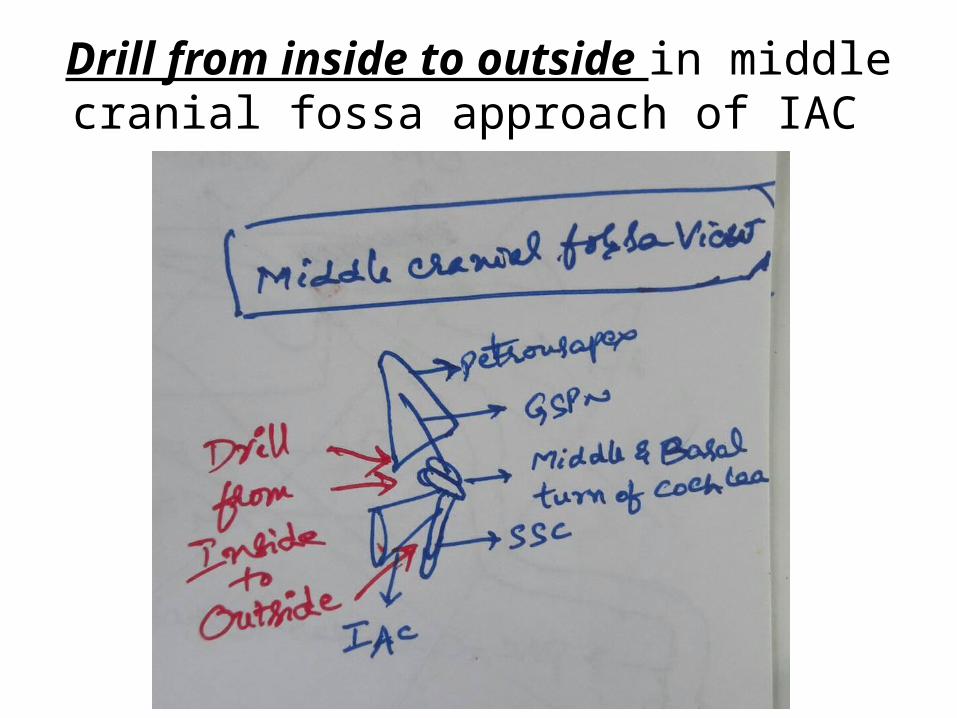
Drill from inside to outside in middle cranial fossa approach of IAC
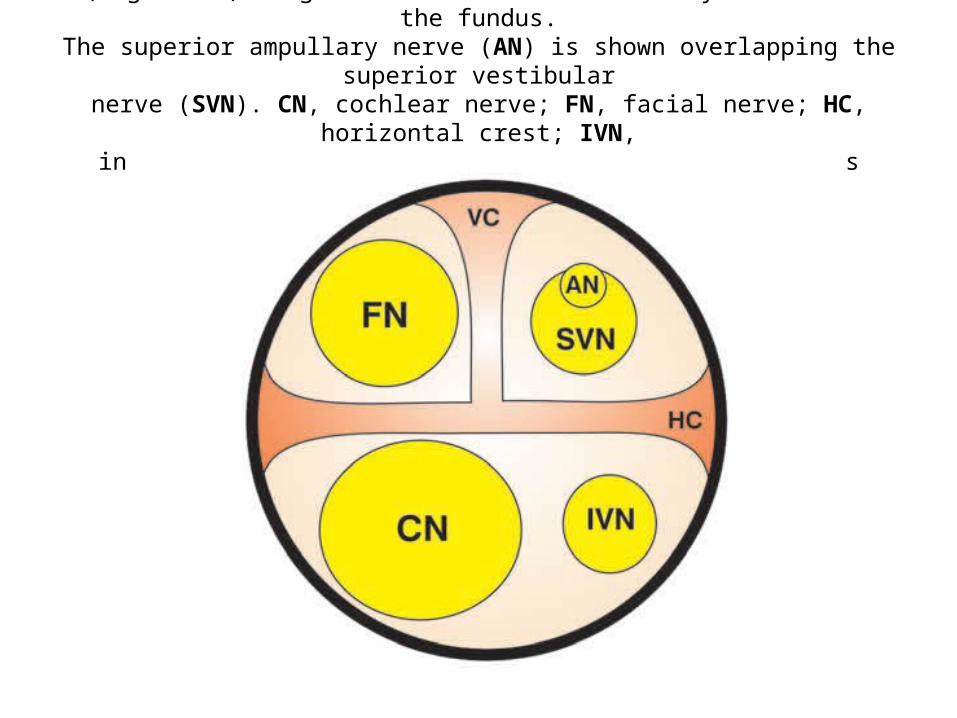
(Right ear) Diagram of the internal auditory canal near the fundus.The superior ampullary nerve (AN) is shown overlapping the superior vestibular
nerve (SVN). CN, cochlear nerve; FN, facial nerve; HC, horizontal crest; IVN,inferior vestibular nerve; VC, vertical crest (Bill’s bar).
Cranial nerves

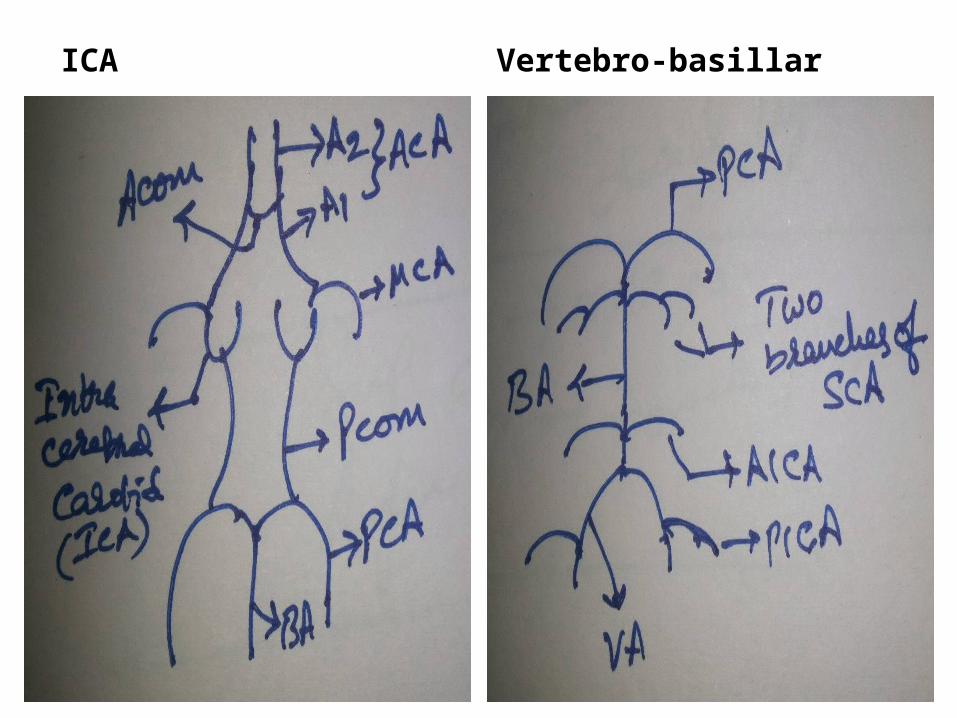
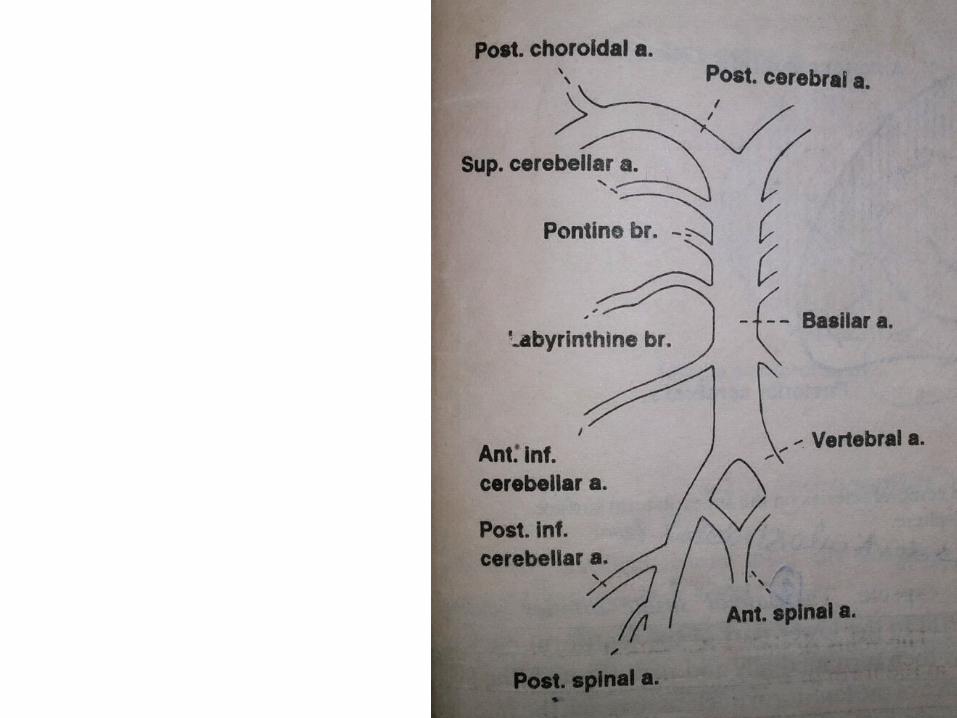
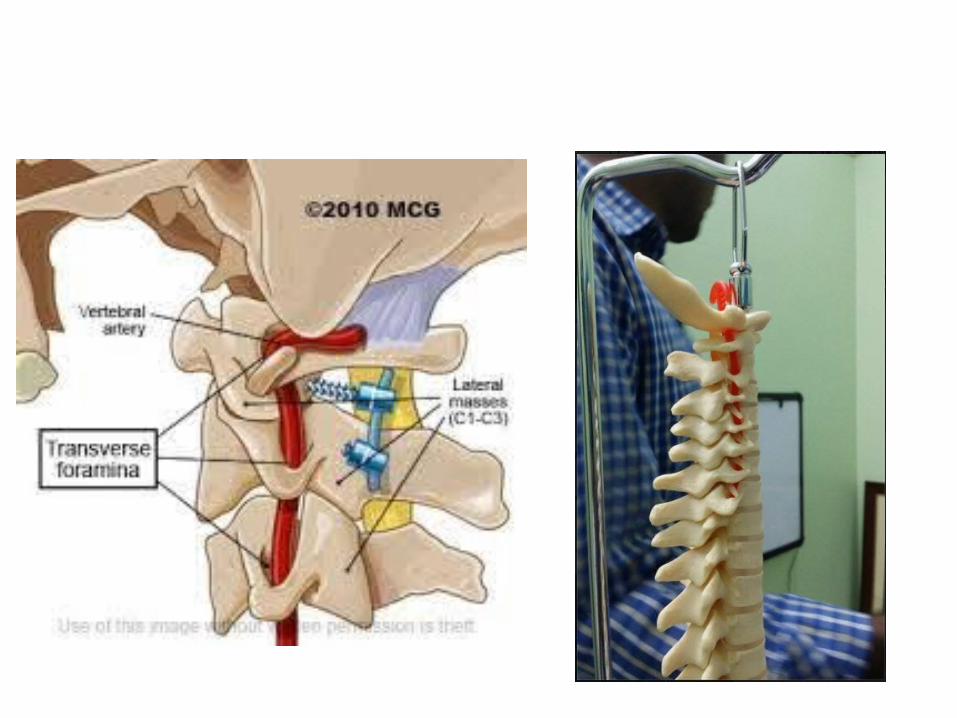
ICA Vertebro-basillar
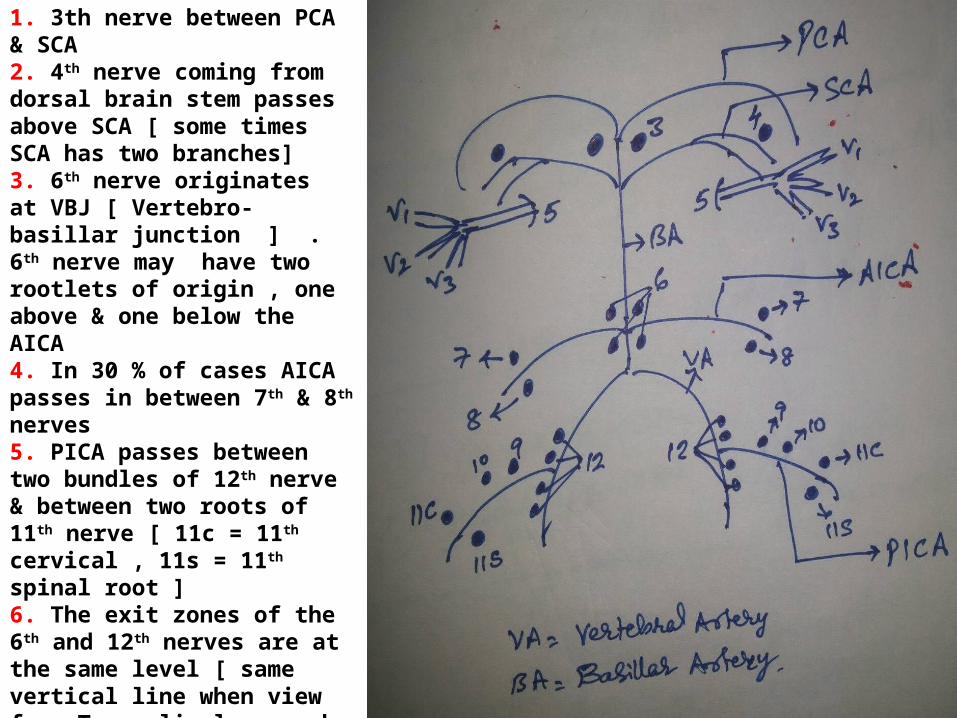
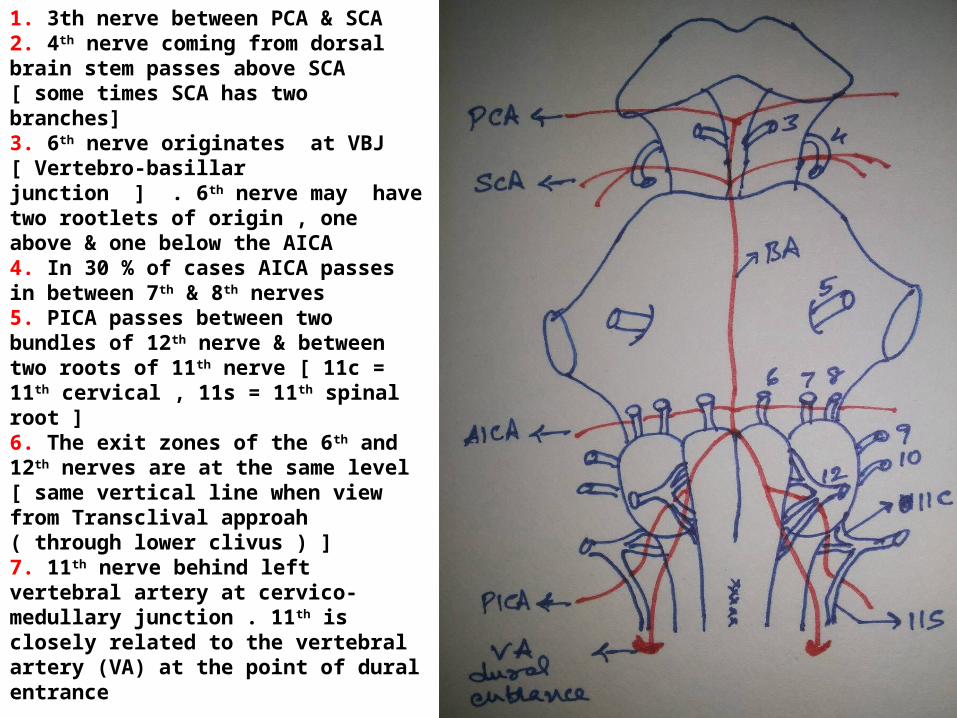
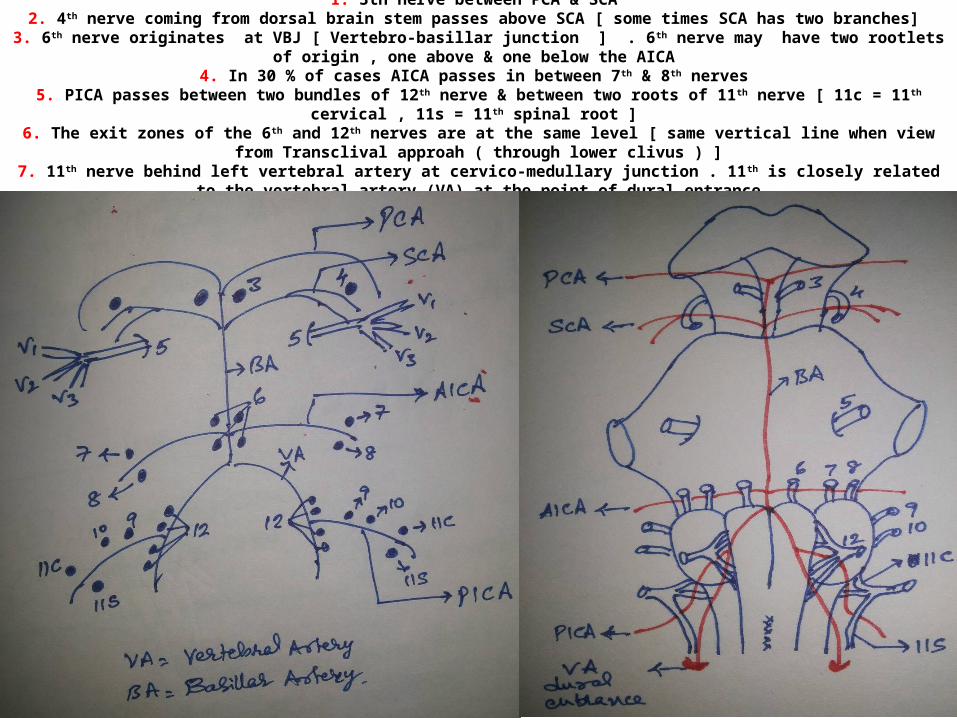
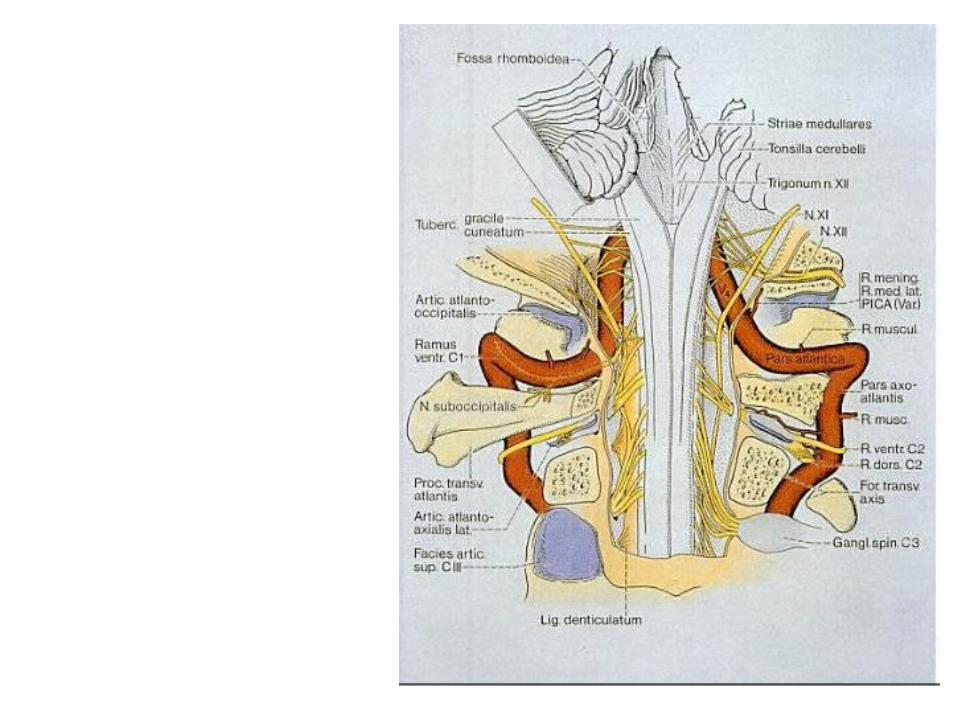
1. 3th nerve between PCA & SCA 2. 4th nerve coming from dorsal brain stem passes above SCA [ some times SCA has two branches] 3. 6th nerve originates at VBJ [ Vertebro-basillar junction ] . 6th nerve may have two rootlets of origin , one above & one below the AICA 4. In 30 % of cases AICA passes in between 7th & 8th nerves 5. PICA passes between two bundles of 12th nerve & between two roots of 11th nerve [ 11c = 11th cervical , 11s = 11th spinal root ] 6. The exit zones of the 6th and 12th nerves are at the same level [ same vertical line when view from Transclival approah ( through lower clivus ) ]7. 11th nerve behind left vertebral artery at cervico-medullary junction . 11th is closely related to the vertebral artery (VA) at the point of dural entrance
1. 3th nerve between PCA & SCA 2. 4th nerve coming from dorsal brain stem passes above SCA [ some times SCA has two branches] 3. 6th nerve originates at VBJ [ Vertebro-basillar junction ] . 6th nerve may have two rootlets of origin , one above & one below the AICA 4. In 30 % of cases AICA passes in between 7th & 8th nerves 5. PICA passes between two bundles of 12th nerve & between two roots of 11th nerve [ 11c = 11th cervical , 11s = 11th spinal root ] 6. The exit zones of the 6th and 12th nerves are at the same level [ same vertical line when view from Transclival approah ( through lower clivus ) ]7. 11th nerve behind left vertebral artery at cervico-medullary junction . 11th is closely related to the vertebral artery (VA) at the point of dural entrance
1. 3th nerve between PCA & SCA 2. 4th nerve coming from dorsal brain stem passes above SCA [ some times SCA has two branches]
3. 6th nerve originates at VBJ [ Vertebro-basillar junction ] . 6 th nerve may have two rootlets of origin , one above & one below the AICA 4. In 30 % of cases AICA passes in between 7th & 8th nerves
5. PICA passes between two bundles of 12th nerve & between two roots of 11th nerve [ 11c = 11th cervical , 11s = 11th spinal root ] 6. The exit zones of the 6th and 12th nerves are at the same level [ same vertical line when view from Transclival approah ( through lower
clivus ) ]7. 11th nerve behind left vertebral artery at cervico-medullary junction . 11th is closely related to the vertebral artery (VA) at the point of dural
entrance
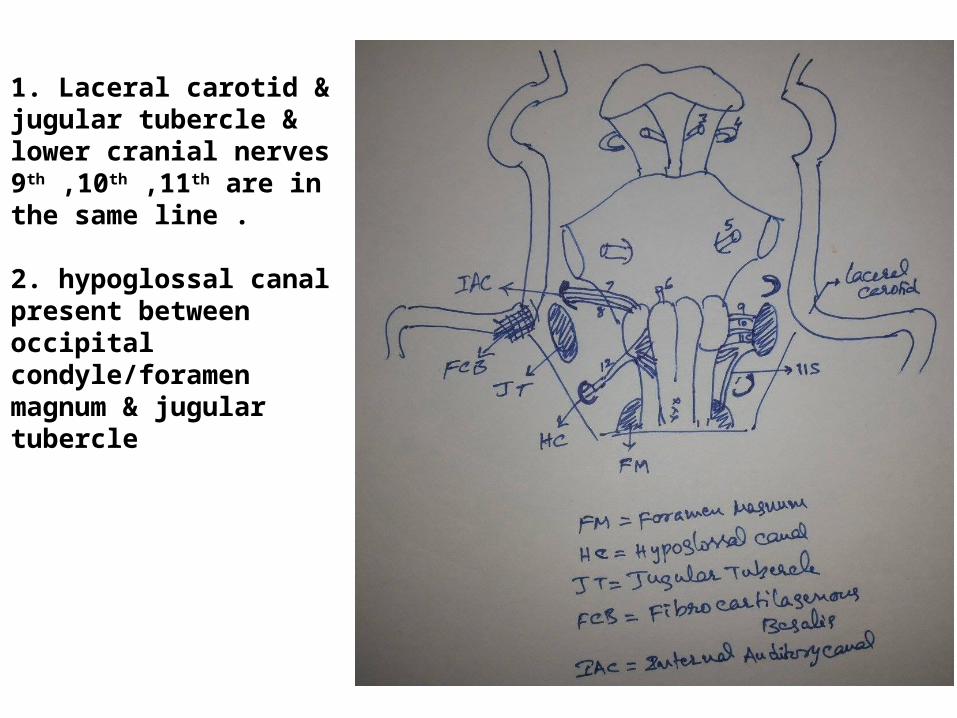
1. Laceral carotid & jugular tubercle & lower cranial nerves 9th ,10th ,11th are in the same line .
2. hypoglossal canal present between occipital condyle/foramen magnum & jugular tubercle
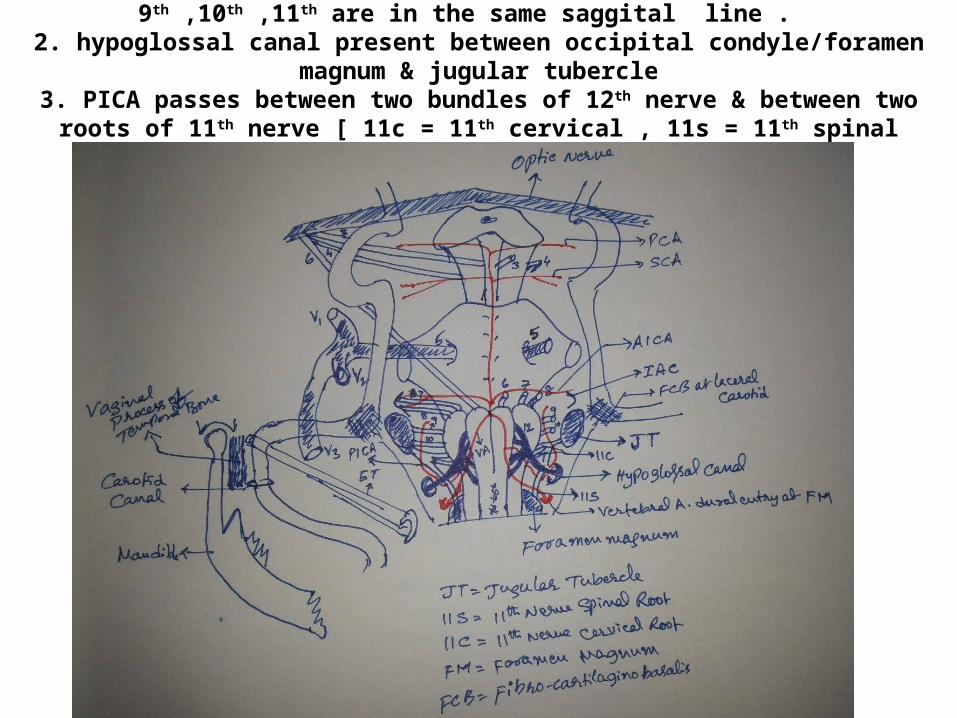
1. Laceral carotid & jugular tubercle & lower cranial nerves 9th ,10th ,11th are in the same saggital line .
2. hypoglossal canal present between occipital condyle/foramen magnum & jugular tubercle3. PICA passes between two bundles of 12th nerve & between two roots of 11th nerve [ 11c =
11th cervical , 11s = 11th spinal root ] & encirlces lower cranial nerves 9th ,10th ,11th
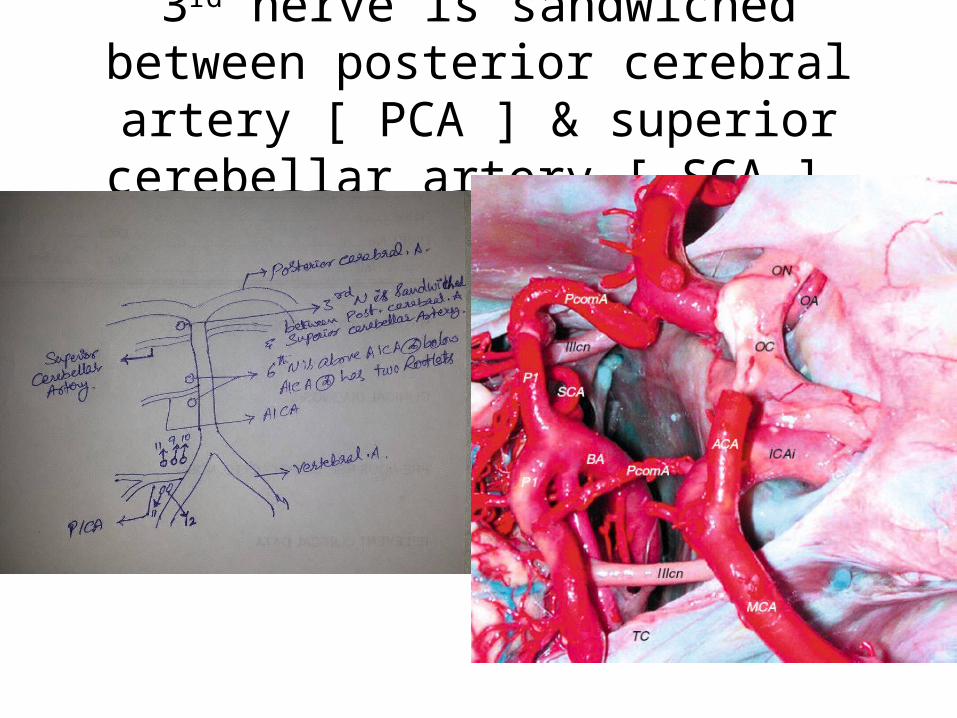
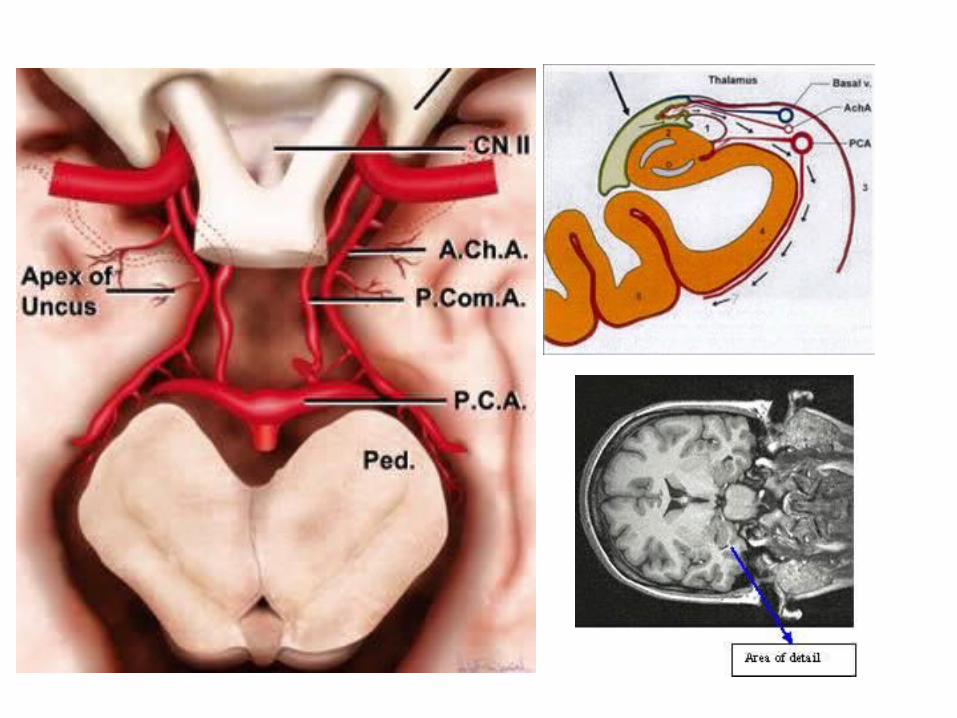
3rd nerve is sandwiched between posterior cerebral artery [ PCA ] & superior
cerebellar artery [ SCA ]
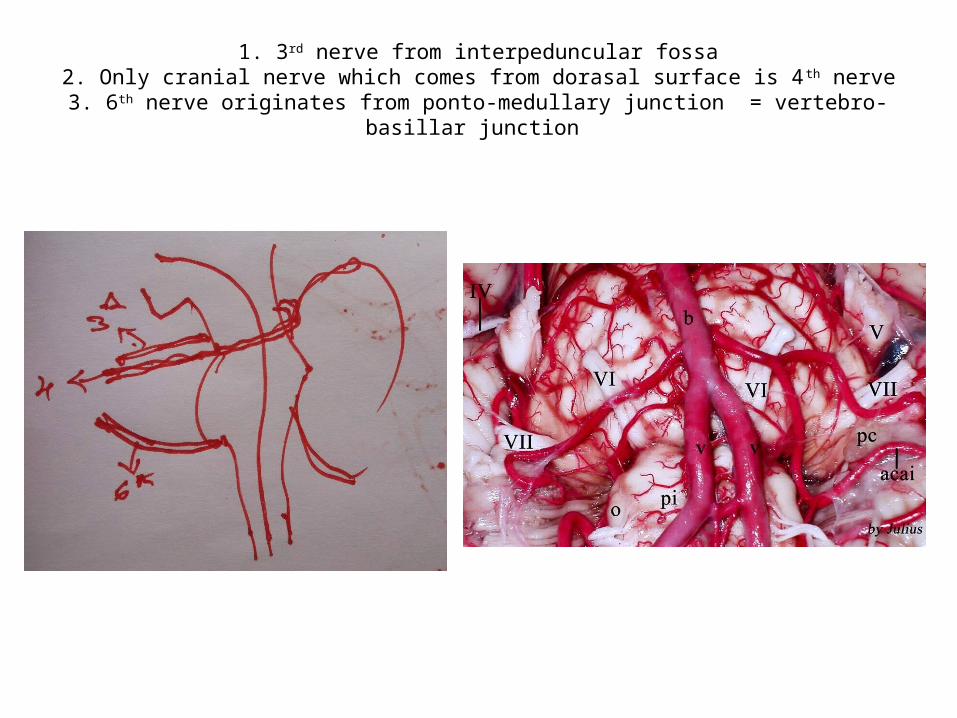
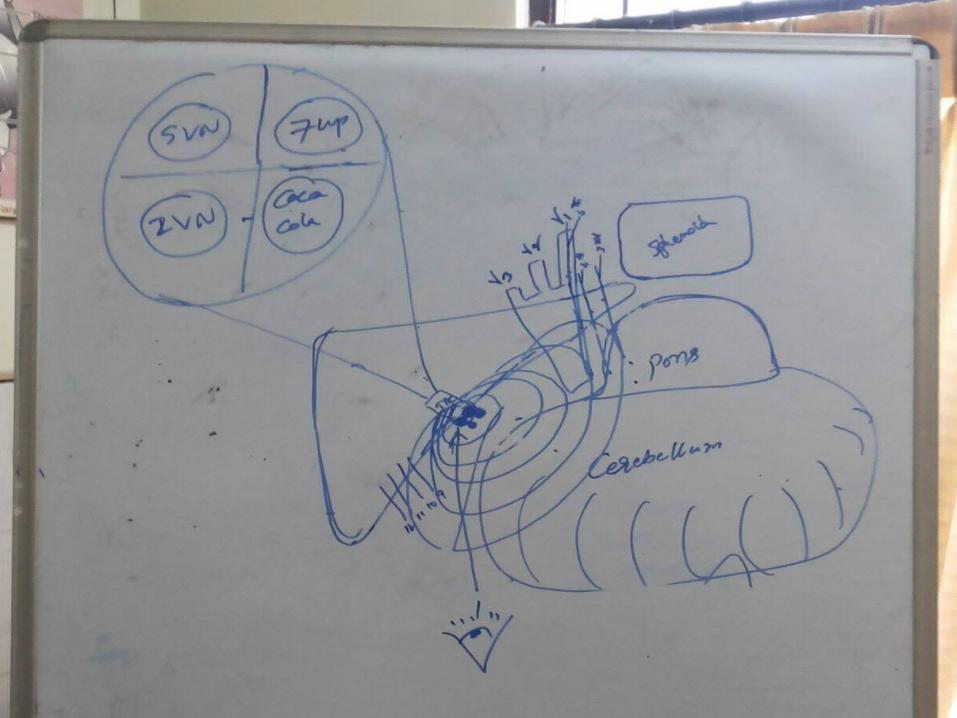
1. 3rd nerve from interpeduncular fossa2. Only cranial nerve which comes from dorasal surface is 4th nerve
3. 6th nerve originates from ponto-medullary junction = vertebro-basillar junction

Both sides 6th nerves in dorello’s canals present medial to para-clival carotids in mid-clivus & crosses Para-clival & Para-sellar carotids
juction in cavernous sinus

6th nerve (the snake nerve)
6th nerve originates above the VBJ [ vertebro-basillar junction ] – Prof.
Amin Kassam

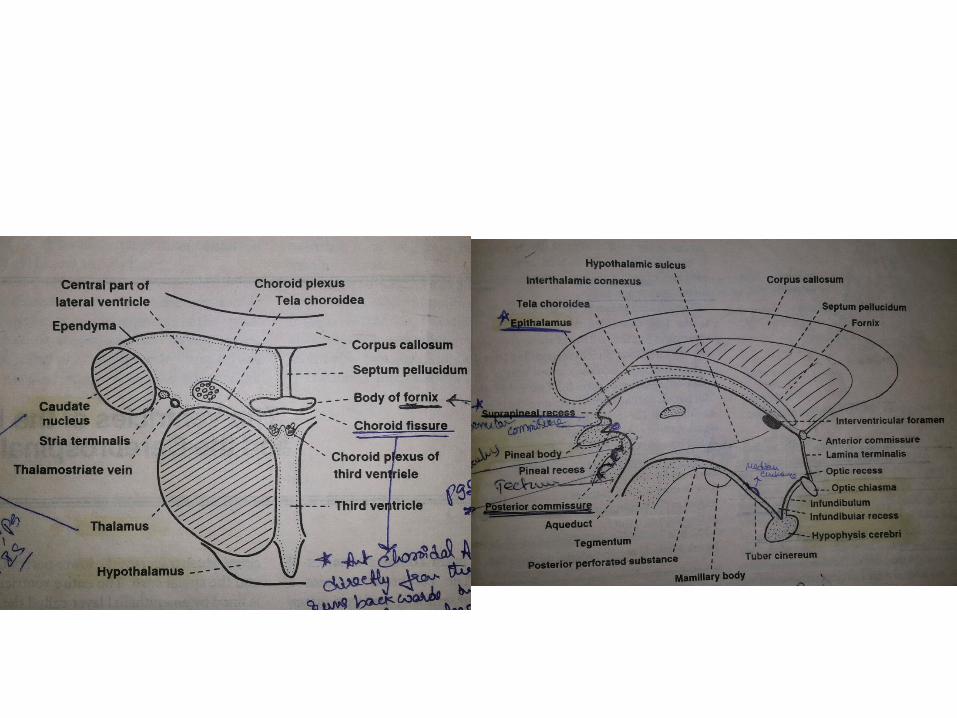
3rd ventricle

Anterior choraoid arteries goes towards optic tract
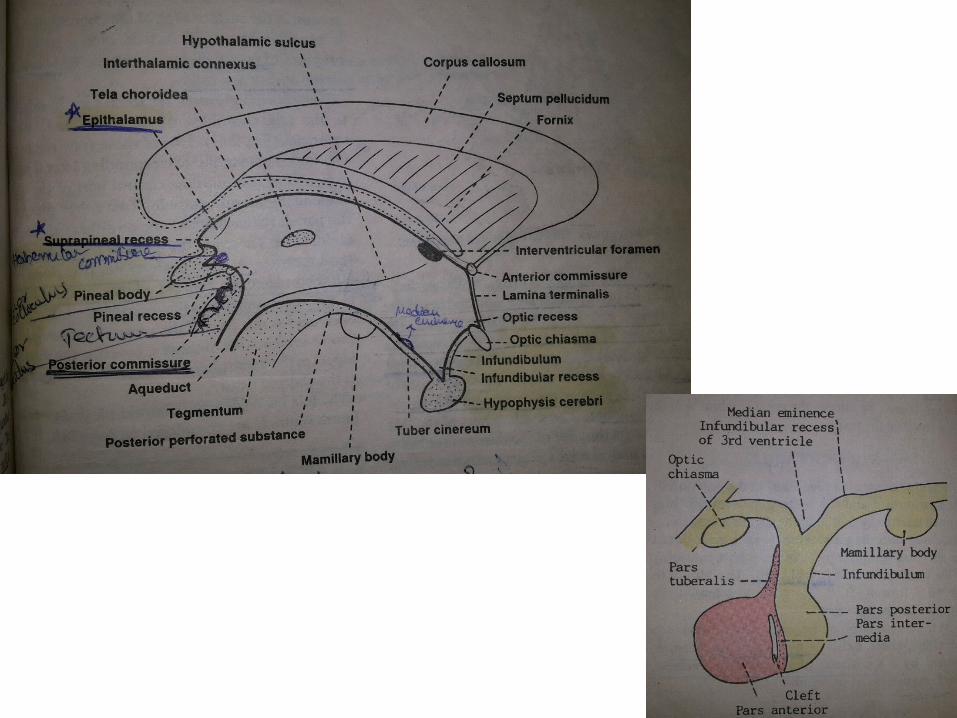
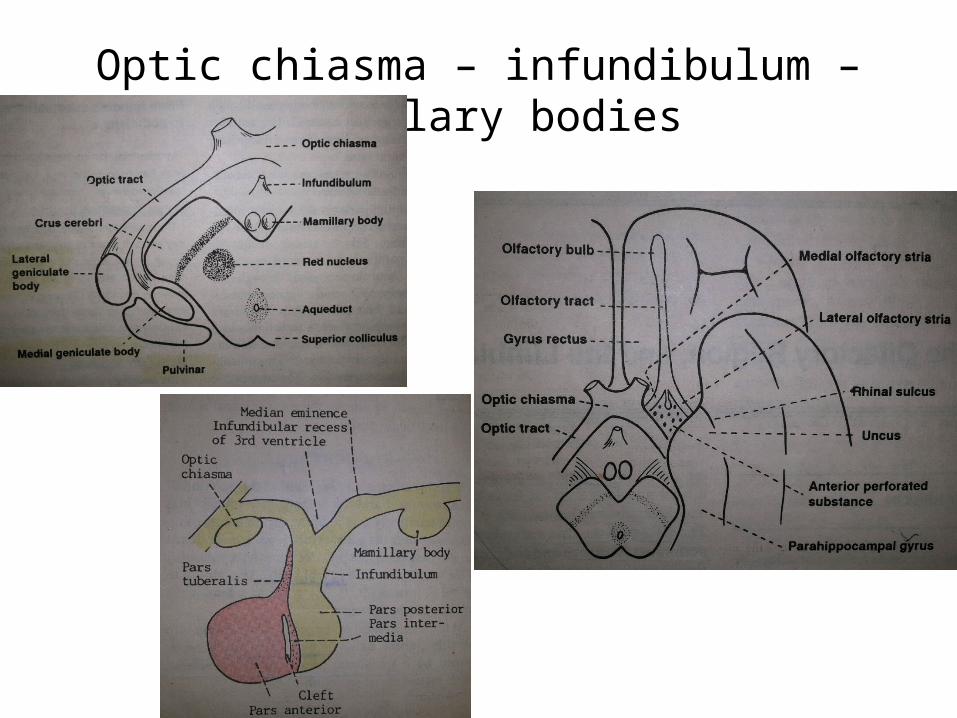
Optic chiasma – infundibulum – Mamillary bodies
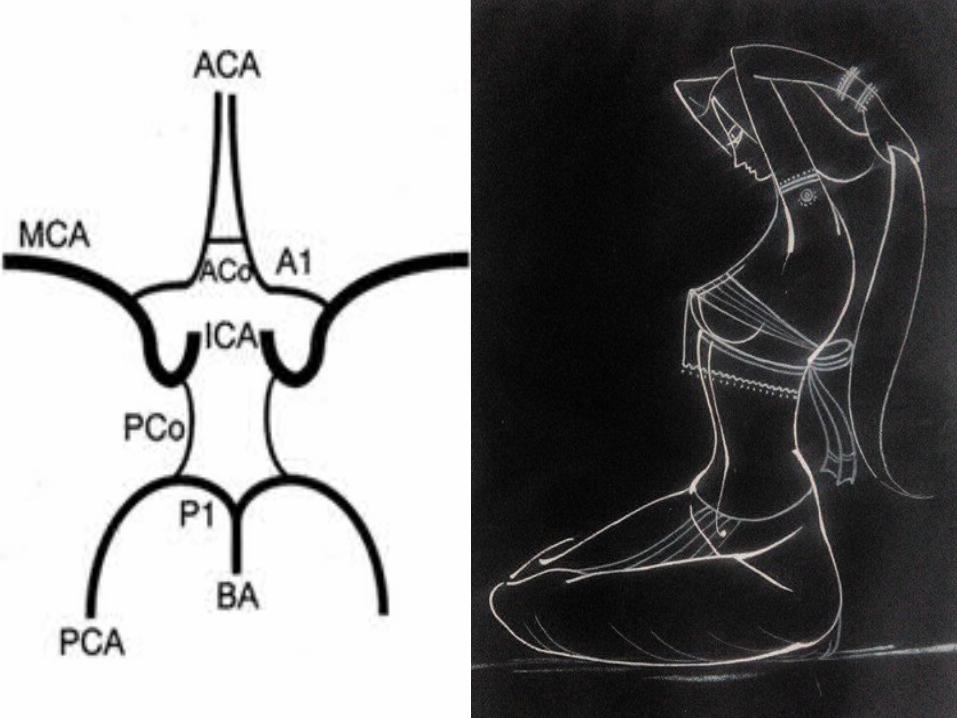
Circle of willis
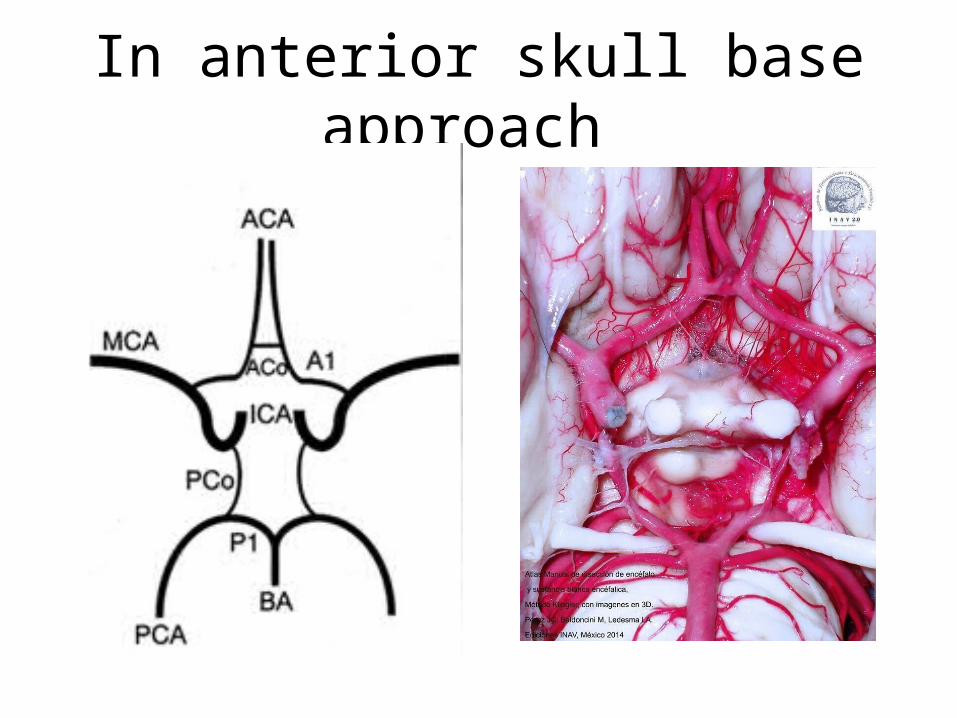
In anterior skull base approach
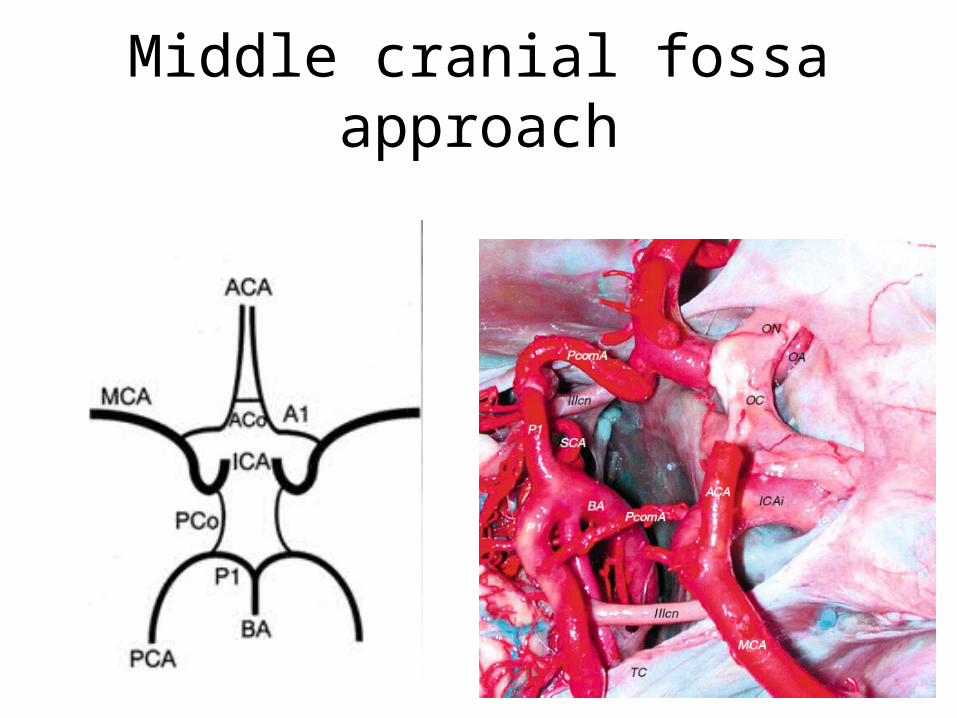
Middle cranial fossa approach
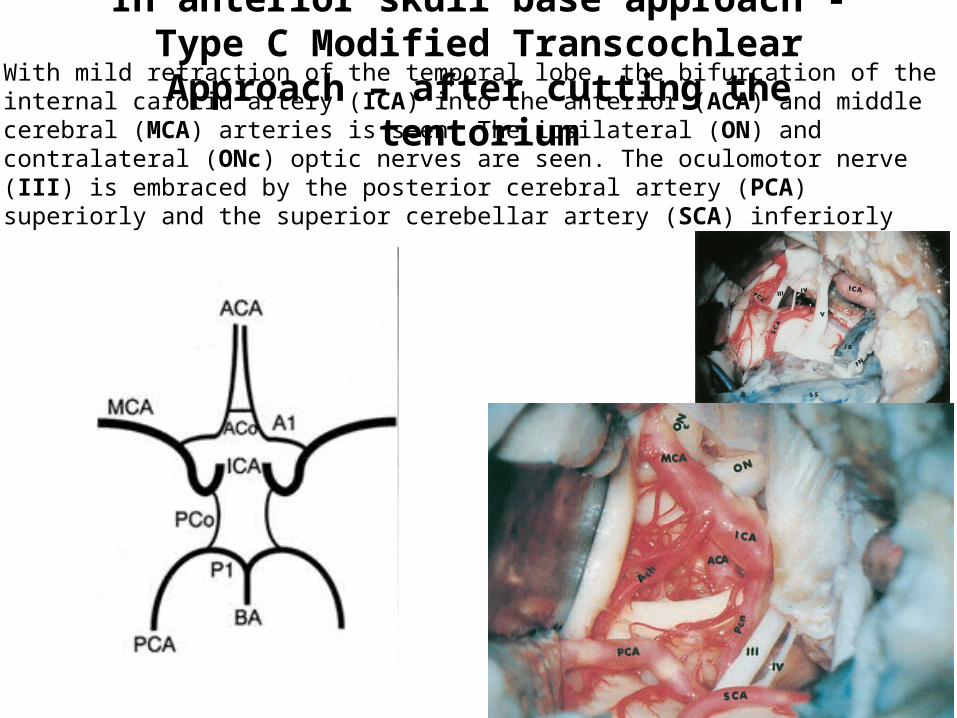
In anterior skull base approach - Type C Modified Transcochlear Approach – after cutting the tentorium
With mild retraction of the temporal lobe, the bifurcation of the internal carotid artery (ICA) into the anterior (ACA) and middle cerebral (MCA) arteries is seen. The ipsilateral (ON) and contralateral (ONc) optic nerves are seen. The oculomotor nerve (III) is embraced by the posterior cerebral artery (PCA) superiorly and the superior cerebellar artery (SCA) inferiorly
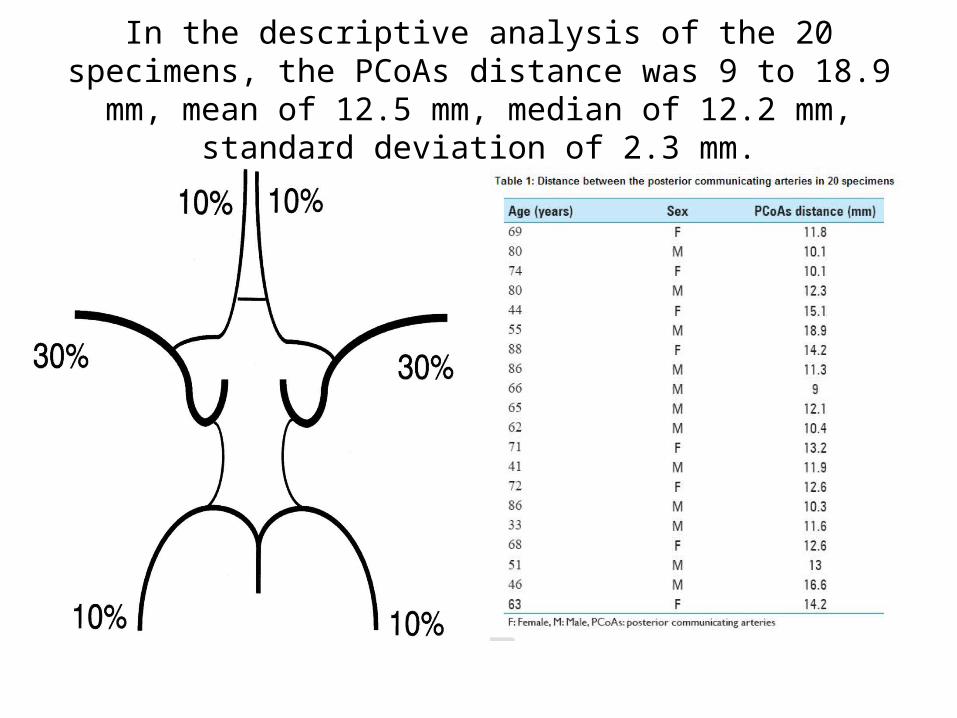
In the descriptive analysis of the 20 specimens, the PCoAs distance was 9 to 18.9 mm, mean of 12.5 mm, median of 12.2
mm, standard deviation of 2.3 mm.
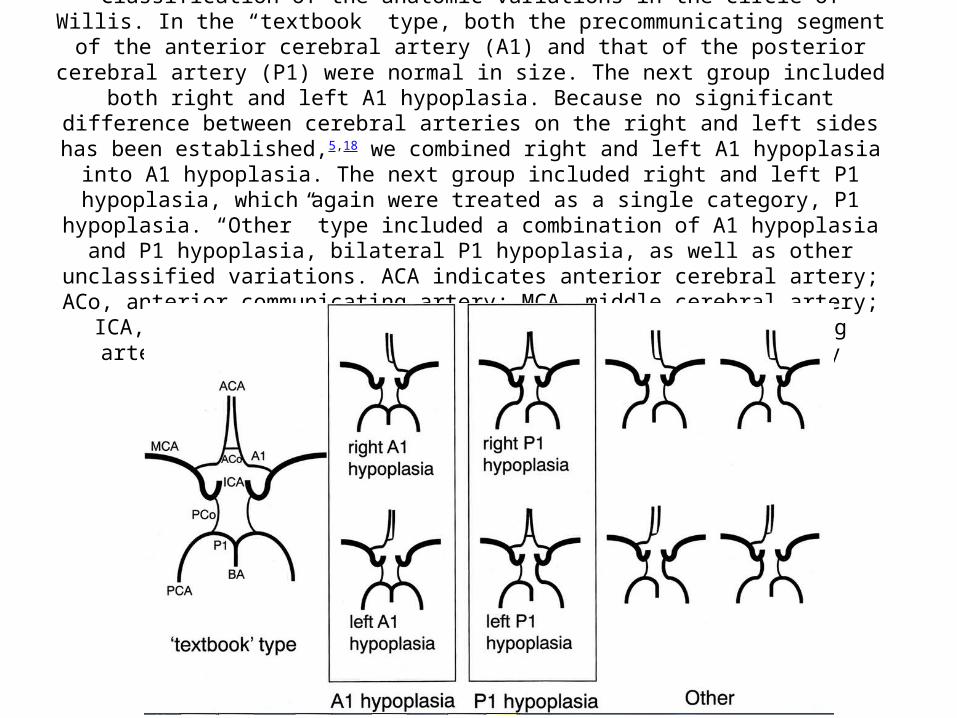
http://www.ajnr.org/content/27/8/1770/F2.expansion.htmlClassification of the anatomic variations in the circle of Willis. In the “textbook” type, both the
precommunicating segment of the anterior cerebral artery (A1) and that of the posterior cerebral artery (P1) were normal in size. The next group included both right and left A1 hypoplasia.
Because no significant difference between cerebral arteries on the right and left sides has been established,5,18 we combined right and left A1 hypoplasia into A1 hypoplasia. The next group
included right and left P1 hypoplasia, which again were treated as a single category, P1 hypoplasia. “Other” type included a combination of A1 hypoplasia and P1 hypoplasia, bilateral P1
hypoplasia, as well as other unclassified variations. ACA indicates anterior cerebral artery; ACo, anterior communicating artery; MCA, middle cerebral artery; ICA, internal cerebral artery; PCo,
posterior communicating artery; PCA, posterior cerebral artery; BA, basilar artery
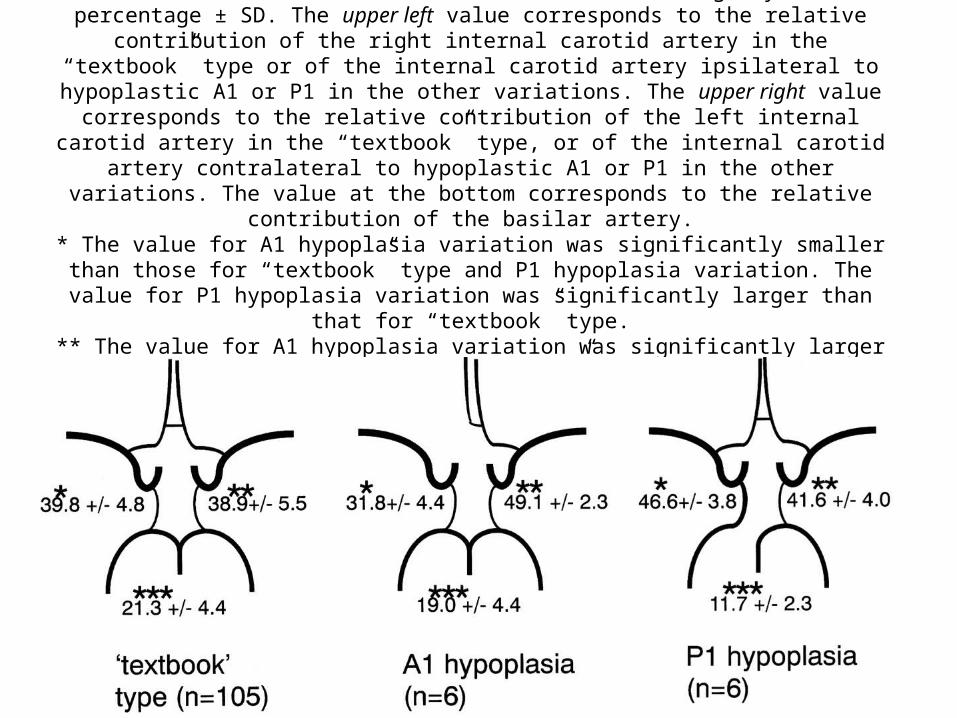
http://www.ajnr.org/content/27/8/1770/F3.expansion.htmlRelative contribution of proximal arteries to total volume flow in variations in the circle of Willis.
Values signify mean percentage ± SD. The upper left value corresponds to the relative contribution of the right internal carotid artery in the “textbook” type or of the internal carotid
artery ipsilateral to hypoplastic A1 or P1 in the other variations. The upper right value corresponds to the relative contribution of the left internal carotid artery in the “textbook” type, or of the internal carotid artery contralateral to hypoplastic A1 or P1 in the other variations. The
value at the bottom corresponds to the relative contribution of the basilar artery.* The value for A1 hypoplasia variation was significantly smaller than those for “textbook” type and P1 hypoplasia variation. The value for P1 hypoplasia variation was significantly larger than
that for “textbook” type.** The value for A1 hypoplasia variation was significantly larger than that for “textbook” type.
*** The value for P1 hypoplasia variation was significantly smaller than that for “textbook” type.
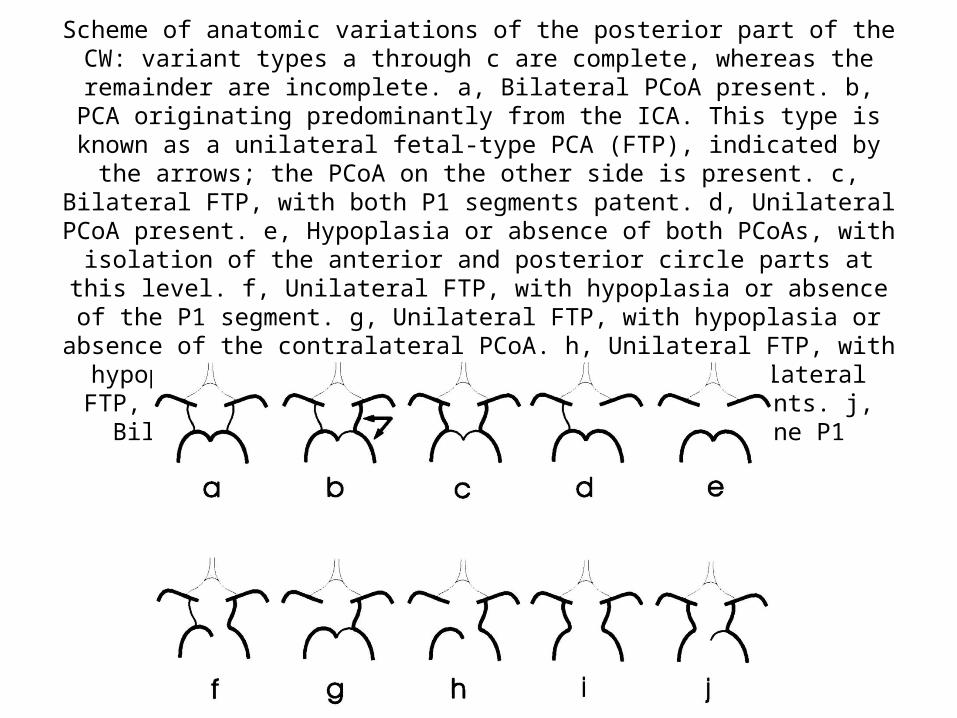
http://stroke.ahajournals.org/content/30/12/2671/F2.expansion.htmlScheme of anatomic variations of the posterior part of the CW: variant types a through
c are complete, whereas the remainder are incomplete. a, Bilateral PCoA present. b, PCA originating predominantly from the ICA. This type is known as a unilateral fetal-
type PCA (FTP), indicated by the arrows; the PCoA on the other side is present. c, Bilateral FTP, with both P1 segments patent. d, Unilateral PCoA present. e, Hypoplasia or absence of both PCoAs, with isolation of the anterior and posterior circle parts at
this level. f, Unilateral FTP, with hypoplasia or absence of the P1 segment. g, Unilateral FTP, with hypoplasia or absence of the contralateral PCoA. h, Unilateral FTP, with
hypoplasia or absence of the P1 and PCoA. i, Bilateral FTP, with hypoplasia or absence of both P1 segments. j, Bilateral FTP, with hypoplasia or absence of one P1 segment.
Open skull base approaches
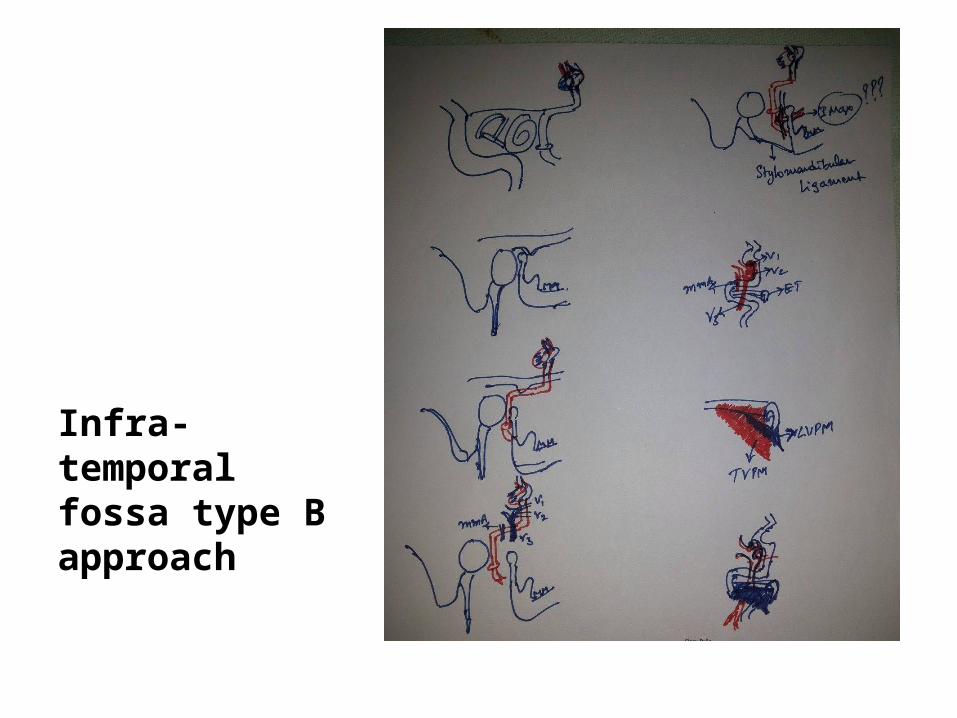
Infra-temporal fossa type B approach

For Other powerpoint presentatioins of “ Skull base 360° ”
I will update continuosly with date tag at the end as I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with Facebook account for downloading.