Levine H-challenges in the Cgmp Manufacturing of Hescs-lessons Learned From Monoclonal...
24
BioProcess Technology Consultants www.bptc.com Challenges in the cGMP Manufacturing of hESCs: Lessons Learned from Monoclonal Antibodies ISCT 2011 Annual Meeting Rotterdam, The Netherlands May 18 – 21, 2011
Transcript of Levine H-challenges in the Cgmp Manufacturing of Hescs-lessons Learned From Monoclonal...

BioProcess Technology Consultantswww.bptc.com
Challenges in the cGMP Manufacturing of hESCs: Lessons Learned from Monoclonal Antibodies
ISCT 2011 Annual MeetingRotterdam, The Netherlands May 18 – 21, 2011

Important Considerations in cGMP Manufacturing
Performance/Productivity
Capacity
Quality/Regulatory
Speed
Cost
Scalability
Flexibility
From Clone to Clinic®

Growth in Monoclonal Antibody Product Sales
0
5
10
15
20
25
30
35
40
45
2002 2003 2004 2005 2006 2007 2008 2009
Annu
al Sales ($
Billions)
Largest class of biologic
products today
From Clone to Clinic®

Hurdles in Monoclonal Antibody Development
ImmunogenicityHAMA limited early product development
Product ConsistencyReproducible glycosylation with scale and process
ProductivityLow titers and poor purification yields caused initial high COGS
From Clone to Clinic®

Evolution of Monoclonal Antibody Products
1976 1986 1997 2000 2002
First murine MAbapproval
Köhler & Milstein discover MAbs
First fully human MAb approval
First Chimeric MAb approval
ZenapaxFirst humanized MAb approval
First IgG‐fusion protein approval
Centoxinapproved but withdrawn from market
1991
From Clone to Clinic®

Approval of Monoclonal Antibody Products by Year
0
1
2
3
4
5
6
No. Produ
cts A
pproved
From Clone to Clinic®

Standardized Production Host and Culture Conditions
CHO adapted for suspension culture
From Clone to Clinic®
SP2/0NS0
CHO
Chemically defined, serum (or protein)‐
free media
Operating parameters improve productivity to ≥50 pg/cell/day
Fed‐batch culture with specific nutrient feeds
Increased peak cell densities and run
duration

0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
11000
0 2 4 6 8 10 12 14 16 18 20 22
Tite
r (m
g/L)
Days
“Typical” Monoclonal Antibody Cell Culture Process10 – 100 mL vial
50 L 7,500 L 20,000 L1,000 L200 L
High cell density and high growth rate media enable maximal seed density in inoculum train and production bioreactor
Cell densities at harvest ≥3 x 1010 cells/L Titers ≥5 g/L in 12 – 15 day culture Culture time from vial to harvest
~22 – 25 days
From Clone to Clinic®

Innovation has Increased Titers and Yields
1
10
100
1,000
10,000
1980 1985 1990 1995 2000 2005 2010 2015 2020
Titer in mg/L
Antibodies Recombinant Antibodies Hybridoma Fc Fusion
New technologies to improve cell line development and expression levels coupled with improved and optimized media, supplements, and bioreactor conditions have increased titers
Over 3 log increase in titer over the last 20 years Current commercial products range from 0.2 – 3.0 g/L
Ref: W. Noe (2011), T. Charlebois (2006), M. Smith, (2005), F. Wurm (2004) From Clone to Clinic®

Platform Processes Enable Large Scale Purification
Ref: B. Kelley, ACS Conference, (2006) From Clone to Clinic®

Cost of Manufacturing Monoclonal Antibodies Phase of
DevelopmentQuantity
Required (Kg)Relative
Production Scale Estimated Cost
1 0.5 – 2 1 $0.75 – 1.2 MMPer batch
2 1 – 10 1 – 3 $1.8 – 2.5 MMPer batch
3 5 – 25 3 – 5 $2.5 – 5.0 MMPer batch
Commercial 10 – 1,000(per year) 5 – 10 ≤$1,000/gram
Typically ≤$150
Early stage production typically priced on per batch basis due to small scale and incomplete process development
Batch prices similar at each scale but larger batch size lowers COGS Commercial production at 2,000 – 20,000 L Higher titers lowering average commercial scale bioreactor requirements
From Clone to Clinic®

52%
7%
19%
9%13%
Depreciation
Raw Materials
Consumables
Labor
Misc.
Large Scale Monoclonal Antibody Production Costs
MAb Titer g/L
Cost $/gram
Based on annual production of 100 Kg/year;bioreactor size ranging from 1,000 – 10,000 L
$‐
$100
$200
$300
$400
$500
0 3 6 9 12
From Clone to Clinic®

Issues in the Manufacture of Stem Cells Product complexity greater than monoclonal antibodies
• Final product not homogeneous― May contain partially differentiated or undifferentiated cells
• Induced pluripotent stem cells are genetically modified Manufacturing challenges
• Anchorage dependent growth requires microcarriers• Production scale limited due to metabolic concerns, low density
propagation, and limited experience― Wide variety of culture systems currently in use which may have
limited scalability Unique supply chain issues
• Fragility of cells may require frozen storage and shipping• Limited shelf‐life of product• Shipping protocols must ensure product viability and sterility
From Clone to Clinic®

Allogeneic Cell Therapy Products in Development
0
10
20
30
40
50
60
Market Phase 3 Phase 2 Phase 1 Preclinical
Num
ber o
f Produ
cts
Embryonic Somatic
From Clone to Clinic®
Includes company sponsored products only. Several investigator ‐sponsored trials in progress

As With Early Biologics, “Process = Product”
Will require extensive testing, especially early in development, to ensure product quality and consistency
Potential for different advice or requirements by individual regulatory authorities
Lack of product and process knowledge limit ability to make changes during development
Manufacturing process should be fully cGMP compliant and relatively final prior to Phase 1
Concept very different than monoclonal antibodies Identity testing requires use of expression markers
ProductComplexity
ProcessChanges
ProductQuality
From Clone to Clinic®

Critical Factors in Cell Therapy Manufacturing Quality of all product contact surfaces and media/buffers
• Product contact surfaces can impact differentiation, changing product composition
• Different microcarriers have different impact on cell growth and differentiation
Control of product to prevent contamination• Viral inactivation or removal not possible• Terminal sterilization not possible• Operator training essential
Potency of growth factors used to initiate differentiation• Often several factors used to initiate differentiation
― Balance of activities essential to initiate correct differentiation Limited material available for QC testing
From Clone to Clinic®

Cell Therapy Manufacturing Process
WCB (undifferentiated hECs)
Cell Expansion
Differentiation
Cell Harvest
Formulation and Fill
Cryopreservation
Ref: www.geron.com From Clone to Clinic®

Cell Therapy Process Parameters
From Clone to Clinic®
Typical Harvest Densities 2D culture in T‐flasks – 8.0 x 105 cells/cm square 3D culture in bioreactors un‐optimized – 2.0 x 109 cells/L 3D culture in bioreactors optimized – 2.0 x 1010 cells/L
50% overall recovery yield from bioreactor to vial
Low dose applications, e.g., spinal cord injury 2.0 x 107 cells/dose; single dose
High dose applications, e.g., congestive heart failure 5.0 x 108 cells/dose; single dose
Target patient population of 10,000 – 550,000 patients at market peak Market penetration of 30 – 50% at market peak

From Clone to Clinic®19
Low dose/Small patient population/Low market penetration
High dose/High patient population/High market penetration
Total annual production requirement• 1.4 x 1014 cells
Total annual production volume• 14,000 L
Production in small bioreactors15 batches/yr @ 1,000 L/batch
Very Small Production Volumes Required
Total annual production requirement• 6.6 x 1010 cells
Total annual production volume• 6.6 L
Production in T‐flasks or spinners

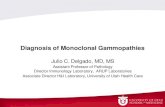
Potential Commercial COGS for hESC Products
From Clone to Clinic®
Case 1 Case 2 Case 3
Bioreactor size (L) 500 1,000 2,000
Cell density at harvest (cells/L) 2.0 x 1010 2.0 x 1010 2.0 x 1010
Overall yield 50% 50% 50%
Total cells per batch (cells) 5.0 x 1012 1.0 x 1013 2.0 x 1013
Doses per batch (5 x 108 cells/dose) 10,000 20,000 40,000
Batches per year 30 15 8
Doses produced per year 300,000 300,000 320,000
Cost per batch ($ million) 11.74 8.41 11.53
Cost per dose ($/dose) 1,174 420 288
Case 1 & 2 = Single use bioreactor; Case 3 = Stainless steel bioreactorCosts based on hypothetical manufacturing process and do not include storage or shipping of productCost predominantly driven by depreciation and raw materials

Single Use Bioreactors for hESC Manufacturing
XcellerexXDRTM Bioreactor
Sartorius StedimBiostat® Culti‐bag
Thermo Fisher (Hyclone)Single‐use Bioreactor
ATMINucleoTMBioreactor
GE HealthcareWave Bioreactor
From Clone to Clinic®

Process Area 6,781 ft2 Total Area 13,014 ft2
Class C 667 ft2 Class D 3,315 ft2
Process Equipment $5.0 MM Total Capital Cost $15 MM
hESC Manufacturing Facility
Upstream
Processing
Cell recoveryCell processingFill/Finish
Inoculum
Media & BufferPreparationWash
Personnel Corridor
Materials CorridorStaging Area
Supply Corridor Class C Areas: Inoculum preparation Fill/finish
Class D Areas: Cell culture (Single use bioreactor) Downstream processing Media and buffer preparation Clean glassware unloading and storage
Media and buffer storage in controlled, non‐classified areas
From Clone to Clinic®

Thank You!
BioProcess Technology Consultants, Inc.12 Gill Street, Suite 5450Woburn, MA 01801
+1.781.281.2703
Howard L. Levine, Ph.D.

Follow us…
www.bptc.com
www.bioprocessblog.com
bptcGlobal
www.linkedin.com/company/bioprocess-technology-consultants-inc.