
Lecture 1 761 Pediatric Dentistry2011.ppt
42
Pediatric tooth development and disturbances Donald Avery & Dean, Dentistry for the Child and olescent, 8 th ed., Chapter 4 pp50-54, Chapter 7 10 ing the textbook to class alicized notes have been questioned on the Dental D
description
Pediataric Dentistry
Transcript of Lecture 1 761 Pediatric Dentistry2011.ppt

Pediatric tooth development and disturbances
McDonald Avery & Dean, Dentistry for the Child and Adolescent, 8th ed., Chapter 4 pp50-54, Chapter 7 103-123Bring the textbook to classItalicized notes have been questioned on the Dental Decks

Overview
Life cycle of TeethInitiationBudProliferationDifferentiationAppositionCalcificationEruptionAttrition
Calcification timingDevelopmental Disturbances

3
6th week in utero:Initiation/Induction. The
mesenchyme induces ectodermal changes:
Primordium of ectodermal portion of the teeth: Base layer of oral epithelial cells thicken, forming:
Dental lamina (also called the Common dental germ) which:
Becomes part of the embryonic jawsGives rise to: primary teeth and all permanent
molars
Life cycle of Teeth
Bud Cap
Bell AppositionMcDonald p 52 4-1

4
Life Cycle
6-9th weeks iuBud stage
Special Dental Germs— 10 swellings bud in each dental lamina enamel organ starts to form
Researchers disagree about the overlap of each of these stages.
We will use McDonald’s dates as our reference. Evidence of human teeth is as early as 6 weeks iu
McDonald p 52 4-1

5
Life Cycle
10th week iuCap/Proliferation StageRapid growth:Cap of epithelial cellsPapilla—epithelial cells under
the cap—will form dentin and pulp
Tooth germ is complete by end of cap and has enamel organ, dental papilla and dental sac with morpho-and histo-differentiation
McDonald p 52 4-1

6
Life Cycle Collaboration Activity
Handouts—Embryos
Consult with the student sitting next to you about the approximate ages of the embryos.

7
Life Cycle 11th week iu--Bell Stage—final shapingContinued Histo- and Morpho-differentiationElongation of inner enamel epithelial cells of
enamel organ causes mesenchymal cells next to dental papilla to become odontoblasts; Inner enamel epithelium will become ameloblasts.
Enamel is from ectoderm; all other tooth structure is from mesenchyme.
Hertwig’s epithelial root sheath (HERS)-inner and outer epithelium at the cervical of the enamel organ which directs root shape (number) as well as dentin formation in the root Therefore, ectodermal cells determine the crown and root shapes.
Follicle or dental sac will form PDL and
cementum
A. Bud
B. Cap
C. Bell McDonald p 52 4-1

8
Life Cycle
Morphodifferentiation:11wk iu-primary centrals13wk iu-primary laterals14 wk iu-primary canines
McDonald p. 52 4-1

9
Life CycleAppositionAmeloblasts and odontoblasts 1. Line up at DEJ and DCJ2. Secrete matrix at “growth
centers” deposits of the first layer of dentin preceeds deposition of the first layer of enamel
3. Start at the apex of cusps
McDonald p. 52 4-1
10
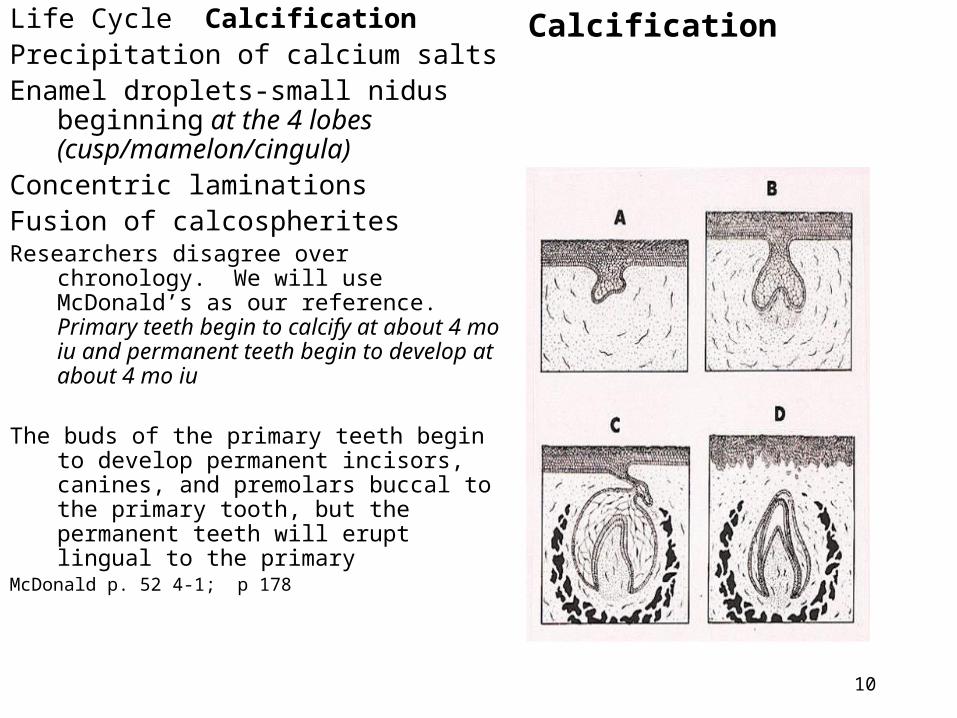
Life Cycle CalcificationPrecipitation of calcium saltsEnamel droplets-small nidus
beginning at the 4 lobes (cusp/mamelon/cingula)
Concentric laminationsFusion of calcospheritesResearchers disagree over chronology.
We will use McDonald’s as our reference. Primary teeth begin to calcify at about 4 mo iu and permanent teeth begin to develop at about 4 mo iu
The buds of the primary teeth begin to develop permanent incisors, canines, and premolars buccal to the primary tooth, but the permanent teeth will erupt lingual to the primary
McDonald p. 52 4-1; p 178
Calcification

11
Primary Calcification
Primary hard tissue formation begins (weeks in utero):
Centrals— 14 13 to 16 w iu
1st molars— 15 ½ 14 ½-17 w iu
Laterals—16 14 2/3 to 16 ½ w iu
Mx canines– 17 15-18 w iu
Md canines—17 16-17 w iu
Md 2nd molars—18 16-23 ½ w iu
Mx 2nd molars—19 16-23 ½ w iuAll 20 primary teeth begin to calcify
by 4-6 mo iu and take 10 months for completion.
McDonald 52 4-1

12
Primary Calcification is complete after birth:
Mx central 1.5 moMx lateral Md central 2.5 moMd lateral 3 moMx 1st molars 5.5
moMx 1st molars 6
moCanines 9 moMd 2nd molars 10 moMx 2nd molars 11 moResearchers disagree over
chronology. We will use McDonald’s as our reference.
McDonald p.52 4-1

13
Bud represents the beginning of formation of the dental lamina and special dental germs
Overview of Disturbances in Bud stage:
Congenital absence of tooth/teeth lack of initiation
Supernumerary teeth—continued budding
McDonald-p.667 shows a
Mesiodens-midline supernumerary
Odontoma (enamel/dentin tumor) p107 (often with odontoma-dysphagia syndrome)
McDonald 667 27-54McDonald 107 7-5
Developmental Disturbances

14
Odontoma or Odontogenic tumorAbnormal proliferationAsymptomaticOften with unerupted tooth/cystOften with odontoma-dysphasia syn.Compound-miniature teeth
anterior maxilla occurrence-14.8 yo
(mean)Complex-amorphous/opaque
posterior mandible occurrence-20.3 yo (mean) affects both genders
equallyTX: enucleate rarely recursResearchers disagree over the
distinctions compound/complexMcDonald p 107 7-5

15
Cap Stage--cell multiplication
Overview of Problems:Congenially missing teeth and
Supernumerary teeth may also occur in cap stage
Odontoma which replaces the normal tooth p107
Extra cusps and roots
Suppression of cusps and roots
Fusion (2 teeth unite into 1 tooth)
Gemination (bifid crown)
Epithelial rests cyst
McDonald 108 7-7 Fusion
McDonald 109 7-8 Gemination

16
Cap disturbancesFusion—2 teeth unite into 1 tooth so
there are separate pulp canals & chambers
anterior location (generally) missing succedaneous teeth (often) family tendency primary or permanent teeth
Differential diagnosis—count teeth TX: may need restoration along line of fusion
McDonald p108 7-7

17
Cap DistrubancesGemination—bifud crown Single tooth tries to divide Wide crown Familial tendency Primary or Permanent teeth Differential from fusion-count teeth TX: Recontour mesiodistal width
If dentin is exposed-restore If pulp is exposed-RCT
Mcdonald 109 7-8

18
Bell—shape and cell finalization Overview of Disturbances:Abnormal forms and sizes:
Dens invaginatisDens evaginatus
Microdontia (such as peg lateral) Macrodontia Taurodontism Dilaceration Hutchinson’s incisors and Mulberry
molarsAmelogenesis Imperfecta

19
Bell DisturbancesDens Invaginatus Dens in Dente—
Lingual invagination of enamelDeep lingual pits;
foramen cecum--some to pulpMaxillary perm. Laterals (7.7%)Frequent (1/77 Caucasians)Familial tendency (autosomal dominant)
Early diagnosis—early TXTX: apply sealant/restoration
Dens in MX lateral McDonald 110 7-10

20
Bell DisturbancesDens Evaginatus
Lingual evagination of toothCone can interfere with eruption
occlusionCones contain pulp hornsTalon cusp—resembles an eagle claw—the term is reserved for anterior teethTX: may need to reduce
interference may require RCT

21
Bell Disturbances Taurodontism Resemble cattle (taurus) teethElongated pulp chamberShort roots 2.5% occurrence in CaucasiansMay occur with syndromes: Otodental dysplasia X-chromosome aneuploidies
(change in number of X’s)Tricho-dento-osseous syndrome
(curly hair, dense bone)Late invagination-Hertwig’s
epithelial root sheath (HERS)
Clinically significant in a RCT
McDonald 123 7-26

22
Bell DisturbancesDilacerationA sharp bend or
angulation of the root
• Result from trauma during tooth development
Clinical significance:• Can complicate tooth
extraction
McDonald 482 21-34

23
Infections during BellCongenital Syphilis—child is
infected iu or while passing through birth canal.
Rare in US due to early detection and treatment
Hutchinson Incisors – result of congenital syphilis
– “screwdriver-shaped” permanent incisors

24
Infections during the Bell stag
Mulberry molars Congenital Syphilis
From - Marquette University School of Dentistry
- Oral & Maxiollofacial Pathology website

25
Apposition--matrix formation of ameloblasts and odontoblasts
Overview of Disturbances:– Enamel hypoplasia
defect in enamel matrix formation
Enamel Hypoplasia from trauma
Enamel Hypoplasia from infection
in apposition stage:
Hutchinson Incisor
Mulberry molar
Turner tooth
Amelogenesis Imperfecta Type 2– Hypoplasia of dentin

26
Enamel hypoplasia (defect in matrix formation) is
Clinically: enamel—hard/thin
pitted/irregular surface
esthetic problems
sensitive teeth
yellow or brown
permanent and/or primary teeth

27
Some causes of enamel hypoplasia:Local infection (localized problem)Local trauma (localized problem)Systemic diseases/conditions, such as
Rubella embryopathyCongenital syphilisHypoparathyroidismGrowth problems 0-6 mo
X-ray radiation- can also effect dentinFluoride; Chronic pediatric lead poisoningNutritional deficiencies – Vitamins A, C , Ca and PCleft lip and palate repair – permanent teeth more
likely to be damaged

28
Enamel hypoplasia may be associated with
• Brain injury
• Neurologic defects
• Nephrotic syndrome
• Allergies

29
Apposition disturbancesEnamel hypoplasia from
infectionsHutchinson Incisor –
result of congenital syphilis
– “screwdriver-shaped” permanent incisors

30
Apposition Disturbances
Enamel hypoplasia from infection
Mulberry molars Congenital Syphilis
From - Marquette University School of Dentistry
- Oral & Maxiollofacial Pathology website

31
Appostion Disturbances: Enamel Hypoplasia Due to local Infection or local Trauma—Turner’s tooth
Infections/caries in primary teeth may malform successors
McDonald 118 7-18

32
Appostion Disturbances: The Location of the localized enamel defect is used to
calculate the timing of the infection/trauma/disease/insult.
At 4-5 years permanent centrals have completed calcification

33
Apposition Disturbances: Enamel hypoplasia from radiation therapy which caused stunted of root
development McDonald p119 7-20

34
Apposition Disturbances: Enamel Hypoplasia resulting from Rubella Embryopathy—
McDonald p 120 7-22
35
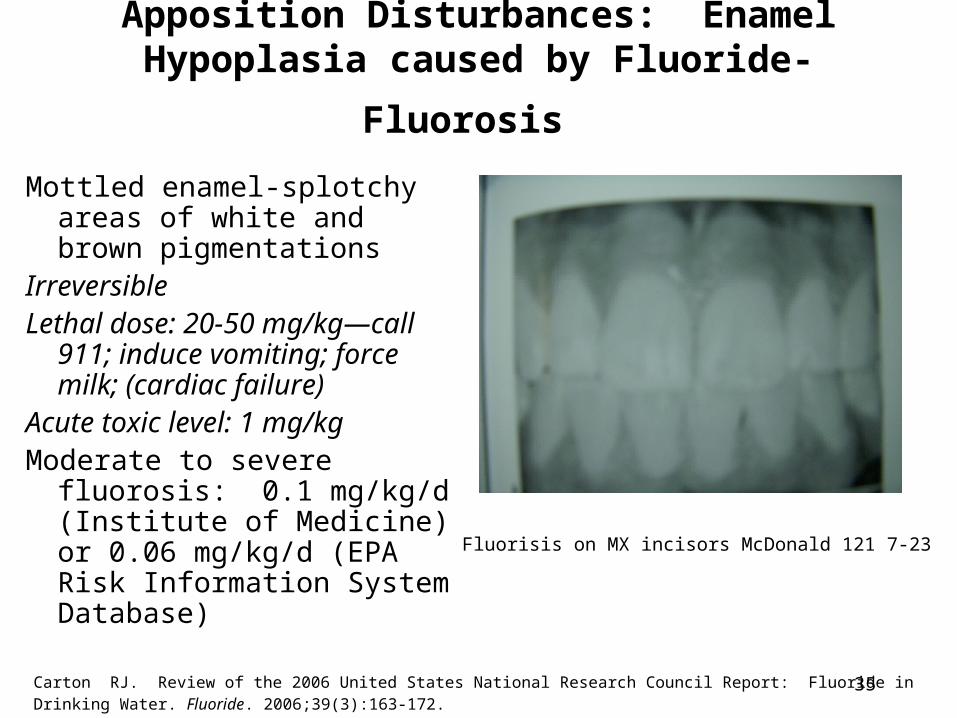
Apposition Disturbances: Enamel Hypoplasia
caused by Fluoride- Fluorosis Mottled enamel-splotchy areas
of white and brown pigmentations
Irreversible Lethal dose: 20-50 mg/kg—
call 911; induce vomiting; force milk; (cardiac failure)
Acute toxic level: 1 mg/kgModerate to severe fluorosis:
0.1 mg/kg/d (Institute of Medicine) or 0.06 mg/kg/d (EPA Risk Information System Database)
Fluorisis on MX incisors McDonald 121 7-23
Carton RJ. Review of the 2006 United States National Research Council Report: Fluoride in Drinking Water. Fluoride. 2006;39(3):163-172.

36
American Academy of Pediatric Dentistry Guideline, revised 2008
• Asses all sources of fluoride: water from home, day care, school; sodas, juices, formula, foods, toothpaste
• Assess caries risk• Recommend: smear of Fluoridated toothpaste
under 2yo; pea-size 2-5yo.• Supplementation schedule for <0.3ppm:
– 0-6m-0; 6m-3y-.25mg; 3-6y-.5 mg 6-16y-1mg
• Supplementation schedule for .3-.6ppm: – 0-6m-0; 6m-3y-0; 3-6y-.25mg 6-16y-.5mg

37
Treatment of defective or carious hypoplastic teeth:
• Confine restoration to involved area • Use composite resin or glass
ionomer in minor defects or caries• Larger defects/carious areas may
require amalgams or Stainless Steel Crowns

38
Treatment of hypoplastic teeth with esthetic problems
• Enamel microabrasion to remove superficial enamel discoloration (less than 250 μm depth)
• Vital tooth bleaching

39
Calcification– precipitation of hydroxyapatite crystallites
[Ca10(PO4)6OH2] in matrix
Overview of Disturbances:Enamel Hypocalcification
A defect in enamel calcification and/or maturation
Pre-eruptive intracoronal resporption
Concrescence
Tetracycline stain
Interglobular dentin
Amelogenesis Imperfecta Type III

40
Calcification disturbances: Pre-eruptive
intracoronal resorption or pre-eruptive caries • Defect in enamel formation• Results in connective tissue
growth into the defect• Not consdered classical
caries involving microorganisms and acids
• Infrequent (<10%)• Examine developing • teeth on radiographs for
such defects.
McDonald 121 7-24

41
Calcification Disturbances: Concrescence
Fusion of two teeth by cementum only
Clinical significance: Important to recognize it and not
extract two teeth when intending to extract one
Considered to be caused by trauma
From “Contemporary oral and maxillofacial pathology” 1997

Next week—continuation of enamel and dentin defects
![[PPT]PowerPoint Presentation - Texas and New Mexico … Pediatric... · Web viewPowerPoint Presentation Last modified by medelling ...](https://static.fdocuments.net/doc/165x107/5ab3cad37f8b9a284c8eb5b5/pptpowerpoint-presentation-texas-and-new-mexico-pediatricweb-viewpowerpoint.jpg)

![[PPT]Pediatric Emergencies II - APLS: The Pediatric … · Web viewTitle Pediatric Emergencies II Author Sunil Bhopale Last modified by dawnp Created Date 1/8/1999 11:04:59 PM Document](https://static.fdocuments.net/doc/165x107/5b2373d27f8b9ac1328b652b/pptpediatric-emergencies-ii-apls-the-pediatric-web-viewtitle-pediatric.jpg)














![[PPT]Pediatric Airway Managementssu.ac.ir/.../rah_hawaei/pediatric_airway_management.ppt · Web viewCauses of Difficult Airway Congenital Anomalies Tumors Infection Musculoskeletal](https://static.fdocuments.net/doc/165x107/5b95a15d09d3f2214e8d079d/pptpediatric-airway-web-viewcauses-of-difficult-airway-congenital-anomalies.jpg)
