Lesclous 1997, Alopecia areata of Dental Origin
3
An unusual case of alopecia areata of dental origin Philippe Lesclous, DCD, MCU, PH, and Louis Maman, DCD, MCU, PH, Montrouge, France FACULTt~DE CHIRURGIE DENTAIRE, UNIVERSITI~PARIS V The relationship between dental foci of infectious or mechanical nature and alopecia areata is analyzed through this case. There are many different causes for this dermatologic disease, and a dental origi n seems to be very uncommon. Such a cause can only be confirmed a posteriori by a complete recovery of the patient after the dental cause is removed. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:290-2) Alopecia areata and dental foci are rarely associated; however, this relationship has been long reported.1 Alopecia areata is characterized by a sudden hair loss restricted to a specific area and is reversible as a gen- eral rule. It mostly affects a young male population. 2 This dermatitis has a strong psychologic impact on the patient, because it involves the face and scalp, where esthetic considerations play an important role in self- perception. Alopecia areata of dental origin can also affect the eyebrows or the beard as is illustrated by the following report. CASE REPORT A 35-year-old male patient arrived for evaluation with 3 days Of diffused, dull, and unceasing bilateral retromandibu- lar pains. His medical history revealed epileptic antecedents, fully stabilized during the previous year by medical treatment that included phenobarbital and valproic acid. Extraoral examination revealed two symmetric labiomental alopecic areas on each side of the face. These dermatologic lesions were small, each approximately 3 cm in diameter, smooth, and well demarcated (Fig. 1). Totally asymptomatic, these areas had appeared over the past 6 months. The beard did not seem affected at the borderline of the alopecic zone. Intraoral examination revealed the absence of the right upper canine and the right and left lower third molars on the dental arches. These teeth were impacted, as shown on the panoramic radiograph (Fig. 2). With no other causes being identified, the third mandibular molars were believed to be the origin of the retromandibular pains bilaterally, and conse- quently their extraction with the patient under local anesthe- sia was planned. The right lower third molar, most painful, was extracted first. Medical treatment including an antibiotic (amoxicillin), an analgesic (dextropropoxyphene)o and oral rinses of anti- septic (chlorhexidine) were prescribed. Surgical follow-up was uneventful, and sutures were removed 1 week later. The patient was not seen again for 6 weeks, during which time his beard grew in the alopecic areas. We noted that the glabrous area had nearly completely disappeared on the side of the extraction and had persisted on the opposite side (Fig. Received for publication June 6, 1996; revised Aug. 13, 1996; accepted Apr. 19, 1997. Copyright © 1997 by Mosby-Year Book, Inc. 1079-2104/97/$5.00 + 0 7/13182954 Fig. 1. Initial presentation of alopecia areata localized on beard on both sides. Fig. 2. Initial panoramic radiograph revealed impaction of right upper canine and right and left lower third molars. 3). The retromandibular pains had also disappeared on the side of the extraction. The left lower third molar was then extracted following the same protocol. Two months later the pains had completely disappeared, and the beard was bushy on both sides (Fig. 4). DISCUSSION There is no general agreement on the cause and pathogenesis of alopecia areata, although the immuno- 290
-
Upload
lorenzo-acerra -
Category
Documents
-
view
34 -
download
2
description
cure of alopecia obtained when an hidden infection of a wisdom tooth was discovered.Italian: guarigione da alopecia ottenuta identificando un'infezione nascosta di un dente del giudizio.(Lesclous 1997)
Transcript of Lesclous 1997, Alopecia areata of Dental Origin

An unusual case of alopecia areata of dental origin Philippe Lesclous, DCD, MCU, PH, and Louis Maman, DCD, MCU, PH, Montrouge, France FACULTt~ DE CHIRURGIE DENTAIRE, UNIVERSITI~ PARIS V
The relationship between dental foci of infectious or mechanical nature and alopecia areata is analyzed through this case. There are many different causes for this dermatologic disease, and a dental origi n seems to be very uncommon. Such a cause can only be confirmed a posteriori by a complete recovery of the patient after the dental cause is removed. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:290-2)
Alopecia areata and dental foci are rarely associated; however, this re la t ionship has been long reported.1 Alopecia areata is characterized by a sudden hair loss restricted to a specific area and is reversible as a gen- eral rule. It most ly affects a young male population. 2
This dermatitis has a strong psychologic impact on the patient, because it involves the face and scalp, where esthetic considerations play an important role in self- perception. Alopec ia areata of dental origin can also affect the eyebrows or the beard as is illustrated by the following report.
CASE REPORT A 35-year-old male patient arrived for evaluation with 3
days Of diffused, dull, and unceasing bilateral retromandibu- lar pains. His medical history revealed epileptic antecedents, fully stabilized during the previous year by medical treatment that included phenobarbital and valproic acid.
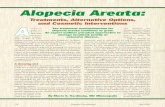
Extraoral examination revealed two symmetric labiomental alopecic areas on each side of the face. These dermatologic lesions were small, each approximately 3 cm in diameter, smooth, and well demarcated (Fig. 1). Totally asymptomatic, these areas had appeared over the past 6 months. The beard did not seem affected at the borderline of the alopecic zone.
Intraoral examination revealed the absence of the right upper canine and the right and left lower third molars on the dental arches. These teeth were impacted, as shown on the panoramic radiograph (Fig. 2). With no other causes being identified, the third mandibular molars were believed to be the origin of the retromandibular pains bilaterally, and conse- quently their extraction with the patient under local anesthe- sia was planned.
The right lower third molar, most painful, was extracted first. Medical treatment including an antibiotic (amoxicillin), an analgesic (dextropropoxyphene)o and oral rinses of anti- septic (chlorhexidine) were prescribed. Surgical follow-up was uneventful, and sutures were removed 1 week later.
The patient was not seen again for 6 weeks, during which time his beard grew in the alopecic areas. We noted that the glabrous area had nearly completely disappeared on the side of the extraction and had persisted on the opposite side (Fig.
Received for publication June 6, 1996; revised Aug. 13, 1996; accepted Apr. 19, 1997. Copyright © 1997 by Mosby-Year Book, Inc. 1079-2104/97/$5.00 + 0 7/13182954
Fig. 1. Initial presentation of alopecia areata localized on beard on both sides.
Fig. 2. Initial panoramic radiograph revealed impaction of right upper canine and right and left lower third molars.
3). The retromandibular pains had also disappeared on the side of the extraction.
The left lower third molar was then extracted following the same protocol. Two months later the pains had completely disappeared, and the beard was bushy on both sides (Fig. 4).
DISCUSSION There is no general agreement on the cause and
pathogenesis of alopecia areata, although the immuno-
290

ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 84, Number 3
LescIous and Maman 291
Fig. 3. Photo of alopecia areata, which almost disappeared on right side of face 6 weeks after right lower third molar was extracted, whereas it persisted on opposite side. Fig. 4. Eight weeks after left lower third molar was extract-
ed, regrowth was complete on both sides of face.
logic hypothesis is most frequently put forward. This hypothesis is based on the presence of a perifollicular lymphocytic infiltrate and a frequent decrease of the cellular mediated immunity during alopecic diseases. 3 This decrease is illustrated by a fall in the circulating T lymphocytes and by a lessened reactivity to delayed hypersensitivity tests. 4 Moreover, nonspecific antibod- ies (antismooth muscle antibodies) or specific ones (antipilous follicle cell antibodies) are observed irregu- larly. 5 For these reasons general or topical immunother- apy is currently the baseline of treatment. 6-9
An emotional factor is very frequently associated with the start of an alopecic disease. Often such patients have an immaturity and a dependence profile. I°
The pathogenesis of alopecia areata of dental origin is usually based on a trigemino-sympathetic reflex. I1 A peripheral stimulus of infectious or mechanical nature could be the origin of a centripetal duct composed of a triple neuron system. This system is composed of a peripheral terminal trigeminal fiber, a bulbothalamic, and a thalamocortical fiber.
The centrifugal duct may be principally composed of a perivascular plexus of sympathetic fibers surrounding external carotid terminal branches with which trigemi- nal branches develop numerous connections. In addi- tion, all along the length of the bulb, the trigeminal descending root is tightly connected to the sympathetic nuclei. This centrifugal duct may induce an angiospasm of the pilosebaceous follicle, resulting in trophic disor- der and subsequent hair loss. 12 However, the piloseba- ceous follicle is still functional, so regrowth is often observed after the peladogenic foci is eradicated. If the tegumentary structure is damaged as in scarred alope- cia, the pilosebaceous follicle will show irreversible atrophy.
Etiopathogenic factors are most often multiple and
l'lllh 1 MOLAil
IN( hORN XN ) ( ~NINE hE('OND MOLAR
PREJ~IOLARS
M A X I L L A
TIIIRD MOI.AR
[ IIIRD MOI.AR [N(I~ORS ~ND ('..kNINE
. . . . . . . SECOND %IOt.A R
IN('lbOR5 AND CANINF FIRST MOLAR
ANDIBL I . I
FIGURE 5: LOCATIONS OF TROPHIC REPERCUSSIONS
Fig. 5. Locations of trophic repercussions.
interrelated, so that the elimination of one factor alone is rarely sufficient to bring about the complete recovery of the patient. Nevertheless, alopecia areata of dental origin can be considered a distinct clinical entity as is illustrated by this case report. With no other treatment than the dental foci eradication, a complete regrowth without any relapse of alopecia was observed.
In the case of alopecia areata where the origin is den- tal, peladic areas are generally small and few in number. They are glabrous in appearance and are clean, smooth, round, and well demarcated. The disease develops sud- denly, and depilation can succeed a dental episode after a few days or even after a few months. Previous medical consultation is thus important. Prognosis is favorable and recovery swift after dental foci eradication.
Alopecia areata of dental origin is generally located on the scalp but occasionally affects the beard and more

292 Lesclous and Maman
exceptionally the eyebrows. For this dermatitis it is gen- erally agreed that trophic repercussions appear on the same side as the dental focus and in specific locatioias characteristic of this lesion. Schematically, the location of the alopecic area is posterior to the causal tooth. Dental irritations of maxillar origin are located above a line starting at the labial commissure and terminating at the occiput. Those of mandibular origin are located below this line.
Rousseau-Decelle 13 has proposed a map of the alopecic area related directly to the causal tooth (Fig. 5). However, this concordance is not always respected as is shown in both this and other case reportsJ 4-16 Indeed, in this case peladic areas should have been related to lower premolars rather than lower third molars. The only clearly established findings of this case report are that (1) the removal of the lower third molars, which the initial panoramic radiograph showed to be very close to the inferior alveolar nerve, immediately preceded the regrowth of hair in the alopecic areas, and (2) the peladic areas were located just at the cutaneous emer- gence of the mental nerve, which is the terminal branch of the inferior alveolar nerve. Hence, mechanical stim- ulation of the nerve resulting in a depilation of the trophic areas can be postulated. In such a dermatitis a global approach is necessary, because unscarred restricted alopecia is most often of multifactorial origin, and so the treatment must be based on a multidiscipli- nary approach. 17
After the focus is eradicated, only complete regrowth can corroborate, a posteriori, whether dental factors are the sole cause.
REFERENCES 1. Jacquet L. Pathogenic de la pelade. Bull Soc Fr Dermatol
1902;13:299-322.
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY September 1997
2. Tobin D J, Fenton DA, Kendall MD. Cell degeneration in alope- cia areata: an ultrastructural study. Am J Dermatopathol 1991;13:248-56.
3. Withing DA. Histopathology of alopecia areata in horizontal sections of scalp biopsies. J Invest Dermatol 1995;104(Suppl): 26-7.
4. Jaworsky C, Kligman AM, Murphy GF. Characterization of inflammatory infiltrates in male pattern alopecia:implications for pathogenesis. Br J Dermatol 1992;127:239-46.
5. Galbraith GMR Thiers BH, Vasily DB, Fudenberg HH. Immunological profiles in alopecia areata. Br J Dermatol 1984;110:163-70.
6. Bertolino AE Clinical hair loss: diagnosis and treatment. J Dermatol 1993;20:604-10.
7. Shapiro J. Alopecia areata: update on therapy. Dermatol CIin 1993;11:35-46.
8. Shapiro J. Topical immunotherapy in the treatment of chronic severe alopecia areata. Dermatol Clin 1993; 11:6 l 1-7.
9. Drake LA, Ceilley RI, Cornelison RL, Dobes NL, Dorner N, Goltz RW, et al. Guidelines of care for alopecia areata. J Am Acad Dermatol 1992;26:247-50.
10. Consoli SG. Psychisme et pathologic du follicule pilo-sdbacte. Rev du Prat 1993;18:2370-4.
11. Romoli M, Cudia G. Alopecia areata and homolateral headache due to an impacted superior wisdom tooth. Int J Maxillofac Surg 1987;16:477-9.
12. Kuffer R, Larnberton JN. Pathologic cutanto-muqueuse et foy- ers bucco-dentaires. Paris: EMC Stomatologie, 1978:22042A10.
13. Rousseau-Decelle L. La pelade d'origine dentaire. Rev Stomatologie 1920;22:493-502.
14. Couturier E Un cas de pelade mentonnitre odontopathique. Inf Dent 1952;45:1124-7.
15. Fassina E Pelade d'origine dentaire. Inf Dent 1948;30:882-3. 16. Lattts A, Bataille R, Claudin D. A propos d'une pelade d'orig-
ine dentaire provoqute par deux germes surnumtraires. Rev Stomatologie 1963;9:863-6.
17. Mc Donagh AJ, Messenger AG. The aetiology and pathogenesis of alopecia areata. J Dermatol Sci 1994;(7 Suppl): 125-35.
Reprint requests: Philippe Lesclous, DCD, MCU, PH Facult6 de Chirurgie Dentaire Paris V 1, Rue Maurice Arnoux 92120 Montrouge France