Lateral Pontine Hemorrhage: Reappraisal of Benign...
4
954 Lateral Pontine Hemorrhage: Reappraisal of Benign Cases Oscar H. Del-Brutto, MD, Carlos A. Noboa, MD, and Fernando Barinagarrementerfa, MD We reviewed 6 computed tomography-documented cases of primary lateral pontine hemorrhage that occurred in our two institutions over a 2-year period. All patients survived the acute stroke, with excellent functional recovery in 4. The level of consciousness of the patient and the size of the hemorrhage had no consistent bearing on outcome. Both of these features have been considered important prognostic indicators in patients with pontine hemorrhage, but in our series benign out- comes were not restricted only to patients who were alert or had small hemorrhages; on the other hand, severe disability was noticed in 1 patient with a small hematoma strategically located in the pontine tegmentum. Our observations suggest that, although some patients with lateral pontine hemorrhage have a good prognosis, there is no single determinant that predicts outcome in a given patient. (Stroke 1987;18:954-956) T he classic syndrome of pontine hemorrhage in- cludes coma, respiratory abnormalities, pin- point pupils, loss of horizontal eye move- ments, quadriplegia, and bilateral corticospinal tract dysfunction. '~ 3 Ocular bobbing 4 and hyperthermia may also be present. Most patients die within the first 24 hours after the acute event.' At necropsy, the hemato- ma usually involves the entire pons with extension into the midbrain and the fourth ventricle. 2 In recent years, several cases of pontine bleeding with favorable outcome and unexpected clinical mani- festations have been reported. 5 " 20 Widespread use of computed tomography (CT) has led to better recogni- tion of such relatively benign cases. 21 In most of these patients the hematoma was small and confined to one side of the pons. 5 ^ 10 " 1418 " 20 Such reports have changed previous concepts about invariance of the lethal out- come of pontine hemorrhage and have prompted many authors to recognize features that are common to the benign cases. 3 " 8 In this paper, we report 6 cases of lateral pontine hemorrhage to further outline the clini- cal features, CT findings, and outcome of these lesions. Subjects and Methods We reviewed all CT-documented cases of lateral pontine hemorrhage that occurred in our institutions over a 2-year period. After exclusion of bleeding asso- ciated with arteriovenous malformations, tumors, or trauma, we found 6 cases of primary hemorrhage that represent the material for this study. Special emphasis was placed on the level of consciousness at admission From the Division de Neurologia, Institute) Nacional de Neuro- logia y Neurocirugia, Mexico DF, Mexico (O.H.D., F.B.) and the Departamento de Neurologia, Hospital Luis Vemaza, Guayaquil, Ecuador (C.A.N.). Presented at the 10th Annual Meeting of the Mexican Academy of Neurology, Guadalajara, November 4, 1986. Address for reprints: Oscar H. Del-Brutto, MD, Institute Na- cional de Neurologia y Neurocirugia, Insurgentes Sur, No. 3877, CP: 14410 Mexico 22, DF. Received October 24, 1986; accepted May 18, 1987. and on CT findings to further correlate both features with the outcome in every patient (Table 1). Results Four patients were women, 2 men. Ages ranged from 38 to 76 years, with a median of 51 years. Arteri- al hypertension was present in 4 patients. One patient was taking oral amphetamines for obesity. Onset was abrupt in 5 patients; gradual progression over a 48- hour interval was seen in 1 patient. Headache and alteration in consciousness appeared as prominent symptoms. On admission, 3 patients were in a coma, 1 was somnolent, and 2 were alert. Two of the 3 patients initially in a coma regained full consciousness 72 and 96 hours later. Frequent neurologic signs were ocular paresis, small reactive pupils, dysarthria, hemiplegia, and limb ataxia. CT scans showed lateral hematomas in all cases. In all but 2 patients, the hemorrhage in- volved the basal and tegmental pons. Rostral extension was documented in 2 cases. In 2 patients, the hemor- rhage invaded the fourth ventricle with obstruction and secondary hydrocephalus. All patients survived the acute stroke. One patient died of aspiration pneumonia while recovering from the stroke, 4 patients showed almost complete recovery with minor motor sequelae, and the last patient was severely incapacitated 1 month after the stroke. Discussion Lateral pontine hemorrhage was recognized before the availability of CT 1>2>22 ; however, it was considered rare. 2 Using CT, it is clear that the incidence of lateral pontine hemorrhage is greater than previously appreci- ated and the clinical signs more varied. 6 " 20 Two clinical syndromes of hemorrhage confined to one side of the pons have been described. 6 - 23 In one, the hematoma involves both the basis pontis and tegmentum and is associated with crossed hemiparesis and ipsilateral brainstem signs. In the other, the hematoma is con- fined to the tegmentum and is associated with ipsilat- eral brainstem signs. The clinical picture in every pa- tient of our series was consistent with one of these by guest on June 2, 2018 http://stroke.ahajournals.org/ Downloaded from
-
Upload
phungthien -
Category
Documents
-
view
226 -
download
3
Transcript of Lateral Pontine Hemorrhage: Reappraisal of Benign...

954
Lateral Pontine Hemorrhage:Reappraisal of Benign Cases
Oscar H. Del-Brutto, MD, Carlos A. Noboa, MD, and Fernando Barinagarrementerfa, MD
We reviewed 6 computed tomography-documented cases of primary lateral pontine hemorrhage thatoccurred in our two institutions over a 2-year period. All patients survived the acute stroke, withexcellent functional recovery in 4. The level of consciousness of the patient and the size of thehemorrhage had no consistent bearing on outcome. Both of these features have been consideredimportant prognostic indicators in patients with pontine hemorrhage, but in our series benign out-comes were not restricted only to patients who were alert or had small hemorrhages; on the otherhand, severe disability was noticed in 1 patient with a small hematoma strategically located in thepontine tegmentum. Our observations suggest that, although some patients with lateral pontinehemorrhage have a good prognosis, there is no single determinant that predicts outcome in a givenpatient. (Stroke 1987;18:954-956)
The classic syndrome of pontine hemorrhage in-cludes coma, respiratory abnormalities, pin-point pupils, loss of horizontal eye move-
ments, quadriplegia, and bilateral corticospinal tractdysfunction. '~3 Ocular bobbing4 and hyperthermia mayalso be present. Most patients die within the first 24hours after the acute event.' At necropsy, the hemato-ma usually involves the entire pons with extension intothe midbrain and the fourth ventricle.2
In recent years, several cases of pontine bleedingwith favorable outcome and unexpected clinical mani-festations have been reported.5"20 Widespread use ofcomputed tomography (CT) has led to better recogni-tion of such relatively benign cases.21 In most of thesepatients the hematoma was small and confined to oneside of the pons.5^10"1418"20 Such reports have changedprevious concepts about invariance of the lethal out-come of pontine hemorrhage and have prompted manyauthors to recognize features that are common to thebenign cases.3"8 In this paper, we report 6 cases oflateral pontine hemorrhage to further outline the clini-cal features, CT findings, and outcome of theselesions.
Subjects and MethodsWe reviewed all CT-documented cases of lateral
pontine hemorrhage that occurred in our institutionsover a 2-year period. After exclusion of bleeding asso-ciated with arteriovenous malformations, tumors, ortrauma, we found 6 cases of primary hemorrhage thatrepresent the material for this study. Special emphasiswas placed on the level of consciousness at admission
From the Division de Neurologia, Institute) Nacional de Neuro-logia y Neurocirugia, Mexico DF, Mexico (O.H.D., F.B.) and theDepartamento de Neurologia, Hospital Luis Vemaza, Guayaquil,Ecuador (C.A.N.).
Presented at the 10th Annual Meeting of the Mexican Academyof Neurology, Guadalajara, November 4, 1986.
Address for reprints: Oscar H. Del-Brutto, MD, Institute Na-cional de Neurologia y Neurocirugia, Insurgentes Sur, No. 3877,CP: 14410 Mexico 22, DF.
Received October 24, 1986; accepted May 18, 1987.
and on CT findings to further correlate both featureswith the outcome in every patient (Table 1).
ResultsFour patients were women, 2 men. Ages ranged
from 38 to 76 years, with a median of 51 years. Arteri-al hypertension was present in 4 patients. One patientwas taking oral amphetamines for obesity. Onset wasabrupt in 5 patients; gradual progression over a 48-hour interval was seen in 1 patient. Headache andalteration in consciousness appeared as prominentsymptoms. On admission, 3 patients were in a coma, 1was somnolent, and 2 were alert. Two of the 3 patientsinitially in a coma regained full consciousness 72 and96 hours later. Frequent neurologic signs were ocularparesis, small reactive pupils, dysarthria, hemiplegia,and limb ataxia. CT scans showed lateral hematomasin all cases. In all but 2 patients, the hemorrhage in-volved the basal and tegmental pons. Rostral extensionwas documented in 2 cases. In 2 patients, the hemor-rhage invaded the fourth ventricle with obstruction andsecondary hydrocephalus. All patients survived theacute stroke. One patient died of aspiration pneumoniawhile recovering from the stroke, 4 patients showedalmost complete recovery with minor motor sequelae,and the last patient was severely incapacitated 1 monthafter the stroke.
DiscussionLateral pontine hemorrhage was recognized before
the availability of CT1>2>22; however, it was consideredrare.2 Using CT, it is clear that the incidence of lateralpontine hemorrhage is greater than previously appreci-ated and the clinical signs more varied.6"20 Two clinicalsyndromes of hemorrhage confined to one side of thepons have been described.6-23 In one, the hematomainvolves both the basis pontis and tegmentum and isassociated with crossed hemiparesis and ipsilateralbrainstem signs. In the other, the hematoma is con-fined to the tegmentum and is associated with ipsilat-eral brainstem signs. The clinical picture in every pa-tient of our series was consistent with one of these
by guest on June 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Del-Brutto et al Lateral Pontine Hemorrhage 955
Table 1. Level of Consciousness, Computed Tomography Findings, and Outcome in 6 Patients with LateralPontine Hemorrhage
Case/sex/age
l/F/76
2/F/43
3/F/38
4/F/39
5/M/48
6/M/62
Level of consciousness
Sudden coma; alert 96 hours later
Somnolence
Sudden coma; stupor few hourslater
Alert
Sudden coma; alert 72 hours later
Alert
Computed tomography
Right pontine hemorrhage withblood in fourth ventricle;hydrocephalus
Left pontine hemorrhage with ros-tral extension into midbrain
Small hemorrhage in right pontinetegmentum; blood in fourthventricle; hydrocephalus
Small hemorrhage in right side ofpons
Left pontine, midbrain hemorrhage
Right pontine hemorrhage
Outcome
Excellent
Excellent
Bedridden
Excellent
Died of aspiration pneumonia
Excellent
pontine syndromes, and CT findings correlated closelywith the neurologic manifestations. Previous reportsstress the presence of arterial hypertension in 60-90%of the cases.125"7 In the present cases, 4 of 6 patientswere hypertensive. It is important to note oral amphet-amine ingestion in 1 patient. The association betweenintracerebral hemorrhage and the use of oral2423 orintravenous26 amphetamines has been noted, but to ourknowledge this is the first case of pontine hemorrhagesecondary to amphetamine abuse.
Another important feature of patients with lateralpontine hemorrhage is their good prognosis. In mostseries, a benign outcome was noted when conscious-ness was not severely impaired at admission.5"1318 Thetransverse diameter of the hematoma has also beenconsidered a prognostic factor. Masiyama et al8 founda direct relation between the maximum transverse di-ameter of the hematoma seen in CT scans and theoutcome. In their series, a diameter of < 2 0 mm wasassociated with favorable outcome.
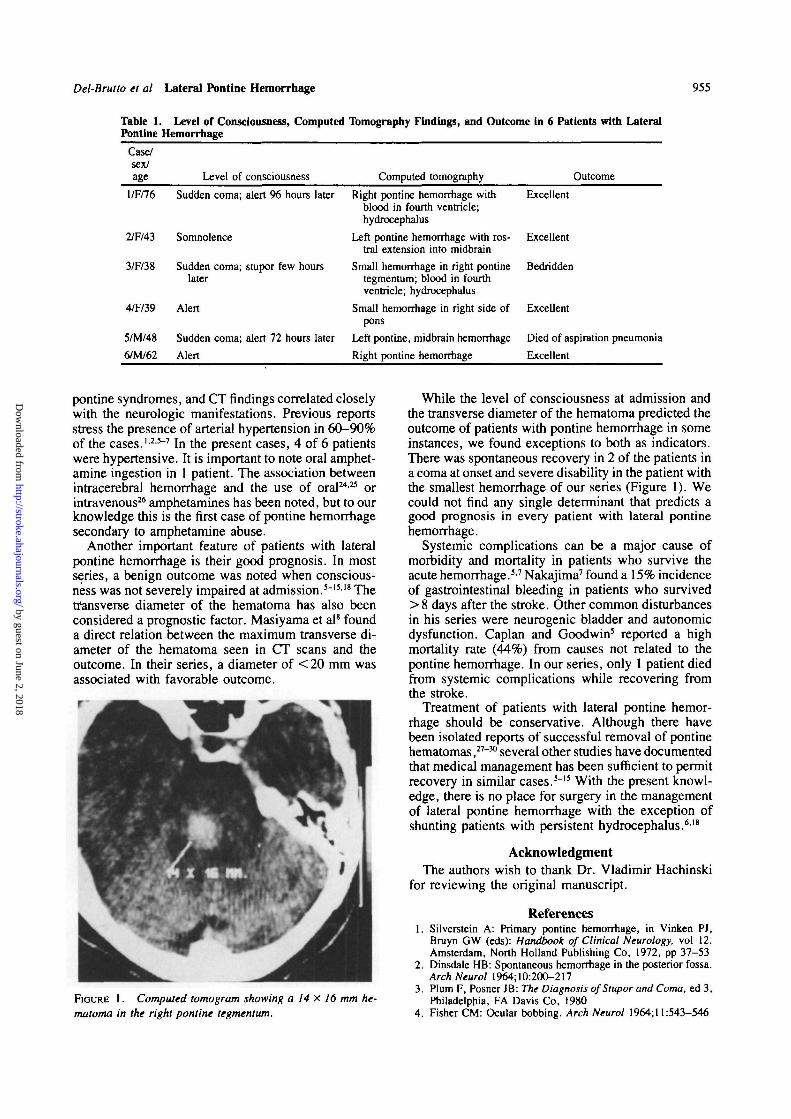
FIOURE 1. Computed tomogram showing a 14 x 16 mm he-matoma in the right pontine tegmentum.
While the level of consciousness at admission andthe transverse diameter of the hematoma predicted theoutcome of patients with pontine hemorrhage in someinstances, we found exceptions to both as indicators.There was spontaneous recovery in 2 of the patients ina coma at onset and severe disability in the patient withthe smallest hemorrhage of our series (Figure 1). Wecould not find any single determinant that predicts agood prognosis in every patient with lateral pontinehemorrhage.
Systemic complications can be a major cause ofmorbidity and mortality in patients who survive theacute hemorrhage.37 Nakajima7 found a 15% incidenceof gastrointestinal bleeding in patients who survived> 8 days after the stroke. Other common disturbancesin his series were neurogenic bladder and autonomicdysfunction. Caplan and Goodwin5 reported a highmortality rate (44%) from causes not related to thepontine hemorrhage. In our series, only 1 patient diedfrom systemic complications while recovering fromthe stroke.
Treatment of patients with lateral pontine hemor-rhage should be conservative. Although there havebeen isolated reports of successful removal of pontinehematomas,27"30 several other studies have documentedthat medical management has been sufficient to permitrecovery in similar cases.3"15 With the present knowl-edge, there is no place for surgery in the managementof lateral pontine hemorrhage with the exception ofshunting patients with persistent hydrocephalus.618
AcknowledgmentThe authors wish to thank Dr. Vladimir Hachinski
for reviewing the original manuscript.
References1. Silverstein A: Primary pontine hemorrhage, in Vinken PJ,
Bruyn GW (eds): Handbook of Clinical Neurology, vol 12.Amsterdam, North Holland Publishing Co, 1972, pp 37-53
2. Dinsdale HB: Spontaneous hemorrhage in the posterior fossa.ArchNeurol 1964; 10:200-217
3. Plum F, Posner JB: The Diagnosis of Stupor and Coma, ed 3,Philadelphia, FA Davis Co, 1980
4. Fisher CM: Ocular bobbing. Arch Neurol 1964; 11:543-546
by guest on June 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

956 Stroke Vol 18, No 5, September-October 1987
5. Caplan LR, Goodwin JA: Lateral tegmental brainstem hemor-rhages. Neurology 1982;32:252-260
6. Kushner MJ, Bressman SB: The clinical manifestations ofpon-tine hemorrhage. Neurology 1985;35:637-643
7. Nakajima K: Clinicopathological study of pontine hemor-rhage. Stroke 1983;14:485-492
8. Masiyama S, Niizuma H, Suzuki J: Pontine haemorrhage: Aclinical analysis of 26 cases. J Neurol Neurosurg Psychiatry1985;48:658-662
9. Lavi E, Rothman S, Reches A: Primary pontine hemorrhagewith complete recovery. Arch Neurol 1981;38:320
10. Kase CS, Maulsby GO, Mohr JP: Partial pontine hematomas.Neurology 1980;30:652-655
11. Gobernado JM, Fernandez de Molina AR, Gimeno A: Puremotor hemiplegia due to hemorrhage in the lower pons. ArchNeurol 1980;37:393
12. Tuhrim S, Yang WC, Rubinowitz H, Weinberger J: Primarypontine hemorrhage and the dysarthria-clumsy hand syn-drome. Neurology 1982;32:1027-1028
13. Schnapper RA: Pontine hemorrhage presenting as ataxic hemi-paresis. Stroke 1982;13:518-519
14. Kudo Y, Fukai M, Yamadori A: Asterixis due to pontine hem-orrhage. J Neurol Neurosurg Psychiatry 1985;48:487-489
15. Payne HA, Maravilla KR, Levinstone A, Heuter J, TindallRSA: Recovery from primary pontine hemorrhage. Ann Neurol1978;4:557-558
16. Portenoy RK, Kurtzberg D, Arezzo JC, Sands GH, Miller A,Vaughan HG: Return to alertness after brain-stem hemorrhage.Arch Neurol 1985;42:85-87
17. Pierrot-Deseilligni C, Chain F, Serdaeu M, Gray F, LhermitteF: The "one-and-a-half syndrome. Electrooculographic analy-ses of five cases with deductions about the physiologic mecha-nism of lateral gaze. Brain 1981; 104:665-699
18. Le Coz P, Woimant F, George B, Merland JJ, Haguenau M,Pepin B: Aspects cliniques et evolutifs des hematomes circon-scrits du tronc ce're'bral. Apport du scanner X. Rev Neurol(Paris) 1986;142:52-60
19. Cascino GD, Adams RD: Brainstem auditory hallucinosis.Neurology 1986;36:1042-1047
20. Goto N, Yamamoto T, Kaneko M, Tomita H: Primary pontinehemorrhage and gustatory disturbance: Clinicoanatomic study.Stroke 1983;14:507-511
21. Drury I, Whisnant JP, Garraway WM: Primary intracerebralhemorrhage: Impact of CT on incidence. Neurology 1984;34:653-657
22. Tyler H, Johnson P: Case records of the Massachusetts GeneralHospital, case: 36-1972. N Engl J Med 1972;287:506-512
23. Kase CS, Caplan LR: Hemorrhage affecting the brain stem andcerebellum, in Barnett HJM (ed): Stroke: Pathophysiology,Diagnosis, and Management, vol 1. New York, Churchill Liv-ingstone, 1986, pp 621-641
24. Harrington H, Heller HA, Dawson D, Caplan L, Rumbaugh C:Intracerebral hemorrhage and oral amphetamine. Arch Neurol1983 ;40:503-507
25. D'Souza T, Shraberg D: Intracerebral hemorrhage associatedwith amphetamine abuse. Neurology 1981;31:922-923
26. Lukes SA: Intracerebral hemorrhage from an arteriovenousmalformation after amphetamine injection. Arch Neurol 1983;40:60-61
27. Murphy MG: Successful evacuation of acute pontine hemato-ma. Case report. J Neurosurg 1972;37:224-225
28. Koss WT, Sunder-Plassmann M, Salah S: Successful removalof a large intrapontine hematoma. Case report. J Neurosurg1969;31:690-694
29. Kowada M, Yamaguchi K, Ito Z, Matsuoka S: Pneumoen-cephaloroulette tomography of operated primary pontinehaemorrhage with long survival: Report of two cases. J NeurolNeurosurg Psychiatry 1972;35:243-246
30. Burns J, Lisak R, Schut L, Silberberg D: Recovery followingbrainstem hemorrhage. Ann Neurol 1980;7:183—184
KEY WORDS • pontine hemorrhage • posterior fossahemorrhage • lateral brainstem hemorrhage • brainstemsyndromes
by guest on June 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

O H Del-Brutto, C A Noboa and F BarinagarrementeríaLateral pontine hemorrhage: reappraisal of benign cases.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1987 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.18.5.954
1987;18:954-956Stroke.
http://stroke.ahajournals.org/content/18/5/954World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from