Limb Arterial Injuries Associated with Limb Fractures ... · of 1.5 to 2 years, the upper and lower...
7
Eur J Vasc Endovasc Surg 9, 64-70 (1995) Limb Arterial Injuries Associated with Limb Fractures: Clinical Presentation, Assessment and Management Asterios N. Katsamouris 1, Kostas Steriopoulos 2, Panos Katonis 2, Kostas Christou a, John Drositis 1, Tatiana Lefaki 4, Sophocles Vassilakis 1 and Emmanuel Dretakis 2 IVascular Surgical Unit, 2Department of Orthopedics and Traumatology, and 4Department of Anaesthesia, University of Crete Medical School, Herakleion University Hospital, Herakleion Crete, Greece, and 3Department of Surgery B2, Hippocrates General Hospital, Thessaloniki, Greece Objectives: Review of limb arterial injuries associated with limb fractures. Design: Retrospective study. Setting: University Hospital. Materials and Methods: The clinical presentation, assessment and management of 25 patients with upper (seven) and lower (18) limb arterial injuries associated with limb bone fractures has been retrospectively reviewed. Main Results: Five patients presented with life threatening injuries and classic signs of acute limb ischaemia, 15 patients had an obvious limb arterial injury, and 5 presented with a suspected limb arterial injury. The site of arterial damage was: superficial femoral (4); popliteal (11); tibioperoneal trunk (3); anterior tibial (4); posterior tibial (3); peroneal (2); axillary (1); brachial (5); radial (4); and ulnar artery (4). The types of arterial repair were: autogenous vein interposition or bypass grafting (17); P.T.F.E. (2); end-to-end anastomosis (14); and Iigation (8). The popliteal vein was injured in six cases, repaired in four and Iigated in two; the superficial femoral vein was injured in four cases, repaired in three and ligated in one; and the axillary vein was injured in one case and was ligated. Primary nerve repair was employed in six out of seven injured nerves. Skeletal fixation preceded vascular repair in 21 patients and in four a Javid shunt was used. Intraoperative fasciotomy was performed in 12 out of 18 patients with lower limb ischaemia. Completion arteriography revealed residual thrombi in the distal foot of four patients, in whom intraarterial thrombolysis was effective. During the follow-up period of 1.5 to 2 years, the upper and lower limb preservation rate was 100 and 89%, respectively. The upper limb function was judged excellent in five patients, good in one and fair in one. In the lower limbs it was excellent in 11 patients, good in three, fair in one and poor in one. Conclusions: To ensure life and functional limb salvage of patients with devastating vascular injuries, a well organised multidisciplinary approach is necessary. Key Words: Arterial injury; Venous injury; Limb bone fracture; Thrombolysis; Arteriography; Acute ischaemia. Introduction Vascular injuries associated with limb bone fractures are sm:prisingly uncommon, with a reported incidence of less than 3%. 1 Most of the recent literature on the subject has consisted of case reports, and collective experience with a uniform approach to the manage- ment of vascular injuries associated with fractures is relatively infrequent. 2-1° The present study was undertaken with the aim of identifying the optimal methods of management leading to functional limb salvage. Please address all correspondence to: Asterios N. Katsamouris, University of Crete Medical School Herakleion University Hospital Herakleion, Crete, Greece. Twenty-five patients with arterial injuries associated with upper or lower limb bone fractures treated during the last 7 years were reviewed retrospectively. Patients whose injuries precluded limb salvage because of severe and extensive extravascular trauma or "cadaveric" limb underwent primary amputation and were not included. Similarl)~ patients who were subsequently referred after initial management and revascularisation in another hospital were not included. The median age was 27 years (range 16 to 62). There were 24 men and 1 woman. The majority of injuries (24) were produced by trauma from motorcycle and other vehicle accidents, Patients and Methods 1078-5884/95/010064 + 07 $08"00/0 © 1995 W. B. Saunders Company Ltd.
Transcript of Limb Arterial Injuries Associated with Limb Fractures ... · of 1.5 to 2 years, the upper and lower...

Eur J Vasc Endovasc Surg 9, 64-70 (1995)
Limb Arterial Injuries Associated with Limb Fractures: Clinical Presentation, Assessment and Management
Aster ios N. Ka tsamour is 1 , Kostas Ster iopoulos 2, Panos Katonis 2, Kostas Chr istou a, John Drosit is 1, Tat iana Lefaki 4, Sophoc les Vassi lak is 1 and Emmanue l Dre tak is 2
IVascular Surgical Unit, 2Department of Orthopedics and Traumatology, and 4Department of Anaesthesia, University of Crete Medical School, Herakleion University Hospital, Herakleion Crete, Greece, and 3Department of Surgery B2,
Hippocrates General Hospital, Thessaloniki, Greece
Objectives: Review of limb arterial injuries associated with limb fractures. Design: Retrospective study. Setting: University Hospital. Materials and Methods: The clinical presentation, assessment and management of 25 patients with upper (seven) and lower (18) limb arterial injuries associated with limb bone fractures has been retrospectively reviewed. Main Results: Five patients presented with life threatening injuries and classic signs of acute limb ischaemia, 15 patients had an obvious limb arterial injury, and 5 presented with a suspected limb arterial injury. The site of arterial damage was: superficial femoral (4); popliteal (11); tibioperoneal trunk (3); anterior tibial (4); posterior tibial (3); peroneal (2); axillary (1); brachial (5); radial (4); and ulnar artery (4). The types of arterial repair were: autogenous vein interposition or bypass grafting (17); P.T.F.E. (2); end-to-end anastomosis (14); and Iigation (8). The popliteal vein was injured in six cases, repaired in four and Iigated in two; the superficial femoral vein was injured in four cases, repaired in three and ligated in one; and the axillary vein was injured in one case and was ligated. Primary nerve repair was employed in six out of seven injured nerves. Skeletal fixation preceded vascular repair in 21 patients and in four a Javid shunt was used. Intraoperative fasciotomy was performed in 12 out of 18 patients with lower limb ischaemia. Completion arteriography revealed residual thrombi in the distal foot of four patients, in whom intraarterial thrombolysis was effective. During the follow-up period of 1.5 to 2 years, the upper and lower limb preservation rate was 100 and 89%, respectively. The upper limb function was judged excellent in five patients, good in one and fair in one. In the lower limbs it was excellent in 11 patients, good in three, fair in one and poor in one. Conclusions: To ensure life and functional limb salvage of patients with devastating vascular injuries, a well organised multidisciplinary approach is necessary.
Key Words: Arterial injury; Venous injury; Limb bone fracture; Thrombolysis; Arteriography; Acute ischaemia.
Introduction
Vascular injuries associated with limb bone fractures are sm:prisingly uncommon, with a reported incidence of less than 3%. 1 Most of the recent literature on the subject has consisted of case reports, and collective experience with a uniform approach to the manage- ment of vascular injuries associated with fractures is relatively infrequent. 2-1°
The present s tudy was under taken with the aim of identifying the optimal methods of management leading to functional limb salvage.
Please address all correspondence to: Asterios N. Katsamouris, University of Crete Medical School Herakleion University Hospital Herakleion, Crete, Greece.
Twenty-five patients with arterial injuries associated with upper or lower limb bone fractures treated dur ing the last 7 years were reviewed retrospectively. Patients whose injuries precluded limb salvage because of severe and extensive extravascular t rauma or "cadaveric" limb underwen t pr imary amputat ion and were not included. Similarl)~ patients who were subsequently referred after initial management and revascularisation in another hospital were not included. The median age was 27 years (range 16 to 62). There were 24 men and 1 woman.
The majority of injuries (24) were produced by t rauma from motorcycle and other vehicle accidents,
Patients and Methods
1078-5884/95/010064 + 07 $08"00/0 © 1995 W. B. Saunders Company Ltd.

Arterial Injuries Associated with Fractures 65
some of which were agricultural, and two injuries were penetrating, caused by single high-velocity missiles. There were forty-one arterial injuries in total. Eighteen patients (72%) sustained fractures to the lower and seven (28%) to the upper limbs. Open fractures dominated (72%). In the group of 18 patients with lower limb fractures, 27 arterial injuries occurred. Popliteal artery injuries were the most common, (11), while superficial femoral, tibioperoneal trunk, anterior tibial, posterior tibial, and peroneal artery injuries occurred in four, three, four, three, and two cases, respectively. In the seven patients with upper limb fractures 14 arterial injuries were incurred. The bra- chial artery was involved in five cases, axillary in one, radial in four, and ulnar in four cases.
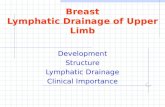
The site of associated arterial damage extended beyond the adjacent fracture site in five patients. One brachial artery injury extending to the brachial artery bifurcation was related to a supracondylar humerus fracture, three cases of popliteal artery injury extend- ing above knee were related with tibial condylar fractures, and one case of popliteal artery trifurcation damage was related to fractures of the lower third of tibia and fibula (Fig. 1). Associated injuries of major veins were identified in 11 patients. The popliteal vein was involved in six cases, superficial femoral vein in four and axillary veins in one case. Associated injuries of major motor nerves were present in seven patients. The median nerve was involved in two cases, tibial nerve in one, common peroneal in one, deep peroneal nerve in one, ulnar in one, and brachial plexus in one case. The associated remote injuries are listed in Table 1. Avulsion involving two or more muscle compart- ments or complete laceration of two or more tendons were identified in 15 patients, and skin loss resulting in delayed closure due to contamination or large avulsion required split-thickness skin graft or flap closure occurred in eight patients. Seven patients required intensive care for more than 24 hours.
According to clinical presentation the patients were classified into three categories.
The first category included five patients with life threatening injuries and classic signs of limb ischae- mia who presented with severe haemorrhagic shock and required immediate exploration to stop bleeding and treat shock. After initial stabilisation of their vital signs, diagnostic arteriogram (intraoperatively) was performed only for the patients presented with lower limb ischaemia.
The second category included the majority (15). These patients had an obvious limb arterial injury, but their t rauma was not life threatening. The arterial injury was disclosed by the presence of a pulseless or ischaemic (pallor and coolness associated with a
Fig. 1. The high diagnostic value of intraoperative arteriography in patients with arterial injuries associated with limb bone fractures is reflected in this Figure. In this case the politeal artery trifurcation damage is related to a distal fracture of the lower third of the tibia and fibula.
regional systolic arterial pressure less than 40 mmHg) limb. These patients underwent urgent surgical exploration and treatment. Four patients had upper limb and 11 lower limb ischaemia. Two of the patients with upper limb ischaemia underwent a preoperative
Table 1. Assoc ia ted remote injuries
Injury No. of patients
Limb bone fractures 5
Rib fractures 6
Head injuries 5
Haemothorax 2
Pneumothorax 2
Flail chest 1
Lung contusion 5
Spleen rupture 2
Liver rupture 1
Eur J Vasc Endovasc Surg Vol 9, January 1995

66 A .N . Katsamouris et aL
diagnostic arteriogram in the vascular radiology unit, while the other two patients with forearm injuries did not. Diagnostic arteriography was employed in the operative room for all patients with lower limb ischaemia.
The third category included five patients who presented with no clinical evidence of arterial injury. However, these patients had high suspicion of an arterial injury because of the nature of the associated bone and soft tissue injuries (all patients), abnormal motor or sensory function (two patients) and decreased regional arterial systolic pressure (three patients). The four patients with lower limb fractures were immediately transferred to the operating room for intraoperative diagnostic arteriography, surgical exploration and treatment. The remaining patient with an upper limb injury underwent diagnostic arteriog- raphy in the vascular radiology unit prior to surgical exploration and treatment.
Preoperative delays were calculated from the time of the accident to arrival in the operating room. The median prehospital delay was 1 hour and 30 minutes (range 15 minutes to 6 hours and 30 minutes). For the patients who underwent diagnostic arteriography intraoperatively, the median time interval from admis- sion to surgery was 1 hour and 30 minutes (range 1 hour to 2 hours and 15 minutes), while for the patients who underwent initial diagnostic arteriography in the vascular radiology unit, the median time was 2 hours and 45 minutes (range 1 hour and 30 minutes to 3 hours and 30 minutes).
All patients were operated upon under general anaesthesia and the vascular and orthopaedic sur- geons were involved in the surgical procedures from the beginning to the end of surgery. Generally, the incision was generous to gain proximal and distal control. In all cases of popliteal artery or tibioperoneal t runk injury, a medial approach was used.
The types of arterial repairs are listed in Table 2, with autogenous vein interposition or bypass grafting in 17 cases, PTFE bypass grafting in two, end-to-end anastomosis in 14, and ligation in eight cases. As indicated in Table 2, arterial ligation was performed for injured calf or forearm arteries. The rationale for the reconstruction of such small arteries was to leave two main calf arteries or one main forearm artery patent. End-to-end anastomosis was performed in cases when no more than 2 cm of the injured artery had been lost. All the autogenous vein grafts were obtained from the greater saphenous vein of the non- injured leg to avoid impairing venous return on the side of injury. PTFE was used as in two patients when the greater saphenous vein was too small for grafting (3 mm or less in diameter).
Table 2. Types of arterial repair
Lower limb Upper limb
Artery No Repair Artery No Repair type type
S.F.* 2 Vein graft
S.F. 1 P.T.F.E. graft
S.F. 1 End-to-end
Popliteal**
(A.K.) 1 P.T.F.E. graft
(A.K.) 1 End-to-end
(B.K.) 5 Vein graft
(B.K.) 2 End-to-end
(A + B.K.) 2 Vein graft
TPT*** 2 Vein graft
TPT 1 End-to-end
A.Tt 4 Ligation
P.T.§ 2 End-to-end
P.T. 1 Vein graft
Peroneal 2 End-to-end
Total number 27
Axillary 1 Vein graft
Brachial 3 Vein graft
Brachial 2 End-to-end
Radial 1 End-to-end
Radial 3 Ligation
Ulnar 2 End-to-end
Ulnar 1 Vein graft
Ulnar 1 Ligation
14
* S.F. = superficial femoral. **(A.K.) = above knee, (B.K.) = below knee, (A + B.K.) = above and below knee. ***TPT = tibioperoneal trunk, i-A.T. = anterior tibial. §P.T. = posterior tibial
The popliteal vein was repaired in four cases (two by an end-to-end anastomosis and two by inter- position of a vein graft) and ligated in two. The superficial femoral vein was repaired in three (two by interposition of a vein graft, one by interposition of a PTFE graft) and ligated in one. Finally, the injured axillary vein was ligated.
Operative skeletal fixation was employed in all patients. Vascular repair preceded skeletal fixation in four patients and vice versa in the rest because of bone instability of the extremity which might have jeopar- dised the vascular repair. An intraluminal Javid shunt was used in four of the patients who required fracture external fixation before vascular repair because of a severely ischaemic, flail lower extremity. The method of skeletal fixation was internal in six patients, with the use of a plating technique in three, intramedullary rods in three, and external in the remaining 19 patients. Primary nerve repair was employed in six cases, and secondary in the remaining brachial plexus injury. All patients with popliteal artery injuries
Eur J Vasc Endovasc Surg Vol 9, January 1995

Arterial Injuries Associated with Fractures 67
associated with vein injuries underwent calf fasciot- omy before vascular reconstruction. Fasciotomy was combined with vascular repair in 12 out of 18 patients presented with ischaemic legs. No fasciotomy was performed in patients presented with upper limb ischaemia.
No patient was sytematically heparinised during surgery. However, in all cases a small amount (100-150 ml) of dilute heparin solution, 50 U/ml, was gently injected into the lumen of the injured artery proxi- mally and distally before the vascular clamps were applied. A balloon catheter was routinely used to clear possible distal thrombotic material.
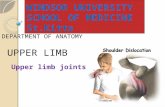
Doppler signals from distal arteries (ulnar, radial, posterior tibial, anterior tibial and peroneal artery) were obtained after arterial repair. When the Doppler signal was normal, completion arteriography was not performed. In five cases it was not normal and arteriography showed a defect in a tibioperoneal arterial end-to-end anastomosis which was corrected in one case and residual arterial thrombi in the foot in the other four (Fig. 2). In these cases a long epidural catheter (28 gauge) was inserted infrapopliteally
Fig. 2. Completion (intraoperative) arteriogram shows no visualisation of small arteries in the distal foot, clue to distal thrombi.
through the superficial femoral artery for continuous diluted heparin infusion during the first 24 post- operative hours (15-20000 U/24 hrs) followed by a continuous infusion of recombinant human tissue- type plasminogen activator (rt-PA) for the next 48 hours, which was again, followed by heparin infusion for another 48 hours period. The rt-PA was given in two divided doses (one dose of 50 rag/6 hrs for each day). All these patients established normal Doppler signals in at least one pedal artery. Postoperatively, vascular integrity was estimated by clinical and a hand-held Doppler examination and colour Doppler in 13 cases.
Results
The follow-up period ranged from 1.5 to 2 years and the results were estimated in terms of patency rate, amputation rate, limb salvage, morbidity and mortality.
The initial arterial reconstruction in the seven patients with upper limb ischaemia was successful in six. One patient with axillary and brachial artery injuries due to a gunshot injury required reoperation on the first postoperative day because of interposition vein graft thrombosis. All these patients had durable arterial repairs during the follow-up period, estimated by Doppler pressures or colour Doppler imaging.
The initial arterial reconstruction in the 18 patients with lower limb ischaemia was successful in 17 (95%). However, amputation was performed in two patients. One patient required an above knee amputa- tion on the 17th postoperative day due to extensive calf muscle necrosis, despite patency of arterial repairs at the time of amputation. The duration of the warm limb ischaemia time prior to surgery was 9 hours. The other patient had a below knee amputation on the 4th postoperative day due to severe sepsis and the arterial repair was found thrombosed at amputation. During the follow-up period, one posterior tibial artery repair thrombosed on the 40th postoperative da~; without affecting limb function. Arterial patency was assessed by Doppler pressures or colour Doppler imaging. Two popliteal venous repairs thrombosed in the early postoperative period, while the other two popliteal and the three femoral venous repairs remained patent during the follow-up period. Colour Doppler imaging was very useful in determining the patency of these major veins.
The median hospital stay was 28 days (range 16 to 46 days). The early morbidity was related mainly to
Eur J Vasc Endovasc Surg Vol 9, January 1995

68 A.N. Katsamouris et aL
the severity of limb and remote organs or structures trauma. No deaths occurred.
The upper and lower limb salvage rate was 100% and 89%, respectively. Limb function was related mainly to the severity of nerve trauma. Upper limb function was excellent in five patients, good in one patient (nerve paresthesia and cold intolerance) and fair in one patient (flexion contructure, nerve par- esthesia and decreased range of motion). Out of 16 patients with lower limb salvage, long-term results were judged excellent in 11 patients, good in three patients (leg edema in one and leg edema ~nd nerve paresthesia in the other two patients), fair in one patient (decreased range of motion) and poor in one patient (foot drop).
Discussion
Vascular injuries associated with limb fractures are usually caused by high energy traumaJ 1'~2 Complex decisions made by vascular and orthopaedic surgeons inevitably focus around efforts aimed at functional limb salvage. However, with the high incidence of multiple systems involved, these injuries demand a well organised multidisciplinary approach for appro- priate management. From Table 1 and the fact that more than 30% of our patients experienced severe skin loss and nearly 30% required intensive care, the significant conclusion is that although vascular and orthopaedic surgeons were team leaders, anaesthesiol- ogists, plastic surgeons and neurosurgeons played an important role in the overall management of these patients. This kind of approach has been also ernphas- ised by other authorsJ' 3, 6, 9, 13, 14
After control of haemorrhage and resuscitation, our top priority in the management of patients with limb injuries was early restitution of arterial flow in the ischaemic limb, in an effort to reduce the limb warm ischaemia time. Therefore, all patients with obvious or high suspicion of lower limb arterial injuries, were transferred immediately to the operat- ing room for urgent surgical exploration and treatment.
Precise and prompt diagnosis of arterial injury is paramount in order to ensure limb viability. 13' 14 In most cases of penetrating or blunt arterial trauma, preoperative diagnostic arteriography is not neces- sary. However, surgical exploration may not be suffi- cient in precisely locating the extension of the arterial damage in all cases, especially when the femoral or
popliteal artery are involved. 15'16 We agree that preoperative diagnostic arteriography performed in the vascular radiology unit is often not appropriate for these patients as it is important to act as fast as possible, for "delay is the e n e m y ' Y Intraoperative arteriography is highly recommended in such cases, as it can be quickly and easily performed by a simple femoral artery puncture. Our strategy is supported by others who also believe that combined limb injuries always warrant diagnostic arteriography in view of the high likelihood of occult vessel injuries. 16" 18 The diagnostic value of colour Doppler vascular imaging 19 in vascular injuries associated with limb bone frac- tures or dislocations has yet to be estimated. Although colour Doppler imaging was employed only in 13 cases it is our opinion that this technique cannot replace preoperative or intraoperative arteriography, especially in those cases presented with large haema- tomas, extensive soft tissue damage and unstable or flail limbs.
A balloon embolectomy catheter was used rou- tinely for clearing all possible distal thrombotic material. In cases with distal arterial thrombosis on completion arteriography, adjunctive therapy with intraarterial thrombolysis may re-establish the arterial circulation of the ischaemic foot in a few hours, with a low complication rateJ °' 25
The concept that as long as there is one uninjured patent infrapopliteal arter)~ the remaining arteries may be either ligated or repaired without any sig- nificant difference in limb salvage and early or late vascular complication, 22 cannot be supported by the present data. Bone non-union with only one patent artery in the lower extremity and subsequent healing after delayed late arterial reconstruction has been reported. ~3 Injuries immediately below the knee or above the ankle are more likely to completely inter- rupt blood flow as compared to mid-leg injuries. 24 Additionally, blunt trauma tends to compromise blood flow in several vessels more often than penetrat- ing injuries. Furthermore, fascial compartments in extremities with extensive bone and soft tissue dam- age may contain significant amount of edema fluid or extravasated blood, indirectly compromising unin- jured vessels and further impeding blood flow. There- fore, we suggest that two infrapopliteal arteries should be patent at the end of surgery in those patients with arterial trauma associated with lower leg fractures.
The optimal management of upper or lower extremity major vein injuries is controversial. In our series, the three patients with ligated popliteal or femoral veins and the two with thrombosed vein grafts in the early postoperative period developed leg
Eur J Vasc Endovasc Surg Vol 9, January 1995

Arterial Injuries Associated with Fractures 69
edema that affected the morbidity but not limb salvage. Although no clear benefit from venous repair is recognised in some series, 25 we believe that local venous repair can be recommended in nearly every instance. It is thought that even temporary patency is beneficial in avoiding acute venous hypertension, edema, and distal compartment syndrome.25, 26 Extended venous reconstruction is complex and time- consuming and the decision to perform them is only justified if the safety of the patient is not jeopardised.3, z6
Early fasciotomy should be considered in most cases of combined lower extremities injury The devastating nature of these injuries, largely due to violent forces, the associated muscle and integument trauma, and the often considerable preoperative and operative warm ischaemia time all favour the devel- opment of tissue edema that may progress to cause a compartment syndrome that may seriously jeopardise a successful arterial reconstruction. 3"~3 Fasciotom)~ therefore, was used liberally in our patients with lower limb ischaemia. Significant morbidity due to fasciotomy was not observed.
The sequence of vascular repair and fracture stabilisation remains unclear. In this series skeletal stabilisation was carried out first in 21 patients because of unstable fractures which might have jeopardised the vascular repair. In four of those patients an intraluminal Javid shunt was initially used. Some surgeons have stressed the importance of initial skeletal fixation followed by vascular repair to prevent possible further damage to the repaired vessels.4, 27 Others prefer vascular repair before skel- etal fixation is undertaken or advocate the use of intraluminal shunts for early restitution of blood flow to the distal extremit)~ followed by skeletal fixation
9 28 and then definite vascular repair. ' In conclusion: 1. Well organised multidisciplinary management
is important for both life and functional limb salvage.
2. In order to ensure limb viability, early restitu- tion of arterial flow in the ischaemic limb should be a high priority.
3. Precise and prompt diagnosis of the site of arterial injury is desirable. Intraoperative diagnostic arteriography of the lower extremity is a simple procedure that should always be performed if time does not permit preoperative arteriography.
4. Although skeletal stabilisation followed by vascular repair appears to be the appropriate sequence for most combined limb injuries with unstable ortho- paedic deformity, the final decision must be made on an individual basis. In this regard, the close co-
operation of vascular and orthopaedic surgeons is important.
References
1 NORGREN L. Vascular complications from limb fractures. In: GREENHALGH ~ and HOLEIER LH, eds. Emergency Vascular Surgery. London: W.B. Saunders Co. 1992, pp. 313-330.
2 SMITH RF, SZILAGYI DE, ELLIOTT JP JJr. Fractures of long bones with arterial injury due to blunt trauma. Arch Surg 1969; 99: 315-318.
30'DONNELL TF, BREWSTER DC, DARLING RC, et al. Arterial injuries associated with fractures and/or dislocations of the knee. J Trauma 1977; 17: 775-784.
4 WOLMA FJI LARRIEU AJ, ALSOP GC. Arterial injuries of legs associated with fractures and dislocations. Am ] Surg 1980; 140: 806~09.
5 EREN N/ OZGEN G, GUREL A, ENER BK, EURTUN K. Vascular injuries and amputation following limb fractures. Thor Cardio- vasc Surg 1990; 38: 48-50.
6 ZEHNTNER MK, PETROPOULOS Pl BUSCH H. Factors determining outcome in fractures of the extremities associated with arterial injuries. J Orthop Trauma 1991; 5: 29-33.
7 WEAVER FA, ROSENTHAL RE, WATEICHOUSE G, et al. Combined skeletal and vascular injuries of the lower extremities. Am Surg 1984; 50: 189-194.
8 MENZOIAN JO, DOYLE JE, CANTELMO NL, et al. A comprehensive approach to extremity vascular trauma. Arch Surg 1985; 120: 801-805.
9 SCHLICKEWEL W, KUNER EH, MULLAJI AB, GOTZE B. Upper and lower limb fractures with concomitant arterial injury. J Bone Joint Surg 1992; 74B: 181-188.
10 DAHL A, VARGHESE M. Salvage of limb with vascular trauma. J Bone Joint Surg 1992; 74B: 189-194.
11 KENNEDY JC. Complete dislocation of the knee joint. ] Bone Joint Surg 1963; 45A: 889-904.
12 ROMAN PD, HOPSON CN, ZENNI EJ Jr. Traumatic dislocation of the knee: a report of 30 cases and literature review. Orthop Rev 1987; 16: 917-924.
13 BARROS D' SA AAB. Leading article: The rationale for arterial and venous shunting in the management of limb vascular injuries. Eur J Vasc Surg 1989; 3: 471-474.
14 BARROS D' SA AAB. Complex vascular and orthopaedic limb injuries (Editorial). J Bone Joint Surg 1992; 74B: 176-178.
15 ANDERSON RJ, HOBSON RW, PADBERG FT, et al. Penetrating extremity trauma: identification of patients at high risk requiring arteriography. J Vasc Surg 1990; 11: 544-548.
16 WALKER ME, POINDEXTER JM, STOVALL I. Principles of manage- ment of shotgun wounds. Surg Gynecol Obstet 1990; 170: 97-101.
17 MANSFIELD AO, et al. Vascular injuries (Editorial). J Bone Joint Surg 1989; 71B: 738.
18 WEAVER FA, YELLIN AE, BAUER MAP, et al. Is arterial proximity a valid indication for arteriography in penetrating extremity trauma? a prospective analysis. Arch Surg 1990; 125: 1256-1260.
19 NICOLAIDES AN, RENTON SC. Duplex scanning: the second sight of the vascular surgeon. Eur ] Vasc Surg 1990; 4: 445-447.
20 McNAMARA TO, BOMBERGER RA, MERCHANT RF. Intra-arterial urocinase as the initial therapy for acutely ischemic lower limbs. Circulation 1991; 83 (suppl): I106-II19.
21 RICOTTA JJ, GREEN RM, DEWEESE JA. Uses and limitations of thrombolytic therapy in the treatment of peripheral arterial ischemia: results of a multi-institutional questionnaire. J Vasc Surg 1987; 6: 45-50.
22 BALLARD JL, BUNT TJ/ MALONE l M. Management of small artery vascular trauma. Am J Surg 1992; 164: 316-319.
Eur J Vasc Endovasc Surg Vol 9, January 1995

70 A .N . Katsamouris et aL
23 DEITZ DM, TAYLOR LM~ BEALS RK, PORTER JM. Role of revascular- isation to treat chronic nonhealing fractures in ischemic limbs. J Vasc Surg 1989; 10: 535-541.
24 I(EELEY SB, SNYDER WH, WEIGELT JA. Arterial injuries below the knee: fifty-one patients with 82 injuries. ] Trauma 1983; 23: 285-292.
25 PECK JJ, EASTMAN B, BERGAN JJ, et al. Popliteal vascular trauma; a community experience. Arch Surg 1990; 125: 1339-1344.
26 RICH MM. Principles and indications for primary venous repair. Surgery 1982; 91: 492-496.
27 BASSETT FH III, SILVER D. Arterial injury associated with fractures. Arch Surg 1966; 92: 13-19.
28 NUNLEY JA, KOMAN LA, URI3ANIAK R. Arterial shunting as an adjunct to major limb re{rascularisation. Ann Surg 1981; 193: 271-273.
Accepted 18 April 1994
Eur J Vasc Endovasc 8urg Vol 9, January 1995