Lecture 1 14 th March, 11 Toxicology Introduction to Toxicology.
140
Lecture 1 Lecture 1 14 14 th th March, 11 March, 11 Toxicology Toxicology Introduction to Introduction to Toxicology Toxicology
-
Upload
dwayne-lewis -
Category
Documents
-
view
230 -
download
0
Transcript of Lecture 1 14 th March, 11 Toxicology Introduction to Toxicology.

Lecture 1 14Lecture 1 14thth March, March, 1111
ToxicologyToxicology
Introduction to Introduction to ToxicologyToxicology

What is toxicologyWhat is toxicology
•Toxicology is the study of Toxicology is the study of the adverse effects of the adverse effects of chemical or physical chemical or physical agents on living agents on living organisms.organisms.

Risk assessmentRisk assessment
•Quantitative estimate of the Quantitative estimate of the potential effects on human potential effects on human health and environmental health and environmental significance of various types significance of various types of chemical exposures (e.g., of chemical exposures (e.g., pesticide residues on food, pesticide residues on food, contaminants in drinking contaminants in drinking water).water).

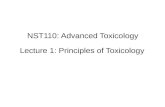
Graphical representation of the interconnections between different areas of toxicology.

Different areas of toxicologyDifferent areas of toxicology
1.1.Mechanistic ToxicologistMechanistic Toxicologist
• Identifying and understanding the Identifying and understanding the cellular, biochemical, and molecular cellular, biochemical, and molecular mechanisms by which chemicals mechanisms by which chemicals exert toxic effects on living organismsexert toxic effects on living organisms
• Mechanistic data (Mechanistic data (saccharinsaccharin to cause to cause bladder cancer, thalidomide in bladder cancer, thalidomide in leprosy and leprosy and AIDSAIDS, , 6-6-mercaptopurinemercaptopurine in leukemias) in leukemias)
• Relative toxic potential of Relative toxic potential of organophosphate insecticidesorganophosphate insecticides

2. Descriptive toxicologist2. Descriptive toxicologist
• concerned directly with toxicity concerned directly with toxicity testing, which provides information testing, which provides information for safety evaluation and regulatory for safety evaluation and regulatory requirements.requirements.
• Risk posed by a company chemical Risk posed by a company chemical (insecticides, herbicides, solvents) to (insecticides, herbicides, solvents) to humans but also to animalshumans but also to animals
• Omics technologiesOmics technologies

3. Regulatory toxicologists3. Regulatory toxicologists• Responsibility for deciding, on the basis of data Responsibility for deciding, on the basis of data
provided by descriptive and mechanistic provided by descriptive and mechanistic toxicologists, whether a drug poses a toxicologists, whether a drug poses a sufficiently low risk to be marketed for a stated sufficiently low risk to be marketed for a stated purpose or subsequent human or purpose or subsequent human or environmental exposure resulting from its use.environmental exposure resulting from its use.
• Food and Drug AdministrationFood and Drug Administration
• Federal Food, Drug and Cosmetic ActFederal Food, Drug and Cosmetic Act
• Environmental Protection AgencyEnvironmental Protection Agency
• Federal Insecticide, Fungicide and Rodenticide ActFederal Insecticide, Fungicide and Rodenticide Act

General characteristics General characteristics of toxic responseof toxic response
• LD 50LD 50
• Microgram dosesMicrogram doses
• Physical state (gas, dust, liquids)Physical state (gas, dust, liquids)
• chemical structure (aromatic amines, chemical structure (aromatic amines, halogenated hydrocarbons)halogenated hydrocarbons)
• Poisoning potential (slight………extreme)Poisoning potential (slight………extreme)
• MOA (alkylating agent, cholinesterase MOA (alkylating agent, cholinesterase inhibitors)inhibitors)

Lecture 2 14Lecture 2 14thth March, March, 1111
ToxicologyToxicology
Principles of ToxicologyPrinciples of Toxicology

Spectrum of undesired Spectrum of undesired effectseffects
• Some effects deleterious others notSome effects deleterious others not
• Some side effects……others indicationSome side effects……others indication
• Diphenhydramine (1Diphenhydramine (1stst generation generation antihistamine”benadryl”) effective antihistamine”benadryl”) effective against allergies but produces CNS against allergies but produces CNS drwsiness as it crosses BBB. Often drwsiness as it crosses BBB. Often used as sleep remedy e.g. tylenol PMused as sleep remedy e.g. tylenol PM
• Sometimes undesirable effects also Sometimes undesirable effects also reffered to as deleterious effectsreffered to as deleterious effects

Allergic reactionsAllergic reactions• For given allergic individuals the For given allergic individuals the
allergic reaction are dose dependentallergic reaction are dose dependent
• Pattern of allergic response (in humans Pattern of allergic response (in humans skin and eyes and in guinae pigs skin and eyes and in guinae pigs bronchial constriction)bronchial constriction)
• Anaphylactic shockAnaphylactic shock
• Hapten-protein complex required time Hapten-protein complex required time for eliciting the formation of antibodiesfor eliciting the formation of antibodies
• Time dependentTime dependent

• IdiosyncraticIdiosyncratic
• Immediate vs delayed toxicityImmediate vs delayed toxicity
• Local vs systemicLocal vs systemic
• Reversible vs irreversibleReversible vs irreversible

Idiosyncratic reactionsIdiosyncratic reactions
• Chemical idiosyncrasy refers to a Chemical idiosyncrasy refers to a genetically determined abnormal genetically determined abnormal reactivity to a chemicalreactivity to a chemical
• A classic example of an idiosyncratic A classic example of an idiosyncratic reaction is provided by patients who reaction is provided by patients who exhibit prolonged muscular exhibit prolonged muscular relaxation and apnea (inability to relaxation and apnea (inability to breathe) lasting several hours after a breathe) lasting several hours after a standard dose of succinylcholine.standard dose of succinylcholine.

• Patients exhibiting this reaction have Patients exhibiting this reaction have genetic polymorphism in the gene for genetic polymorphism in the gene for the enzyme butyrylcholinesterasethe enzyme butyrylcholinesterase

Immediate vs delayed Immediate vs delayed txicitytxicity• Immediate toxic effects can be defined as Immediate toxic effects can be defined as
those that occur or develop rapidly after a those that occur or develop rapidly after a single administration of a substance, single administration of a substance, whereas delayed toxic effects are those whereas delayed toxic effects are those that occur after the lapse of some time.that occur after the lapse of some time.
• Carcinogenic effects of chemicals usually Carcinogenic effects of chemicals usually have a long latency period, often 20 to 30 have a long latency period, often 20 to 30 years after the initial exposure, before years after the initial exposure, before tumors are observed in humans.tumors are observed in humans.

• e.g e.g DiethylstilbestrolDiethylstilbestrol (DES) during (DES) during pregnancy have a greatly increased pregnancy have a greatly increased risk of developing vaginal cancer, but risk of developing vaginal cancer, but not other types of cancer, in young not other types of cancer, in young adulthood, some 20 to 30 years after adulthood, some 20 to 30 years after their in utero exposure to DEStheir in utero exposure to DES

Reversible vs irreversible Reversible vs irreversible toxic effectstoxic effects
• Some toxic effects of chemicals are Some toxic effects of chemicals are reversible, and others are reversible, and others are irreversible.irreversible.
• For example tissue injury of liver nad For example tissue injury of liver nad tissue injury of CNS tissue injury of CNS

Local vs systemic effectsLocal vs systemic effects
• Chlorine gas reacts with lung tissue Chlorine gas reacts with lung tissue at the site of contact, causing at the site of contact, causing damage and swelling of the tissue, damage and swelling of the tissue, with possibly fatal consequences, with possibly fatal consequences, even though very little of the even though very little of the chemical is absorbed into the chemical is absorbed into the bloodstream. (local)bloodstream. (local)

• Tetraethyl lead produces effects on Tetraethyl lead produces effects on skin at the site of absorption and skin at the site of absorption and then is transported systemically to then is transported systemically to produce its typical effects on the CNS produce its typical effects on the CNS and other organs.and other organs.

Lecture 3 18Lecture 3 18thth March, March, 1111
ToxicologyToxicology
Principles of ToxicologyPrinciples of Toxicology

Interactions of chemicalsInteractions of chemicals
• Additive (2+3=5)Additive (2+3=5)
• Synergistic (2+2=20) e.g. carbon Synergistic (2+2=20) e.g. carbon tetrachloride + ethanol leads to tetrachloride + ethanol leads to hepatotoxicityhepatotoxicity
• Potentiative (0+2=10) e.g. Potentiative (0+2=10) e.g. isopropranolol + ethanolisopropranolol + ethanol
• Antagonistic (4+6=8) e.g. Antagonistic (4+6=8) e.g. barbiturates and vasopressorbarbiturates and vasopressor

ToleranceTolerance
• State of decreased responsiveness to State of decreased responsiveness to a toxic effect of a chemical resulting a toxic effect of a chemical resulting from prior exposure to that chemical from prior exposure to that chemical or to a structurally related chemical. or to a structurally related chemical. E.g. carbon tetrachloride and E.g. carbon tetrachloride and cadmium, penicillins and cadmium, penicillins and cephalosporinscephalosporins

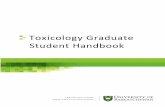
Potential stages in the development of toxicity after chemical exposure.

Potential stages in the Potential stages in the development of toxicitydevelopment of toxicity
• Puffer fish poison (tetrodotoxin) Puffer fish poison (tetrodotoxin) ingestion ingestion and reaches the voltage and reaches the voltage gated Na+ channels of motor neurons, gated Na+ channels of motor neurons, interactioninteraction with target ions, result in with target ions, result in blockade of channels, blockade of channels, inhibitioninhibition of the of the activity of motor neurons & ultimately activity of motor neurons & ultimately skeletal muscle paralysis (no repair for skeletal muscle paralysis (no repair for such toxicity).such toxicity).

• 2,4-dinitrophenol’s 2,4-dinitrophenol’s entranceentrance in in mitochondrial matrix space, mitochondrial matrix space, collapsingcollapsing directly outward across directly outward across the inner membrane the inner membrane causingcausing mitochondrial dysfunction and mitochondrial dysfunction and manifestedmanifested by hyperthermia and by hyperthermia and seizuresseizures

The process of toxicant delivery is the first step in the development of toxicity

Delivery of toxicantDelivery of toxicant• Gastrointestinal transporters Gastrointestinal transporters
(monocarboxylate transporters for (monocarboxylate transporters for salicylates, valporates and peptide salicylates, valporates and peptide transporters for transporters for ββ-lactam antibiotics -lactam antibiotics and ACE inhibitors)and ACE inhibitors)
• Rate of absorptionRate of absorption
• Conc.of chemicalConc.of chemical
• Thickness of stratum corneumThickness of stratum corneum
• Physiochemical properties e.g. lipid Physiochemical properties e.g. lipid solubilitysolubility
• Epithelial circulationEpithelial circulation

• First pass effect e.g. oxidation of First pass effect e.g. oxidation of ethanol by ethanol by alcohol dehydrogenasealcohol dehydrogenase in in gastric mucosa and enterohepatic gastric mucosa and enterohepatic circulation of cyclosporine by circulation of cyclosporine by P-P-glycoprotein transporter glycoprotein transporter and and hydroxylation by CYP450.hydroxylation by CYP450.
• Distribution towards target Distribution towards target mediatedmediated by transporters e.g. by transporters e.g. monocarboxylate transporters, monocarboxylate transporters, peptide transporters, P-glycoprotein peptide transporters, P-glycoprotein transporters, dopaminergic transporters, dopaminergic transporters.transporters.

• Distribution away from target is Distribution away from target is facilitated by facilitated by BBBBBB, binding to plasma , binding to plasma proteins, distribution in storage proteins, distribution in storage tissues like tissues like leadlead in bone and of in bone and of lipophilic drugs lipophilic drugs in adipose tissuein adipose tissue

AbsorptionAbsorption• Gastrointestinal transporters Gastrointestinal transporters
(monocarboxylate transporters for (monocarboxylate transporters for salicylates, valporates and peptide salicylates, valporates and peptide transporters for transporters for ββ-lactam antibiotics -lactam antibiotics and ACE inhibitors)and ACE inhibitors)
• Rate of absorption and Conc.of Rate of absorption and Conc.of chemicalchemical
• Thickness of stratum corneumThickness of stratum corneum
• Physiochemical properties e.g. lipid Physiochemical properties e.g. lipid solubilitysolubility
• Epithelial circulationEpithelial circulation

Pre-systemic EliminationPre-systemic Elimination
• First pass effect e.g. oxidation of First pass effect e.g. oxidation of ethanol by ethanol by alcohol dehydrogenasealcohol dehydrogenase in in gastric mucosa and enterohepatic gastric mucosa and enterohepatic circulation of cyclosporine by circulation of cyclosporine by P-P-glycoprotein transporter glycoprotein transporter and and hydroxylation by CYP450.hydroxylation by CYP450.

Distribution towards and Distribution towards and away from Targetaway from Target
• Distribution towards target Distribution towards target mediatedmediated by transporters e.g. by transporters e.g. monocarboxylate transporters, monocarboxylate transporters, peptide transporters, P-glycoprotein peptide transporters, P-glycoprotein transporters, dopaminergic transporters, dopaminergic transporters.transporters.
• Distribution away from target is Distribution away from target is facilitated by facilitated by BBBBBB, binding to plasma , binding to plasma proteins, distribution in storage proteins, distribution in storage tissues like tissues like leadlead in bone and of in bone and of lipophilic drugs lipophilic drugs in adipose tissuein adipose tissue

ExcretionExcretion• Excretion of drugs from blood to Excretion of drugs from blood to
external environmentexternal environment
• Renal transporters SLC family for Renal transporters SLC family for diffusion of ions and smaller diffusion of ions and smaller molecule < 300 Damolecule < 300 Da
• Excretion on the basis of lipid Excretion on the basis of lipid contents and aciditycontents and acidity
• Highly hydrophillic, organic acids and Highly hydrophillic, organic acids and bases efficiently removed by liver bases efficiently removed by liver and kidneyand kidney

• Highly non volatile and highly Highly non volatile and highly lipophilic eliminate slowly and tend lipophilic eliminate slowly and tend to accumulateto accumulate
• Gases and volatile liquids liquids Gases and volatile liquids liquids diffuse from pulmonary capillaries diffuse from pulmonary capillaries into the alveoli and are exhaledinto the alveoli and are exhaled

ReabsorptionReabsorption
•Toxicants delivered into the Toxicants delivered into the renal tubules may diffuse back renal tubules may diffuse back across the tubular cells into the across the tubular cells into the peritubular capillaries.peritubular capillaries.
•This process is facilitated by This process is facilitated by tubular fluid reabsorption, which tubular fluid reabsorption, which increases the intratubular increases the intratubular concentration as well as the concentration as well as the residence time of the chemical residence time of the chemical by slowing urine flow.by slowing urine flow.

• For organic acids and bases, diffusion is For organic acids and bases, diffusion is inversely related to the extent of inversely related to the extent of ionization,because the nonionized ionization,because the nonionized molecule is more lipid-soluble.molecule is more lipid-soluble.
• The ionization of weak organic acids, The ionization of weak organic acids, such as such as salicylic acid salicylic acid and and phenobarbitalphenobarbital, , and bases, such as and bases, such as amphetamineamphetamine, , procainamideprocainamide, and , and quinidinequinidine, is strongly , is strongly pH-dependent in the physiologic range.pH-dependent in the physiologic range.

ToxicationToxication
• A number of xenobiotics (e.g., A number of xenobiotics (e.g., strong strong acids and bases, nicotine, acids and bases, nicotine, aminoglycosides, ethylene oxide, aminoglycosides, ethylene oxide, methylisocyanate,heavy-metal ions methylisocyanate,heavy-metal ions )) are directly toxic, whereas the are directly toxic, whereas the toxicity of others is due largely to toxicity of others is due largely to metabolites.metabolites.
• Biotransformation to harmful Biotransformation to harmful products is called toxication or products is called toxication or metabolic activation.metabolic activation.

• With some xenobiotics, toxication confers With some xenobiotics, toxication confers physicochemical properties that physicochemical properties that adversely alter the microenvironment of adversely alter the microenvironment of biological processes or structures.biological processes or structures.
• For example, For example, oxalic acid oxalic acid formed from formed from ethylene glycol ethylene glycol may cause acidosis and may cause acidosis and hypocalcaemia as well as obstruction of hypocalcaemia as well as obstruction of renal tubules by precipitation as calcium renal tubules by precipitation as calcium oxalate.oxalate.

Reaction of the ultimate toxicant with the target molecule: the second step in the development of toxicity

Alteration of the regulatory or maintenance function of the cell: third first step in the development of toxicity

Lecture 4 21Lecture 4 21stst March, March, 1111
ToxicologyToxicology
Adverse Drug ReactionsAdverse Drug Reactions

Adverse Drug ReactionsAdverse Drug Reactions
•ADR’s (definition and statistical ADR’s (definition and statistical figures)figures)
•Classification of ADR’sClassification of ADR’s
•Type A and Type B reactions Type A and Type B reactions (characteristics and types)(characteristics and types)
•Anaphylaxis (signs and Anaphylaxis (signs and symptoms, diagnosis, symptoms, diagnosis, management)management)

ToxicologyToxicology
antidote antidote : ATROPINE: ATROPINE
Lecture 5 25Lecture 5 25thth March, March, 1111

ACTHACTH•Neurotransmitter in both the Neurotransmitter in both the
peripheral nervous system (PNS) peripheral nervous system (PNS) and central nervous system (CNS)and central nervous system (CNS)
•Ester of acetic acid and choline with Ester of acetic acid and choline with chemical formula CHchemical formula CH33COOCHCOOCH22CHCH22NN++
(CH(CH33))33
•Bethanechol, Melathione,Nicotine, Bethanechol, Melathione,Nicotine, Pilocarpine, SuxamethoniumPilocarpine, Suxamethonium

ACTHACTH
• In the peripheral nervous system, In the peripheral nervous system, acetylcholine activates muscles, and acetylcholine activates muscles, and is a major neurotransmitter in the is a major neurotransmitter in the autonomic nervous system.autonomic nervous system.
• In the central nervous system, In the central nervous system, acetylcholine and the associated acetylcholine and the associated neurons form a neurotransmitter neurons form a neurotransmitter system, the cholinergic system, system, the cholinergic system, which tends to cause anti-excitatory which tends to cause anti-excitatory actions.actions.

AtropineAtropine•Therapeutic categoryTherapeutic category
•Dosage formsDosage forms
•Available brandsAvailable brands
•Mechanism of actionMechanism of actionBlocks the action of ACTH at Blocks the action of ACTH at
parasympathetic sites in smooth parasympathetic sites in smooth muscles, secretory glands and muscles, secretory glands and heart. Increases cardiac output, heart. Increases cardiac output, dries secretions, antagonizes dries secretions, antagonizes histamine.histamine.

• UseUse
• DosingDosingOrganophosphate pesticides:Organophosphate pesticides:
I/V 0.02-0.05 mg/kg every 10 to 20 I/V 0.02-0.05 mg/kg every 10 to 20 minutes until dry flushed skin, minutes until dry flushed skin, tachycardia and mydriasis are observed tachycardia and mydriasis are observed then every 1-4 hours for at least 24 hoursthen every 1-4 hours for at least 24 hours
Bradycardia:Bradycardia:
I/V maximum total dose of 1 mg in children I/V maximum total dose of 1 mg in children and 2 mg in adolescents in repeated and 2 mg in adolescents in repeated doses.doses.

•Monitoring parametersMonitoring parameters
Heart rate, blood pressure, pulse, Heart rate, blood pressure, pulse, mental status, cardiac monitoringmental status, cardiac monitoring
•Adverse reactions Adverse reactions
(palpitation, drowsiness, (palpitation, drowsiness, hallucinations, urticaria, loss of hallucinations, urticaria, loss of taste, NVD, urinary retention, taste, NVD, urinary retention, blurred vision, pulmonary blurred vision, pulmonary edema, )edema, )

• InteractionsInteractions
with drugs having anti cholinrgic with drugs having anti cholinrgic activities( phenothiazines and activities( phenothiazines and TCA’s)TCA’s)
•Overdosage treatmentOverdosage treatment
Physostigmine 1-2 mg (children: 0.5 Physostigmine 1-2 mg (children: 0.5 mg or 0.02 mg/kg) S/C or slow I/Vmg or 0.02 mg/kg) S/C or slow I/V

ToxicologyToxicology
Antidote Antidote : DEFEROXAMINE: DEFEROXAMINE
Lecture 6 28th March, Lecture 6 28th March, 1111

Iron poisoningIron poisoning
•Iron overload that leads to Iron overload that leads to ulceration in stomach then ulceration in stomach then brain and liver toxicity brain and liver toxicity following metabolic acidosis.following metabolic acidosis.
•Treated by deferoxamine and Treated by deferoxamine and then dialysisthen dialysis

Aluminum poisoningAluminum poisoning
• Aluminum sources leads to colic, Aluminum sources leads to colic, rickets, GI disturbances, poor Ca rickets, GI disturbances, poor Ca metabolism, extreme nervousness, metabolism, extreme nervousness, anemia, headache, decreased liver anemia, headache, decreased liver and kidney function, forgetfulness, and kidney function, forgetfulness, speech disturbances, and memory speech disturbances, and memory loss, softening of the bones, and loss, softening of the bones, and weak, aching musclesweak, aching muscles
• Treated by chelation therapyTreated by chelation therapy

DeferoxamineDeferoxamine• Source (bacterial siderophore Source (bacterial siderophore
produced by produced by Streptomyces pilosus). Streptomyces pilosus). Siderphores (iron carriers) small, Siderphores (iron carriers) small, high-affinity iron chelating high-affinity iron chelating compounds secreted by compounds secreted by microorganisms such as bacteria, microorganisms such as bacteria, fungi and grasses.fungi and grasses.
• Therapeutic categoryTherapeutic category
• Dosage formsDosage forms
• Available brandsAvailable brands

• MOAMOA
Complexes with trivalent ions (ferric Complexes with trivalent ions (ferric ions) to form ferrioxamine, which is ions) to form ferrioxamine, which is removed by the kidneysremoved by the kidneys
• UseUse
Acute iron intoxication, diagnostic test Acute iron intoxication, diagnostic test for iron overload, investigational use for iron overload, investigational use in the treatment of aluminum in the treatment of aluminum accumulation in renal failure accumulation in renal failure

•DosingDosing
I/M 90 mg/kg/dose every 8 hrs; I/M 90 mg/kg/dose every 8 hrs; maximum dose 6 g/daymaximum dose 6 g/day
OROR
I/V 15 mg/kg/hr; maximum 6 I/V 15 mg/kg/hr; maximum 6 gm/daygm/day
•Monitoring parametersMonitoring parameters
Serum ferritin, body weight. , B.P., Serum ferritin, body weight. , B.P., ophthalmologic examsophthalmologic exams

• Adverse ReactionsAdverse Reactions
Hypotension, seizures, dementia, Hypotension, seizures, dementia, urticaria, dysuria, thrombocytopenia, urticaria, dysuria, thrombocytopenia, leukopenia, anaphylaxisleukopenia, anaphylaxis
• Drug interactionsDrug interactions
Vitamin C: concomitant usage can Vitamin C: concomitant usage can leads to cardiac impairment leads to cardiac impairment
• Over dosage treatmentOver dosage treatment
Symptomatic and supportive, dialysisSymptomatic and supportive, dialysis

ToxicologyToxicology
Antidote Antidote : FLUMAZENIL: FLUMAZENIL
Lecture 7 1st April, Lecture 7 1st April, 1111

Points to refresh Points to refresh . . . . . . . . . . . . . . . . . .
•NeurotransmitterNeurotransmitter
•SynapseSynapse
•GABA receptorsGABA receptors
•Hyper polarization (-ve Hyper polarization (-ve membrane potential )membrane potential )

• BenzodiazepinesBenzodiazepines
BZD enhance the effect of the BZD enhance the effect of the neurotransmitter (GABA), which neurotransmitter (GABA), which results in sedative, hypnotic (sleep-results in sedative, hypnotic (sleep-inducing), anxiolytic (anti-anxiety), inducing), anxiolytic (anti-anxiety), anticonvulsant, muscle relaxant and anticonvulsant, muscle relaxant and amnesic action.amnesic action.
• Examples of BZDExamples of BZD
Diazepam, alprazolam, Lorazepam Diazepam, alprazolam, Lorazepam

FlumazenilFlumazenil
•Therapeutic category:Therapeutic category:
Antidote, BZD antagonistAntidote, BZD antagonist
•Dosage forms:Dosage forms:
Injection: 0.1mg/mlInjection: 0.1mg/ml
Solution : 10 mlSolution : 10 ml
•Available brands:Available brands:
Inj. Anexate 0.1 mg/ml (10 ml Inj. Anexate 0.1 mg/ml (10 ml ampoule)ampoule)

FlumazenilFlumazenil
•Mode of Action:Mode of Action:
Antagonizes the effects of BZD on Antagonizes the effects of BZD on the GABA/BZD receptor complex.the GABA/BZD receptor complex.
•Uses:Uses:
BZD antagonist, reverse sedative BZD antagonist, reverse sedative effects of BZD, used in general effects of BZD, used in general anesthesia or conscious sedationanesthesia or conscious sedation

FlumazenilFlumazenil
• Dosing:Dosing:
Management of BZD overdose:Management of BZD overdose:
Initial dose: 0.01 mg/kg (max. Initial dose: 0.01 mg/kg (max. dose: 0.2 mg) with repeat doses dose: 0.2 mg) with repeat doses of 0.01 mg/kg (max. dose: 0.2 of 0.01 mg/kg (max. dose: 0.2 mg) given every minute to a mg) given every minute to a maximal total cumulative dose of maximal total cumulative dose of 1 mg.1 mg.

FlumazenilFlumazenil
•Monitoring parameters:Monitoring parameters:
Level of consciousness and re- Level of consciousness and re- sedationsedation
•Drug interactions:Drug interactions:
Use with caution in mixed drug Use with caution in mixed drug overdose; especially with overdose; especially with TCA’sTCA’s

FlumazenilFlumazenil
•Over dosage treatment:Over dosage treatment:Maintain airway/ support Maintain airway/ support
ventilation as necessaryventilation as necessaryAdminister I.V fluidsAdminister I.V fluidsFor seizures:For seizures:
Diazepam, PhenytoinDiazepam, Phenytoin

ToxicologyToxicology
Antidote Antidote : Penicillamine: Penicillamine
Lecture 8 4th April, 11Lecture 8 4th April, 11

PenicillaminePenicillamine
•Therapeutic category:Therapeutic category:
Antidote for copper and lead Antidote for copper and lead toxicitytoxicity
Chelating agentChelating agent
•Dosage forms:Dosage forms:
Capsule: 250 mg ; Tablet : 250 mgCapsule: 250 mg ; Tablet : 250 mg
Solution : 10 mlSolution : 10 ml
•Available brands:Available brands:
Vistamine Tab 250 mgVistamine Tab 250 mg

PenicillaminePenicillamine•Mode of Action:Mode of Action:
Chelates with lead, copper, mercury, Chelates with lead, copper, mercury, iron and other heavy metals to iron and other heavy metals to form stable, soluble complexes form stable, soluble complexes that are ecreted in urine.that are ecreted in urine.
•Uses:Uses:
Cystinuria, Wilson’s disease, lead Cystinuria, Wilson’s disease, lead poisoning and primary biliary poisoning and primary biliary cirrhosis.cirrhosis.

PenicillaminePenicillamine• DosingDosing
Lead poisoning:Lead poisoning:
20-30 mg/kg/day in 3-4 divided doses; 20-30 mg/kg/day in 3-4 divided doses; initiating treatment at 25% and initiating treatment at 25% and maximum dose: 1.5 g/daymaximum dose: 1.5 g/day
Arsenic poisoningArsenic poisoning
100 mg/kg/day divided every 6 hrs for 100 mg/kg/day divided every 6 hrs for 5 days5 days

PenicillaminePenicillamine
• Monitoring parameters:Monitoring parameters:
CBC, hemoglobin, platelet countCBC, hemoglobin, platelet count
• Interactions:Interactions:
Food, antimalarials, goldFood, antimalarials, gold

ToxicologyToxicology
Oral TestOral Test
Lecture 9 15th April, Lecture 9 15th April, 1111

ToxicologyToxicology
PresentationsPresentations
Lecture 10, 11 & 12 25th Lecture 10, 11 & 12 25th April, 11April, 11

ToxicologyToxicology
Arsenic toxicityArsenic toxicity
Lecture 13 29th April, Lecture 13 29th April, 1111

Arsenic toxicityArsenic toxicity
• King of Poisons, King of Poisons, Arsenic trioxide, Arsenic trioxide, sodium arsenite, arsenic acid, sodium arsenite, arsenic acid, arsenilic acid & arsenosugars.arsenilic acid & arsenosugars.
• Arsine (AsH3) is an important Arsine (AsH3) is an important gaseous arsenical.gaseous arsenical.
• Occupational exposure to arsenic Occupational exposure to arsenic occurs in the manufacture of occurs in the manufacture of pesticides, herbicides, and other pesticides, herbicides, and other agricultural products.agricultural products.
• Arsenic contaminated drinking water.Arsenic contaminated drinking water.

Arsenic toxicityArsenic toxicity
• Environmental exposure by burning Environmental exposure by burning of coal containing naturally high of coal containing naturally high levels of arsenic and perhaps from levels of arsenic and perhaps from wood reacted with arsenical wood reacted with arsenical compounds.compounds.
• Food, especially seafood. Arsenic in Food, especially seafood. Arsenic in seafood is largely in an organic form seafood is largely in an organic form called arsenobetaine.called arsenobetaine.
• Used as Fowler's solution in psoriasisUsed as Fowler's solution in psoriasis

Arsenic toxicityArsenic toxicity• Inhibits citric acid cycle by blocking Inhibits citric acid cycle by blocking
lipoic acid which is a cofactor for lipoic acid which is a cofactor for pyruvate dehydrogenase; and also pyruvate dehydrogenase; and also by competing with phosphate and by competing with phosphate and stops oxidative phosphorylation, and stops oxidative phosphorylation, and thus inhibit energy-linked reduction thus inhibit energy-linked reduction of NAD+, mitochondrial respiration of NAD+, mitochondrial respiration and ATP synthesis.and ATP synthesis.

Arsenic toxicityArsenic toxicity• Hydrogen peroxide production is also Hydrogen peroxide production is also
increased, which might form ROS increased, which might form ROS and causes oxidative stress. and causes oxidative stress.
• These metabolic interferences lead These metabolic interferences lead to death of multi-system organ to death of multi-system organ failure, probably from necrotic cell failure, probably from necrotic cell death, not apoptosis.death, not apoptosis.
• A post mortem reveals brick red A post mortem reveals brick red coloured mucosa, owing to severe coloured mucosa, owing to severe haemorrhage.haemorrhage.

Arsenic toxicityArsenic toxicity
• Skin is a potential route of exposure Skin is a potential route of exposure presenting sign of white bands in presenting sign of white bands in fingernails.fingernails.
• Profuse sweating.Profuse sweating.
• UTI’s as indicator of urinary arsenic UTI’s as indicator of urinary arsenic toxicity.toxicity.

• For acute arsenic poisoning, For acute arsenic poisoning, treatment is symptomatic, with treatment is symptomatic, with particular attention to fluid volume particular attention to fluid volume replacement and support of b.p.replacement and support of b.p.
• The oral chelator penicillamine.The oral chelator penicillamine.
• The best strategy for preventing The best strategy for preventing chronic arsenic poisoning is by chronic arsenic poisoning is by reducing exposure.reducing exposure.

ToxicologyToxicology
General Management of General Management of ToxicityToxicity
Lecture 14 2nd May, Lecture 14 2nd May, 1111

General Management of
Toxicity

General Management of General Management of ToxicityToxicity
• Antidotes exert a beneficial effect by;Antidotes exert a beneficial effect by;Forming an inert complex with the Forming an inert complex with the
poison e.g. deferoxaminepoison e.g. deferoxamineReducing the rate of conversion of Reducing the rate of conversion of
the poison to more toxic compound the poison to more toxic compound e.g. ethanole.g. ethanol

General Management of General Management of ToxicityToxicity
Competing with toxic substances for Competing with toxic substances for essential receptor sites e.g. oxygen, essential receptor sites e.g. oxygen, naloxone, Vit. K.naloxone, Vit. K.
Blocking essential receptors through which Blocking essential receptors through which the toxic responses are mediated e.g. the toxic responses are mediated e.g. atropineatropine
REDUCTION OF POISON ABSORPTIONREDUCTION OF POISON ABSORPTIONINCREASED POISON ELIMINATIONINCREASED POISON ELIMINATION

ToxicologyToxicology
REDUCTION OF POISON REDUCTION OF POISON ABSORPTIONABSORPTION
Lecture 15 6th May, Lecture 15 6th May, 1111

ToxicologyToxicology
Mid Term Paper discussionMid Term Paper discussion
Lecture 16 16th May, Lecture 16 16th May, 1111

ToxicologyToxicology
Increasing Poison Increasing Poison EliminationElimination
Lecture 17 20th May, Lecture 17 20th May, 1111

Increasing Poison Increasing Poison EliminationElimination
1.1.Urine alkalinizationUrine alkalinization
• Unionized and lipid soluble Unionized and lipid soluble molecules are largely molecules are largely reabsorbed by the renal tubulesreabsorbed by the renal tubules
• With alkalinization drugs With alkalinization drugs become fully ionized and there become fully ionized and there is reduction in reabsorption is reduction in reabsorption leading to enhanced elimination.leading to enhanced elimination.

Increasing Poison Increasing Poison EliminationElimination
•Alkalinization is achieved by Alkalinization is achieved by incresing urine pH to incresing urine pH to approximately 7.5 by approximately 7.5 by administering I/V sodium administering I/V sodium bicarbonate. bicarbonate.

Increasing Poison Increasing Poison EliminationElimination
2. 2. Multiple dose activated charcoal Multiple dose activated charcoal administrationadministration
3. 3. HaemodialysisHaemodialysis
• In acute renal failure (ARF)In acute renal failure (ARF)
• In severe clinical features and high In severe clinical features and high plasma concentration of ethanol, plasma concentration of ethanol, methanol, lithium, isopropanol and methanol, lithium, isopropanol and salicylates.salicylates.

Some Physical Signs of Some Physical Signs of Specific PoisoningSpecific Poisoning
• Constricted pupilsConstricted pupils
1.1.OpioidsOpioids
2.2.Organophosphorus insecticidesOrganophosphorus insecticides
• ConvulsionsConvulsions
1.1.TCA’sTCA’s
2.2.OpioidsOpioids
3.3.IsoniazidIsoniazid

Some Physical Signs of Some Physical Signs of Specific PoisoningSpecific Poisoning
•Dilated pupilsDilated pupils
1.1.TCA’sTCA’s
2.2.AntimuscarinicAntimuscarinic
•Dystonic reactionsDystonic reactions
1.1.MetoclopramideMetoclopramide
2.2.PhenothiazinesPhenothiazines

Some Physical Signs of Some Physical Signs of Specific PoisoningSpecific Poisoning
• Delirium and HallucinationsDelirium and Hallucinations
1.1.Antimuscarinic drugsAntimuscarinic drugs
• Loss of visionLoss of vision
1.1.MetahnolMetahnol
2.2.QuinineQuinine
• HypertoniaHypertonia
1.1.TCA’sTCA’s

Some Physical Signs of Some Physical Signs of Specific PoisoningSpecific Poisoning
• PapilloedemaPapilloedema
1.1.Carbon monoxideCarbon monoxide
2.2.MethanolMethanol
• NystagmusNystagmus
1.1.PhenytoinPhenytoin
2.2.CarbamazapineCarbamazapine

Some Physical Signs of Some Physical Signs of Specific PoisoningSpecific Poisoning
• Tinnitus and deafnessTinnitus and deafness
1.1.SalicylatesSalicylates
2.2.QuinineQuinine
• HyperthermiaHyperthermia
1.1.MDMA (ecstasy)MDMA (ecstasy)

ToxicologyToxicology
antidote: NALOXONEantidote: NALOXONE
Lecture 18 27th May, Lecture 18 27th May, 1111

OPIOIDSOPIOIDS• An An opioidopioid is a chemical that works by binding is a chemical that works by binding
to opioid receptors, which are found to opioid receptors, which are found principally in the central and peripheral principally in the central and peripheral nervous system and the gastrointestinal tract.nervous system and the gastrointestinal tract.
• Obtained from opium plants.Obtained from opium plants.
• The analgesic effects of opioids are due to The analgesic effects of opioids are due to decreased perception of pain, decreased decreased perception of pain, decreased reaction to pain as well as increased pain reaction to pain as well as increased pain tolerance. tolerance.

OPIOIDSOPIOIDS
•Opioids bind to specific opioid Opioids bind to specific opioid receptors in the nervous system and receptors in the nervous system and other tissues. There are three other tissues. There are three principal classes of opioid receptors, principal classes of opioid receptors, μ, κ, δ.μ, κ, δ.
•Morphine, Mepiridine, Fentanyl, Morphine, Mepiridine, Fentanyl, AlfentanilAlfentanil

OPIOIDSOPIOIDS
•The side effects of opioids The side effects of opioids include sedation, respiratory include sedation, respiratory depression, constipation, and a depression, constipation, and a strong subjective sense of strong subjective sense of euphoria.euphoria.

OPIOIDSOPIOIDS
•Opioids can cause cough Opioids can cause cough suppression, which can be both suppression, which can be both an indication for opioid an indication for opioid administration or an unintended administration or an unintended side effect.side effect.
•Opioid dependence can develop Opioid dependence can develop with ongoing administration.with ongoing administration.

NALOXONE

Therapeutic categoryTherapeutic category
• Antidote for narcotic agentsAntidote for narcotic agents
Dosage formsDosage forms
• 400mcg/ml ampoule. (I.V, I.M, S.C)400mcg/ml ampoule. (I.V, I.M, S.C)

Available brandsAvailable brands
• Nalox Inj. 0.4 mg/mlNalox Inj. 0.4 mg/ml
• Naloxone Inj. 0.4 mg/mlNaloxone Inj. 0.4 mg/ml

Mechanism of ActionMechanism of Action
• Pure opioid antagonist that competes Pure opioid antagonist that competes and displaces narcotics at opioid and displaces narcotics at opioid receptor sites.receptor sites.

Uses/IndicationsUses/Indications
• Reverses CNS and respiratory Reverses CNS and respiratory depression in suspected narcotics depression in suspected narcotics overdose;overdose;
• Neonatal opiate depressionNeonatal opiate depression

DosingDosing
Opiate overdose:Opiate overdose:
• Adult (0.4-2mg/dose repeat every 2-Adult (0.4-2mg/dose repeat every 2-3 minutes)3 minutes)
Post anesthesia narcotic reversal:Post anesthesia narcotic reversal:
• Adult (0.1-0.2 mg direct I.V)Adult (0.1-0.2 mg direct I.V)

Monitoring parametersMonitoring parameters
• Respiratory rateRespiratory rate
• Heart rateHeart rate
• Blood pressureBlood pressure

Adverse Reactions:Adverse Reactions:
• Cardiac arrestCardiac arrest
• HypertensionHypertension
• ArrhythmiasArrhythmias
Contraindications:Contraindications:• Hypersensitivity to naloxoneHypersensitivity to naloxone

ToxicologyToxicology
Marine ToxicityMarine Toxicity
Lecture 19 30th May, Lecture 19 30th May, 1111

Ciguatera Fish PoisoningCiguatera Fish Poisoning
• 4000 spp have been reported as 4000 spp have been reported as ciguatoxic (cigua mean toxic; used for ciguatoxic (cigua mean toxic; used for poisonous snail)poisonous snail)
• CiguateraCiguatera is a foodborne illness is a foodborne illness caused by eating certain reef fishes caused by eating certain reef fishes whose flesh is contaminated with toxins whose flesh is contaminated with toxins originally produced by dinoflagellatesoriginally produced by dinoflagellates
• Lipid soluble and heat stable Lipid soluble and heat stable compoundscompounds
• MOA: inhibition of acetyl cholinesterase MOA: inhibition of acetyl cholinesterase activityactivity

Ciguatera Fish PoisoningCiguatera Fish Poisoning
• Clinical features:Clinical features:
• The onset of symptoms occur from a few The onset of symptoms occur from a few minutes to 30 hrs. after ingestion of toxic minutes to 30 hrs. after ingestion of toxic fish.fish.
• Signs are: abdominal cramps, nausea, Signs are: abdominal cramps, nausea, vomiting, watery diarrhea, numbness and vomiting, watery diarrhea, numbness and parasthesias of lips, tongue and throat, parasthesias of lips, tongue and throat, malaise, dty mouth, metallic taste, malaise, dty mouth, metallic taste, myalgia, arthralgia, blurred vision, myalgia, arthralgia, blurred vision, photophobia and transient blindness.photophobia and transient blindness.

Ciguatera Fish PoisoningCiguatera Fish Poisoning• Recovery takes from 48 hrs to one Recovery takes from 48 hrs to one
week in the mild form.week in the mild form.
• Treatment:Treatment:Treatment is symptomatic although Treatment is symptomatic although
atropine has occasionally lessened atropine has occasionally lessened some of the cardiovascular and some of the cardiovascular and gastrointestinal manifestations.gastrointestinal manifestations.
Gabapentin may be useful in Gabapentin may be useful in lessening persistent parasthesias.lessening persistent parasthesias.

Ciguatera Fish PoisoningCiguatera Fish Poisoning
• There is some evidence that calcium channel There is some evidence that calcium channel blocker type drugs such as Nifedipine and blocker type drugs such as Nifedipine and Verapamil are effective in treating some of Verapamil are effective in treating some of the symptoms that remain after the initial the symptoms that remain after the initial sickness passes, such as poor circulation and sickness passes, such as poor circulation and shooting pains through the chest.shooting pains through the chest.
• Steroids and vitamin supplements support Steroids and vitamin supplements support the body's recovery rather than directly the body's recovery rather than directly reducing toxin effects.reducing toxin effects.

Scombrotoxic Fish PoisoningScombrotoxic Fish Poisoning
• This is due to the action of bacteria such This is due to the action of bacteria such as Proteus as Proteus morganimorgani and Klebsiella and Klebsiella pneumoniaepneumoniae in decomposing the flesh of in decomposing the flesh of fish if the fish are stored at insufficiently fish if the fish are stored at insufficiently low temperatures.low temperatures.
• The spoiled fish can contain excessively The spoiled fish can contain excessively high conc of hiostamines (muscle high conc of hiostamines (muscle histidine is broken down by the bacteria histidine is broken down by the bacteria to histamine).to histamine).

Scombrotoxic Fish PoisoningScombrotoxic Fish Poisoning
• Clinical Features: The mean Clinical Features: The mean incubation period is 30 minutes.incubation period is 30 minutes.
• The illness is characterized by The illness is characterized by flushing, headache, sweating , flushing, headache, sweating , dizziness, burning of the mouth and dizziness, burning of the mouth and throat, abdominal cramps, nausea, throat, abdominal cramps, nausea, vomiting and diarrhea.vomiting and diarrhea.

Scombrotoxic Fish PoisoningScombrotoxic Fish Poisoning
• HistamineHistamine is an organic nitrogen is an organic nitrogen compound involved in local immune compound involved in local immune responses as well as regulating responses as well as regulating physiological function in the gut and physiological function in the gut and acting as a neurotransmitter.acting as a neurotransmitter.
Histamine triggers the inflammatory Histamine triggers the inflammatory response. response.

Scombrotoxic Fish PoisoningScombrotoxic Fish Poisoning
•Treatment:Treatment:Treatment is symptomatic and Treatment is symptomatic and
supportive. Antihistami9nes may supportive. Antihistami9nes may suppress the illness.suppress the illness.

Stings from Marine animalsStings from Marine animals
• Several spp of fish have venomous stings Several spp of fish have venomous stings in their fins.these include weaver fish, in their fins.these include weaver fish, short spine cottus, spiny dog fish and the short spine cottus, spiny dog fish and the sting rays.sting rays.
• Clinical Features:Clinical Features:
• Intense local pain, swelling, bruising, Intense local pain, swelling, bruising, blistering, necrosis and if the poisonous blistering, necrosis and if the poisonous spine is not removed, chronic sepsis may spine is not removed, chronic sepsis may takes place. takes place.

Stings from Marine animalsStings from Marine animals
• Treatment:Treatment:
• Immersing the affected part in hot Immersing the affected part in hot water may relieve local symptoms as water may relieve local symptoms as this denatures the thermo labile this denatures the thermo labile toxin.toxin.

Jelly FishJelly Fish
• The stings of jelly fish contains a The stings of jelly fish contains a toxic peptide phospholipase A and a toxic peptide phospholipase A and a hstamine liberating factor.hstamine liberating factor.
• Clinical features: local pain occurs Clinical features: local pain occurs followed by myalgia, nausea, followed by myalgia, nausea, gripping abdominal pain, dyspnoea gripping abdominal pain, dyspnoea and even death.and even death.

Jelly FishJelly Fish
• Treatment:Treatment:Vinegar (3 to 10% aqueous acetic acid) is Vinegar (3 to 10% aqueous acetic acid) is
a common remedy to help with jellyfish a common remedy to help with jellyfish stingsstings
Adhesive tape my be used to remove Adhesive tape my be used to remove any tentacles still adherent to the any tentacles still adherent to the patient. Local analgesia and patient. Local analgesia and antihistamine creams provide antihistamine creams provide symtomatic relief.symtomatic relief.

ToxicologyToxicology
antidote: Protamine antidote: Protamine SulfateSulfate
Lecture 20 3rd June, Lecture 20 3rd June, 1111

HeparinHeparin
• highly-sulfated mucopolysaccharide, is highly-sulfated mucopolysaccharide, is widely used as an injectable widely used as an injectable anticoagulantanticoagulant
• naturally-occurring anticoagulant naturally-occurring anticoagulant produced by basophils and mast cellsproduced by basophils and mast cells
• pharmaceutically heparin is derived from pharmaceutically heparin is derived from mucosal tissues of slaughtered meat mucosal tissues of slaughtered meat animals such as porcine (pig) intestine or animals such as porcine (pig) intestine or bovine (cow) lungbovine (cow) lung

HeparinHeparin
• acts as an anticoagulant, preventing acts as an anticoagulant, preventing the formation of clots and extension the formation of clots and extension of existing clots within the bloodof existing clots within the blood
• does not break down clots that have does not break down clots that have already formed but allows the body's already formed but allows the body's natural clot lysis mechanisms to work natural clot lysis mechanisms to work normally to break down clots that normally to break down clots that have formedhave formed

HeparinHeparin• Heparin and its low molecular weight Heparin and its low molecular weight
derivatives (e.g. enoxaparin, dalteparin, derivatives (e.g. enoxaparin, dalteparin, tinzaparin) are effective at preventing deep tinzaparin) are effective at preventing deep vein thromboses and pulmonary emboli in vein thromboses and pulmonary emboli in patients at riskpatients at risk
• Heparin binds to the enzyme inhibitor Heparin binds to the enzyme inhibitor antithrombin III (AT) causing a conformational antithrombin III (AT) causing a conformational change that results in its activation through change that results in its activation through an increase in the flexibility of its reactive site an increase in the flexibility of its reactive site looploop

HeparinHeparin
• The activated AT then inactivates The activated AT then inactivates thrombin and other proteases thrombin and other proteases involved in blood clotting, most involved in blood clotting, most notably factor Xa. The rate of notably factor Xa. The rate of inactivation of these proteases by AT inactivation of these proteases by AT can increase by up to 1000-fold due can increase by up to 1000-fold due to the binding of heparin.to the binding of heparin.

Protamine Sulfate

Protamine SulfateProtamine Sulfate
Therapeutic categoryTherapeutic category
•Antidote for heparinAntidote for heparin
Dosage formsDosage forms
• Injection 10 mg/ml, solution as Injection 10 mg/ml, solution as sulfate (5 ml, 25 ml)sulfate (5 ml, 25 ml)

Protamine SulfateProtamine SulfateMechanism of actionMechanism of action
•Combines with strongly acidic heparin to Combines with strongly acidic heparin to form a stable complex (salt) neutralizing form a stable complex (salt) neutralizing the anticoagulant activity of drug.the anticoagulant activity of drug.
Uses/IndicationsUses/Indications
•Treatment of heparin over dosage; Treatment of heparin over dosage; neutralize heparin during surgery or neutralize heparin during surgery or dialysis procedures.dialysis procedures.

Protamine SulfateProtamine Sulfate
DosingDosing
•1 mg of protamine neutralizes 90 1 mg of protamine neutralizes 90 units of heparin.units of heparin.
•Maximum of 50 mg in any 10 Maximum of 50 mg in any 10 minute periodminute period

Protamine SulfateProtamine Sulfate
Monitoring parametersMonitoring parameters
•Coagulation tests, APTT or ACT, Coagulation tests, APTT or ACT, Cardiac monitor and blood Cardiac monitor and blood pressure monitoring required pressure monitoring required during administration.during administration.

Protamine SulfateProtamine Sulfate
Adverse reactionsAdverse reactions
•Sudden fall in blood, Sudden fall in blood, hypotension, hemorrhage, hypotension, hemorrhage, dyspnea, hypersensitivity dyspnea, hypersensitivity reactionsreactions

ToxicologyToxicology
EntomotoxicologyEntomotoxicology
Lecture 21 10th June, Lecture 21 10th June, 1111

EntomotoxicologyEntomotoxicology• EntomotoxicologyEntomotoxicology is the analysis of is the analysis of
toxins in arthropods (mainly flies and toxins in arthropods (mainly flies and beetles) that feed on carrion.beetles) that feed on carrion.
• Carrion refers to the carcass of a Carrion refers to the carcass of a dead animal.dead animal.
• Using arthropods at a crime scene, Using arthropods at a crime scene, investigators can determine whether investigators can determine whether toxins were present in a body at the toxins were present in a body at the time of death.time of death.

EntomotoxicologyEntomotoxicology• This technique is a major advance in This technique is a major advance in
forensics; previously, such forensics; previously, such determinations were impossible in determinations were impossible in the case of severely decomposed the case of severely decomposed bodies devoid of intoxicated tissue bodies devoid of intoxicated tissue and bodily fluids.and bodily fluids.

EntomotoxicologyEntomotoxicology
TechniquesTechniques
1. Sample preparation1. Sample preparation
• Entomological samples are analyzed Entomological samples are analyzed in similar standards to human tissue in similar standards to human tissue samples. Once the specimens have samples. Once the specimens have been removed from the body, or the been removed from the body, or the crime scene, they are washed with crime scene, they are washed with deionized or tap water. deionized or tap water.

EntomotoxicologyEntomotoxicology
• The specimens are then frozen for The specimens are then frozen for storage at a temperature ranging from -storage at a temperature ranging from -20°C to 4°C until they are needed for 20°C to 4°C until they are needed for analyses.analyses.
• To prepare for analysis of To prepare for analysis of inorganic inorganic substancessubstances, the arthropods are taken , the arthropods are taken out of storage, washed, and then dried out of storage, washed, and then dried to insure the removal of any foreign to insure the removal of any foreign human fluids. human fluids.

EntomotoxicologyEntomotoxicology
• The arthropods are then crushed and The arthropods are then crushed and stored in a porcelain crucible at a stored in a porcelain crucible at a constant 650°C for 24 hours. The constant 650°C for 24 hours. The resulting ash has a high resulting ash has a high concentration of metals, which are concentration of metals, which are then analyzed by acid digestion then analyzed by acid digestion using 70% HNOusing 70% HNO33 (nitric acid). (nitric acid).

EntomotoxicologyEntomotoxicology
• For preparation of For preparation of organic organic substancessubstances, the specimens are first , the specimens are first washed and dried. Between 1–10 washed and dried. Between 1–10 grams of larvae are finely cut and an grams of larvae are finely cut and an internal standard solution is added.internal standard solution is added.
• The specimens are then The specimens are then homogenized, in a 0.9% saline homogenized, in a 0.9% saline solution, and centrifuged. solution, and centrifuged.

EntomotoxicologyEntomotoxicology
• Chitinous samples are prepared by Chitinous samples are prepared by adding an internal standard solution adding an internal standard solution to finely chopped casings and placing to finely chopped casings and placing the sample in test tubes. Strong the sample in test tubes. Strong acids or bases break down the acids or bases break down the chitinous exoskeleton to release any chitinous exoskeleton to release any toxins.toxins.

EntomotoxicologyEntomotoxicology
• Hydrochloric acid is added to the test Hydrochloric acid is added to the test tube, and the sample is allowed to tube, and the sample is allowed to extract overnight at a temperature of extract overnight at a temperature of 65°C.65°C.
• The acid solution is then removed The acid solution is then removed and the substances are fully and the substances are fully available for further analyses.available for further analyses.

EntomotoxicologyEntomotoxicology
2. Analysis2. Analysis
• Substances are analyzed using Substances are analyzed using inductively coupled plasma (ICP), inductively coupled plasma (ICP), atomic emission spectroscopy (AES), atomic emission spectroscopy (AES), and flame atomic absorption and flame atomic absorption spectrometry (FAAS).spectrometry (FAAS).