Lindsey E. Eberman, MS, ATC, LAT Chapter 10 Thoracic and Lumbar Spine.
38
Lindsey E. Eberman, MS, ATC, LAT Chapter 10 Thoracic and Lumbar Spine
-
Upload
mavis-kelley -
Category
Documents
-
view
215 -
download
0
Transcript of Lindsey E. Eberman, MS, ATC, LAT Chapter 10 Thoracic and Lumbar Spine.

Lindsey E. Eberman, MS, ATC, LAT
Chapter 10Thoracic and Lumbar Spine
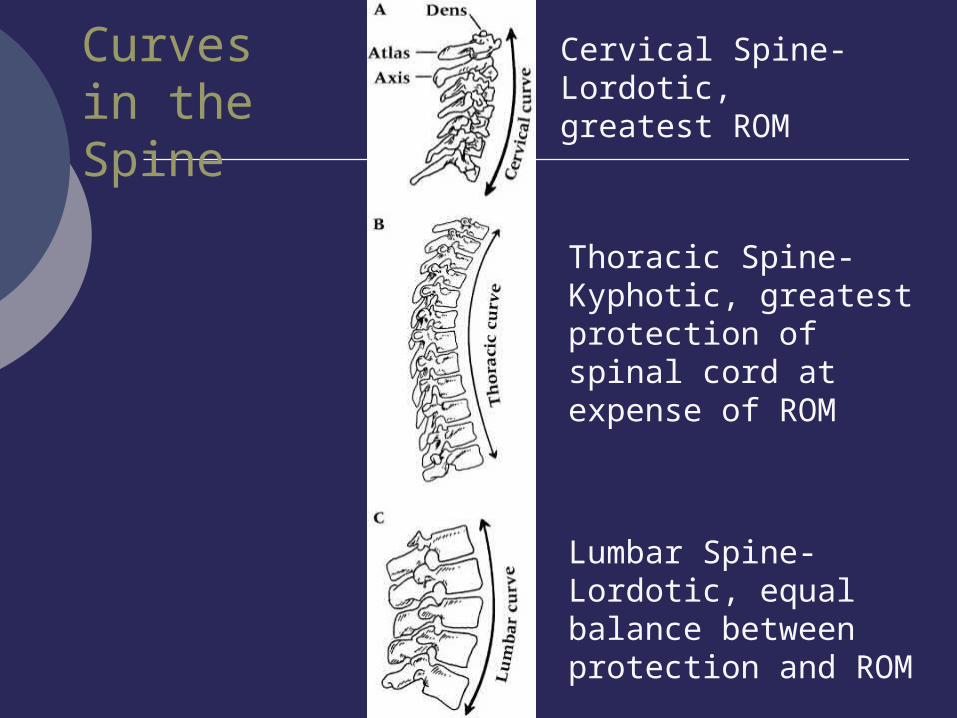
Curves in the Spine
Cervical Spine- Lordotic, greatest ROM
Thoracic Spine- Kyphotic, greatest protection of spinal cord at expense of ROM
Lumbar Spine- Lordotic, equal balance between protection and ROM

Characteristics of Vertebrae

Joints
Costovertebral Joint Rib and thoracic vertebrae
Zygopopheseal Joint Superior and inferior articulating facets
Intervertebral Joint Vertebral bodies




Ligamentous Support

Ligament Name Description
Anterior Longitudinal Ligament (ALL) A primary spine stabilizer
About one-inch wide, the ALL runs the entire length of the spine from the base of the skull to the sacrum. It connects the front (anterior) of the vertebral body to the front of the annulus fibrosis.
Posterior Longitudinal Ligament (PLL) A primary spine stabilizer
About one-inch wide, the PLL runs the entire length of the spine from the base of the skull to sacrum. It connects the back (posterior) of the vertebral body to the back of the annulus fibrosis.
Supraspinous Ligament This ligament attaches the tip of each spinous process to the other.
Interspinous Ligament This thin ligament attaches to another ligament, called the ligamentum flavum that runs deep into the spinal column.
Ligamentum Flavum The strongest ligament
This yellow ligament is the strongest one. It runs from the base of the skull to the pelvis, in front of and behind the lamina, and protects the spinal cord and nerves. The ligamentum flavum also surrounds the facet joint capsules.
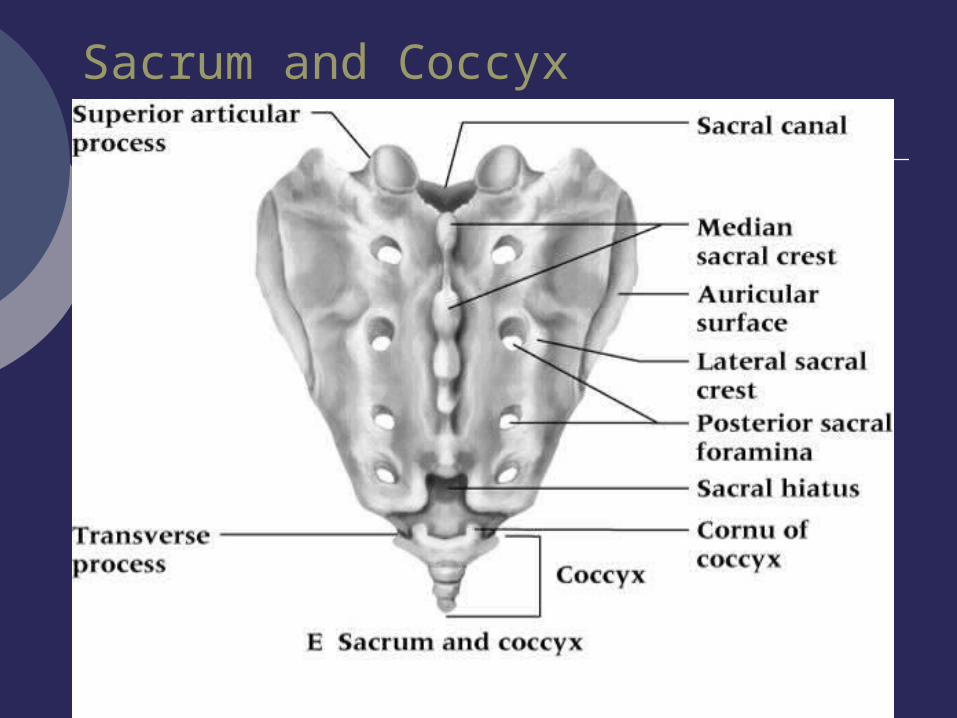
Sacrum and Coccyx

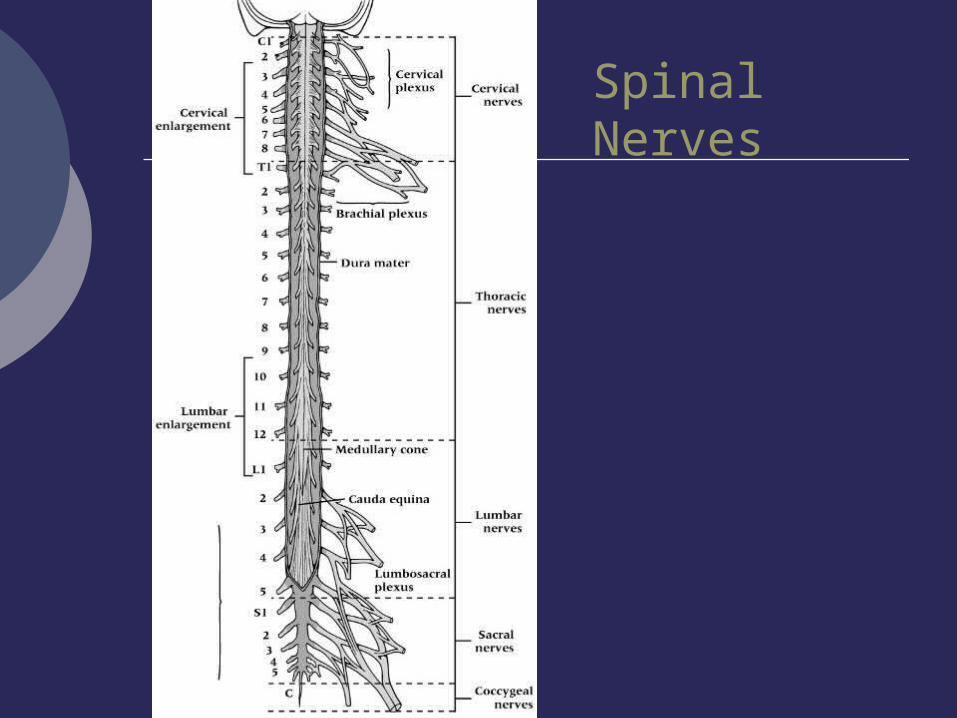
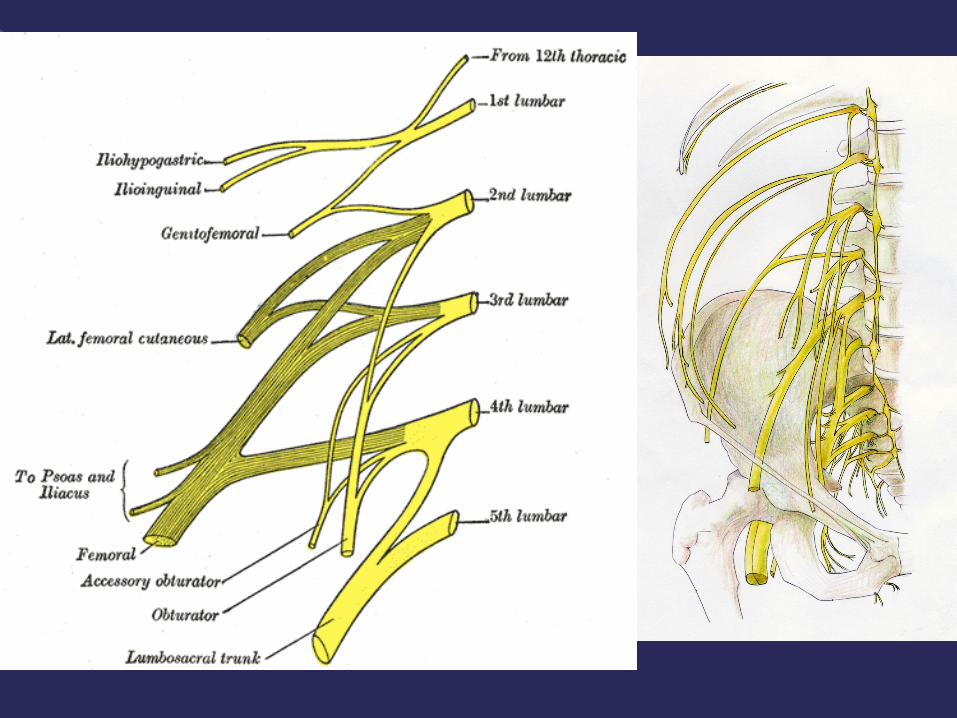
Spinal Nerves


Extrinsic Muscles


Muscle Action
Iliocostalis Lumborum B: ExtensionU: Same side lateral bending
Iliocostalis Thoracis B: ExtensionU: Same side lateral bending
Longissimus Thoracis B: ExtensionU: lateral bending
Spinalis Thoracis B: ExtensionU: Same side lateral bending
Semispinalis Thoracis B: Extension of thoracic and cervical spineU: Opposite side rotation
Multifidus B: StabilizationU: Opposite side rotation
Rotatores B: Extension, StabilizationU: Rotation
Intrinsic Muscles of the Spine

History
Key Questions ADLs Time of day Postural positions
Location of Pain Pain radiating into extremities, peripheral
parasthesia (numbness) Impingement- pressure on a nerve root exiting the
intervertebral foramen Dural irritation- proximal to site of pain
Pain around PSIS, radiating pain into hip/groin SI joint pathology
Sciatic nerve dysfunction/irritation Piriformis spasm

History
Onset of Pain Acute
Patients may be capable of describing a singular incident
Chronic Accumulation of repetitive stress,
macrotrauma Insidious
Being a disease that progresses with few or no symptoms to indicate its gravity

History
MOI Direct blow
Contusions Hyperextension sports
Gymnastics, Offensive line (FB), Cheerleading, Diving, Crew (Rowing), Weightlifting
Compressive forces Shear forces
History
Consistency of pain Constant
No change in pain level with change in posture Chemical- Dural sheath irritation
Intermittent Symptoms inc and dec with repositioning
Mechanical- Compression/stretching of nerve root
Bowel/Bladder signs Incontinence or urinary retention
Lower nerve root lesion (Cauda equina syndrome)
Spinal cord injury

History
History of spinal injury Structural degeneration Predispositions
Changes Activity
Level Intensity Duration
Surfaces Footwear
Training shoes Competition shoes
Sleeping location/habits
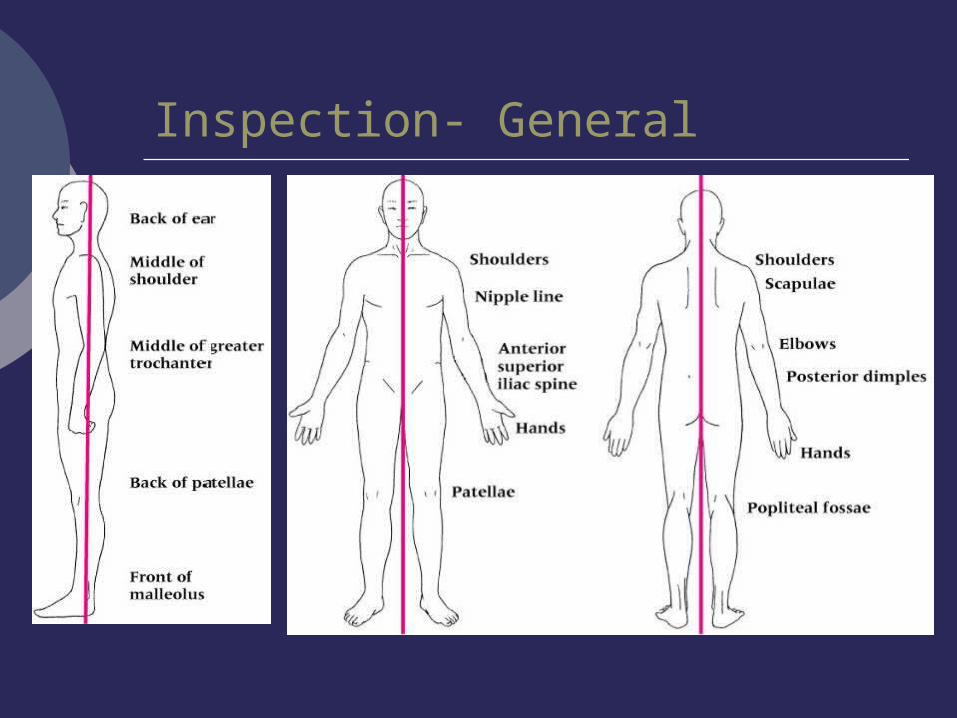
Inspection- General
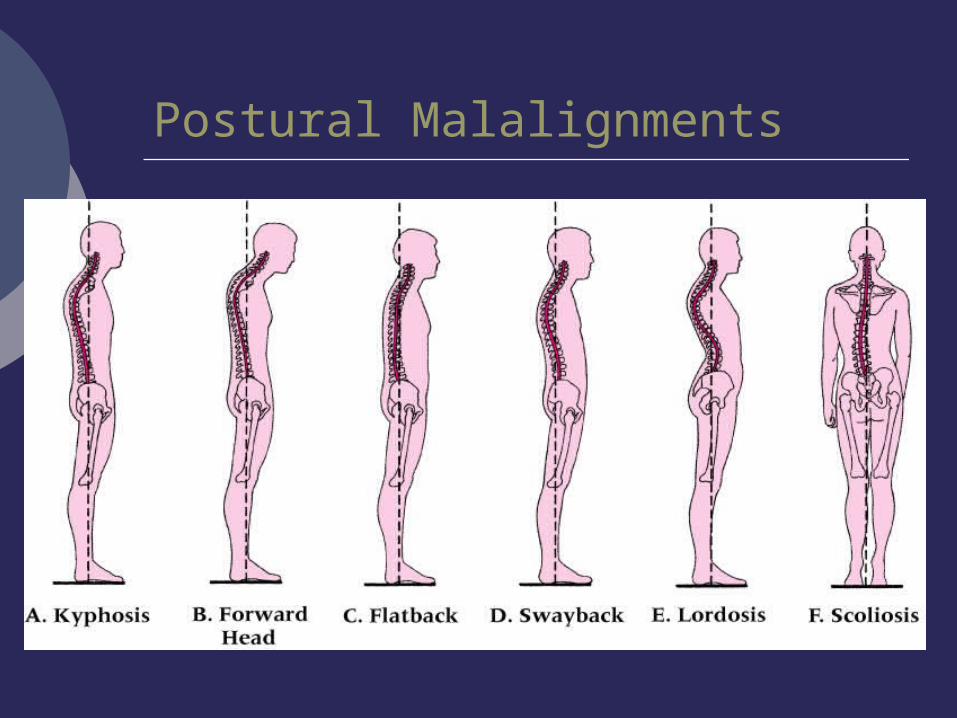
Postural Malalignments

Frontal Curvature
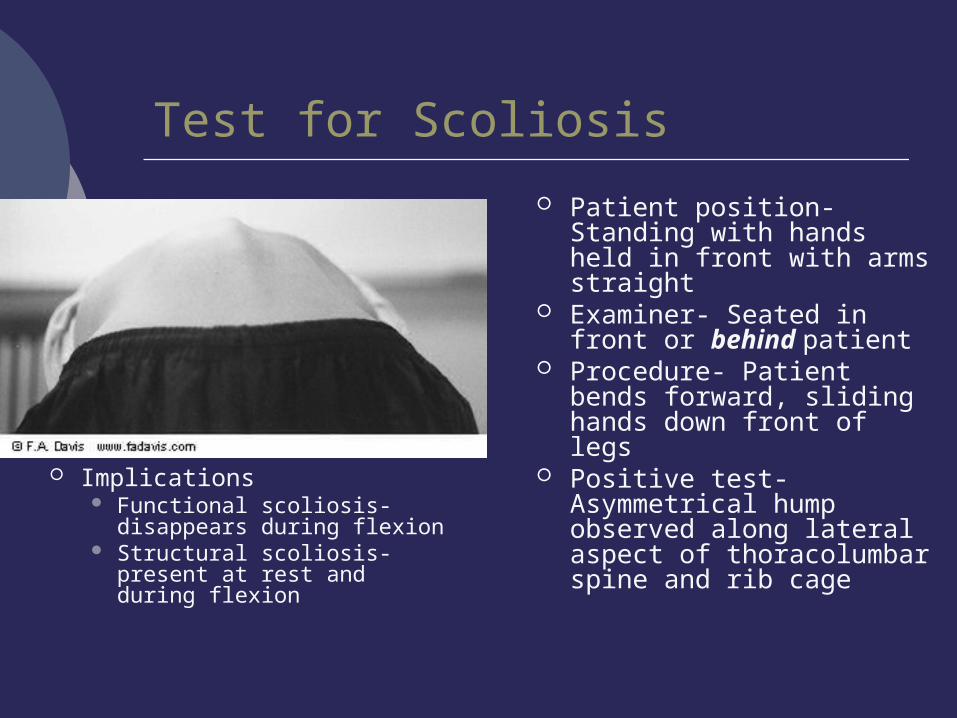
Test for Scoliosis
Patient position- Standing with hands held in front with arms straight
Examiner- Seated in front or behind patient
Procedure- Patient bends forward, sliding hands down front of legs
Positive test- Asymmetrical hump observed along lateral aspect of thoracolumbar spine and rib cage
Implications Functional scoliosis-
disappears during flexion Structural scoliosis-
present at rest and during flexion
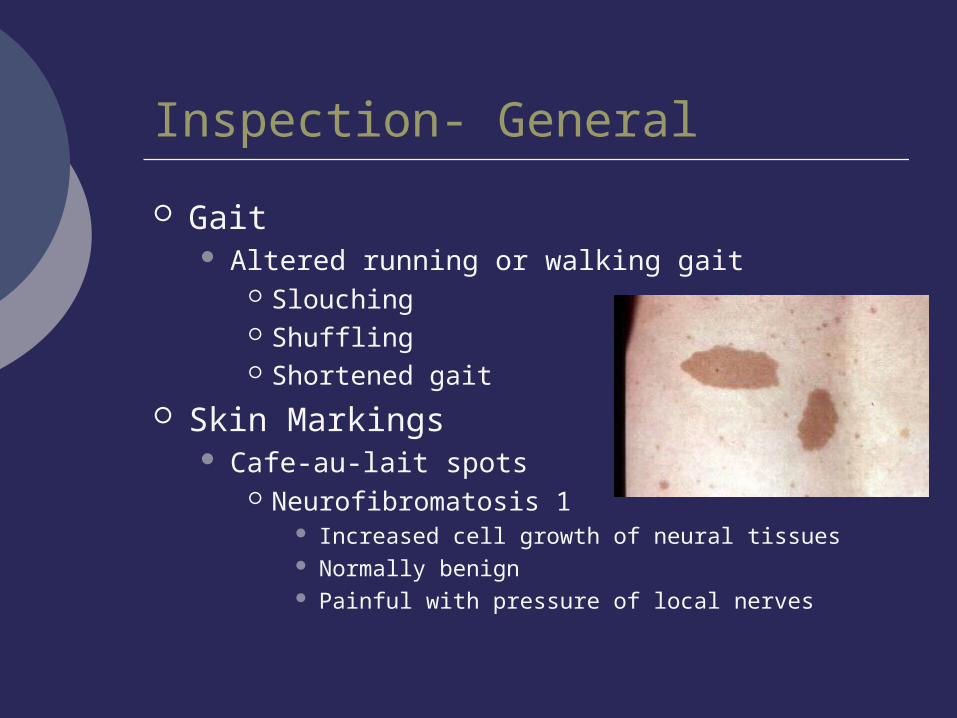
Inspection- General
Gait Altered running or walking gait
Slouching Shuffling Shortened gait
Skin Markings Cafe-au-lait spots
Neurofibromatosis 1 Increased cell growth of neural tissues Normally benign Painful with pressure of local nerves

Inspection- Thoracic Spine
Breathing patterns Irregular, shallow breathing
Injury to T vertebrae, pressure on T nerve roots, trauma to costal cartilage or ribs
Bilateral comparison of skin folds Asymmetry, unevenness
Bilateral muscle imbalance, kyphosis, scoliosis Shape of chest
Vertebral rotation causing rib prominence posteriorly
“Rib hump”

Inspection- Lumbar Spine
General movement and posture Improper standing or sitting Improper lifting mechanics
Lordotic curvature Reduced curve
Acute pain, muscle spasm, hamstrings tightness Increased curve
Hip flexor tightness, abdominal muscle weakness
Standing posture Lateral shift in trunk or pelvis
Impingement

Inspection- Lumbar Spine
Erector muscle tone Unilateral hypertrophy or atrophy
Weak muscles Poor, abnormal posture
Faun’s beard Tuft or hair in lumbar or sacral spine
Spina bifida occulta
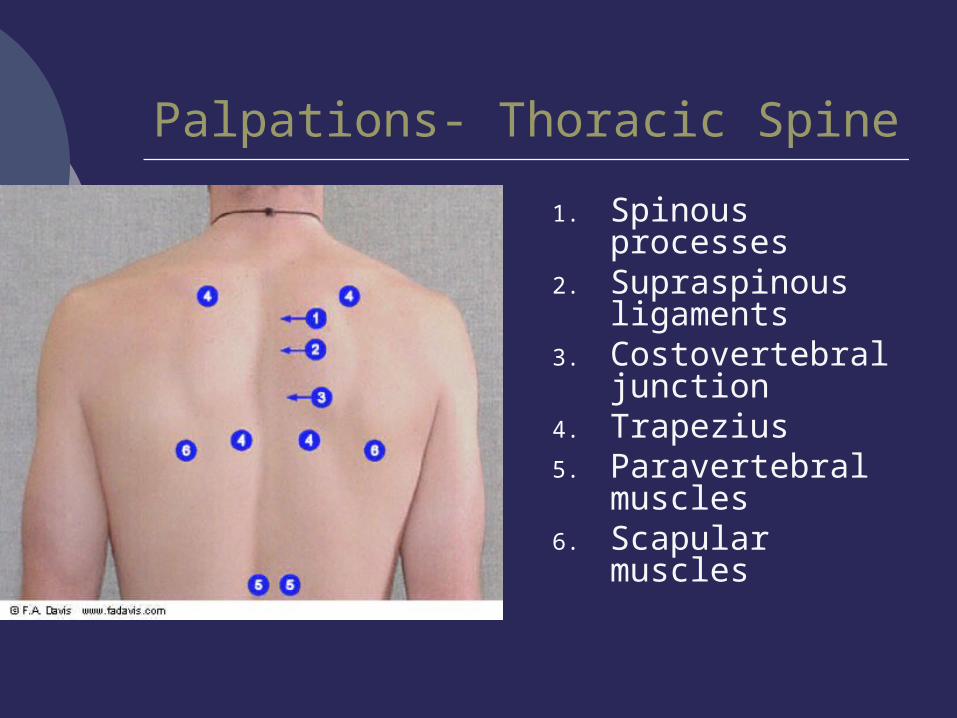
Palpations- Thoracic Spine
1. Spinous processes
2. Supraspinous ligaments
3. Costovertebral junction
4. Trapezius5. Paravertebral
muscles6. Scapular
muscles

Palpations- Lumbar Spine
1. Spinous processes
2. Step-off deformity
3. Paravertebral muscles
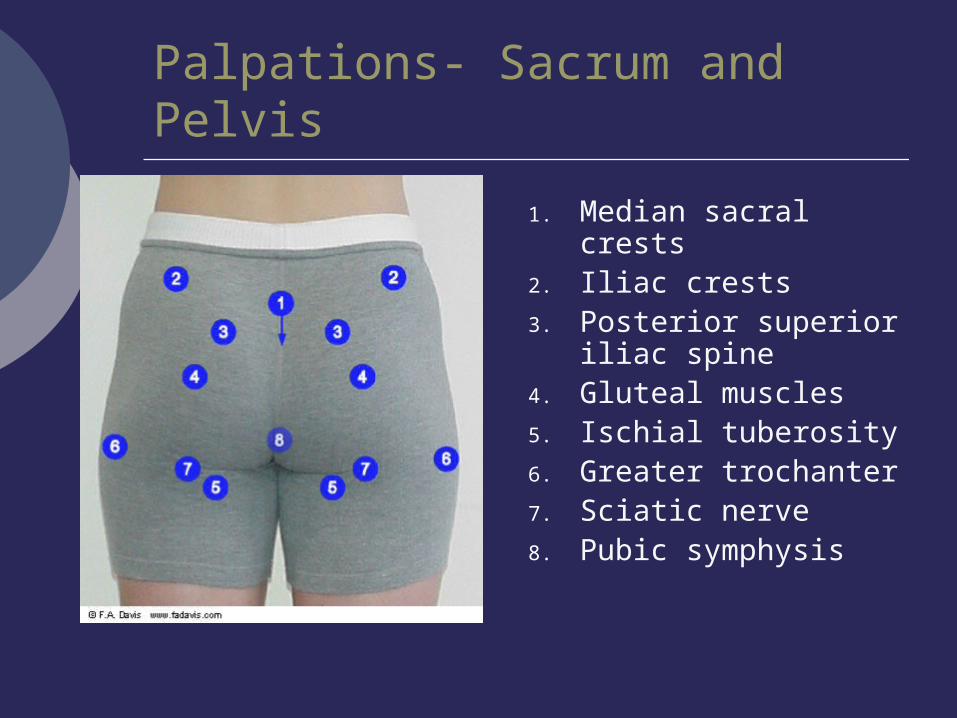
Palpations- Sacrum and Pelvis
1. Median sacral crests
2. Iliac crests3. Posterior superior
iliac spine4. Gluteal muscles5. Ischial tuberosity6. Greater trochanter7. Sciatic nerve8. Pubic symphysis
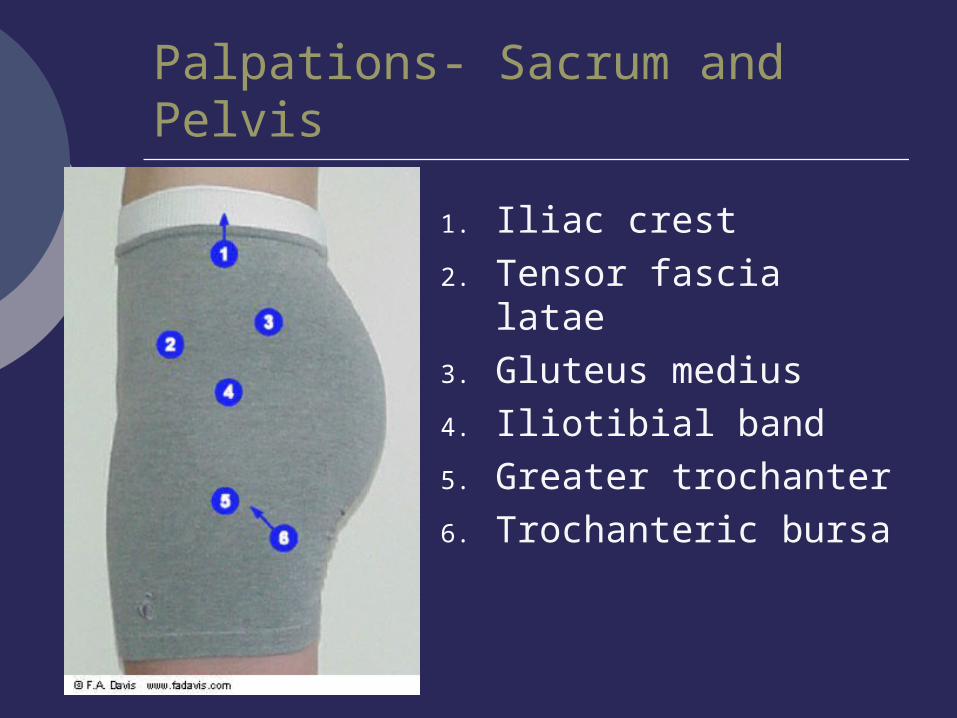
Palpations- Sacrum and Pelvis
1. Iliac crest2. Tensor fascia latae3. Gluteus medius4. Iliotibial band5. Greater trochanter6. Trochanteric bursa
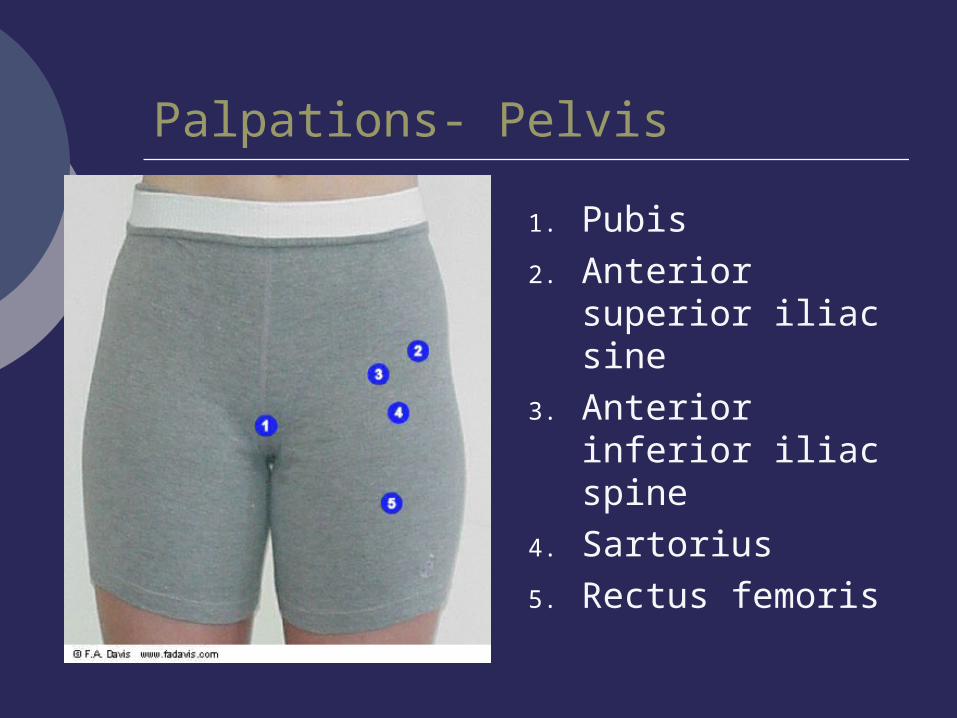
Palpations- Pelvis
1. Pubis2. Anterior superior
iliac sine3. Anterior inferior
iliac spine4. Sartorius5. Rectus femoris

ROM- Goniometric Measurements
Patient position- standing with knees extended, spine in neutral position
Procedure Initial- measure
distance between C7 and S1
Motion- trunk fully flexed or extended
Final- measure distance between C7 and S1

ROM- Goniometric Measurements
Patient position- standing with knees extended and spine in neutral position
Procedure Fulcrum- Aligned over S1
SP Stationary arm- Aligned
over median sacral crest Movement arm- Aligned
with C7 SP
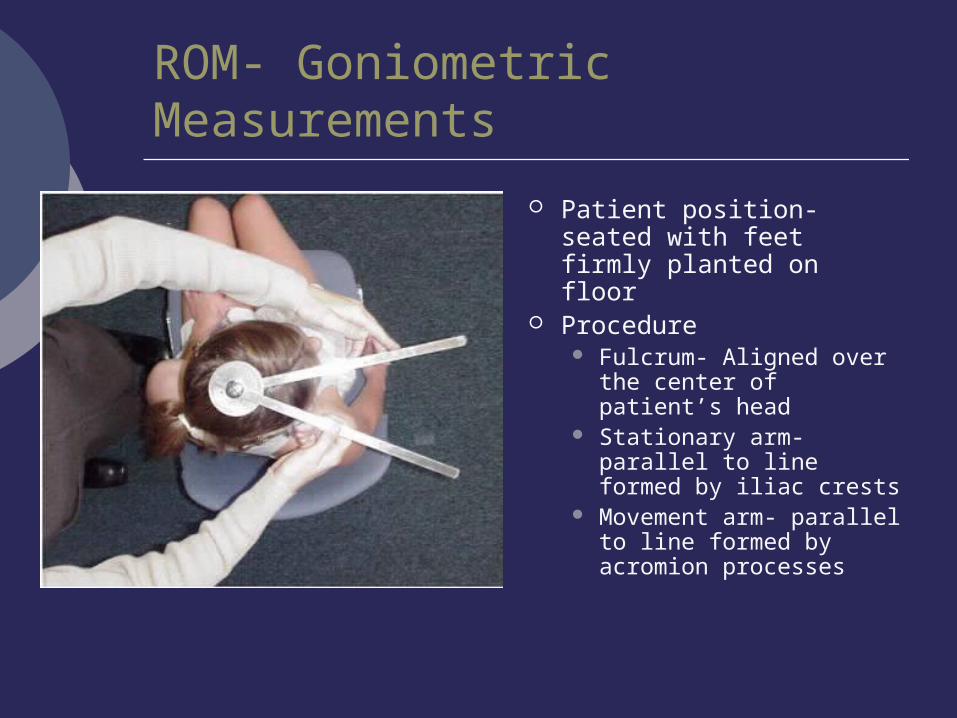
ROM- Goniometric Measurements
Patient position- seated with feet firmly planted on floor
Procedure Fulcrum- Aligned over
the center of patient’s head
Stationary arm- parallel to line formed by iliac crests
Movement arm- parallel to line formed by acromion processes