Leptomeningeal Carcinomatosis as the Sole Manifestation of ... · • Leptomeningeal carcinomatosis...
5
Central Bringing Excellence in Open Access JSM General Surgery: Cases and Images Cite this article: Jones GD, Niotis K, Rajjoub R (2016) Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case Report. JSM Gen Surg Cases Images 1(3): 1015. *Corresponding author Gregory D. Jones, The Commonwealth Medical College, 414 Kings Highway, Carnegie, PA,15016, USA, Tel: (412)-722-9470; Fax: (412)-922-2922; Email: Submitted: 17 October 2016 Accepted: 30 October 2016 Published: 01 Novemebr 2016 Copyright © 2016 Jones et al. OPEN ACCESS Keywords • Leptomeningeal carcinomatosis • Carcinomatous meningitis • Recurrent gastric cancer • Metastasis • Signet ring Case Report Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case Report Gregory D. Jones 1,2 *, KellyannNiotis 1,2 , and Rodwan Rajjoub 3 1 The Commonwealth Medical College, USA 2 New York Presbyterian Hospital-Weill Cornell Medical Center, USA 3 Williamsport Regional Medical Center, USA Abstract Cancer of the leptomeninges, known as leptomeningeal carcinomatosis (LMC), is diffuse infiltration of malignant cells throughout the pia mater and the arachnoids membrane. LMC is most commonly seen with breast cancer, lung cancer, melanoma, leukemia, and large cell lymphoma. Rarely, LMC is found in gastric cancer. The prevalence of LMC in gastric cancer patients is reported to be between 0.16-0.69% and is usually found with widespread metastatic disease. To date, there have been 3 cases of LMC as the sole manifestation of gastric cancer recurrence. In this case; we present a 60 year old man who was diagnosed with Stage T2bN3M0 signet ring cell gastric adenocarcinoma. After surgical resection and adjuvant chemo-radiation, he had no evidence of disease with appropriate follow-up for 3 years. He then presented with a one-month history of confusion, ataxia, falls, and weakness concerning for normal pressure hydrocephalus. Gadolinium-enhanced MRI showed enlargement of the lateral and third ventricles, without meningeal enhancement. Lumber puncture cytology revealed gastric adenocarcinoma. The patient died three weeks later. This case raises interesting questions regarding the biology and metastatic behavior of gastric cancer. Physicians should have a high index of suspicion for LMC in patients with a history of cancer that present with changing neurological status. These patients should be evaluated with lumbar puncture and MRI with gadolinium. The median overall survival for patients with gastric LMC is only 4-6 weeks if untreated and 2-4 months with chemo/radiation therapy. ABBREVIATIONS LMC: Leptomeningeal Carcinomatosis; GERD: Gastroesophageal Reflux Disease; ED: Emergency Department; NCCN: National Comprehensive Cancer Network INTRODUCTION Cancer of the meninges, referred to as leptomeningeal carcinomatosis (LMC), is diffuse infiltration of malignant cells throughout the pia mater and the arachnoid membrane [1] (in contrast to the pachymeninges, which is also known as the dura mater). Primary carcinoma arising from the meninges, which is usually sarcoma thought to be associated with previous radiation therapy to the brain, is far less common than secondary involvement of the meninges due to metastasis [2]. Of those tumors that metastasize to the meninges, primary central nervous system tumors such as medulloblastoma, ependymoma, and glioblastoma multiforme have been reported. However, LMC is more commonly associated with cancers such as breast, lung, melanoma, leukemia, and large cell lymphoma [3]. Leptomeningeal carcinomatosis is estimated to occur in 3-8% of solid carcinomas [4]. Gastric carcinoma, which classically has been subdivided into diffuse and intestinal types, most commonly metastasizes to the liver, lung and peritoneum [5]. However, gastrointestinal malignancies can also metastasize to the meninges. The prevalence of LMC in gastric cancer patients is reported to be as low as 0.16-0.69% [1]. Leptomeningeal carcinomatosis caused by gastric cancer usually presents during late disease with metastasis to the peritoneum and liver generally occurring first [6]. In a study of 54 gastric cancer patients with LMC, the most frequently observed presenting symptoms were nonspecific, such as headache (85%)
Transcript of Leptomeningeal Carcinomatosis as the Sole Manifestation of ... · • Leptomeningeal carcinomatosis...
-
CentralBringing Excellence in Open Access
JSM General Surgery: Cases and Images
Cite this article: Jones GD, Niotis K, Rajjoub R (2016) Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case Report. JSM Gen Surg Cases Images 1(3): 1015.
*Corresponding authorGregory D. Jones, The Commonwealth Medical College, 414 Kings Highway, Carnegie, PA,15016, USA, Tel: (412)-722-9470; Fax: (412)-922-2922; Email:
Submitted: 17 October 2016
Accepted: 30 October 2016
Published: 01 Novemebr 2016
Copyright© 2016 Jones et al.
OPEN ACCESS
Keywords•Leptomeningeal carcinomatosis•Carcinomatous meningitis•Recurrent gastric cancer•Metastasis•Signet ring
Case Report
Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case ReportGregory D. Jones1,2*, KellyannNiotis1,2, and Rodwan Rajjoub31The Commonwealth Medical College, USA2New York Presbyterian Hospital-Weill Cornell Medical Center, USA3Williamsport Regional Medical Center, USA
Abstract
Cancer of the leptomeninges, known as leptomeningeal carcinomatosis (LMC), is diffuse infiltration of malignant cells throughout the pia mater and the arachnoids membrane. LMC is most commonly seen with breast cancer, lung cancer, melanoma, leukemia, and large cell lymphoma. Rarely, LMC is found in gastric cancer. The prevalence of LMC in gastric cancer patients is reported to be between 0.16-0.69% and is usually found with widespread metastatic disease. To date, there have been 3 cases of LMC as the sole manifestation of gastric cancer recurrence. In this case; we present a 60 year old man who was diagnosed with Stage T2bN3M0 signet ring cell gastric adenocarcinoma. After surgical resection and adjuvant chemo-radiation, he had no evidence of disease with appropriate follow-up for 3 years. He then presented with a one-month history of confusion, ataxia, falls, and weakness concerning for normal pressure hydrocephalus. Gadolinium-enhanced MRI showed enlargement of the lateral and third ventricles, without meningeal enhancement. Lumber puncture cytology revealed gastric adenocarcinoma. The patient died three weeks later. This case raises interesting questions regarding the biology and metastatic behavior of gastric cancer. Physicians should have a high index of suspicion for LMC in patients with a history of cancer that present with changing neurological status. These patients should be evaluated with lumbar puncture and MRI with gadolinium. The median overall survival for patients with gastric LMC is only 4-6 weeks if untreated and 2-4 months with chemo/radiation therapy.
ABBREVIATIONSLMC: Leptomeningeal Carcinomatosis; GERD:
Gastroesophageal Reflux Disease; ED: Emergency Department; NCCN: National Comprehensive Cancer Network
INTRODUCTIONCancer of the meninges, referred to as leptomeningeal
carcinomatosis (LMC), is diffuse infiltration of malignant cells throughout the pia mater and the arachnoid membrane [1] (in contrast to the pachymeninges, which is also known as the dura mater). Primary carcinoma arising from the meninges, which is usually sarcoma thought to be associated with previous radiation therapy to the brain, is far less common than secondary involvement of the meninges due to metastasis [2]. Of those tumors that metastasize to the meninges, primary central nervous system tumors such as medulloblastoma, ependymoma,
and glioblastoma multiforme have been reported. However, LMC is more commonly associated with cancers such as breast, lung, melanoma, leukemia, and large cell lymphoma [3]. Leptomeningeal carcinomatosis is estimated to occur in 3-8% of solid carcinomas [4].
Gastric carcinoma, which classically has been subdivided into diffuse and intestinal types, most commonly metastasizes to the liver, lung and peritoneum [5]. However, gastrointestinal malignancies can also metastasize to the meninges. The prevalence of LMC in gastric cancer patients is reported to be as low as 0.16-0.69% [1].
Leptomeningeal carcinomatosis caused by gastric cancer usually presents during late disease with metastasis to the peritoneum and liver generally occurring first [6]. In a study of 54 gastric cancer patients with LMC, the most frequently observed presenting symptoms were nonspecific, such as headache (85%)
-
CentralBringing Excellence in Open Access
Jones et al. (2016)Email:
JSM Gen Surg Cases Images 1(3): 1015 (2016) 2/5
and nausea/vomiting (58%) [1]. In addition, various neurological signs and symptoms were noted including altered mental status, seizure, motor weakness, sensory change, diplopia, hearing loss, and facial palsy. In a different series of 90 patients with LMC and various solid primary tumors, the most common neurological signs included reflex asymmetry (71%), weakness (60%), and mental status changes (31%), while the most common symptoms were lower motor neuron weakness (38%), headache (33%), and paraesthesias (31%) [3].
It is very uncommon for gastric cancer to present with only meningeal metastasis at the time of initial diagnosis, as most studies are small case series or case reports. Delaunoit et al., described four cases of gastric linitis adenocarcinoma with metastasis to the meninges [7]. However, all but one of these cases had widespread metastatic disease at the time of diagnosis of LMC. Even rarer, there have been few reports of LMC as the sole manifestation of recurrent gastric cancer. Saad et al., described an additional case of meningeal carcinomatosis due to primary gastric adenocarcinoma that was resected with negative margins one year prior [8]. This patient’s surveillance computed tomography (CT) 10 days prior to diagnosis of meningeal carcinomatosis did not show any evidence of widespread disease. To date, a total of 3 cases of LMC as the sole manifestation of metastatic gastric carcinoma recurrence have been reported in the literature [8,9].
We present a case of leptomeningeal carcinomatosis in a 64 year-old man with diffuse type adenocarcinoma without widespread metastasis, as various imaging modalities failed to show involvement of any other organs or tissues, and CSF cytologic analysis demonstrated that the tumor was present in the meninges.
CASE PRESENTATIONA 60 year-old man with a past medical history of
hypertension, hypercholesterolemia, and GERD presented to his primary care physician in March of 2011 for evaluation of upper abdominal discomfort and reflux unresponsive to medications. Upper endoscopy the following month showed one gastric ulcer, which was biopsied and shown to be a poorly differentiated adenocarcinoma with signet ring cell features and cytokeratin reactivity. The patient did not have any family history of oncologic disease, but was a previous 37.5 pack year smoker and consumed alcohol once daily, and was exposed to various occupational toxins and chemicals including asbestos. Staging CT scan showed evidence of three hepatic nodules concerning for malignant disease, however PET scan at this time demonstrated only mild focal FDG uptake in the distal stomach, with no other sites of uptake identified. However, subsequent ultrasound of the liver nodules (and later, their long-term unchanged appearance) suggested benign hemangiomas. A CEA level was also normal at 1.1.The tumor was classified as a Stage pT2bN3M0 gastric adenocarcinoma (as per the UICC classification, 7th edition), and partial gastrectomy was performed in July of 2011. The patient had an unremarkable postoperative course. Although margins were negative, twenty-three of twenty-four nodes were positive on postoperative pathological report. The following adjuvant treatment was initiated based on current NCCN guidelines:
1 cycle of 5-fleurouracil (5-FU) and Leucovorin followed by chemoradiation using Capecitabine followed by further treatment with 5-FU and Leucovorin. The patient was determined to be in remission upon completion of therapy. CT scans of the thorax, abdomen, and pelvis were negative at 3, 6, 9, and 12 months.
Over three and a half years after initial diagnosis, the patient presented to the ED after failing to improve from symptoms of a pressing, frontal headache thought to be due to sinusitis. At this time, the patient also reported a one-month history of worsening confusion, difficulty walking, falls, and generalized weakness greater in the legs than arms, in addition to recent low-grade fever, poor appetite, and weight loss. Neurologic exam revealed varying levels of alertness, and orientation to person but not place or time. The patient was able to follow commands, but had impaired attention demonstrated by inability to spell the word “world” backwards, along with frequent pauses after questions. The patient was noted to have coarse saccades, with an otherwise normal ophthalmologic exam. Motor testing was 5/5, with norigidity noted and absent Babinski and Hoffman sign. Tone was minimally to mildly increased and deep tendon reflexes were 2+ bilaterally. On sensory examination, there was decreased vibration, pinprick, and temperature to the distal lower extremities. Cerebellar testing by rapid alternating movements appeared to be impaired, in addition to mild dysmetria, but it was unclear if this was due to cerebellar pathology or difficulty understanding the command. A left greater than right postural tremor was present, unchanged since the early 1990s. The remainder of the physical exam was normal.
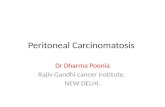
A head CT was obtained, which showed mild hydrocephalus, and thus a brain MRI with and without contrast was ordered. Figure (1) below shows the brain MRI with enlargement of the lateral and third ventricles, without leptomeningeal enhancement. At this time it was felt that normal pressure hydrocephalus was less likely, due to the subacute nature of the presenting symptoms in addition to the prominent systemic symptoms. A lumbar puncture was then performed to rule out normal pressure hydrocephalus; results as shown in Table (1), notable for as
Figure 1a (Left) Axial image of the FLAIR sequence MRI showing enlarged lateral ventricles. Periventricular white matter hyperintensities are noted, which are nonspecific and have been shown to increase with age. There is no DWI correlate indicating acute changes as evidenced by the image on the right. Note the lack of FLAIR signal within the sulci on the left image.
-
CentralBringing Excellence in Open Access
Jones et al. (2016)Email:
JSM Gen Surg Cases Images 1(3): 1015 (2016) 3/5
follows: CSF total protein >250, 7 WBCs (80% lymphocytes, 0% PMNs), IgG = 16.5, opening pressure = 450 mm H2O, and cytology consistent with metastatic gastric carcinoma. The elevated protein level, very high opening pressure, and low glucose levels further point to a malignant origin of the hydrocephalus. CT scan of the chest, abdomen and pelvis showed, changes of COPD but no masses, nodules, or lymphadenopathy, and subsequent PET scan confirmed no recurrence of disease. The patient declined further treatment and was transferred to the Palliative Medicine team. Over the next 3 weeks the patient worsened and eventually died in his home five weeks after presenting to the ED, and nearly 4 years since his initial gastric cancer diagnosis.
DISCUSSIONThe striking clinical picture that this LMC patient presents
raises interesting questions regarding the biology and metastatic behavior of certain subclasses of gastric cancer. Two major theories exist regarding the pathophysiology of leptomeningeal metastasis in general: direct contiguous infiltration and hematogenous spread. The first involves afocus of disease (often undetectable by imaging) on the surface of the cerebrum, rupturing superiorly into the subarachnoid space and seeding the leptomeningesa long the usual path of CSF flow. Hematogenous spread to the leptomeninges can also occur, by seeding of the choroid plexus along perivascular spaces [2]. A newer theory has also been proposed, when a study of 28 cases of pure LMC (most with lung or breast as the primary tumor) revealed parameningeal metastases and suggested the possibility of propagation through the perineural spaces in cases of upper gastrointestinal tract tumors [3]. Studies regarding the possible link of between site of tumor within the meninges and route of spread are ongoing.
Regardless of route, however, imaging the entire neuraxis (preferably MRI) in addition to cytologic examination of the CSF is the standard diagnostic methods for presumed leptomeningeal carcinomatosis. CSF findings include increased opening pressure, pleocytosis, elevated protein concentration, increased LDH, decreased glucose concentration, and the presence of tumor markers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9) in the case of gastric cancer [4]. As the diagnostic accuracy of lumbar puncture (LP) is only 50-60% after a single LP and 90% after 3 LPs, MRI is considered complementary and can be invaluable, detecting up to 50% of cases with false-negative LPs [1]. Mahendru et al., stressed the importance of understanding physiologic meningeal enhancement in a contrast-enhanced MRI in order to successfully diagnose pathological enhancement. Thin, smooth, discontinuous enhancement of the cerebral convexities occurs during MRI in a patient with physiologic enhancement, as the durra lacks a blood-brain barrier and thus allows the leptomeninges to display uptake following administration of intravenous contrast [2]. On the other hand, leptomeningeal carcinomatosis can cause focal or diffuse enhancement of ependymal lining and perivascular spaces, not necessarily corresponding to the cerebral convexities.
More specifically, both MRI and CT can demonstrate multiple masses within the subarachnoid space, hydrocephalus without a discernible cause, or diffuse leptomeningeal enhancement. The latter enhancement pattern, further described as focal areas of
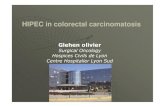
Figure 1b (Left) Axial image of the FLAIR sequence MRI showing enlarged 3rd and occipital horn of the lateral ventricles. Periventricular white matter hyperintensities are again noted. There is no DWI correlate indicating acute changes shown on the right sided image. Note the lack of FLAIR signal within the sulci on the left image.
Figure 1c Axial image of the FLAIR sequence MRI showing enlargement of the 4th ventricle. Note the lack of enhancement throughout the leptomeningeal spaces of the posterior fossa and cerebellum.
Table 1: CSF analysis values from lumbar puncture performed on 1/7/2015. Note the increase in total protein, IgG, opening pressure, and metastatic gastric cytology.
CSF Characteristics Patient Value Reference Value
Total Protein >250 mg/dL 15-45 mg/dL
WBC Count7 cells/µL (80%
lymphocytes, 0% PMNs)
0-5 cells/µL
IgG 16.5 mg/dL 0-9.1 mg/dL
RPR Negative Negative
Lyme Antibody Negative Negative
Opening Pressure 450 mm H2O 60% serum glucose
Cytology Metastatic Gastric CA N/A
-
CentralBringing Excellence in Open Access
Jones et al. (2016)Email:
JSM Gen Surg Cases Images 1(3): 1015 (2016) 4/5
linear enhancement, especially in a nodular pattern, has been referred to as “cake icing” or “zuckerguss” and can be found in the brain, spine, or both [1,14]. Sensitivity rates have risen with advances in MRI technology, particularly better T1-weighted images as well as the advent of 3-dimensional T1-weighted sequences and post contrast fluid attenuated inversion recovery (FLAIR) [13]. FLAIR has been shown to be useful in these circumstances as it demonstrates increased signal of the sulci reflecting the abnormal subarachnoid space, although contrast enhanced T1 MRI has characteristically been more sensitive than FLAIR [1]. No large recent study has determined MRI sensitivity in detecting LMC, although many studies have postulated that it is in the 70-90% range.
The median survival after diagnosis of LMC for patients with solid tumors ranges from 4 to 11 months [10]. In LMC from gastric carcinoma, the median overall survival for patients after diagnosis of LMC is only 4-6 weeks if left untreated. Even despite vigorous therapy, many patients do poorly and the median survival is only about four months [11]. The optimum choice of therapy depends upon a thorough assessment of the neurologic extent of disease, which should include complete neuraxis imaging. Patients with extensive bulky disease may be best treated with systemic chemotherapy, whereas those with a positive CSF cytology but negative imaging may be treated with intrathecal (IT) chemotherapy and spared the systemic toxicity of intravenous drug. Methotrexate remains the most frequently utilized drug for IT administration, despite its limited success [12]. Occasionally, for palliation, radiotherapy has been shown to be effective for selected patients with severe neurologic dysfunction or mass lesions with a high tumor burden [1].
This patient’s initial presentation was suggestive of normal pressure hydrocephalus (NPH) without a previously discernable cause, which is not uncommon for initial presentation of LMC in the literature. It should be noted that the patient’s leg weakness could also be an indicator of disease in the spinal cord, although no gross metastatic disease was seen on imaging, and hydrocephalus secondary to LMC appears to be more likely. Referral for ventricular peritoneal (VP) shunt placement was initially discussed, but it was decided that a lumbar puncture was necessary prior to proceeding, especially given his duration of symptoms and accompanying systemic symptoms. This case highlights the importance of lumbar puncture for cytology prior to VP shunt placement in patients with a history of gastric carcinoma that present with evidence of NPH, as placement of a VP shunt would result in widespread seeding of the abdomen with malignant cells. Although the life expectancy of patients diagnosed with LMC is quite low, subjecting these patients to an additional procedure and increasing the burden of disease would be counterproductive. Physicians should have a high index of suspicion for LMC in patients with a history of cancer that present
with unremitting headache or changing neurological status. Although headache is thought to be the most common presenting symptom of LMC, any neurologic symptom, especially those that involve different regions of the neuraxis (i.e. cerebral, spinal, and/or cranial nerve symptoms) should prompt immediate further investigation with LP and MRI with gadolinium.
REFERENCES1. Kim N-H, Kim J-H, Chin H-M, Jun K-H. Leptomeningeal carcinomatosis
from gastric cancer: single institute retrospective analysis of 9 cases. Ann Surg Treat Res. 2014; 86: 16-21.
2. Mahendru G, Chong V. Meninges in cancer imaging. Cancer Imaging. 2009; 14-21.
3. Braeuninger S, Mawrin C, Malfertheiner P, Schildhaus HU, Seiler C, Dietzmann K, et al. Gastric adenocarcinoma with leptomeningeal carcinomatosis as the presenting manifestation: an autopsy case report. Eur J Gastroenterol Hepatol. 2005; 17: 577-579.
4. Lee HG, Lee B, Kim SM, Suh BJ, Yu HJ. A Case of gastric adenocarcinoma presenting as meningeal carcinomatosis. Korean J Intern Med. 2007; 22: 304-307.
5. Metastatic Cancer. National Cancer Institute. 12 May 2016.
6. Guo J-W, Zhang X-T, Chen X-S, Zhang X-C, Zheng G-J, Zhang B-P, et al. Leptomeningeal carcinomatosis as the initial manifestation of gastric adenocarcinoma: A case report. World J Gastroenterol. 2014; 20: 2120-2126.
7. Delaunoit T, Boige V, Belloc J, Elias D, Lasser P, Duvillard P, et al. Gastric linitis adenocarcinoma and carcinomatous meningitis: An infrequent but aggressive association - report of four cases. Ann Oncol. 2001; 12: 869-871.
8. Nibal S, Ahmad Alsibai, Tarik Hadid. Carcinomatous Meningitis Due to Gastric Adenocarcinoma: A Rare Presentation of Relapse. World J Gastrointest Oncol. 2014; 6: 450-453
9. Rizvi S, Fateh S, Abbi Kamal KS, Jiang Y. Leptomeningeal Carcinomatosis as the Only Manifestation of Disease in Recurrent Gastroesophageal Cancers. Gastrointest Cancer Res. 2011; 4: 68-71.
10. Taghizadeh-Kermani A, Emadi-Torghabeh A, Taraz-Jamshidi S. A report of a rare gastric cancer case: leptomeningeal carcinomatosis. Iran J Cancer Prev. 2015; 8: 60-62.
11. DeAngelis LM, Boutros D. Leptomeningeal metastasis. Cancer Invest. 2005; 23: 145-154.
12. Oh SY, Lee S-J, Lee J, Lee S, Kim S-H, Kwon H-C, et al. Gastric leptomeningeal carcinomatosis: Multi-center retrospective analysis of 54 cases. World J Gastroenterol. 2009; 15: 5086-5090.
13. Tomura N, Narita K, Takahashi S, Otani T, Sakuma I, Yasuda K , et al. Contrast-enhanced multi-shot echo-planar FLAIR in the depiction of metastatic tumors of the brain: comparison with contrast-enhanced spin-echo T1-weighted imaging. Acta Radiol. 2007; 48: 1032-1037.
14. Collie DA, Brush JP, Lammie GA, Grant R, Kunkler I, Leonard R, et al. Imaging features of leptomeningeal metastases. Clin Radiol. 1999; 54: 765-771.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3994606/http://www.ncbi.nlm.nih.gov/pubmed/19965290http://www.ncbi.nlm.nih.gov/pubmed/19965290http://www.ncbi.nlm.nih.gov/pubmed/15827450http://www.ncbi.nlm.nih.gov/pubmed/15827450http://www.ncbi.nlm.nih.gov/pubmed/15827450http://www.ncbi.nlm.nih.gov/pubmed/15827450https://www.ncbi.nlm.nih.gov/pubmed/18309694https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3934485/https://www.ncbi.nlm.nih.gov/pubmed/11484967https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4266818/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4266818/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4266818/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3109883/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4360353/http://www.ncbi.nlm.nih.gov/pubmed/15813508http://www.ncbi.nlm.nih.gov/pubmed/15813508https://www.ncbi.nlm.nih.gov/pubmed/19860003http://www.ncbi.nlm.nih.gov/pubmed/17957522http://www.ncbi.nlm.nih.gov/pubmed/17957522http://www.ncbi.nlm.nih.gov/pubmed/17957522http://www.ncbi.nlm.nih.gov/pubmed/17957522http://www.ncbi.nlm.nih.gov/pubmed/10580769http://www.ncbi.nlm.nih.gov/pubmed/10580769http://www.ncbi.nlm.nih.gov/pubmed/10580769
-
CentralBringing Excellence in Open Access
Jones et al. (2016)Email:
JSM Gen Surg Cases Images 1(3): 1015 (2016) 5/5
Jones GD, Niotis K, Rajjoub R (2016) Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case Report. JSM Gen Surg Cases Images 1(3): 1015.
Cite this article
Leptomeningeal Carcinomatosis as the Sole Manifestation of Recurrent Gastric Adenocarcinoma: A Case AbstractAbbreviationsIntroductionCase PresentationDiscussionReferencesFigure 1aFigure 1bFigure 1cTable 1