Leader Neurologicalparaneoplastic syndromes · Leader Neurologicalparaneoplastic syndromes...
6
I Clin Pathol 1997;50:975-980 Leader Neurological paraneoplastic syndromes U Nath, R Grant Abstract Paraneoplastic neurological syndromes are uncommon, however, their diagnosis is of major practical importance. The identifi- cation of antibodies in the serum or cerebrospinal fluid in central nervous sys- tem paraneoplastic syndromes confirms the clinical diagnosis of a paraneoplastic syndrome and allows early identification of an underlying tumour at a stage when it is localised and more amenable to treatment. The failure to identify antibodies in pa- tients with characteristic presentations of underlying neurological paraneoplastic syndromes does not exclude an underlying cancer. Necrotising myelopathy, dermato- myositis, and chronic inflammatory demy- elinating polyneuropathy all occur more frequently than expected in patients with cancer but autoantibodies have not yet been identified. Although significant ad- vances have been made in diagnosis, fuir- ther research is needed in the detection of autoantibodies and the elucidation of their role in the aetiology of neurological dis- ease. (y Clin Pathol 1997;50:975-980) Keywords: neurological paraneoplastic syndromes; Lambert-Eaton myasthenic syndrome Neurological complications of systemic cancer are very common (fig 1) and may be due to direct involvement from cancer or non- metastatic complications. The term paraneo- plastic neurological syndrome is used to describe a group of well defined non-metastatic conditions that probably have an autoimmune basis. Paraneoplastic syndromes exclude can- cer related vascular disease, infections, meta- bolic or nutritional disease, and complications of treatment. Neurological paraneoplastic syndromes af- fect fewer than 1% of all cancer patients but they are important because the neurological syndrome is often severe and precedes the identification of the cancer in about 50% of cases.' Identification of the syndrome may allow diagnosis at a time when the primary tumour is small and localised and therefore more amenable to treatment. Recognition of specific neurological paraneoplastic syndromes helps focus the search for particular cancers, and identification of antibodies helps to confirm the diagnosis. Aetiology The aetiology of paraneoplastic syndromes is uncertain but an immune related mechanism is the most plausible. The evidence for a direct A CorifUsion Agitatior Nil focal 1 DrLus 2: Metabolic endocrine 31 Infective 4: NuLtritiornal 5: VascLilar 6 Paraneoplastic Departnent of Clinical Neurosciences, Western General Hospital, Crewe Road South, Edinburgh, UK U Nath R Grant Correspondence to: Dr Grant. Focal sigins 1: Seconrdary deposits 2: Abscess enceph .HSV, 3. Hydrocephalis 4 VascuJlar B Ataxia 1 1Seconidar-y deposits 21 Drugs 3i Inifective 4i Nutritiornal - thiarmninre cdeficierncy 51 Vascular 6i Subacute cerebellar cdegerg OMA C Paraparesis Senrsory level 1: Secoridary deposits 2r Infective 3i Nutritional - B-.2 deficierncy 4i VascLular 5i Paranieoplastic D Facial BUlbar weakness 1 Myaesthernia cgravis 21 LEMS E Proximal vweakness I 1Metabolic endocrine 2 Derriiato polyrmyositis 3: Myaesthenia gravis 4: LEMS F Arref lexia G Sensory loss ± weaikness 1 DrUggs- chemotherapy, alcohol 2i DM renial hepatic thyroid 3i NUtritional 41 Paraneoplastic Accepted for publication 2 September 1997 Figure 1 Causes of neurological disorders related to neoplasia. LEMS, Lambert-Eaton myasthenic syndrome. 975 on March 15, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.50.12.975 on 1 December 1997. Downloaded from
Transcript of Leader Neurologicalparaneoplastic syndromes · Leader Neurologicalparaneoplastic syndromes...
I Clin Pathol 1997;50:975-980
Leader
Neurological paraneoplastic syndromes
U Nath, R Grant
AbstractParaneoplastic neurological syndromes areuncommon, however, their diagnosis is ofmajor practical importance. The identifi-cation of antibodies in the serum orcerebrospinal fluid in central nervous sys-tem paraneoplastic syndromes confirmsthe clinical diagnosis of a paraneoplasticsyndrome and allows early identification ofan underlying tumour at a stage when it islocalised and more amenable to treatment.The failure to identify antibodies in pa-tients with characteristic presentations ofunderlying neurological paraneoplasticsyndromes does not exclude an underlyingcancer. Necrotising myelopathy, dermato-myositis, and chronic inflammatory demy-elinating polyneuropathy all occur morefrequently than expected in patients withcancer but autoantibodies have not yetbeen identified. Although significant ad-vances have been made in diagnosis, fuir-ther research is needed in the detection ofautoantibodies and the elucidation of theirrole in the aetiology of neurological dis-ease.(y Clin Pathol 1997;50:975-980)
Keywords: neurological paraneoplastic syndromes;Lambert-Eaton myasthenic syndrome
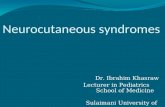
Neurological complications of systemic cancerare very common (fig 1) and may be due todirect involvement from cancer or non-metastatic complications. The term paraneo-plastic neurological syndrome is used todescribe a group ofwell defined non-metastaticconditions that probably have an autoimmunebasis. Paraneoplastic syndromes exclude can-cer related vascular disease, infections, meta-bolic or nutritional disease, and complicationsof treatment.
Neurological paraneoplastic syndromes af-fect fewer than 1% of all cancer patients butthey are important because the neurologicalsyndrome is often severe and precedes theidentification of the cancer in about 50% ofcases.' Identification of the syndrome mayallow diagnosis at a time when the primarytumour is small and localised and thereforemore amenable to treatment. Recognition ofspecific neurological paraneoplastic syndromeshelps focus the search for particular cancers,and identification of antibodies helps toconfirm the diagnosis.
AetiologyThe aetiology of paraneoplastic syndromes isuncertain but an immune related mechanism isthe most plausible. The evidence for a direct
A CorifUsion Agitatior
Nil focal1 DrLus2: Metabolic endocrine31 Infective4: NuLtritiornal5: VascLilar6 Paraneoplastic
Departnent of ClinicalNeurosciences,Western GeneralHospital, Crewe RoadSouth, Edinburgh, UKU NathR Grant
Correspondence to:Dr Grant.
Focal sigins1: Seconrdary deposits2: Abscess enceph .HSV,3. Hydrocephalis4 VascuJlar
B Ataxia1 1Seconidar-y deposits21 Drugs3i Inifective4i Nutritiornal - thiarmninre cdeficierncy51 Vascular6i Subacute cerebellar cdegerg OMA
C Paraparesis Senrsory level1: Secoridary deposits2r Infective3i Nutritional - B-.2 deficierncy4i VascLular5i Paranieoplastic
D Facial BUlbar weakness1 Myaesthernia cgravis21 LEMS
E Proximal vweaknessI 1Metabolic endocrine2 Derriiato polyrmyositis3: Myaesthenia gravis4: LEMS
F Arreflexia
G Sensory loss ± weaikness1 DrUggs- chemotherapy, alcohol2i DM renial hepatic thyroid3i NUtritional41 Paraneoplastic
Accepted for publication2 September 1997 Figure 1 Causes of neurological disorders related to neoplasia. LEMS, Lambert-Eaton myasthenic syndrome.
975
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from

Nath, Grant
Table 1 Common paraneoplastic syndromes affecting the nervous system
Terminology
Immunohisto-Syndrome chemistry Western immunoblot Common tumour site
Brain and cranial nervesLimbic encephalitis or encephalomyelitis ANNA-1 35-38 kDA Lung (Hodgkin's)Subacute cerebellar degenerationA APCA 34, 62 kDA Gynaecological, breast, lungB ANNA-1 35-38 kDA LungC Negative Negative Hodgkin's disease
Opsoclonus-myoclonus-ataxia ANNA-2 55, 80 kDA Neuroblastoma (children)Breast, lung (adults)
Photoreceptor degeneration ANNA-1 47 kDa Lung
Dorsal root gangliaSubacute sensory neuronopathy ANNA-1 35-38 kDa Lung
Peripheral nervesAcute inflammatory demyelinating Uncertain Uncertain Hodgkin's, adenocarcinoma,
polyneuropathy osteosclerotic myelomaChronic inflammatory demyelinating Uncertain Uncertain Hodgkin's, adenocarcinoma,
polyneuropathy osteosclerotic myeloma
Neuromuscularjunction and muscleLambert-Eaton myasthenic syndrome Voltage gated calcium channel Lung, prostate, cervix
antibodyDermatomyositis Uncertain Uncertain Breast, ovary, lung, lymphoma
autoimmune basis is strongest for Lambert-Eaton myasthenic syndrome (LEMS).' Voltagegated calcium channel antibodies have beenidentified in the serum of patients with LEMS,and passive transfer of IgG from affectedpatients induces the disorder in experimentalanimals.2" Voltage gated calcium channel anti-bodies bind to the presynaptic calcium chan-nels of the neuromuscular junction, disruptingthe structure of the channels, and causing fail-ure of release of calcium in response to anaction potential that results in a reduction inacetyl choline release.3
Paraneoplastic syndromes involving the cen-tral nervous system probably also have anautoimmune basis as they are associated withserum autoantibodies. It is likely that thepatient's immune system recognises a tumourrelated antigen as foreign and produces anantibody response. The antibody cross reactswith shared antigens or epitopes in the centralnervous system and may result in a paraneo-plastic neurological syndrome. Despite theassociation of autoantibodies with centralnervous system paraneoplastic neurologicalsyndromes (table 1) passive transfer of immu-noglobulin from patients with paraneoplasticcentral nervous system disease to experimentalanimals does not reproduce the clinical syn-drome or result in pathological changes.Furthermore, immunisation of mice with para-neoplastic antigen does not produce any clini-cal or pathological changes.4
TerminologyThe terminology used to describe paraneo-plastic antibodies has been the subject ofheated controversy. Some groups favour adescriptive generic nomenclature-that is,anti-Purkinje cell antibody (APCA), anti-neuronal nuclear antibody type 1 (ANNA-1),and antineuronal nuclear antibody type 2(ANNA-2) based on immunohistochemistryalone, while others favour the case for an anti-body and antigen specific nomenclature (anti-
Yo, anti-Hu, and anti-Ri) determined by acombination of immunohistochemistry andwestern immunoblotting. 6An international symposium on the topic
developed consensus guidelines for the detec-tion of paraneoplastic antineuronal specificantibodies.7 The consensus opinion is that thetwo terminologies are not interchangeable asimmunohistochemistry alone is not sufficientlyspecific. If antibody is detected in serum orcerebrospinal fluid (CSF) using immunohisto-chemistry alone the result should be referred toas APCA or ANNA depending on immunohis-tochemical findings. ANNA antibody may beassociated with Sjogren's syndrome as well asother autoimmune conditions, whereasanti-Hu is more specific for underlying neopla-sia, usually small cell lung cancer.8 The findingof anti-Hu or anti-Yo in serum or CSF (at adilution of > 1:500 and > 1:50, respectively) byimmunohistochemistry and western immuno-blotting has a specificity of greater than 95%for a paraneoplastic neurological syndrome.9Some patients who have small cell lung cancerwithout neurological symptoms may harbourlow titres of anti-Hu antibody that can only bedetected by western immunoblotting usinghigh affinity purified recombinant proteins.'1An outline of methods used in immunohisto-chemistry and western blotting is given below;further details are available elsewhere.6 7 10
ClassificationA useful clinical classification divides theneurological paraneoplastic syndromes accord-ing to their anatomical level: brain and cranialnerves, spinal cord and dorsal root ganglia,peripheral nerves, neuromuscular junction,and muscle (table 1).1
PARANEOPLASTIC ENCEPHALOMYELITISThis condition is found in around three ofevery 1000 cancer patients and can presentwith a variety of clinical features: seizures,subacute dementia, and personality change
976
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from

Neurological paraneoplastic syndromes
3 S& I I
. qt '
I ~~~~~Ia
t . I I
4t *i is _t
41 4~~~~44 ~~~~~~~~~~~~V.
4,
& a... I.E
4 4
.
9
q
,t
N_ ¢F
;0
a
lbi ;
s
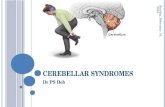
Figure 2 Indirect immunoperoxidase staining. (A) Cerebral cortex section with control serum (1/500 dilution).(B) Cerebral cortex section with serum from a patient with limbic encephalitis and small cell lung cancer (1/500 dilution).Neuronal nuclear staining with faint staining seen in cytoplasm and axons.
(limbic encephalitis), subacute cerebellar signs,and autonomic dysfunction." Paraneoplasticencephalomyelitis has been reported with vari-ous other paraneoplastic syndromes such as
brainstem encephalitis, sensory neuronopathy,and painless visual loss due to paraneoplasticoptic neuritis. Cancer associated spinal corddisease is usually metastatic but when paraneo-
plastic in origin usually occurs in conjunctionwith paraneoplastic encephalomyelitis. Exam-ples of paraneoplastic spinal cord diseaseinclude necrotising myelopathy and myelitis.Magnetic resonance imaging of the brain is
usually normal in paraneoplastic encephalo-myelitis but it may demonstrate temporal lobeatrophy or high signal changes in the temporallobes on T2 weighted images.'2The associated antibody (ANNA-1/anti-Hu)
reacts with a neuronal nuclear antigen thatbelongs to a family of RNA binding proteinsand is present in higher concentrations in CSFthan serum.'3 Identification of anti-Hu antibod-ies (by immunohistochemistry and westernimmunoblot) at a concentration greater than1/500 in serum is highly specific for a paraneo-
plastic neurological syndrome and 80% ofpatients with this finding will have small celllung cancer.
Patients tend to be middle aged and bothsexes are equally affected, although those whohave anti-Hu antibody are more commonlyfemale. The anti-Hu antibody may also bepresent in low titres in patients with small celllung cancer without encephalomyelitis andthese patients tend to be female with lessextensive malignant disease.'0 Other cancers
associated with encephalomyelitis include
breast, gynaecological, and gastrointestinalcancers, and Hodgkin's disease." Patients withencephalomyelitis or sensory neuronopathywho are antibody positive have a betterprognosis than those in whom antibodies are
not identified.' There are no other known anti-bodies associated with paraneoplastic brain-stem encephalitis, optic neuritis or necrotisingmyelopathy. Necrotising myelopathy is associ-ated with lymphomas, leukaemias, and cancer
of the lung.
PathologicalfindingsThe pathological process in paraneoplasticencephalomyeltis occurs diffusely throughoutthe central nervous system. Cases with andwithout anti-Hu antibody are indistin-guishable.' Pathological findings are localisedto the areas of the nervous system that are
involved clinically. '" In limbic encephalitisthere is perivascular lymphocytic cuffing, neu-
ronophagia with microglial proliferation, andastrocytosis. Neuronal loss is most obvious inthe limbic cortex and insula.'" The immunohis-tochemical staining pattern of ANNA-1/anti-Hu consists of strong staining of all centraland peripheral nervous system neuronal nucleiwith sparing of nucleoli and weaker granularcytoplasmic staining; no staining of systemictissues occurs (fig 2).7 Necrotising myelopathyshows widespread necrosis throughout thespinal cord.
PARANEOPLASTIC CEREBELLAR DEGENERATION
Although perhaps the best known of the para-neoplastic neurological syndromes, paraneo-
plastic cerebellar degeneration is rare, occur-
A E
977
I
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from

Nath, Grant
cerebellar disease often follows the diagnosisof lymphoma. Spontaneous or treatment asso-ciated remissions are more common in thissubgroup. Anti-Purkinje cell antibodies re-sembling but not identical to APCA-1/anti-Yohave been found in a small proportion of thesepatients at low titres.Without antineuronal antibodies-Some cases ofparaneoplastic cerebellar degeneration areassociated with small cell lung cancer and mayoccur in association with LEMS.'7 Some ofthese patients have voltage gated calciumchannel antibodies.
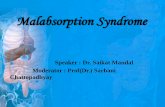
PathologicalfindingsThe pathological process in APCA/anti-Yoantibody positive patients is very site specific.There is severe loss of Purkinje cells through-out the cerebellum, with or without lym-phocytic infiltration, with remaining cellsshowing axonal swelling.' There is atrophy ofthe granular and molecular layers with micro-glial proliferation and astrocytosis but relativesparing of basket cells. The deep cerebellarnuclei and the cerebellar connections to thebrain stem are normal. Patients with APCA-1/anti-Yo antibody tend to show more inflamma-tory changes and characteristic immunofluo-rescence patterns with coarse granular stainingof Purkinje cell cytoplasm as well as proximalaxons and dendrites; nuclei and systemictissues are not stained (fig 3).7 Cases ofparaneoplastic cerebellar degeneration associ-ated with ANNA-1/anti-Hu stain the corticaland cerebellar neuronal nuclei.
Figure 3 Indirect immunoperoxidase technique. (A) Cerebellar section with control serum(11500 dilution). (B) Cerebellar section with serum from a patient with paraneoplasticcerebellar ataxia andfallopian tube carcinoma (11500 dilution). Intense staining of thecytoplasm of Purkinje cells and axons (APCA positive).
ring in two of every 1000 patients with cancer.
There are about 300 cases reported in theliterature. The clinical features are subacutepancerebellar dysfunction with truncal andlimb ataxia, as well as dysarthria and nystag-mus, which develops over weeks. There is oftensevere residual disability. Magnetic resonance
imaging can show cerebellar atrophy in ad-vanced cases.'5 Paraneoplastic cerebellar de-generation can be categorised into four mainsubgroups that differ in prognostic significanceand have different associated autoantibodies.'Associated with APCAlanti-Yo antibody-Thisoccurs in middle aged women with occult ovar-
ian or breast cancer that is usually indolent; thecerebellar disease often precedes identificationof the cancer. Many cases are associated withhigh titres of serum (> 1/500) or CSF (> 1/50)antibodies that react with the Purkinje cells inthe cerebellum (APCA-1/anti-Yo).'6 The anti-gens belong to a family of DNA bindingproteins.Associated with ANNA-llanti-Hu antibody-ANNA-1/anti-Hu antibody can be associatedwith cerebellar degeneration either in isolationor with encephalomyelitis.Associated with Hodgkin 's lymphoma-Thesepatients are usually young men and the
CANCER ASSOCIATED RETINOPATHY
Cancer associated retinopathy is a rare para-
neoplastic condition that presents with epi-sodic visual obscurations and loss of acuitywith associated scotomata. Pathological find-ings include inflammatory infiltrates into bothphotoreceptor and ganglion cells and antibod-ies have been reported against antigens in boththese types of cell.
OPSOCLONUS-MYOCLONUS-ATAXIAParaneoplastic opsoclonus is associated withmyoclonus and truncal ataxia and onset isoften acute."8 Immunohistochemistry of serumor CSF shows an antineuronal nuclear anti-body (ANNA-2). The antibody, anti-Ri, isidentical to ANNA-1 on immunohistochemi-cal criteria but shows a different bandingpattern with western immunoblotting. Westernimmunoblotting identifies bands at 55 and80 kDa and this is referred to as ANNA-2/anti-Ri. The presence of antibody identifies a
subset of patients with this syndrome, usuallyadults, who commonly have a breast or lungneoplasm although it can be associated withgynaecological malignancies. In half of theadult cases with this syndrome neurologicalsymptoms and signs precede the diagnosis ofmalignancy. Children who present withopsoclonus-myoclonus-ataxia do not harbourthe ANNA-2/anti-Ri antibody but are com-
monly found to have neuroblastoma.'°
A
B
978
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from

Neurological paraneoplastic syndromes
PathologicalfindingsMicroscopic appearances described in somecases include mild perivascular inflammatorychanges, loss of Purkinje cells, and abnormali-ties in the dentate nuclei.'820 Immunohisto-chemistry patterns of anti-Ri include strongstaining of only central nervous system neuro-
nal nuclei, sparing of nucleoli, weak granularcytoplasmic staining, and no staining ofsystemic tissues.7
PARANEOPLASTIC SUBACUTE SENSORYNEURONOPATHY (DORSAL ROOTGANGLIONOPATHY)This paraneoplastic syndrome occurs inaround seven of every 1000 cancer patients.Although it is probably the most common
paraneoplastic neurological syndrome it isprobably under recognised. Patients presentwith pure sensory loss developing over weeks tomonths and involving all modalities. It can
involve either upper or lower limbs and can
rarely present in the face.' It precedes identifi-cation of the cancer in the majority of cases andthe occult tumour is usually small cell lungcancer.21
PathologicalfindingsAbnormalities are found in the dorsal rootganglia with infiltration by lymphocytes andmacrophages. In longstanding symptomaticpatients there is neuronal loss and capsular cellproliferation, but little in the way of inflamma-tion. Secondary axonal degeneration occurs inthe dorsal nerve roots, peripheral sensorynerves, and posterior columns of the spinalcord. The lateral and anterior columns are wellpreserved.22
LAMBERT-EATON MYASTHENIC SYNDROMELEMS occurs in around two of every 1000cancer patients and is characterised by limbweakness, usually of the lower limbs, and iscommonly associated with autonomicdysfunction. ' The deep tendon reflexes are
reduced but show facilitation after exercise.Sixty per cent of all cases are associated with anunderlying malignancy and in 40% the LEMSoccurs as an autoimmune condition in its ownright. Non-paraneoplastic cases of LEMSoccur more commonly in middle aged women.When cancer is identified it is usually small celllung cancer, although cancer of the prostate or
cervix have been described. Antibodies againstvoltage gated calcium channels are present inmost patients. Electromyography shows char-acteristic changes of a decrement in compoundmuscle action potential amplitude with lowrates of repetitive stimulation (2-10 Hz) andan increment with high rates (20-40 Hz).2'
PathologicalfindingsMuscle biopsy changes are non-specific usinglight microscopy. Electron microscopic tech-niques are much more helpful and demonstratehypertrophy of the postsynaptic membranewith atrophy of the terminal axons andincreased branching of nerve terminals.24
Treatment of paraneoplastic syndromesIn the vast majority of cases paraneoplasticsyndromes are refractory to any form of treat-ment. Spontaneous remission of neurologicalsymptoms can occur in patients withopsoclonus-myoclonus-ataxia and very rarelyin limbic encephalitis and paraneoplastic cere-bellar degeneration.' Symptoms of LEMS canshow clinical improvement following oraltreatment with 3,4-diaminopyridine. There isincreasing evidence that if paraneoplasticsyndromes can be proved early in the course ofthe disease, treatment directed at the immuneresponse (for example, intravenous immuno-globulin, plasmapheresis, immunosuppression)or at the underlying tumour (surgery, radio-therapy, chemotherapy) can halt or evenreverse the neurological syndrome. Thiamineand clonazepam may be helpful in some casesof paraneoplastic cerebellar degeneration andimmunoadsorption has been of benefit in para-neoplastic opsoclonus.2"
ConclusionAlthough paraneoplastic neurological syn-dromes are uncommon their diagnosis is ofmajor practical importance. The identificationof antibodies in the serum or CSF in centralnervous system paraneoplastic syndromes con-firms the clinical diagnosis and allows earlyidentification of an underlying tumour at astage when it is localised and more amenable totreatment. Identification of antibodies may beof prognostic importance as the presence ofcertain antibodies are associated with a goodresponse to treatment of the underlyingcancer.26 The failure to identify antibodies inpatients with characteristic presentations ofunderlying neurological paraneoplastic syn-dromes does not exclude an underlying cancer.Necrotising myelopathy, dermatomyositis, andchronic inflammatory demyelinating polyneu-ropathy all occur more frequently than ex-pected in patients with cancer but autoantibod-ies have not yet been identified using currenttechniques. Although significant advances havebeen made in diagnosis, further research isneeded in the detection of autoantibodies andthe elucidation of their role in the aetiology ofneurological disease.
We thank Dr J W Ironside for his helpful comments on thismanuscript.
1 Posner JB. Neurologic complications of cancer. Contempo-rary neurology series: 45. Philadelphia, 1995:353-85.
2 Lang B, Newsom-Davis J, Wray D. Autoimmune aetiologyfor Eaton-Lambert myasthenic syndrome. Lancet 1981 ;i:224-6.
3 Rosenfeld MR, Wong E, Dalmau J, et al. Cloning and char-acterisation of a Lambert-Eaton myasthenic syndromeantigen. Ann Neurol 1993;33:113-20.
4 Sillevis Smitt PAE, Manley GT, Posner JB. Immunisationwith the paraneoplastic encephalomyelitis antigen HuDdoes not cause neurologic disease in mice. Neurology 1995;5:1873-8.
5 Lennon VA. Paraneoplastic autoantibodies: the case for adescriptive generic nomenclature. Neurology 1994;44:2236-40.
6 Dalmau J, Posner JB. Neurologic paraneoplastic antibodies(anti-Yo; anti-Hu;anti-Ri): case for a nomenclature basedon antibody and antigen specificity. Neurology 1994;44:2241-6.
7 Moll JWB, Antoine JC, Brashear HR, et al. Guidelines forthe detection of paraneoplastic antineuronal-specificantibodies: report from the workshop to the fourth meetingof the International Society ofNeuroimmunology on Para-neoplastic Neurological Disease, 22-23 October 1994,Rotterdam, the Netherlands. Neurology 1995;45: 1937-41.
979
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from

Nath, Grant
8 Moll JWB, Markusse HM. Antineuronal antibodies inpatients with neurological complications of primarySjogren's syndrome. Neurology 1993;43:2574-81.
9 Twijnstra A, Keyser A, Ongerboer de Visser BW Neuro-oncology-primary tunmours and neurological complications ofcancer. Amsterdam: Elsevier, 1993.
10 Dalmau J, Furneaux HM, Gralla RJ, Kris MG, Posner JB.Detection of anti-Hu antibody in serum of patients withsmall cell lung cancer; a quantitative western blot analysis.Ann Neurol 1990,27:544-52.
11 Dalmau J, Graus F, Rosenblum MK, Posner JB. Anti-Huassociated paraneoplastic encephalomyelitis/sensory neu-ronopathy. A clinical study of 71 patients. Medicine71;2:59-71.
12 Lacomis D,Khosbin S, Schich RM. Magnetic resonanceimaging of paraneoplastic limbic encephalitis. J CompuitAssist Tonmogr 1990;14:115- 17.
13 Furneaux HM, Reich L, Posner JB. Autoantibody synthesisin the CNS of patients with paraneoplastic syndromes.Neurology 1990;40:1085-91.
14 Dalmau J, Furneaux HM, Rosenblum MK. Detection ofanti-Hu antibody in specific regions of the nervous systemand tumour from patients with paraneoplastic encephalo-myelitis and sensory neuropathy. Neurology 1991 ;41:1757-64.
15 Greenberg HS. Paraneoplastic cerebellar degeneration; aclinical and CT study. J Neurooncology 1984;2:337-82.
1 Hetzel DS, Stanhope CR, O'Neil GP. Gynaecologicalcancer in patients with subacute paraneoplastic cerebellardegeneration predicted by APCA antibodies and limited inmetastatic volume. Mayo Clin Proc 1982;57:15-21.
17 Blumenfeld AM, Recht LD, Chad DA. Coexistence ofLambert-Eaton myasthenic syndrome and paraneoplastic
cerebellar degeneration; differential effects of therapy. Neut-rology 1991;41:1682-5.
18 Luque FA, Furneaux HM, Posner JB. Anti-Ri: an antibodyassciated with paraneoplastic opsoclonus and breastcancer. Ann Neurol 1991;29:241-51.
19 Ridley A, Kennard C, Scholtz CL. Omnipause neurones intwo cases of opsoclonus associated with oat-cell carcinomaof the lung. Brain 1987; 110: 1699-709.
20 Ross AJ, Zeman W Opsoclonus,adult cancer and chemicalpathology in the dentate nuclei. Arch.Nceirol 1967;17:546-51.
21 Graus F, Elkon KB, Cordon-Cardo C, Posner JB. Sensoryneuronopathy and small cell lung cancer. An]_Med 1986;80:45-52.
22 Anderson NE, Cunningham JM, Posner JB. Autoimmunepathogenesis of paraneoplastic neurological syndromes.Crit Rev Neurobiol 1987;3:245-99.
23 Lambert EH. Defects of the neuromuscular junction in syn-dromes other than myasthenia gravis. Ann NY Acad Sci1966;135:367-84.
24 Fukuhara N, Takamori M, Gutmann L, Chow SM. EatonLambert syndrome. Ultrastructural study of motor endplates. Arch Neurol 1972;27:67.
25 Nausieda PA, Tanner CM, Weiner WJ. Opsocloniccerebellopathy: a paraneoplastic syndrome responsive tothiamine. Arch Neurol 1981;38:780- 1.
26 Graus F, Dalmau J, Rene R, Tora M, et al. Anti-Hu antibod-ies in patients with small cell lung cancer: association withcomplete response to therapy and improved survival[abstract]. 7Neuro-Onc 1996;30: 129.
Molecular Pathology-December 1997 contents
Reviews
Genetic prognostic markers in colorectal cancerR S Houlston, I PM Tomlinson
Cadherin and catenin biology represent a global mechanism for epithelial cancer progressionJfA J7ankowski, R Bruton, N Shepherd, S Sanders
Papers
Modification of cystatin C activity by bacterial proteinases and neutrophil elastase in periodontitisM Abrahamson,M Wikstrom, _J Potempa, S Renvert, A Hall
Immunohistochemical pattern of insulin-like growth factor (IGF) I, IGF II, and IGF bindingproteins 1 to 6 in carcinoma in situ of the testisB Drescher, H Lauke,M Hartmann,M S Davidoff, WZumkeller
Microvessel density, p53 overexpression, and apoptosis in invasive breast carcinomaF Gonzalez-Palacios, M Sancho, Jf Carlos Martinez, C Bellas
Chromosomal mapping and expression of the human cyr61 gene in tumour cells from thenervous systemC Martinerie, E Viegas-Pequignot, V C Nguyen, B Perbal
Double immunostaining for p53 and molecular chaperone hsp72/73 in gastric carcinomaMA Villaseca, I Roa, 7 C Araya, J C Roa, P Flores
Technical report
Amplification of fluorescent in situ hybridisation signals in formalin fixed paraffin wax embeddedsections of colon tumour using biotinylated tyramideJfA McKay, G I Murray, WN Keith, H L McLeod
Short report
Heterogeneity of clonal lymphocytes with regard to bcl-2 protein concentration and cell sizeTJ7 Bromidge, D _J Howe, S A J7ohnson, S 7 Rule
Miscellanea
Correspondence 0 Book reviews 0 List of assessors 0 Annual author index to volume 50 * Annualsubject index to volume 50 * Annual contents index to volume 50
980
on March 15, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.12.975 on 1 Decem
ber 1997. Dow
nloaded from