

Latent Tuberculosis Infection
40
© National HIV Curriculum PDF created January 7, 2022, 7:08 pm Latent Tuberculosis Infection This is a PDF version of the following document: Module 4: Co-Occurring Conditions Lesson 1: Latent Tuberculosis Infection You can always find the most up to date version of this document at https://www.hiv.uw.edu/go/co-occurring-conditions/latent-tuberculosis/core-concept/all . Background Epidemiology of Tuberculosis in the United States Although the incidence of tuberculosis in the United States has substantially decreased since the early 1990s (Figure 1 ), tuberculosis continues to occur at a significant rate among certain populations, including persons from tuberculosis-endemic settings, individual in correctional facilities, persons experiencing homelessness, persons who use drugs, and individuals with HIV.[1 ,2 ] In recent years, the majority of tuberculosis cases in the United States were among the persons who were non-U.S.-born (71% in 2019), with an incidence rate approximately 16 times higher than among persons born in the United States (Figure 2 ).[2 ] Cases of tuberculosis in the United States have occurred at higher rates among persons who are Asian, Hispanic/Latino, or Black/African American (Figure 3 ).[1 ,2 ] In the general United States population, the prevalence of latent tuberculosis infection (LTBI) is estimated between 3.4 to 5.8%, based on the 2011 and 2012 National Health and Nutrition Examination Survey (NHANES).[3 ,4 ] Another study estimated LTBI prevalence within the United States at 3.1%, which corresponds to 8.9 million persons living with latent TB; this LTBI prevalence estimate was calculated using surveillance data of active tuberculosis cases from 2011 through 2015, at the state and local level, along with assumptions on rates of LTBI reactivation.[5 ] These data also demonstrate the geographic variability of LTBI in the United States, with some counties at less than 1% prevalence and some with greater than 3%.[5 ] The prevalence of LTBI among persons with HIV sampled in NHANES was 7.6%.[4 ] Epidemiology of Tuberculosis in Persons with HIV In the late 1980s and early 1990s, HIV contributed to the significant increase of tuberculosis in the United States (48% of tuberculosis cases occurred in persons with HIV coinfection in 1993).[6 ] In the last 10 years, the overall number (Figure 4 ) and proportion (Figure 5 ) of tuberculosis cases involving persons who had HIV coinfection substantially decreased.[2 ] For 2019, the CDC reported that HIV status was known for 90.7% of the persons diagnosed with tuberculosis and among those with known HIV status, 4.7% had HIV coinfection.[2 ] In contrast to the overall decline of new tuberculosis cases in persons with HIV, the incidence of tuberculosis among persons with HIV who are non-U.S.-born has remained stable.[7 ,8 ] Tuberculosis continues to cause significant morbidity and mortality among people with HIV in the United States and other low tuberculosis burden areas.[7 ,9 ] The risk of mortality among individuals with HIV who develop tuberculosis is higher than those with tuberculosis alone, even in the era of readily available antiretroviral therapy,[9 ] highlighting the importance of tuberculosis prevention in those with HIV.[10 ] Page 1/40
Transcript of Latent Tuberculosis Infection
© National HIV CurriculumPDF created January 7, 2022, 7:08 pm
Latent Tuberculosis Infection
This is a PDF version of the following document:Module 4: Co-Occurring ConditionsLesson 1: Latent Tuberculosis Infection
You can always find the most up to date version of this document athttps://www.hiv.uw.edu/go/co-occurring-conditions/latent-tuberculosis/core-concept/all.
Background
Epidemiology of Tuberculosis in the United States
Although the incidence of tuberculosis in the United States has substantially decreased since the early 1990s(Figure 1), tuberculosis continues to occur at a significant rate among certain populations, including personsfrom tuberculosis-endemic settings, individual in correctional facilities, persons experiencing homelessness,persons who use drugs, and individuals with HIV.[1,2] In recent years, the majority of tuberculosis cases inthe United States were among the persons who were non-U.S.-born (71% in 2019), with an incidence rateapproximately 16 times higher than among persons born in the United States (Figure 2).[2] Cases oftuberculosis in the United States have occurred at higher rates among persons who are Asian,Hispanic/Latino, or Black/African American (Figure 3).[1,2]
In the general United States population, the prevalence of latent tuberculosis infection (LTBI) is estimatedbetween 3.4 to 5.8%, based on the 2011 and 2012 National Health and Nutrition Examination Survey(NHANES).[3,4] Another study estimated LTBI prevalence within the United States at 3.1%, which correspondsto 8.9 million persons living with latent TB; this LTBI prevalence estimate was calculated using surveillancedata of active tuberculosis cases from 2011 through 2015, at the state and local level, along withassumptions on rates of LTBI reactivation.[5] These data also demonstrate the geographic variability of LTBIin the United States, with some counties at less than 1% prevalence and some with greater than 3%.[5] Theprevalence of LTBI among persons with HIV sampled in NHANES was 7.6%.[4]
Epidemiology of Tuberculosis in Persons with HIV
In the late 1980s and early 1990s, HIV contributed to the significant increase of tuberculosis in the UnitedStates (48% of tuberculosis cases occurred in persons with HIV coinfection in 1993).[6] In the last 10 years,the overall number (Figure 4) and proportion (Figure 5) of tuberculosis cases involving persons who had HIVcoinfection substantially decreased.[2] For 2019, the CDC reported that HIV status was known for 90.7% ofthe persons diagnosed with tuberculosis and among those with known HIV status, 4.7% had HIVcoinfection.[2] In contrast to the overall decline of new tuberculosis cases in persons with HIV, the incidenceof tuberculosis among persons with HIV who are non-U.S.-born has remained stable.[7,8]
Tuberculosis continues to cause significant morbidity and mortality among people with HIV in the UnitedStates and other low tuberculosis burden areas.[7,9] The risk of mortality among individuals with HIV whodevelop tuberculosis is higher than those with tuberculosis alone, even in the era of readily availableantiretroviral therapy,[9] highlighting the importance of tuberculosis prevention in those with HIV.[10]
Page 1/40

Progression from LTBI to Active TB
Development of tuberculosis disease can occur in the setting of recent exposure to Mycobacteriumtuberculosis (primary or active disease) or with reactivation of LTBI.[11,12] The development of tuberculosisdisease is based on complex interactions between host immune status and the bacillary load; in persons withHIV, this balance is impacted both by HIV-related immunosuppression and restoration of immune function byantiretroviral therapy (Figure 6).[11]
Investigators have identified several comorbidities that contribute to the risk of developing active disease,including HIV infection, diabetes, malnutrition, low body weight, smoking, lung disease, drug use, and recentor current use of immunosuppressant medications.[13] The risk of progression from LTBI to active disease ismarkedly increased in individuals infected with HIV (3 to 16% per year) compared with those uninfected (5 to10% lifetime risk).[10,14,15] The increased risk of LTBI reactivation begins soon after acquisition of HIV.[16]
Prevention of Tuberculosis in Persons with HIV
Combination antiretroviral therapy decreases the risk of developing active tuberculosis disease byapproximately 67%, with greater declines in tuberculosis occurring with more substantial increases in CD4cell counts and longer duration of antiretroviral therapy.[17] Nevertheless, the risk of incident tuberculosisremains significantly higher among those with HIV compared to those without HIV, even after CD4 recoveryon antiretroviral therapy, or initiation of antiretroviral therapy at higher CD4 cell counts.[18] Identifying thosewith LTBI who may benefit from treatment to prevent tuberculosis disease is an important part of tuberculosisprevention in people with HIV.[10]
Individuals with HIV who have positive LTBI testing, either tuberculin skin test (TST) or interferon gammarelease assay (IGRA), are associated with increased risk of progression to active tuberculosis.[19,20,21,22]Among persons with HIV who have a positive tuberculin skin test, treating LTBI significantly decreases theirrisk of developing active tuberculosis and mortality (62% and 26% reduction, respectively).[23,24,25] Thecombination of antiretroviral therapy and LTBI treatment decreases the risk of tuberculosis more than eitherintervention alone.[26]
Page 2/40

Rationale and Indications for LTBI Screening
Rationale for LTBI Screening
Multiple factors underscore the rationale for LTBI screening in persons with HIV, including increased risk ofprogression from LTBI to tuberculosis, poor outcomes associated with active tuberculosis disease, availabilityof screening tests to identify those with LTBI, and effective treatment for LTBI to prevent progression to activetuberculosis disease. For all these reasons, individuals with HIV should be routinely screened and offeredtreatment if found to have LTBI.[10,27]
Indication and Timing of LTBI Screening
The Adult and Adolescent Opportunistic Infection Guidelines recommends screening for LTBI at the time ofinitial HIV diagnosis or entry into medical care, regardless of the presence or absence of other epidemiologictuberculosis risk factors.[10,28] Despite this recommendation, adherence to recommendations for LTBIscreening of persons with HIV in the United States has been variable, with reports of adherence to routinescreening practices ranging from 47 to 79%.[29,30,31,32] Recent contact with a known tuberculosis caseshould prompt LTBI screening, evaluation for active disease, and empiric therapy for latent tuberculosis ifthere is no evidence of active tuberculosis.
Repeat LTBI Screening
Individuals with advanced HIV disease (CD4 count less than 200 cells/mm3) with initially negative LTBI testingshould have repeat testing after they initiate antiretroviral therapy and reach a CD4 count of at least 200cells/mm3, due to the possibility of false-negative results in the setting of advanced immunosuppression.[10]Yearly repeat testing for LTBI is recommended only in situations when individuals with HIV have high risk forongoing or repeat exposure to persons with active tuberculosis.[10]
Page 3/40

Methods Used to Test for Latent TuberculosisThere are two primary methods for detection of LTBI: tuberculin skin test and interferon gamma release assay(IGRA).[33,34] Both methods are indirect measures of tuberculosis infection that for a positive test resultrequire infection with M. tuberculosis and the host’s ability to mount a T-cell mediated response. The testsdiffer in that tuberculin skin testing is an in-vivo skin test, while IGRA is an in-vitro blood-based approach.[35]Routine dual testing with both the tuberculin skin test and IGRA is not recommended, though CDC guidelinesrecommend that repeat testing (with the other test) may be appropriate when the initial test was negative inpersons at high risk for tuberculosis infection.[31] Importantly, a positive tuberculin skin test or IGRA does notdistinguish between LTBI and active disease, nor does negative LTBI testing rule out active tuberculosis. Afterinfection with M. tuberculosis, the TST and IGRA tests may not become positive for 2 to 10 weeks.
Tuberculin Skin Test
The Mantoux tuberculin skin testing method consists of giving an intradermal injection of 5 tuberculin units ofpurified protein derivative that contains M. tuberculosis antigens (Figure 7) and then evaluating thecutaneous induration 48 to 72 hours later.[33] In persons infected with M. tuberculosis (past or current),intradermal injection of the PPD will stimulate a T-lymphocyte mediated type IV delayed hypersensitivityresponse, leading to induration of the site of injection within 48 to 72 hours.[35] The transverse diameter ofinduration (not erythema) should be measured at a follow-up visit 48 to 72 hours after placement of the PPDand should be performed by an individual trained in reading a tuberculin skin test (Figure 8).[33]
Criteria for Positive Tuberculin Skin Test: For individuals with HIV, induration of 5 mm or greateris considered a positive test.[28] Following exposure to M. tuberculosis, the tuberculin skin testconversion to positive typically occurs within 8 weeks.[36] The sensitivity of tuberculin skin test forthe diagnosis of LTBI is estimated at 45 to 85% and specificity at approximately 85%.[31,37,38]Persons with prior treatment of tuberculosis (latent or active) typically have a persistently positivetuberculin skin test.False-Positive Tuberculin Skin Test: Previous exposure to nontuberculous mycobacteria, as wellas immunization with bacille Calmette–Guérin (BCG), can cause a false-positive tuberculin skintest.[34] Receipt of BCG in infancy is thought to have a relatively minimal effect on tuberculin skintesting, especially if at least 10 years have elapsed after administration.[39]False-Negative Tuberculin Skin Test: False-negative tests can occur in the setting of advancedHIV disease, malnutrition, active tuberculosis or early in the window period after recent M.tuberculosis infection.[34]
Interferon Gamma Release Assay (IGRA)
For the diagnosis of LTBI, the two most commonly used FDA approved interferon gamma releaseassays (IGRAs) in the United States are the QuantiFERON-TB Gold Plus (QFT-Plus) assay and the T-SPOT.TB (T-SPOT) assay (Figure 9).[31] The QFT-Plus and T-SPOT are in vitro tests that measure the release of interferongamma by T-lymphocytes after stimulation to a peptide antigen cocktail that simulates two M. tuberculosisspecific antigens: early secreted antigenic target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10).[34,40,41]The ESAT-6 and CFP-10 mycobacterial antigens are absent from all mycobacterial strains used in BCGvaccines and from most nontuberculous mycobacteria, except for M. marinum, M. kansasii, and M.szulgai.[34]
QuantiFERON-TB Gold Plus (QFT-Plus): This test has replaced the QuantiFERON-TB Gold test andhas the advantage of measuring both CD4 and CD8 T-lymphocyte responses.[42,43,44] To performthe test, blood is drawn into 4 specialized collection tubes: (1) Nil (negative control), (2) mitogen(positive control), (3) TB1 (primarily detects CD4 T cell response), and (4) TB2 (optimized for detectionof CD4 and CD8 T cell responses) (Figure 10).[42,45,46,47] The interferon gamma response isquantified in international units (IU) per millimeter and test results are reported as positive, negative,
Page 4/40

or indeterminate (Figure 11).[45] Reversion from a positive to negative test result canoccur,[48,49,50] but this tends to occur when the initial test is close to the cutoff threshold.[34,42,46]Initial studies using the QFT-Plus assay indicate concordance with QFT results for several settings,including active tuberculosis cases, individuals with recent exposure to M. tuberculosis, and inhealthcare workers from areas of low tuberculosis incidence.[42,46,47,51]T-SPOT.TB (T-SPOT): The T-SPOT is an enzyme-linked immunosorbent spot (ELISPOT) assay thatquantitates the response of mononuclear T-cells to M. tuberculosis antigens. First, a blood sample isobtained and peripheral blood mononuclear cells are separated from whole blood and counted. Theperipheral blood mononuclear cells are then placed into microtiter wells pre-coated with high affinityantibodies to interferon-gamma; four different panels are set up by coincubating with either M.tuberculosis ESAT-6 antigens (Panel A), M. tuberculosis CFP10 antigens (Panel B), positive control thatcontains phytohemagglutinin (Panel C), or Nil negative control (Panel D).[52] The number of T-cellsproducing interferon gamma (spot-forming cells) are then counted (Figure 12). The test results arecategorized as either positive, borderline, negative, or indeterminate (Figure 13).[31] In a meta-analysis of IGRA studies in persons with HIV, the pooled sensitivity was 72% for T-SPOT and 61% forQFT.[53]
Performance of IGRA Tests
The presence of immunosuppression decreases the sensitivity of IGRAs, but the impact is relatively less thanon the tuberculin skin test.[34] In addition, the IGRA tests have greater specificity than the tuberculin skintest and these tests are not impacted by prior receipt of BCG vaccine.[10] Although IGRA testing requires ablood draw, unlike tuberculin skin testing, it does not require a follow-up visit for test result reading. Inaddition, IGRA cutoffs are not stratified by risk-group, including HIV status. Persons with prior treatment ofLTBI or active tuberculosis (and a prior positive IGRA) usually have persistently positive IGRAs. Similar to TST,the IGRA tests may be negative early in the window period after recent M. tuberculosis infection.
Page 5/40

Recommended LTBI Testing in Persons with HIV
Choice of Test Method For LTBI Screening
Use of either tuberculin skin test or IGRA is appropriate for LTBI screening in persons with HIV.[10,31,33] Thecorrelation between positive tuberculin skin test and IGRA in persons with HIV is poor tomoderate.[22,53,54,55] In recent years, many clinics have predominantly used IGRAs because of severalnegative aspects of tuberculin skin testing, including the requirement for a second visit to read the test, false-positive results in people immunized with BCG vaccine, and lower sensitivity in persons with advancedimmunosuppression. Some experts acknowledge the benefit of performing a second LTBI diagnostic test (e.g.a tuberculin skin test after a negative IGRA result or vice versa) as a strategy to increase sensitivity in thesetting of an individual likely to be infected and at high risk of progression to active disease. From a practicalstandpoint, the decision regarding which test to use is often based on a combination of the availability of thetest, trained staff, lab capability, and likelihood of patient follow-up for a second visit to read a tuberculin skintest.
LTBI TESTING IN PERSONS WITH HIV
The Adult and Adolescent Opportunistic Infection Guidelines recommendations regarding testing for LTBI inpersons with HIV are summarized as follows:[10]
All persons with HIV should undergo testing for LTBI at the time of HIV diagnosis, regardless of theirepidemiological risk of TB exposure.The tuberculin skin test or IGRA can be used as the screening method for LTBI and the decision forwhich one to use may be based on likelihood of patient follow-up for reading a tuberculin skin test.Annual testing for LTBI is recommended for persons with HIV who are at high risk for repeated orongoing exposure to persons with active TB.Persons with HIV and advanced immunosuppression (CD4 count less than 200 cells/mm3) who havenegative tuberculin skin test result should undergo repeat testing for latent tuberculosis infection afterthey start on antiretroviral therapy and have an increase in CD4 count to 200 cells/mm3 or greater.The routine use of both tuberculin skin test and IGRAs to screen for LTBI is not routinelyrecommended, though some experts recommend dual testing to increase the sensitivity in individualswho have a high likelihood of having infection with M. tuberculosis and a high risk of progression toactive disease.All persons with a positive tuberculin skin test or IGRA should be evaluated for the possibility of activeTB disease.
Page 6/40

Evaluation of Persons with a Positive LTBI Screening TestAny individual with HIV who has a new positive LTBI screening test should undergo tuberculosis symptomscreening as well as chest radiography to exclude active tuberculosis disease.[29] A meta-analysis ofindividual participant data of more than 8,000 persons with HIV found that having at least one positivesymptom in a 4-symptom tuberculosis screen (cough, fever, weight loss, or night sweats) has sensitivity78.9%, specificity 49.6%, and negative predictive value of 97.7% (at a 5% prevalence) to identify those withculture-confirmed pulmonary tuberculosis.[56] A more recent systematic review and meta-analysis thatincluded 1,599 people with active tuberculosis found this 4-symptom tuberculosis screen had a lower pooledsensitivity for people on antiretroviral therapy than for those not on antiretroviral therapy (51.0% versus89.4%). The pooled specificity was much higher for those on antiretroviral therapy (70.7%) than in personswho were antiretroviral therapy-naive (28.1%).[57] Sputum examination, including acid fast smearmicroscopy and culture is indicated for those with either an abnormal chest radiograph or a positive symptomscreen (even if their chest radiograph is negative).[58] The Adult and Adolescent Opportunistic InfectionGuidelines recommend that in a low burden setting such as in the United States, routine use of sputumculture to screen for tuberculosis in asymptomatic individuals with a negative chest radiograph is notconsidered cost-effective.[10]
Page 7/40
Management of LTBI in Persons with HIV
Indications for LTBI
A positive tuberculin skin test or IGRA is associated with a significantly increased risk of developingtuberculosis disease.[22,53,54,55] The risk of progression to active tuberculosis disease is even higher amongrecent LTBI test converters.[54,59,60] Some studies indicate a positive IGRA is a stronger predictor thantuberculin skin test for the risk of developing tuberculosis disease.[61,62] All individuals with HIV who have anew positive testing for LTBI and a negative workup for active tuberculosis should be offered LTBItreatment.[10] In addition, individuals with HIV who have close contact with an active tuberculosis caseshould receive treatment for latent tuberculosis infection after active tuberculosis has been excluded,irrespective of LTBI test result. A history of BCG vaccination should not affect the decision whether to treatLTBI in persons with HIV.
Regimens for LTBI
The following summarizes recommendations in the Adult and Adolescent Opportunistic InfectionGuidelines and Adult and Adolescent ARV Guidelines preferred and alternative regimens for the treatment ofLTBI in adults with HIV (Table 1).[10,63] In the situation where a patient has evidence of LTBI and a history ofexposure to a person with drug-resistant tuberculosis, the clinician should consult with a tuberculosis expertto determine an appropriate regimen for the treatment of LTBI. The choice for the LTBI regimen shouldstrongly consider the individual’s antiretroviral regimen.[63]
Preferred Therapies for LTBI
Isoniazid for 6 Months (6H) or 9 Months (9H): The standard-length treatments for LTBI in personswith HIV are isoniazid 300 mg daily for 6 or 9 months, given with pyridoxine 25 to 50 mg daily.[10,63]These regimens are referred to as 6H and 9H since they consist of taking 6 or 9 months of isoniazid(INH). The pyridoxine (vitamin B6) is given to reduce the risk of isoniazid-induced peripheralneuropathy.[10]
Interactions with Antiretroviral Medications: Isoniazid has few drug interactions withantiretroviral medications.[10,63] With the daily 6H or 9H regimen, any antiretroviral regimencan be used and no dose adjustments are required.
Isoniazid plus Rifapentine for 3 Months (3HP): This short-course 3-month regimen consists ofweekly rifapentine (weight-based dosing, maximum dose of 900 mg) plus isoniazid (15 mg/kg,maximum weekly dose of 900 mg); pyridoxine 50 mg weekly is also added to prevent isoniazid-induced peripheral neuropathy.[10,27,63,64] A total of 12 doses are given. This regimen is commonlyreferred to as 3HP, with this designation based on the regimen duration (3 months) using isoniazid(INH) and rifapentine (RPT). The 3HP regimen has efficacy equal to standard isoniazid monotherapy,with the added benefit of likely improved adherence due to shorter duration.[64,65,66] In arandomized trial from three African countries that compared three different LTBI regimens inapproximately 4,000 persons with HIV, the 3HP regimen was associated with higher treatmentcompletion rates compared to daily isoniazid for tuberculosis prevention.[67]
Interactions with Antiretroviral Medications: With the 3HP regimen, the limited antiretroviralregimen options consist of an anchor drug efavirenz 600 mg once daily, raltegravir 400 mgtwice daily, or dolutegravir 50 mg once daily (for those in whom once-daily dolutegravir isappropriate) in combination with the backbone drugs tenofovir DF-emtricitabine or abacavir-lamivudine.[10,63] When 3HP was given to 60 adults with HIV who were taking once dailydolutegravir as part of their antiretroviral regimen, suppressed HIV RNA levels weremaintained, despite a 50 to 60% reduction in dolutegravir serum trough levels.[68] Rifapentineshould not be given to adults who require twice daily dosing of dolutegravir, such as thosewith clinically suspected or proven integrase inhibitor resistance.[10,63] Concurrent use oftenofovir alafenamide and rifapentine is not recommended unless the benefit outweigh the
Page 8/40

risks.[10,27,63,64] The antiretroviral regimen bictegravir-tenofovir alafenamide-emtricitabineshould be avoided with rifapentine due to reduced plasma concentrations of bictegravir.[69]
Rifampin for 4 Months (4R): This short-course 4-month regimen, which consists of rifampin 600 mgdaily, is referred to as 4R, based on 4 months of rifampin (RIF).[10,63,70] In a recent largeinternational open label clinical trial that enrolled persons with and without HIV, investigatorsdemonstrated 4 months of rifampin was non-inferior to 9 months of isoniazid for the treatment ofLTBI.[71] Furthermore, the rifampin regimen cohort had higher rates of treatment completion andfewer adverse effects.[71] Among all study participants, only 4% had HIV.[71] Accordingly, caution isneeded when attempting to generalize these results for the treatment of LTBI in persons with HIV.
Interactions with Antiretroviral Medications: The use of rifampin is not recommended for use inpersons receiving an antiretroviral regimen that contains a protease inhibitor, doravirine,etravirine, rilpivirine, or elvitegravir-cobicistat.[10,63] If dolutegravir is used in combinationwith rifampin, the dose should be increased to 50 mg twice daily. Raltegravir, whencoadministered with rifampin, should be increased to 800 mg twice daily. The regimenbictegravir-tenofovir alafenamide-emtricitabine should be avoided with rifampin due toreduced plasma concentrations of bictegravir.[69]
Alternative Therapy for LTBI
Isoniazid plus Rifapentine Daily for 1 month (1HP): This short-course regimen, which is analternative regimen, consists of isoniazid 300 mg daily plus daily weight-based rifapentine (maximum600 mg), with pyridoxine 25 to 50 mg daily to prevent peripheral neuropathy.[63] In the BRIEF-TB/A5279 trial, a short-course 1-month regimen of daily isoniazid plus rifapentine was noninferior to 9months of isoniazid alone in preventing tuberculosis in persons with HIV who were taking efavirenz- ornevirapine-based antiretroviral therapy, with fewer adverse events, and higher completion rates.[72]The 1-month regimen of daily isoniazid plus daily rifapentine is referred to as 1HP (1 month, INH,RPT).
Interactions with Antiretroviral Medications: With the use of daily rifapentine in the 1HPregimen, the only recommended antiretroviral regimens are efavirenz 600 mg daily incombination with either tenofovir DF-emtricitabine or abacavir-lamivudine.[10] Studies areongoing regarding PK and safety with coadministration with dolutegravir.
Medication-Related Adverse Effects
Individuals on LTBI therapy should undergo clinical monitoring on a monthly basis. Isoniazid is associated withan increased risk of hepatitis, particularly in patients with older age, alcohol use, and pregnancy.[73,74] Inaddition, they should receive education on the signs and symptoms of hepatitis (jaundice, abdominaldiscomfort, nausea and vomiting) and be advised to promptly stop isoniazid and report their symptoms totheir provider if they occur. Baseline hepatic aminotransferase levels should be obtained. Individuals atincreased risk of hepatotoxicity, including those with abnormal baseline tests, persons who are pregnant,persons with hepatitis B or C coinfection, or those receiving antiretroviral therapy, should have routine labmonitoring during treatment with isoniazid.[10] The Adult and Adolescent Opportunistic Infection Guidelinesrecommend withholding isoniazid if the hepatic aminotransferase level exceeds three times the upper limit ofnormal (with associated symptoms) or five times the upper limit of normal (with or without associatedsymptoms).[10] The 2-month short course regimen of rifampin and pyrazinamide has been studied, but thisregimen has an unacceptably high risk of causing severe liver injury and thus should never be used fortreatment of latent TB.[10,75,76]
Management with Missed Doses or Treatment Interruption
If interruptions were frequent or prolonged enough to preclude completion of treatment within therecommended time frame, therapy should be extended or restarted. When treatment has been interruptedfor more than 2 months, the patient should be reevaluated for tuberculosis.
Page 9/40

Page 10/40

Considerations in Special Populations
LTBI in Pregnancy
Screening for LTBI in Pregnancy
All pregnant persons with HIV who have not had previous screening for LTBI (or who are at high risk ofexposure to individuals with active tuberculosis) should have testing for LTBI during pregnancy.[10] Althoughdata remain conflicting whether pregnancy stage affects both TST and IGRA testing,[77,78,79] either test isconsidered appropriate for screening in pregnancy.
Treatment of LTBI in Pregnancy
Based on studies that demonstrating adverse pregnancy outcomes in individuals with HIV who receivedisoniazid for LTBI treatment during pregnancy, the Adult and Adolescent Opportunistic Infection Guidelinesnow recommend delaying isoniazid LTBI until the postpartum period, unless the pregnant woman reportssignificant close contact with an active TB case or the clinician believes that the risk of developing active TBoutweighs the risk of adverse birth outcomes.[10,80] Although isoniazid is not considered teratogenic, datafrom two randomized-controlled trials suggest that persons who are pregnant or in the postpartum periodmay have a higher risk for isoniazid-associated hepatotoxicity.[80,81] In contrast, two recent observationalstudies from South African have demonstrated no hepatotoxicity and improved pregnancy outcomes inwomen with HIV on antiretroviral therapy who are given isoniazid for LTBI.[82,83] If LTBI therapy is requiredduring in pregnancy, the recommended regimen is isoniazid, given with pyridoxine.[10] There are inadequatedata for the use of rifampin or rifapentine. Although animal data with rifapentine suggest this medication maycause congenital malformations and fetal loss, a more recent Phase I/II study that evaluated thepharmacokinetics and safety of 3HP among pregnant women with or without HIV did not report anyadverse drug-related adverse events.[84,85,86] In this same Phase I/II study, investigators found that womentaking efavirenz had a higher clearance of rifapentine than expected during pregnancy.[86]
Treatment of LTBI in Persons with Liver Disease
Individuals with chronic liver disease are at increased risk of LTBI treatment-associated hepatitis. Activehepatitis and end-stage liver disease are relative contraindications for LTBI treatment. Isoniazid or rifampinhave been used in this population in the setting of stable liver disease, but close clinical and laboratorymonitoring is recommended.[87] In addition, management of LTBI in a patient with chronic liver diseaseshould involve consultation with a tuberculosis expert.
LTBI in Children
Screening for LTBI in Children
The risk of progression from M. tuberculosis infection to active tuberculosis disease is high in children: 50% inthose younger than 1 year, 20 to 30% at age 1 to 2 years, and 10 to 20% in those older than 10 years.[88]Most tuberculosis disease in young children is due to primary infection.[89] All children with HIV should bescreened for LTBI.[90] The American Academy of Pediatrics recommends using tuberculin skin testing forscreening in children younger than 2 years of age.[91] Measles vaccine can temporarily suppress thetuberculin skin test reactivity for 4 to 6 weeks. The effect of other live virus vaccines (varicella, yellow fever,live-attenuated influenza) in tuberculin skin test and IGRA testing is unknown. Therefore, tuberculin skin testsand IGRAs should either be performed the same day as these vaccines are administered, or delayed for atleast 6 weeks after live vaccine administration.
Treatment of LTBI in Children
A 9-month course of isoniazid is the recommended treatment of LTBI in children with HIV who are 2 through
Page 11/40

11 years of age.[90] Pyridoxine supplementation (1 to 2 mg/kg, maximum 50 mg/day) is recommended for allchildren with HIV who are taking isoniazid.[90] The use of sorbitol-based liquid preparations of isoniazidshould be avoided if possible due to increased abdominal cramping and diarrhea. Tablets can be crushed orcapsules opened and the contents placed in food if necessary. Rifampin may be used in the setting ofisoniazid intolerance or known exposure to an isoniazid-resistant tuberculosis case; in these situations therecommended treatment length with rifampin is 6 months. The 3HP regimen is not recommended for childrenyounger than 2 years of age or in children with HIV on antiretroviral therapy.[84,90] The CDC and National TBController’s Association conditionally recommend 3 months of daily isoniazid (10 to 20 mg/kg, maximum 300mg/day) plus rifampin (15 to 20 mg/kg, maximum 600 mg/day) as an option for the treatment of latenttuberculosis in children with HIV, as permitted by drug interactions.[27] This 3-month regimen is not currentlyrecommended in the Pediatric Opportunistic Infection Guidelines.[90]
Page 12/40

Summary Points
Despite declining incidence of tuberculosis in the United States, individuals with HIV remain atsignificant risk for tuberculosis.Compared to people without HIV, individuals with HIV are at increased risk for tuberculosis, even whentaking antiretroviral therapy.All individuals with HIV should undergo screening for LTBI at either the time of HIV diagnosis or entryinto care.Testing for LTBI should be performed with either a tuberculin skin test or IGRA test. Limitations totuberculin skin testing include requirement of a second visit to read the test, lower specificityespecially in people immunized with BCG vaccine, and potentially lower sensitivity with advancedimmunosuppression.Severe immunosuppression can lead to false-negative LTBI tests; therefore, LTBI screening should berepeated once CD4 counts increase to at least 200 cells/mm3 on antiretroviral treatment.All individuals with HIV and positive LTBI screening tests should be offered LTBI treatment, after activetuberculosis has been ruled out.All individuals with HIV and a recent exposure to a person with active tuberculosis should be offeredLTBI treatment, irrespective of tuberculin skin test and/or IGRA results.The preferred standard-length regimen for LTBI treatment in persons with HIV is daily isoniazid for 6 or9 months. The preferred short-course regimens for LTBI consist of a 3- month course of weeklyisoniazid plus rifapentine or a 4-month course of daily rifampin. Alternative LTBI regimen for persons with HIV consists of a 1-month course of daily isoniazid plusrifapentine.
Page 13/40

Citations
1. Centers for Disease Control (CDC). Health Disparities in TB 2013.[CDC] -
2. Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA: U.S.Department of Health and Human Services, CDC.[CDC] -
3. Ghassemieh BJ, Attia EF, Koelle DM, Mancuso JD, Narita M, Horne DJ. Latent Tuberculosis Infection TestAgreement in the National Health and Nutrition Examination Survey. Am J Respir Crit Care Med.2016;194:493-500.[PubMed Abstract] -
4. Miramontes R, Hill AN, Yelk Woodruff RS, et al. Tuberculosis Infection in the United States: PrevalenceEstimates from the National Health and Nutrition Examination Survey, 2011-2012. PLoS One.2015;10:e0140881.[PubMed Abstract] -
5. Haddad MB, Raz KM, Lash TL, et al. Simple Estimates for Local Prevalence of Latent TuberculosisInfection, United States, 2011-2015. Emerg Infect Dis. 2018;24:1930-3.[PubMed Abstract] -
6. Centers for Disease Control and Prevention. TB Incidence in the United States, 1953-2013 Atlanta,Georgia: CDC; 2013.[CDC] -
7. Albalak R, O'Brien RJ, Kammerer JS, et al. Trends in tuberculosis/human immunodeficiency viruscomorbidity, United States, 1993-2004. Arch Intern Med. 2007;167:2443-52.[PubMed Abstract] -
8. Trieu L, Li J, Hanna DB, Harris TG. Tuberculosis rates among HIV-infected persons in New York City,2001-2005. Am J Public Health. 2010;100:1031-4.[PubMed Abstract] -
9. Metcalfe JZ, Porco TC, Westenhouse J, et al. Tuberculosis and HIV co-infection, California, USA,1993–2008. Emerg Infect Dis. 2013;19:400-6.[PubMed Abstract] -
10. Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the preventionand treatment of opportunistic infections in adults and adolescents with HIV: recommendations fromthe Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV MedicineAssociation of the Infectious Diseases Society of America. Mycobacterium tuberculosis infection anddisease. Last update: September 27, 2019.[HIV.gov] -
11. Lawn SD, Wood R, Wilkinson RJ. Changing concepts of "latent tuberculosis infection" in patients livingwith HIV infection. Clin Dev Immunol. 2011;2011. pii: 980594.[PubMed Abstract] -
12. Drain PK, Bajema KL, Dowdy D, et al. Incipient and Subclinical Tuberculosis: a Clinical Review of EarlyStages and Progression of Infection. Clin Microbiol Rev. 2018;31(4). pii: e00021-18.[PubMed Abstract] -
Page 14/40

13. Horsburgh CR Jr, Rubin EJ. Clinical practice. Latent tuberculosis infection in the United States. N Engl JMed. 2011;364:1441-8.[PubMed Abstract] -
14. Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk of tuberculosis among intravenousdrug users with human immunodeficiency virus infection. N Engl J Med. 1989;320:545-50.[PubMed Abstract] -
15. Comstock GW, Livesay VT, Woolpert SF. The prognosis of a positive tuberculin reaction in childhoodand adolescence. Am J Epidemiol. 1974;99:131-8.[PubMed Abstract] -
16. Sonnenberg P, Glynn JR, Fielding K, Murray J, Godfrey-Faussett P, Shearer S. How soon after infectionwith HIV does the risk of tuberculosis start to increase? A retrospective cohort study in South Africangold miners. J Infect Dis. 2005;191:150-8.[PubMed Abstract] -
17. Lawn SD, Wood R, De Cock KM, Kranzer K, Lewis JJ, Churchyard GJ. Antiretrovirals and isoniazidpreventive therapy in the prevention of HIV-associated tuberculosis in settings with limited health-care resources. Lancet Infect Dis. 2010;10:489-98.[PubMed Abstract] -
18. Kufa T, Mabuto T, Muchiri E, et al. Incidence of HIV-associated tuberculosis among individuals takingcombination antiretroviral therapy: a systematic review and meta-analysis. PLoS One.2014;9:e111209.[PubMed Abstract] -
19. Aichelburg MC, Rieger A, Breitenecker F, et al. Detection and prediction of active tuberculosis diseaseby a whole-blood interferon-gamma release assay in HIV-1-infected individuals. Clin Infect Dis.2009;48:954-62.[PubMed Abstract] -
20. Elzi L, Schlegel M, Weber R, et al. Reducing tuberculosis incidence by tuberculin skin testing,preventive treatment, and antiretroviral therapy in an area of low tuberculosis transmission. ClinInfect Dis. 2007;44:94-102.[PubMed Abstract] -
21. Kim YJ, Kim SI, Kim YR, Wie SH, Park YJ, Kang MW. Predictive value of interferon-γ ELISPOT assay inHIV 1-infected patients in an intermediate tuberculosis-endemic area. AIDS Res Hum Retroviruses.2012;28:1038-43.[PubMed Abstract] -
22. Markowitz N, Hansen NI, Hopewell PC, et al. Incidence of tuberculosis in the United States among HIV-infected persons. The Pulmonary Complications of HIV Study Group. Ann Intern Med.1997;126:123-32. [PubMed Abstract] -
23. Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent tuberculosis infection in HIV infectedpersons. Cochrane Database Syst Rev. 2010;:CD000171.[PubMed Abstract] -
24. Durovni B, Saraceni V, Moulton LH, et al. Effect of improved tuberculosis screening and isoniazidpreventive therapy on incidence of tuberculosis and death in patients with HIV in clinics in Rio de
Page 15/40

Janeiro, Brazil: a stepped wedge, cluster-randomised trial. Lancet Infect Dis. 2013;13:852-8.[PubMed Abstract] -
25. Golub JE, Saraceni V, Cavalcante SC, et al. The impact of antiretroviral therapy and isoniazidpreventive therapy on tuberculosis incidence in HIV-infected patients in Rio de Janeiro, Brazil. AIDS.2007;21:1441-8.[PubMed Abstract] -
26. TEMPRANO ANRS 12136 Study Group, Danel C, Moh R, et al. A Trial of Early Antiretrovirals andIsoniazid Preventive Therapy in Africa. N Engl J Med. 2015;373:808-22.[PubMed Abstract] -
27. Sterling TR, Njie G, Zenner D, et al. Guidelines for the Treatment of Latent Tuberculosis Infection:Recommendations from the National Tuberculosis Controllers Association and CDC, 2020. MMWRRecomm Rep. 2020;69:1-11.[PubMed Abstract] -
28. Targeted tuberculin testing and treatment of latent tuberculosis infection. This official statement ofthe American Thoracic Society was adopted by the ATS Board of Directors, July 1999. This is a JointStatement of the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention(CDC). This statement was endorsed by the Council of the Infectious Diseases Society of America.(IDSA), September 1999, and the sections of this statement. Am J Respir Crit Care Med.2000;161:S221-47.[PubMed Abstract] -
29. Backus LI, Boothroyd DB, Phillips BR, et al. National quality forum performance measures for HIV/AIDScare: the Department of Veterans Affairs experience. Arch Intern Med. 2010;170:1239-46.[PubMed Abstract] -
30. Lee LM, Lobato MN, Buskin SE, Morse A, Costa OS. Low adherence to guidelines for preventing TBamong persons with newly diagnosed HIV infection, United States. Int J Tuberc Lung Dis.2006;10:209-14.[PubMed Abstract] -
31. Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K. Updated guidelines for using InterferonGamma Release Assays to detect Mycobacterium tuberculosis infection - United States, 2010. MMWRRecomm Rep. 2010;59:1-25.[PubMed Abstract] -
32. Pascopella L, Franks J, Marks SM, et al. Opportunities for tuberculosis diagnosis and prevention amongpersons living with HIV: a cross-sectional study of policies and practices at four large Ryan WhiteProgram-Funded HIV clinics. PLoS One. 2014;9:e101313.[PubMed Abstract] -
33. Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American Thoracic Society/Infectious DiseasesSociety of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosisof Tuberculosis in Adults and Children. Clin Infect Dis. 2017;64:e1-e33.[PubMed Abstract] -
34. Pai M, Denkinger CM, Kik SV, et al. Gamma interferon release assays for detection of Mycobacteriumtuberculosis infection. Clin Microbiol Rev. 2014;27:3-20.[PubMed Abstract] -
35. Andersen P, Munk ME, Pollock JM, Doherty TM. Specific immune-based diagnosis of tuberculosis.
Page 16/40

Lancet. 2000;356:1099-104.[PubMed Abstract] -
36. National Tuberculosis Controllers Association; Centers for Disease Control and Prevention (CDC).Guidelines for the investigation of contacts of persons with infectious tuberculosis. Recommendationsfrom the National Tuberculosis Controllers Association and CDC. MMWR Recomm Rep. 2005;54:1-47.[Pub Med Abstract] -
37. Metcalfe JZ, Everett CK, Steingart KR, et al. Interferon-γ release assays for active pulmonarytuberculosis diagnosis in adults in low- and middle-income countries: systematic review and meta-analysis. J Infect Dis. 2011;204 Suppl 4:S1120-9.[PubMed Abstract] -
38. Santin M, Muñoz L, Rigau D. Interferon-γ release assays for the diagnosis of tuberculosis andtuberculosis infection in HIV-infected adults: a systematic review and meta-analysis. PLoS One.2012;7:e32482.[PubMed Abstract] -
39. Farhat M, Greenaway C, Pai M, Menzies D. False-positive tuberculin skin tests: what is the absoluteeffect of BCG and non-tuberculous mycobacteria? Int J Tuberc Lung Dis. 2006;10:1192-204.[PubMed Abstract] -
40. Teixeira HC, Abramo C, Munk ME. Immunological diagnosis of tuberculosis: problems and strategiesfor success. J Bras Pneumol. 2007;33:323-34.[PubMed Abstract] -
41. Metcalfe JZ, Cattamanchi A, McCulloch CE, Lew JD, Ha NP, Graviss EA. Test variability of theQuantiFERON-TB gold in-tube assay in clinical practice. Am J Respir Crit Care Med. 2013;187:206-11.[PubMed Abstract] -
42. Moon HW, Gaur RL, Tien SS, Spangler M, Pai M, Banaei N. Evaluation of QuantiFERON-TB Gold-Plus inHealth Care Workers in a Low-Incidence Setting. J Clin Microbiol. 2017;55:1650-1657.[PubMed Abstract] -
43. Day CL, Abrahams DA, Lerumo L, et al. Functional capacity of Mycobacterium tuberculosis-specific Tcell responses in humans is associated with mycobacterial load. J Immunol. 2011;187:2222-32.[PubMed Abstract] -
44. Rozot V, Vigano S, Mazza-Stalder J, et al. Mycobacterium tuberculosis-specific CD8+ T cells arefunctionally and phenotypically different between latent infection and active disease. Eur J Immunol.2013;43:1568-77.[PubMed Abstract] -
45. Qiagen. QuantiFERON®-TB Gold Plus (QFT®-Plus). Package Insert. July 2018[Qiagen] -
46. Hoffmann H, Avsar K, Göres R, Mavi SC, Hofmann-Thiel S. Equal sensitivity of the new generationQuantiFERON-TB Gold plus in direct comparison with the previous test version QuantiFERON-TB GoldIT. Clin Microbiol Infect. 2016;22:701-3.[PubMed Abstract] -
47. Petruccioli E, Vanini V, Chiacchio T, et al. Analytical evaluation of QuantiFERON- Plus andQuantiFERON- Gold In-tube assays in subjects with or without tuberculosis. Tuberculosis (Edinb).2017;106:38-43.
Page 17/40

[PubMed Abstract] -
48. Aichelburg MC, Reiberger T, Breitenecker F, Mandorfer M, Makristathis A, Rieger A. Reversion andconversion of interferon-γ release assay results in HIV-1-infected individuals. J Infect Dis.2014;209:729-33.[PubMed Abstract] -
49. Gray J, Reves R, Johnson S, Belknap R. Identification of false-positive QuantiFERON-TB Gold In-Tubeassays by repeat testing in HIV-infected patients at low risk for tuberculosis. Clin Infect Dis.2012;54:e20-3.[PubMed Abstract] -
50. Pullar ND, Steinum H, Bruun JN, Dyrhol-Riise AM. HIV patients with latent tuberculosis living in a low-endemic country do not develop active disease during a 2 year follow-up; a Norwegian prospectivemulticenter study. BMC Infect Dis. 2014;14:667.[PubMed Abstract] -
51. Barcellini L, Borroni E, Brown J, et al. First evaluation of QuantiFERON-TB Gold Plus performance incontact screening. Eur Respir J. 2016;48:1411-19.[PubMed Abstract] -
52. Oxford Immunotec. T-SPOT.TB[Oxford Immunotec] -
53. Cattamanchi A, Smith R, Steingart KR, et al. Interferon-gamma release assays for the diagnosis oflatent tuberculosis infection in HIV-infected individuals: a systematic review and meta-analysis. JAcquir Immune Defic Syndr. 2011;56:230-8.[PubMed Abstract] -
54. Watkins RE, Brennan R, Plant AJ. Tuberculin reactivity and the risk of tuberculosis: a review. Int JTuberc Lung Dis. 2000;4:895-903.[PubMed Abstract] -
55. Hill PC, Brookes RH, Fox A, et al. Longitudinal assessment of an ELISPOT test for Mycobacteriumtuberculosis infection. PLoS Med. 2007;4:e192.[PubMed Abstract] -
56. Getahun H, Kittikraisak W, Heilig CM, et al. Development of a standardized screening rule fortuberculosis in people living with HIV in resource-constrained settings: individual participant datameta-analysis of observational studies. PLoS Med. 2011;8:e1000391.[PubMed Abstract] -
57. Hamada Y, Lujan J, Schenkel K, Ford N, Getahun H. Sensitivity and specificity of WHO's recommendedfour-symptom screening rule for tuberculosis in people living with HIV: a systematic review and meta-analysis. Lancet HIV. 2018;5:e515-e523.[PubMed Abstract] -
58. Centers for Disease Control (CDC). Latent Tuberculosis Infection: A Guide for Primary Health CareProviders 2014 [updated November 26, 2014].[CDC] -
59. Machingaidze S, Verver S, Mulenga H, et al. Predictive value of recent QuantiFERON conversion fortuberculosis disease in adolescents. Am J Respir Crit Care Med. 2012;186:1051-6.[PubMed Abstract] -
Page 18/40

60. Diel R, Loddenkemper R, Meywald-Walter K, Niemann S, Nienhaus A. Predictive value of a whole bloodIFN-gamma assay for the development of active tuberculosis disease after recent infection with Mycobacterium tuberculosis. Am J Respir Crit Care Med. 2008;177:1164-70.[PubMed Abstract] -
61. Diel R, Loddenkemper R, Niemann S, Meywald-Walter K, Nienhaus A. Negative and positive predictivevalue of a whole-blood interferon-γ release assay for developing active tuberculosis: an update. Am JRespir Crit Care Med. 2011;183:88-95.[PubMed Abstract] -
62. Leung CC, Yam WC, Ho PL, et al. T-Spot.TB outperforms tuberculin skin test in predicting developmentof active tuberculosis among household contacts. Respirology. 2015;20:496-503.[PubMed Abstract] -
63. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviralagents in adults and adolescents with HIV. Department of Health and Human Services. Considerationsfor antiretroviral use in patients with coinfections: Tuberculosis/HIV coinfection. June 3, 2021.[HIV.gov] -
64. Borisov AS, Bamrah Morris S, Njie GJ, et al. Update of Recommendations for Use of Once-WeeklyIsoniazid-Rifapentine Regimen to Treat Latent Mycobacterium tuberculosis Infection. MMWR MorbMortal Wkly Rep. 2018;67:723-6.[PubMed Abstract] -
65. Sterling TR, Villarino ME, Borisov AS, et al. Three months of rifapentine and isoniazid for latenttuberculosis infection. N Engl J Med. 2011;365:2155-66.[PubMed Abstract] -
66. Sterling TR, Scott NA, Miro JM, et al. Three months of weekly rifapentine and isoniazid for treatment ofMycobacterium tuberculosis infection in HIV-coinfected persons. AIDS. 2016;30:1607-15.[PubMed Abstract] -
67. Churchyard G, Cárdenas V, Chihota V, et al. Annual tuberculosis preventive therapy for Ppersons withHIV infection: a randomized trial. Ann Intern Med. 2021;174:1367-76.[PubMed Abstract] -
68. Dooley KE, Savic R, Gupte A, et al. Once-weekly rifapentine and isoniazid for tuberculosis preventionin patients with HIV taking dolutegravir-based antiretroviral therapy: a phase 1/2 trial. Lancet HIV.2020;7:e401-e409.[PubMed Abstract] -
69. Pham HT, Mesplède T. Bictegravir in a fixed-dose tablet with emtricitabine and tenofovir alafenamidefor the treatment of HIV infection: pharmacology and clinical implications. Expert Opin Pharmacother.2019;20:385-397.[PubMed Abstract] -
70. Martinson NA, Barnes GL, Moulton LH, et al. New regimens to prevent tuberculosis in adults with HIVinfection. N Engl J Med. 2011;365:11-20.[PubMed Abstract] -
71. Menzies D, Adjobimey M, Ruslami R, et al. Four Months of Rifampin or Nine Months of Isoniazid forLatent Tuberculosis in Adults. N Engl J Med. 2018;379:440-53.[PubMed Abstract] -
Page 19/40

72. Swindells S, Ramchandani R, Gupta A, et al. One Month of Rifapentine plus Isoniazid to Prevent HIV-Related Tuberculosis. N Engl J Med. 2019;380:1001-11.[PubMed Abstract] -
73. Centers for Disease Control and Prevention (CDC). Severe isoniazid-associated liver injuries amongpersons being treated for latent tuberculosis infection - United States, 2004-2008. MMWR Morb MortalWkly Rep. 2010;59:224-9.[PubMed Abstract] -
74. Saukkonen JJ, Cohn DL, Jasmer RM, et al. An official ATS statement: hepatotoxicity of antituberculosistherapy. Am J Respir Crit Care Med. 2006;174:935-52.[PubMed Abstract] -
75. Centers for Disease Control and Prevention (CDC). Update: Fatal and severe liver injuries associatedwith rifampin and pyrazinamide treatment for latent tuberculosis infection. MMWR Morb Mortal WklyRep. 2002;51:998-9.[PubMed Abstract] -
76. Centers for Disease Control and Prevention (CDC); American Thoracic Society. Update: adverse eventdata and revised American Thoracic Society/CDC recommendations against the use of rifampin andpyrazinamide for treatment of latent tuberculosis infection--United States, 2003. MMWR Morb MortalWkly Rep. 2003;52:735-9.[PubMed Abstract] -
77. LaCourse SM, Cranmer LM, Matemo D, et al. Effect of Pregnancy on Interferon Gamma Release Assayand Tuberculin Skin Test Detection of Latent TB Infection Among HIV-Infected Women in a HighBurden Setting. J Acquir Immune Defic Syndr. 2017;75:128-136.[PubMed Abstract] -
78. Mathad JS, Bhosale R, Sangar V, et al. Pregnancy differentially impacts performance of latenttuberculosis diagnostics in a high-burden setting. PLoS One. 2014;9:e92308.[PubMed Abstract] -
79. Covelli HD, Wilson RT. Immunologic and medical considerations in tuberculin-sensitized pregnantpatients. Am J Obstet Gynecol. 1978;132:256-9.[PubMed Abstract] -
80. Gupta A, Montepiedra G, Aaron L, et al. Isoniazid Preventive Therapy in HIV-Infected Pregnant andPostpartum Women. N Engl J Med. 2019;381:1333-1346.[PubMed Abstract] -
81. Franks AL, Binkin NJ, Snider DE Jr, Rokaw WM, Becker S. Isoniazid hepatitis among pregnant andpostpartum Hispanic patients. Public Health Rep. 1989;104:151-5.[PubMed Abstract] -
82. Kalk E, Heekes A, Mehta U, et al. Safety and Effectiveness of Isoniazid Preventive Therapy in PregnantWomen Living with Human Immunodeficiency Virus on Antiretroviral Therapy: An Observational StudyUsing Linked Population Data. Clin Infect Dis. 2020;71:e351-e358.[PubMed Abstract] -
83. Salazar-Austin N, Cohn S, Lala S, et al. Isoniazid Preventive Therapy and Pregnancy Outcomes inWomen Living With Human Immunodeficiency Virus in the Tshepiso Cohort. Clin Infect Dis.2020;71:1419-26.
Page 20/40

[PubMed Abstract] -
84. Centers for Disease Control and Prevention (CDC). Recommendations for use of an isoniazid-rifapentine regimen with direct observation to treat latent Mycobacterium tuberculosis infection.MMWR Morb Mortal Wkly Rep. 2011;60:1650-3.[PubMed Abstract] -
85. Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the preventionand treatment of opportunistic infections in adults and adolescents with HIV: recommendations fromthe Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV MedicineAssociation of the Infectious Diseases Society of America. Table 8. Summary of pre-clinical and humandata on, and indications for, opportunistic infection drugs during pregnancy. Last updated: February11, 2020.[HIV.gov] -
86. Mathad JS, Savic RM, Britto P, et al. Rifapentine pharmacokinetics and safety in pregnant women withand without HIV on 3HP. Conference on Retroviruses and Opportunistic Infections 2020; Boston, MA.Abstract 144.[CROI] -
87. Centers for Disease Control (CDC). Targeted Tuberculosis (TB) Testing and Treatment of Latent TBInfection 2011.[CDC] -
88. Marais BJ, Gie RP, Schaaf HS, et al. The clinical epidemiology of childhood pulmonary tuberculosis: acritical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis. 2004;8:278-85.[PubMed Abstract] -
89. Donald PR, Maher D, Qazi S. A research agenda to promote the management of childhood tuberculosiswithin national tuberculosis programmes. Int J Tuberc Lung Dis. 2007;11:370-80.[PubMed Abstract] -
90. Panel on Opportunistic Infections in HIV-Exposed and HIV-Infected Children. Guidelines for theprevention and treatment of opportunistic infections among HIV-exposed and HIV-infected children. Mycobacterium tuberculosis. November 6, 2013.[HIV.gov] -
91. Starke JR. Interferon-γ release assays for diagnosis of tuberculosis infection and disease in children.Pediatrics. 2014;134:e1763-73.[PubMed Abstract] -
References
Ahmad Khan F, Verkuijl S, Parrish A, et al. Performance of symptom-based tuberculosis screeningamong people living with HIV: not as great as hoped. AIDS. 2014;28:1463-72.[PubMed Abstract] -
Albalak R, O'Brien RJ, Kammerer JS, et al. Trends in tuberculosis/human immunodeficiency viruscomorbidity, United States, 1993-2004. Arch Intern Med. 2007;167:2443-52.[PubMed Abstract] -
Badje A, Moh R, Gabillard D, et al. Effect of isoniazid preventive therapy on risk of death in westAfrican, HIV-infected adults with high CD4 cell counts: long-term follow-up of the Temprano ANRS
Page 21/40

12136 trial. Lancet Glob Health. 2017;5:e1080-e1089.[PubMed Abstract] -
Belknap R, Holland D, Feng PJ, et al. Self-administered Versus Directly Observed Once-WeeklyIsoniazid and Rifapentine Treatment of Latent Tuberculosis Infection: A Randomized Trial. Ann InternMed. 2017;167:689-97.[PubMed Abstract] -
Bennett DE, Courval JM, Onorato I, et al. Prevalence of tuberculosis infection in the United Statespopulation: the national health and nutrition examination survey, 1999-2000. Am J Respir Crit CareMed. 2007;177:348-55.[PubMed Abstract] -
Centers for Disease Control (CDC). Managing Drug Interactions in the Treatment of HIV-RelatedTuberculosis 2013[CDC] -
Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2015 Atlanta, GA: U.S.Department of Health and Human Services, CDC; 2016.[CDC] -
Centers for Disease Control and Prevention (CDC). Severe isoniazid-associated liver injuries amongpersons being treated for latent tuberculosis infection - United States, 2004-2008. MMWR Morb MortalWkly Rep. 2010;59:224-9.[MMWR] -
Ermann J, Rao DA, Teslovich NC, Brenner MB, Raychaudhuri S. Immune cell profiling to guidetherapeutic decisions in rheumatic diseases. Nat Rev Rheumatol. 2015;11:541-51.[PubMed Abstract] -
Gedde-Dahl T. Tuberculous infection in the light of tuberculin matriculation. Am J Hyg.1952;56:139-214.[PubMed Abstract] -
Gupta A, Wood R, Kaplan R, Bekker LG, Lawn SD. Tuberculosis incidence rates during 8 years of follow-up of an antiretroviral treatment cohort in South Africa: comparison with rates in the community. PLoSOne. 2012;7:e34156.[PubMed Abstract] -
Hanna DB, Gupta LS, Jones LE, Thompson DM, Kellerman SE, Sackoff JE. AIDS-defining opportunisticillnesses in the HAART era in New York City. AIDS Care. 2007;19:264-72.[PubMed Abstract] -
Hoffmann CJ, Variava E, Rakgokong M, et al. High prevalence of pulmonary tuberculosis but lowsensitivity of symptom screening among HIV-infected pregnant women in South Africa. PLoS One.2013;8:e62211.[PubMed Abstract] -
Johnson JL, Okwera A, Hom DL, et al. Duration of efficacy of treatment of latent tuberculosis infectionin HIV-infected adults. AIDS. 2001;15:2137-47.[PubMed Abstract] -
Jonnalagadda S, Lohman Payne B, Brown E, et al. Latent tuberculosis detection by interferon γ releaseassay during pregnancy predicts active tuberculosis and mortality in human immunodeficiency virus
Page 22/40

type 1-infected women and their children. J Infect Dis. 2010;202:1826-35.[PubMed Abstract] -
Kahwati LC, Feltner C, Halpern M, et al. Primary Care Screening and Treatment for Latent TuberculosisInfection in Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force.JAMA. 2016;316:970-83.[PubMed Abstract] -
Kancheya N, Luhanga D, Harris JB, et al. Integrating active tuberculosis case finding in antenatalservices in Zambia. Int J Tuberc Lung Dis. 2014;18:1466-72.[PubMed Abstract] -
Pepper T, Joseph P, Mwenya C, et al. Normal chest radiography in pulmonary tuberculosis: implicationsfor obtaining respiratory specimen cultures. Int J Tuberc Lung Dis. 2008;12:397-403.[PubMed Abstract] -
Podany AT, Bao Y, Swindells S, et al. Efavirenz Pharmacokinetics and Pharmacodynamics in HIV-Infected Persons Receiving Rifapentine and Isoniazid for Tuberculosis Prevention. Clin Infect Dis.2015;61:1322-7.[PubMed Abstract] -
Qiagen. QuantiFERON®-TB Gold. Package Insert.[Qiagen] -
Rangaka MX, Wilkinson RJ, Glynn JR, et al. Effect of antiretroviral therapy on the diagnostic accuracy ofsymptom screening for intensified tuberculosis case finding in a South African HIV clinic. Clin InfectDis. 2012;55:1698-706.[PubMed Abstract] -
Rivero A, López-Cortés L, Castillo R, et al. [Randomized clinical trial investigating threechemoprophylaxis regimens for latent tuberculosis infection in HIV-infected patients]. Enferm InfeccMicrobiol Clin. 2007;25:305-10.[PubMed Abstract] -
Stennis NL, Trieu L, Ahuja SD, Harris TG. Estimated Prevalence of Tuberculosis Infection Among a NewYork City Clinic Population Using Interferon-gamma Release Assays. Open Forum Infect Dis.2014;1:ofu047.[PubMed Abstract] -
Stewart RJ, Tsang CA, Pratt RH, Price SF, Langer AJ. Tuberculosis - United States, 2017. MMWR MorbMortal Wkly Rep. 2018;67:317-23.[PubMed Abstract] -
Sutherland JS, Young JM, Peterson KL, et al. Polyfunctional CD4(+) and CD8(+) T cell responses totuberculosis antigens in HIV-1-infected patients before and after anti-retroviral treatment. J Immunol.2010;184:6537-44.[PubMed Abstract] -
Takasaki J, Manabe T, Morino E, et al. Sensitivity and specificity of QuantiFERON-TB Gold Pluscompared with QuantiFERON-TB Gold In-Tube and T-SPOT.TB on active tuberculosis in Japan. J InfectChemother. 2018;24:188-92.[PubMed Abstract] -
Telisinghe L, Amofa-Sekyi M, Maluzi K, et al. The sensitivity of the QuantiFERON®-TB Gold Plus assay in
Page 23/40

Zambian adults with active tuberculosis. Int J Tuberc Lung Dis. 2017;21:690-6.[PubMed Abstract] -
Weiner M, Egelund EF, Engle M, et al. Pharmacokinetic interaction of rifapentine and raltegravir inhealthy volunteers. J Antimicrob Chemother. 2014;69:1079-85.[PubMed Abstract] -
Whalen CC, Johnson JL, Okwera A, et al. A trial of three regimens to prevent tuberculosis in Ugandanadults infected with the human immunodeficiency virus. Uganda-Case Western Reserve UniversityResearch Collaboration. N Engl J Med. 1997;337:801-8.[PubMed Abstract] -
Zwerling A, van den Hof S, Scholten J, Cobelens F, Menzies D, Pai M. Interferon-gamma release assaysfor tuberculosis screening of healthcare workers: a systematic review. Thorax. 2012;67:62-70.[PubMed Abstract] -
Page 24/40

Figures
Figure 1 Tuberculosis Cases in United States, 1980-2019
Source: Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA:U.S. Department of Health and Human Services, CDC.
Page 25/40

Figure 2 Tuberculosis Case Rates per 100,000 Population among U.S.-Born versus Non-U.S.-Born, 1993–2019
Source: Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA:U.S. Department of Health and Human Services, CDC.
Page 26/40
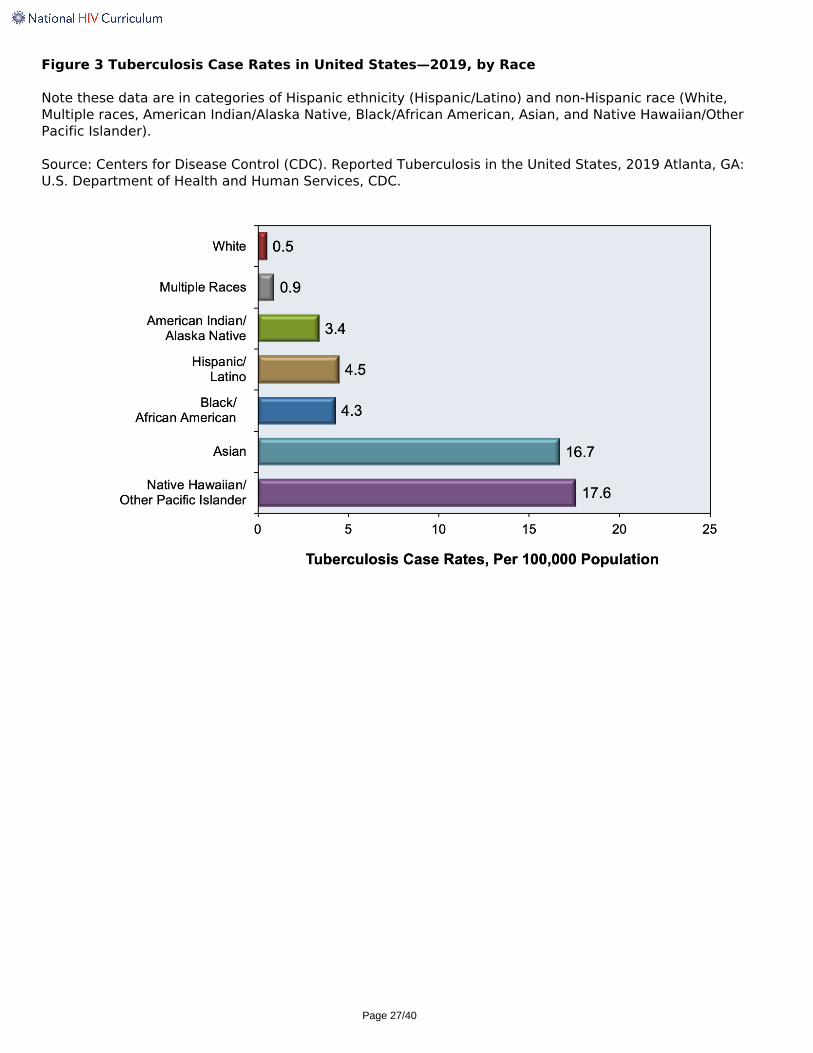
Figure 3 Tuberculosis Case Rates in United States—2019, by Race
Note these data are in categories of Hispanic ethnicity (Hispanic/Latino) and non-Hispanic race (White,Multiple races, American Indian/Alaska Native, Black/African American, Asian, and Native Hawaiian/OtherPacific Islander).
Source: Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA:U.S. Department of Health and Human Services, CDC.
Page 27/40

Figure 4 Tuberculosis Cases among Persons with HIV—United States, 1993-2019
This graphic shows the number of persons diagnosed with tuberculosis who had HIV coinfection. These dataare from tuberculosis cases in which an HIV test result was reported. California began reporting HIV testresults to the CDC in 2011. Consequently, 2011 was the first year in which HIV status was 90% or greatercomplete.
Source: Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA:U.S. Department of Health and Human Services, CDC.
Page 28/40
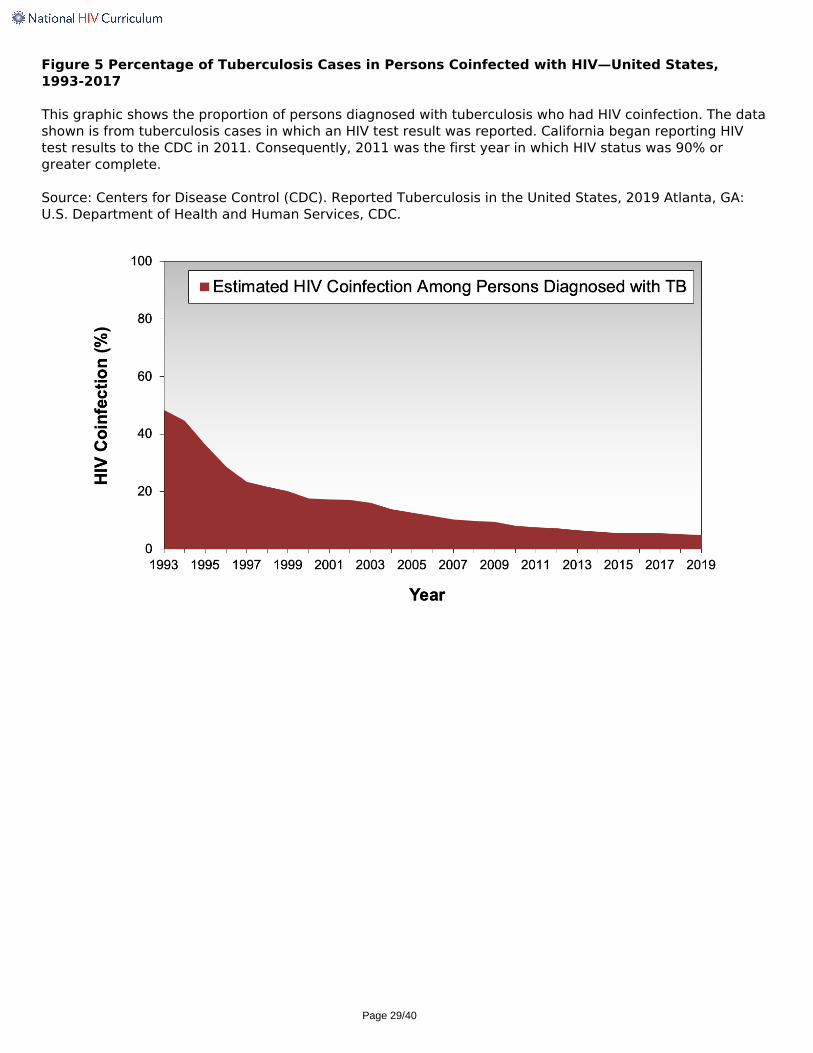
Figure 5 Percentage of Tuberculosis Cases in Persons Coinfected with HIV—United States,1993-2017
This graphic shows the proportion of persons diagnosed with tuberculosis who had HIV coinfection. The datashown is from tuberculosis cases in which an HIV test result was reported. California began reporting HIVtest results to the CDC in 2011. Consequently, 2011 was the first year in which HIV status was 90% orgreater complete.
Source: Centers for Disease Control (CDC). Reported Tuberculosis in the United States, 2019 Atlanta, GA:U.S. Department of Health and Human Services, CDC.
Page 29/40

Figure 6 Interrelationship of Host Immune Control in Person with LTBI
This graphic shows the impact of HIV-related immunosuppression on the course of latent tuberculosisinfection. With progressive HIV-related immune suppression, mycobacterial load increases and symptomatictuberculosis may develop. In contrast, taking antiretroviral therapy will restore some HIV-related immunesuppression and contribute to immune control of Mycobacterium tuberculosis.
Source: Lawn SD, Wood R, Wilkinson RJ. Changing concepts of latent tuberculosis infection in patients livingwith HIV infection. Clin Dev Immunol. 2011;2011. pii: 980594.
Page 30/40

Figure 7 Mantoux Tuberculin Skin Test
The standard Mantoux tuberculin skin test is performed by injecting 0.1 mL of 5 tuberculin purified proteinderivative (PPS) units of liquid tuberculin between the layers of the skin (intradermally) on the volar surfaceof the forearm.
Source: Centers for Disease Control and Prevention (CDC)
Page 31/40

Figure 8 Reading a Tuberculin Skin Test
The Mantoux tuberculin skin test should be read 48 to 72 hours after the intradermal administration of thepurified protein derivative. The transverse diameter of cutaneous induration (not erythema) should bemeasured. Use a reliable method to determine the edge of the induration on one side and mark this (blackdot shown here); then do the exact same thing on the opposite side. Using a millimeter ruler, measure thedistance between the two dots and that is the size in mm for the test result. In the example shown theinduration is 11 mm.
Source: Centers for Disease Control and Prevention (CDC)
Page 32/40
Figure 9 Interferon-Gamma Release Assays (IGRAs)
Source: Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K. Updated guidelines for usingInterferon Gamma Release Assays to detect Mycobacterium tuberculosis infection - United States, 2010.MMWR Recomm Rep. 2010;59:1-25.
Page 33/40

Figure 10 QuantiFERON-TB Gold Plus Blood Draw Tubes
The QuantiFERON-TB Gold utilizes four tubes and 1 mL of blood is required for each tube: (1) the gray top Niltube that serves as a negative control to adjust for background interferon gamma production; (2) the greentop TB1 tube that primarily detects CD4 T-lymphocytes responses to mycobacterial antigens; (3) the yellowtop TB2 tube that is optimized for detection of CD4 and CD8 T-lymphocyte responses to mycobacterialantigens; and (4) the purple top Mitogen tube that functions as a positive control to confirm baselineimmune status; a low response may indicate inability to generate interferon gamma.
Source: Qiagen
Page 34/40

Figure 11 Interpretation Criteria for QuantiFERON-TB Gold Plus (QFT-Plus)
Source: Qiagen
Page 35/40

Figure 12 Interpretation of T-SPOT Results
Results are interpreted by subtracting the spot count in the negative (Nil) control from the spot count inPanels A and B. The test is considered positive if Panel A minus Nil and/or Panel B minus Nil is 8 or morespots. The test is considered negative if both Panel A minus Nil and Panel B minus Nil is less than or equal to4 spots. The test is considered borderline (equivocal) if the highest of the Panel A or Panel B spot count issuch that the (Panel minus Nil) spot count is 5, 6, or 7 spots.
Source: Oxford Immunotec. T-SPOT.TB. Prescribing Information.
Page 36/40

Figure 13 Interpretation Criteria for the T-SPOT.TB Test (T-Spot)
Source: Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K. Updated guidelines for usingInterferon Gamma Release Assays to detect Mycobacterium tuberculosis infection - United States, 2010.MMWR Recomm Rep. 2010;59:1-25.
Page 37/40

Table 1. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults andAdolescents with HIV
Treating Latent Tuberculosis Infection in Persons with HIV
Indications:
(+) screening test (tuberculin skin test or IGRA) for latent tuberculosis infection, no evidence of activeTB, and no prior history of treatment for active or latent TB (AI);Close contact with a person with infectious TB, regardless of screening test result (AII)
Preferred Therapies for Latent Tuberculosis:
Note: the selection of one of the following regimens should take into account the individual's antiretroviralregimen
6H or 9H: Isoniazid 300 mg PO daily plus pyridoxine 25-50 mg PO daily for 6 or 9 months (AIII)3HP: Isoniazid 15 mg/kg weekly (900 mg maximum dose) plus Rifapentine (weight-based, 900 mgmaximum dose) PO weekly plus plus pyridoxine 50 mg weekly for 12 weeks. This regimen should onlyfor individuals receiving an antiretroviral regimen that has an anchor one of three anchordrugs—efavirenz (600 mg once daily) (AII), raltegravir (400 mg twice daily) (AII), or dolutegravir (50mg once daily) (BII)—used in combination with a backbone of tenofovir DF-emtricitabine orabacavir-lamivudine. Dolutegravir should only be used in persons for whom once daily dosing isappropriate. The weekly rifapentine weight-based doses are:
750 mg for person weighing 32.1–49.9 kg900 mg for persons weighing ≥50.0 kg
4R: Rifampin 600 mg PO daily for 4 months (BI)Alternative Therapy for Latent Tuberculosis:
1HP: Isoniazid 300 mg PO daily plus rifapentine (weight-based) PO daily plus pyridoxine 25 to 50 mgdaily for 4 weeks—this regimen should only be used for individuals receiving an antiretroviral regimenof efavirenz (600 mg once daily) in combination with tenofovir DF-emtricitabine or abacavir-lamivudine. The daily rifapentine weight-based doses are:
300 mg for persons weighing <35 kg450 mg for persons weighing 35-45 kg 600 mg for persons weighing >45 kg
Suspected Drug-Resistant TB
For persons exposed to drug-resistant TB, select anti-TB drugs after consultation with experts or with publichealth authorities (AII)Strength of RecommendationA: Strong recommendation for the statementB: Moderate recommendation for the statementC: Optional recommendation for the statement
Quality of Evidence for the Recommendation I: One or more randomized trials with clinical outcomes and/or validated laboratory endpointsII: One or more well-designed, non-randomized trials or observational cohort studies with long-termclinical outcomes III: Expert opinion
Source:
Page 38/40

Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviralagents in adults and adolescents with HIV. Department of Health and Human Services. Considerationsfor antiretroviral use in patients with coinfections: Tuberculosis/HIV coinfection. June 3, 2021.[HIV.gov]Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the preventionand treatment of opportunistic infections in adults and adolescents with HIV: recommendations fromthe Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV MedicineAssociation of the Infectious Diseases Society of America. Mycobacterium tuberculosis infection anddisease. Last update: September 27, 2019. [HIV.gov]
Page 39/40


















