LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT - … · LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT...
12
Clinical Guideline Template Page 1 of 12 LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT - CLINICAL GUIDELINE
Transcript of LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT - … · LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT...

Clinical Guideline Template
Page 1 of 12
LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT
- CLINICAL GUIDELINE

Clinical Guideline Template
Page 2 of 12
1. Aim/Purpose of this Guideline All clinical staff working in the Division of women, children & sexual health to provide evidence based guidance in the Investigation and Management of Late Onset Sepsis on the Neonatal Unit
2. The Guidance
Investigation and Management of Late Onset Sepsis on the Neonatal Unit Defined as sepsis diagnosed at >72 hours of age. Features that may indicate sepsis
Temperature instability or >37.5oC or <36.5oC Tachypnoea / Apnoeas / Respiratory distress Tachycardia / Bradycardia Neurological features: Lethargy, poor tone, poor feeding, irritability, seizures Other features: Jaundice, hepatomegaly, vomiting, abdominal distension, diarrhoea,
Initial investigations
Investigation Further information
In all cases :
Blood culture May identify bacteria and fungal infection
Full blood count Looking at neutrophils and platelets
CRP NICE guideline on EOS suggests levels of >10 are abnormal.
Blood gas Acidosis/ lactic acid level
To consider based on clinical context :
Urine culture Aim to perform a urine culture on all babies with sepsis >72h old
Clean catch/ SPA/ catheter sample
Other cultures From any potential foci of infection e.g.
- purulent eye drainage
- pustules
- tracheal aspirate – send on all ventilated babies with LOS
Lumbar puncture Consider in all cases of suspected LOS if no contraindications and if
baby able to tolerate the procedure.
Clinical signs suggesting meningitis can be lacking in neonates.
Giving antibiotics before performing LP underestimates meningitis

Clinical Guideline Template
Page 3 of 12
incidence by 50% in VLBW infants
Chest x-ray If respiratory symptoms are present
Initial management
Commence empiric antimicrobial therapy. Administer within 60 minutes of decision to treat.
Diagnosis Empiric therapy
Late onset sepsis, meningitis
not immediately suspected
Flucloxacillin + Gentamicin
Always consider risk of HSV and
add acyclovir if appropriate
Suspected neonatal meningitis Amoxicillin + Cefotaxime
Ensure the infant is in an environment allowing close monitoring.
Inform a middle grade doctor or consultant. Have a low threshold for removal of indwelling lines. If lines are left in at this point :
The baby needs daily blood cultures until they are recovered or the line is removed
Consider removing the line if the baby is still unwell 24 hours or more after initial suspicion of LOS
Ongoing management
Repeat CRP 18-24 hours after initial suspected LOS presentation.
Usually continue antibiotics, once started, until 36 hour blood culture result.
If 36 hour blood culture is negative, decision to continue or cease antibiotics is senior-led.
Note : antibiotics do not need to be continued in this situation, even if CRP or neutrophils raised, if an
alternative diagnosis to LOS is strongly suspected.6
If meningitis clinically suspected but CSF microscopy is normal, continue meningitis Treatment until CSF cultures negative. If CSF is culture positive, consider repeat LP after 2 days. Usually start anti-fungal therapy (oral miconazole and topical clotrimazole) if antibiotics continue for longer than 36-48 hours. These antifungals should continue for 2 days after the antibiotics stop.
If blood culture is positive : In all cases :
Consider removing an indwelling lines that were not removed at first suspicion of LOS
Complete a Datix, as all healthcare associated bacteraemias must be Datixed
Clinical Guideline Template
Page 4 of 12
Inform neonatal research nurse for uploading to Neonin database
If a CoNS (coagulase negative staphylococcus) is grown on blood culture :
Switch to vancomycin and stop gentamicin
If an as yet undetermined Staphylococcus species is grown on blood culture AND the baby has a central/long line AND the baby is not clearly responding to flucloxacillin and gentamicin :
Switch to vancomycin
Consider need for continuing Gram negative cover : remember increased toxicity risk with vancomycin and gentamicin in combination
Discuss with Clinical Microbiology
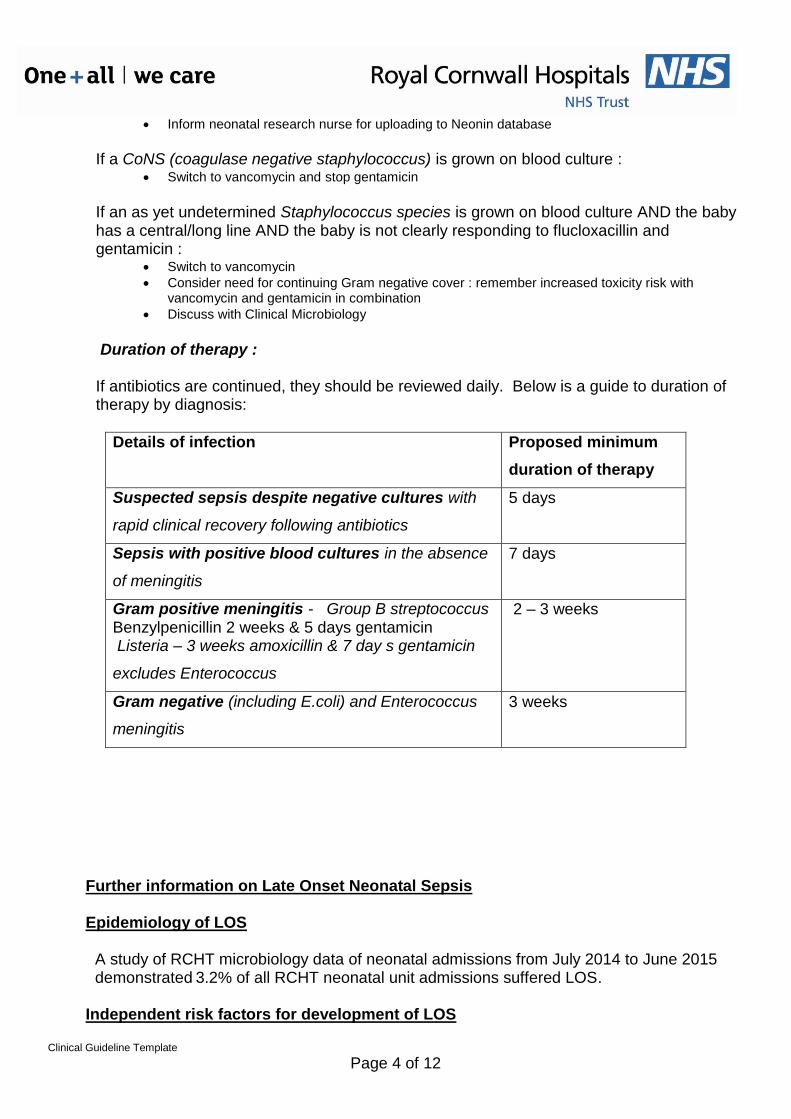
Duration of therapy : If antibiotics are continued, they should be reviewed daily. Below is a guide to duration of therapy by diagnosis:
Details of infection Proposed minimum
duration of therapy
Suspected sepsis despite negative cultures with
rapid clinical recovery following antibiotics
5 days
Sepsis with positive blood cultures in the absence
of meningitis
7 days
Gram positive meningitis - Group B streptococcus Benzylpenicillin 2 weeks & 5 days gentamicin Listeria – 3 weeks amoxicillin & 7 day s gentamicin
excludes Enterococcus
2 – 3 weeks
Gram negative (including E.coli) and Enterococcus
meningitis
3 weeks
Further information on Late Onset Neonatal Sepsis Epidemiology of LOS
A study of RCHT microbiology data of neonatal admissions from July 2014 to June 2015
demonstrated 3.2% of all RCHT neonatal unit admissions suffered LOS.
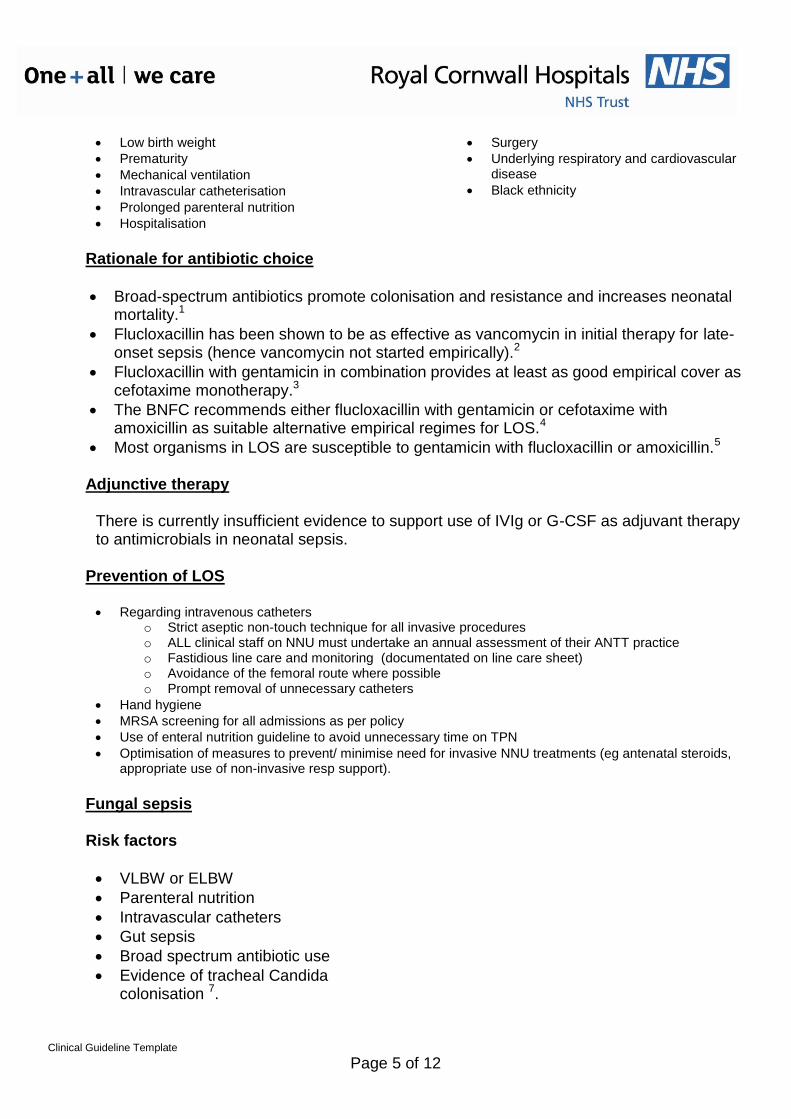
Independent risk factors for development of LOS
Clinical Guideline Template
Page 5 of 12
Low birth weight
Prematurity
Mechanical ventilation
Intravascular catheterisation
Prolonged parenteral nutrition
Hospitalisation
Surgery
Underlying respiratory and cardiovascular disease
Black ethnicity
Rationale for antibiotic choice
Broad-spectrum antibiotics promote colonisation and resistance and increases neonatal mortality.1
Flucloxacillin has been shown to be as effective as vancomycin in initial therapy for late-onset sepsis (hence vancomycin not started empirically).2
Flucloxacillin with gentamicin in combination provides at least as good empirical cover as cefotaxime monotherapy.3
The BNFC recommends either flucloxacillin with gentamicin or cefotaxime with amoxicillin as suitable alternative empirical regimes for LOS.4
Most organisms in LOS are susceptible to gentamicin with flucloxacillin or amoxicillin.5
Adjunctive therapy
There is currently insufficient evidence to support use of IVIg or G-CSF as adjuvant therapy to antimicrobials in neonatal sepsis.
Prevention of LOS
Regarding intravenous catheters
o Strict aseptic non-touch technique for all invasive procedures o ALL clinical staff on NNU must undertake an annual assessment of their ANTT practice o Fastidious line care and monitoring (documentated on line care sheet) o Avoidance of the femoral route where possible o Prompt removal of unnecessary catheters
Hand hygiene
MRSA screening for all admissions as per policy
Use of enteral nutrition guideline to avoid unnecessary time on TPN
Optimisation of measures to prevent/ minimise need for invasive NNU treatments (eg antenatal steroids, appropriate use of non-invasive resp support).
Fungal sepsis Risk factors
VLBW or ELBW
Parenteral nutrition
Intravascular catheters
Gut sepsis
Broad spectrum antibiotic use
Evidence of tracheal Candida colonisation 7.

Clinical Guideline Template
Page 6 of 12
Prophylaxis
Recommended for infants continuing antibiotics beyond 36-48 hours.
Limited evidence. At present this is not part of routine practice in the UK.
Clinical features
25-50% mortality risk
Features as bacterial sepsis
Consider especially in infants who have not responded to antibiotics
Investigations
As above, also urine culture and microscopy for budding yeast and hyphae, request renal ultrasound
scan, and arrange retinal examination
Treatment
Amphotericin B alone or in combination with 5-fluorocytosine remains the standard of care for
neonatal candidiasis.
Evidence for choice and duration of therapy is limited
Consultant decision in liaison with microbiology
See http://www.doctorfungus.org/mycoses/human/candida/neonatal.htm for an extensive review on investigation and treatment of neonatal candidiasis.
Further updates to this guideline
Any update to this guideline should include: Results of the PREVAIL trial (PREVenting infection using Antimicrobial Impregnated Long lines)
which is due to be completed on 31/08/2017.
Any new data released by NeonIN on demographics of neonatal infections (most recent published data is from 2006-2008).
Any new research on other potential preventative measures such as probiotics, prebiotics, lactoferrin and early enteral trophic feed with breast milk
Any updates on the efficacy of IVIg or G-CSF as adjuvant therapy to antimicrobials.
References 1 Isaacs D, 2000 2 (Karlowicz M, et al, 2000) 3 [NeonIN at ESPID 2016] 4 See https://www.medicinescomplete.com/mc/bnfc/current/PHP78491-blood-infections-bacterial.htm?q=sepsis&t=advanced&ss=ts&tot=8&p=2#_hit 5Dong et al, Archives Fetal Neonatal 2015: 100:F257-F263 (open access, see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4413803/pdf/fetalneonatal-2014-306213.pdf) 6 A 2015 American ‘consensus’ paper stated that ‘isolated abnormal hematological or acute-phase-reactant measurements should not justify continuation of empiric antibiotics for more than 48 hours in well-appearing infants with negative culture results.’ 7. Roen J et al, 1994.

Clinical Guideline Template
Page 7 of 12
3. Monitoring compliance and effectiveness
Element to be monitored
Ad hoc review of cases
Lead Dr Paul Munyard, Consultant
Tool Ad hoc review of cases
Frequency annual
Reporting arrangements
Neonatal Guidelines Meeting
Acting on recommendations and Lead(s)
Neonatal Business Meeting
Change in practice and lessons to be shared
Required changes to practice will be identified and actioned within 3 months. A lead member of the team will be identified to take each change forward where appropriate. Lessons will be shared with all the relevant stakeholders
4. Equality and Diversity 4.1. This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement which can be found in the 'Equality, Diversity & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.

Clinical Guideline Template
Page 8 of 12
Appendix 1. Governance Information
Document Title LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT - CLINICAL GUIDELINE
Date Issued/Approved: 14/06/2017
Date Valid From: 01/08/2017
Date Valid To: 01/08/2020
Directorate / Department responsible (author/owner):
Paul Munyard Consultant Neonatology
Contact details: 01872 253293
Brief summary of contents
All clinical staff working in the Division of women, children & sexual health to provide evidence based guidance in the Investigation and Management of Late Onset Sepsis on the Neonatal Unit
Suggested Keywords: Sepsis, Late Onset Sepsis, Neonatal, neonatal sepsis, Neonatology
Target Audience RCHT PCH CFT KCCG
Executive Director responsible for Policy:
Medical Director
Date revised: 14/ Jun/2017
This document replaces (exact title of previous version):
LATE ONSET SEPSIS (LOS) ON THE NEONATAL UNIT - CLINICAL GUIDELINE
Approval route (names of committees)/consultation:
Divisional Manager confirming approval processes
Mr David Smith
Name and Post Title of additional signatories
Not Required
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder
Links to key external standards See

Clinical Guideline Template
Page 9 of 12
https://www.medicinescomplete.com/mc/bnfc/current/PHP78491-blood-infections-bacterial.htm?q=sepsis&t=advanced&ss=ts&tot=8&p=2#_hit 5Dong et al, Archives Fetal Neonatal 2015: 100:F257-F263 (open access, see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4413803/pdf/fetalneonatal-2014-306213.pdf)
Related Documents:
1 Isaacs D, 2000 2 (Karlowicz M, et al, 2000) 3 [NeonIN at ESPID 2016] 4 See https://www.medicinescomplete.com/mc/bnfc/current/PHP78491-blood-infections-bacterial.htm?q=sepsis&t=advanced&ss=ts&tot=8&p=2#_hit 5Dong et al, Archives Fetal Neonatal 2015: 100:F257-F263 (open access, see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4413803/pdf/fetalneonatal-2014-306213.pdf) 6 A 2015 American ‘consensus’ paper stated that ‘isolated abnormal hematological or acute-phase-reactant measurements should not justify continuation of empiric antibiotics for more than 48 hours in well-appearing infants with negative culture results.’ 7. Roen J et al, 1994.
Training Need Identified? No
Version Control Table
Date Version No
Summary of Changes Changes Made by (Name and Job Title)
14 Jun 17 V1.0 Paul Munyard Neonatal Consultant
Clinical Guideline Template
Page 10 of 12
All or part of this document can be released under the Freedom of Information Act 2000 This document is to be retained for 10 years from the date of expiry. This document is only valid on the day of printing Controlled Document This document has been created following the Royal Cornwall Hospitals NHS Trust Policy on Document Production. It should not be altered in any way without the express permission of the author or their Line Manager.

Clinical Guideline Template
Page 11 of 12
Appendix 2. Initial Equality Impact Assessment Form
Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Rationale for Assessment / Existing Evidence
Age X
Name of Name of the strategy / policy /proposal / service function to be assessed (hereafter referred to as policy) (Provide brief description): INVESTIGATION AND MANAGEMENT OF LATE ONSET SEPSIS ON THE NEONATAL UNIT
Directorate and service area: Neonatal
Is this a new or existing Policy? New
Name of individual completing assessment: Mr Paul Munyard
Telephone: 01872 253293
1. Policy Aim* Who is the strategy / policy / proposal / service function aimed at?
All clinical staff working in the Division of women, children & sexual health to provide evidence based guidance in the Investigation and Management of Late Onset Sepsis on the Neonatal Unit
2. Policy Objectives*
As above
3. Policy – intended Outcomes*
As above
4. *How will you measure the outcome?
See section 3
5. Who is intended to benefit from the policy?
All Neonatal patients
6a) Is consultation required with the workforce, equality groups, local interest groups etc. around this policy? b) If yes, have these *groups been consulted? C). Please list any groups who have been consulted about this procedure.
No
7. The Impact Please complete the following table.

Clinical Guideline Template
Page 12 of 12
Sex (male, female, trans-
gender / gender reassignment)
X
Race / Ethnic communities /groups
X
Disability - learning disability, physical disability, sensory impairment and mental health problems
X
Religion / other beliefs
X
Marriage and civil partnership
X
Pregnancy and maternity X
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
X
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have been identified as not requiring consultation. or
Major service redesign or development
8. Please indicate if a full equality analysis is recommended. Yes No X
9. If you are not recommending a Full Impact assessment please explain why.
Signature of policy developer / lead manager / director Date of completion and submission
Names and signatures of members carrying out the Screening Assessment
1. Dr Paul Munyard 2.
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead, c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD A summary of the results will be published on the Trust’s web site. Signed _______________ Date ________________