Let's Talk Research Annual Conference - 24th-25th September 2014 (Paula Bennett)
27
A quantitative study investigating the effects of computerised clinical decision support in the emergency department Paula Bennett – Nurse Consultant Emergency Department
-
Upload
nhsnwrd -
Category
Healthcare
-
view
55 -
download
0
Transcript of Let's Talk Research Annual Conference - 24th-25th September 2014 (Paula Bennett)

A quantitative study investigating the
effects of computerised clinical decision
support in the emergency department
Paula Bennett – Nurse Consultant
Emergency Department
Objectives
• Quality & safety in ED
• eTriage
• The research
• The future
Stockport
• DGH
• New department in 1995 (63,000)
• 2013 - 90,091
• Pre 2010 no IT in ED at all!
The Quality & Safety Challenge
• Rising attendances
• Increasing elderly population
• Performance (95%)
• Workforce issues
• Economy

Local and international experience
• Increasing numbers of clinical guidelines
• Common
• Rare
• Risky
• If followed
• Risk managed
• Improved patient experience
• Appropriate tests
• Appropriate timely referrals
• If not followed……………………
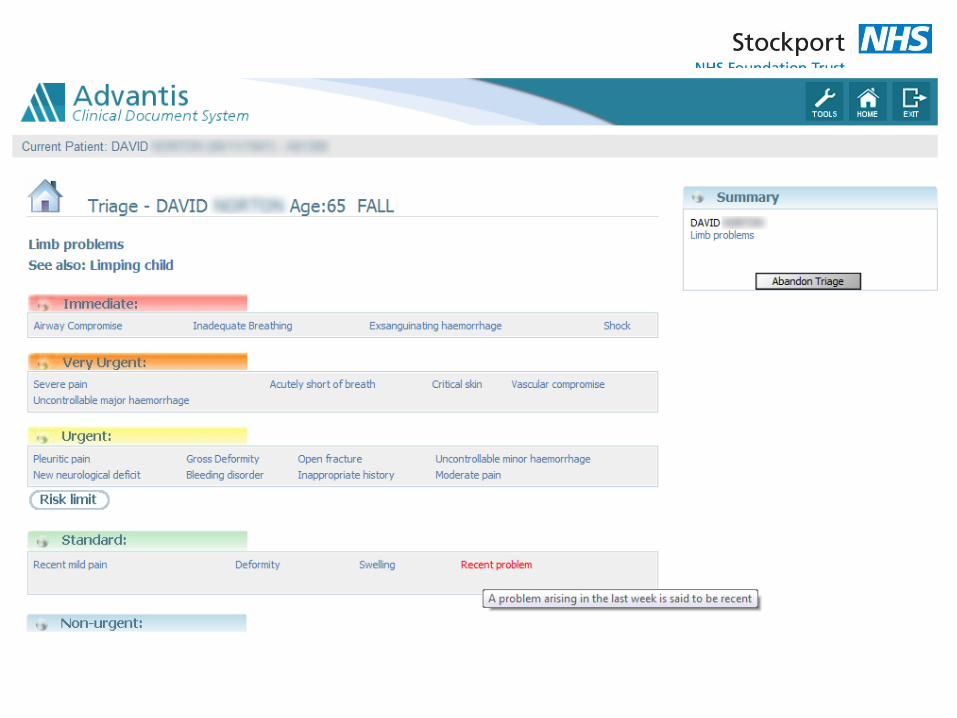
eTriage
2008 – Discussions began about development
Launch 12/4/2010
by 17/6/13 – 293,206 “eTriaged”
2013 – Results of research






The Study
• Research Question
Does the introduction of a computerised clinical-decision support system improve the quality of triage decisions and safety within the ED?

CCDSS
"Clinical Decision Support systems link health observations with health
knowledge to influence choices by clinicians for improved health care".
Elements of a CCDSS
• Individualized patients data is entered
• Computerised database
• Pt specific recommendations are generated

Systematic Review CCDSS Literature
Acute Care – majority improved process much less likely to improve outcome
Prevention – some positive evidence for screening, less evidence for
outcomes, safety, cost & satisfaction
Chronic Disease – improved processes, some improved patients health
Test ordering – some modify clinicians behaviours
Drug Prescribing – poor evidence – no recommendations to adopt
Drug monitoring – can improve process of care esp. insulin and Vit K. effects
on outcome uncertain
Haynes 2011 http://www.implementationscience.com/series/CCDSS
CCDSS in ED
• 23 studies of computerised decision-support in EDs
• 13 demonstrated significant impact on clinical care with the use of a
CCDSS
• Increased guideline adherence
• Increased “speed”
• Time to antibiotics
• Improved documentation

Quasi-experimental study
Outcome Measures • Quality
• Pain Assessment
• Was pain scored?
• Pain management
• Was appropriate pain relief given?
• Safety
• Triage decision
• Was the right priority allocated?
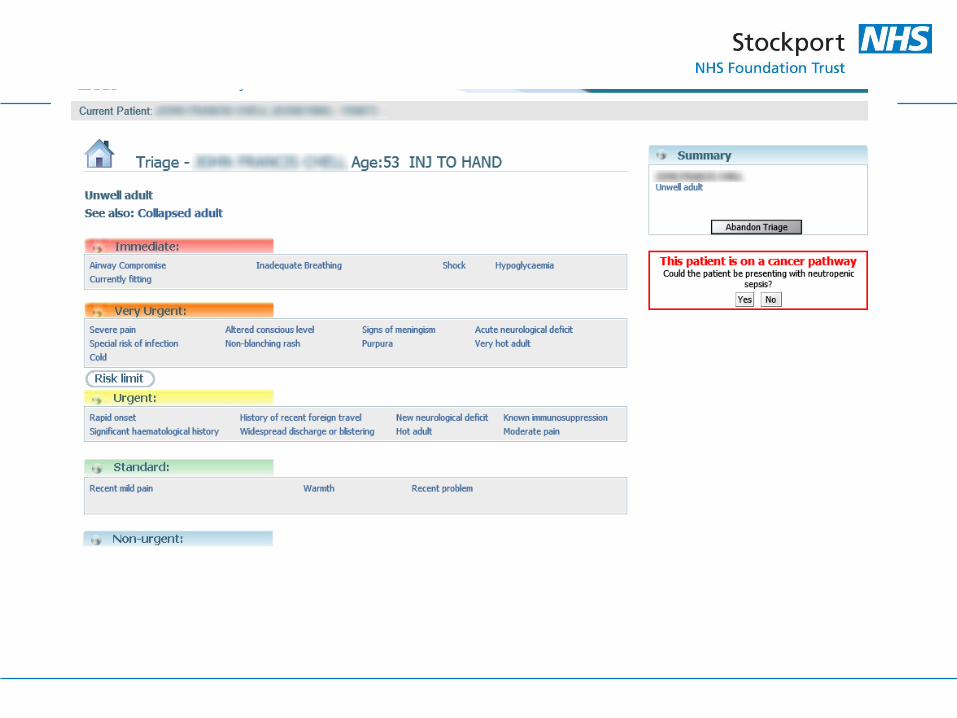
• Neutropenic sepsis
• Urgent priority
• Immediate FBC
• IV antibiotics <1hr

Research method
• Interrupted time series design
• Pre-eTriage
• 400 randomised records.
• 26 pts with chemotherapy induced neutropenia
• Post-eTriage
• 400 randomised records.
• 18 pts with chemotherapy induced neutropenia
Data collection
points
1
2
3
4
X
5
6
7
8
Time intervals
April 2009
July 2009
Oct 2009
Jan 2009
12th April 2010
April 2011
July 2011
Oct 2011
Jan 2012

• Inter-rater reliability
– >80% agreement
– Kappa
• fair to moderate agreement
• Ethics
– Not required as “service evaluation” not research
• Research Governance
– Safe storage of data

Results
• Chi Square
• Did eTriage improve quality?
• Was there an improvement in pain assessment – YES
• p<0.01
• Was there an improvement in appropriate pain relief – YES
• p<0.01
• Did eTriage improve safety?
• Was there an improvement in prioritisation – YES
• p<0.01
• Was there improvement in the management of patients with Neutropenic sepsis – No significant difference

Results – logistic regression
• Confounding variables
• Age
• Gender
• Mode of arrival
• Triage nurse experience
• Time
• Intervention (eTriage)
• Correct triage priority
– Mode of arrival
• p<0.001
• OR 1.962 [CI 1.298-2.965]
– Intervention
• p<0.034
• OR 14.499 [CI 1.221-172.228]
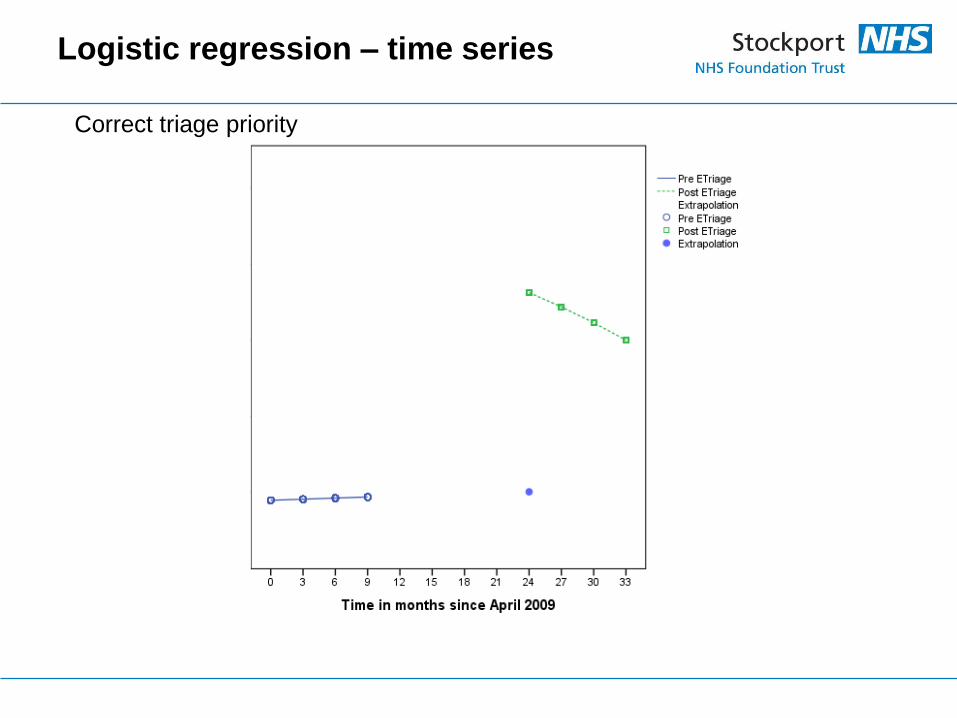
Logistic regression – time series
Correct triage priority

Limitations
• 1 system
• 1 department
• Judgments of researcher may have led to unintentional bias
• Small sample of “high risk” patients – further research required on larger samples. • Only captured those with confirmed neutropenia not all those
suspected of it

Conclusion
• CCDSS in ED does improve the quality and safety of Triage
decisions
– Consistent safety
– Consistent quality
• The effect on the management of patients with “high risk” conditions
was not shown to be significant
– Further research needed
• In the current ED climate clinicians must harness the potential that
technological solutions can offer

The future……………………
Any questions?