Aortic coarctation, diagnosis and treatment Coarctação da ...
Thorax (1975), 30, 31.
Late complications of surgery for coarctationof the aorta
J. KEITH ROSS, J. L. MONRO, and C. G. SBOKOS
Wessex Cardiac and Thoracic Centre, Southampton Western Hospital, Southampton S09 4WQ
Ross, J. K., Monro, J. L., and Sbokos, C. G. (1975). Thorax, 30, 31-39. Late complica-tions of surgery for coarctation of the aorta. The problem of the patient who has hadone operation for coarctation of the aorta and who then requires another because of a
late complication at or near the coarctation site is a demanding one. The safety of aorticcross-clamping at the second operation depends on the adequacy or otherwise of thecollateral circulation, and this in turn depends on the presence or absence of residualor recurrent aortic obstruction. Three illustrative cases are described in which therewas complete, incomplete, and no aortic obstruction respectively at the time ofreoperation, two of the cases presenting the additional complication of local aneurysmformation. The various aspects of management of such individuals are discussed, andthe relevant literature has been reviewed in an attempt to provide a systematic approachto these difficult patients.The methods for assessing collateral circulation are both clinical and radiological
with trial clamping of the aorta and pressure measurement as the most reliable ultimatetest. A pressure of 50 mmHg in the distal aorta is accepted as indicating an adequateperipheral circulation, but it is recommended that the trial clamping should alwaysinclude both the left subclavian artery and any particularly large local collaterals. Theuse of a perfusion technique to sustain the distal tissues is also recommended,although local bypass shunts have a place when their use is dictated in the interests ofsafety for the patient.
From the early days of coarctation surgery latecomplications have been recognized and recorded(Owens and Swan, 1963). These have been relatedto infection (Martin, Kirklin, and DuShane, 1956;Roesch and Bond, 1960; Oldham et al., 1973),unfavourable anatomy, inadequacies of technique,and, in small children, the problem of growthfailure at the suture line (Parsons and Astley,1966).The question of late reoperation is often not an
easy one and the second operation itself can bedifficult and dangerous. Apart from the localhazards in the region of the previous repair,which can include aneurysm formation, denseadhesion to surrounding structures, and abnormalthinning of the aortic wall (Cerilli and Lauridsen,1965), the most serious risk in reoperation is thatof spinal cord damage and consequent paralysis(Brewer et al., 1972). This risk is related to theefficiency of the collateral circulation when theaorta is clamped or to the efficiency of the method
31
chosen to protect the distal tissues when aorticblood flow is interrupted. The state of the col-lateral circulation itself at the time of the secondoperation reflects the presence or absence ofresidual or recurrent aortic obstruction and itsduration and degree when present.
This communication describes the problempresented by three patients, all requiring latesecond operation, who had respectively total, par-tial, and no obstruction to the aortic lumen at thetime of their reoperation. The three patientsrepresent, therefore, both in the local condition atthe coarctation site and in the varying degree ofaortic obstruction an almost complete illustrationof the problems which have to be faced when asecond operation is needed.
PATIENTS
CASE 1 M. K. aged 35. Coarctation of the aorta wasdiscovered during the course of investigation for aurinary tract infection at the age of 22.
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
J. K. Ross, J. L. Monro, and C. G. Sbokos
At the first operation, undertaken at another hospi-tal in August 1961, a one-inch narrowed segment ofaorta was resected and replaced by a tubular Teflonprosthesis. The femoral pulses did not reappear post-operatively and the patient experienced pain in thelegs and an unusual amount of dyspnoea. She subse-quently had two successful full-term pregnancies.Twelve years after her first operation she presented
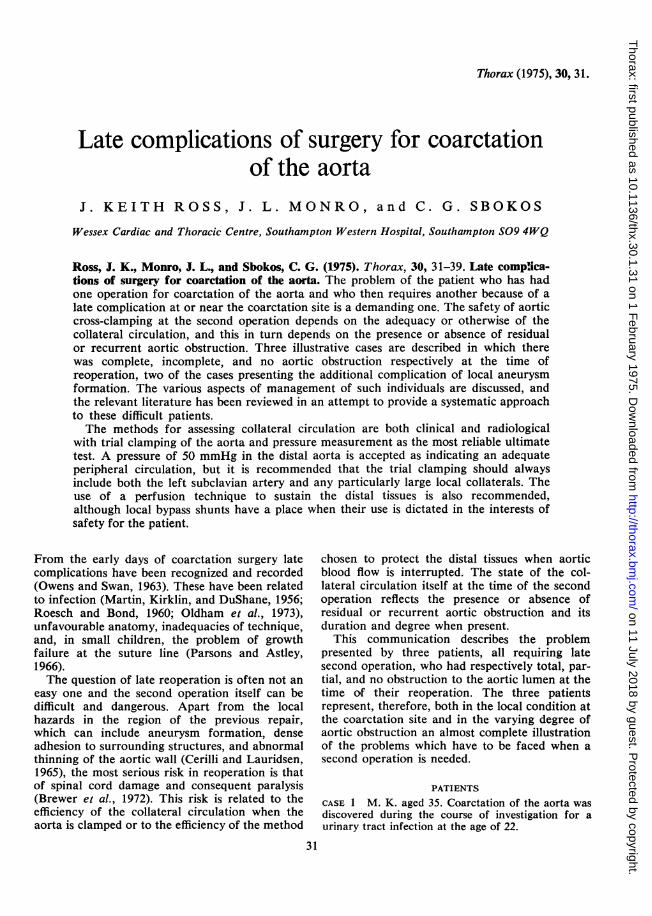
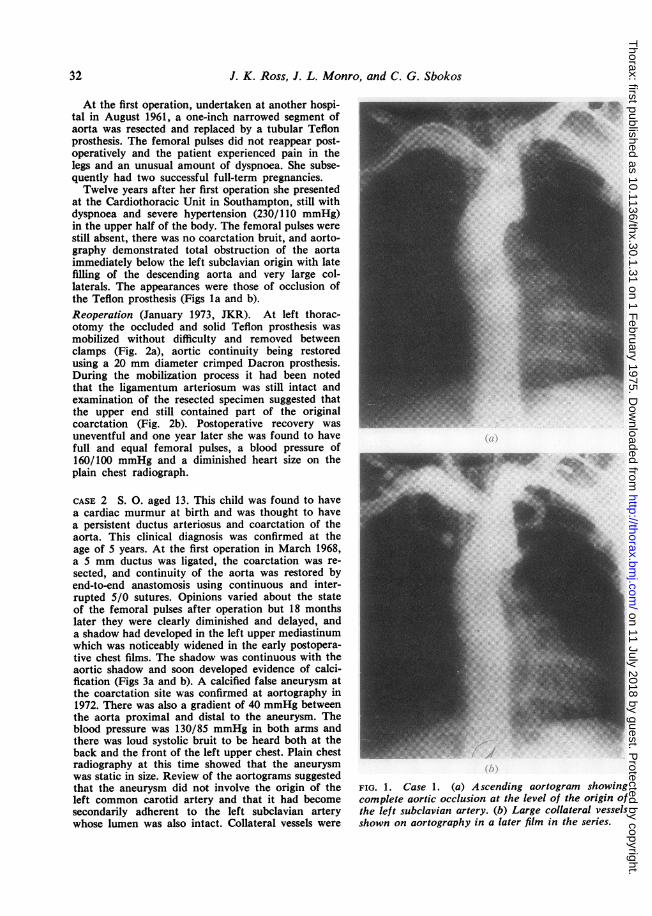
at the Cardiothoracic Unit in Southampton, still withdyspnoea and severe hypertension (230/110 mmHg)in the upper half of the body. The femoral pulses werestill absent, there was no coarctation bruit, and aorto-graphy demonstrated total obstruction of the aortaimmediately below the left subclavian origin with latefilling of the descending aorta and very large col-laterals. The appearances were those of occlusion ofthe Teflon prosthesis (Figs la and b).Reoperation (January 1973, JKR). At left thorac-otomy the occluded and solid Teflon prosthesis wasmobilized without difficulty and removed betweenclamps (Fig. 2a), aortic continuity being restoredusing a 20 mm diameter crimped Dacron prosthesis.During the mobilization process it had been notedthat the ligamentum arteriosum was still intact andexamination of the resected specimen suggested thatthe upper end still contained part of the originalcoarctation (Fig. 2b). Postoperative recovery wasuneventful and one year later she was found to havefull and equal femoral pulses, a blood pressure of160/100 mmHg and a diminished heart size on theplain chest radiograph.
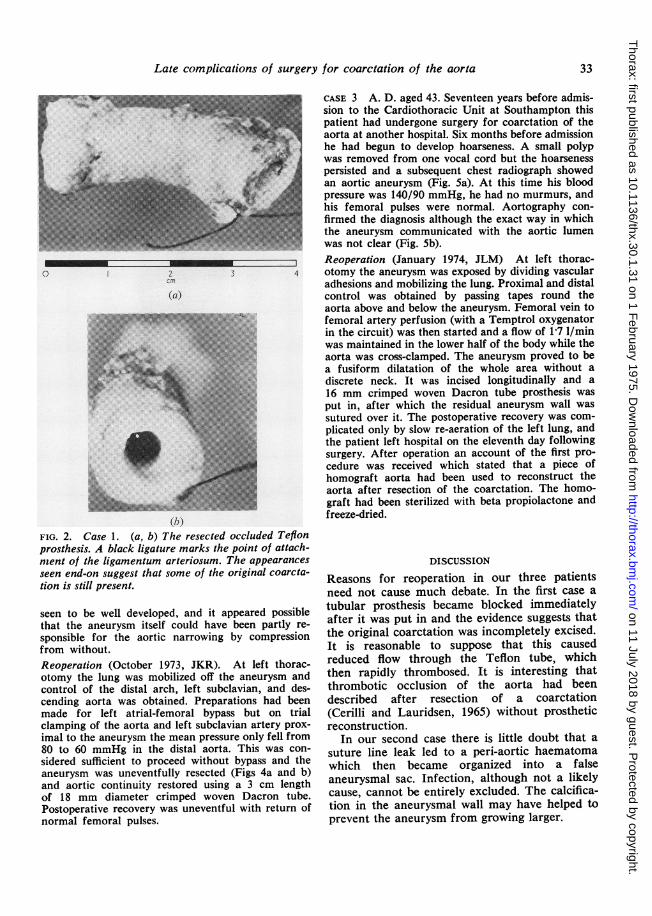
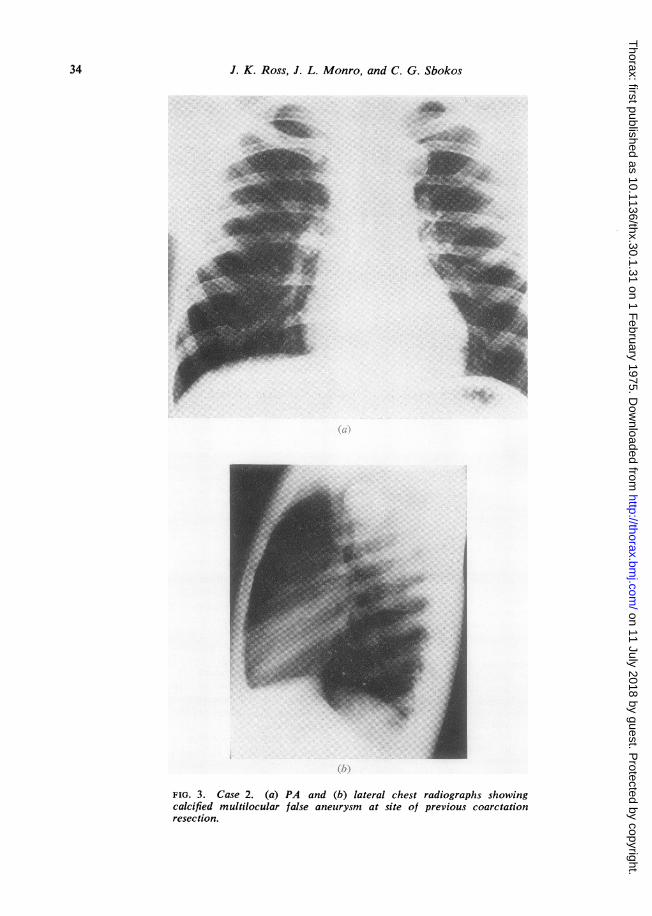
CASE 2 S. 0. aged 13. This child was found to havea cardiac murmur at birth and was thought to havea persistent ductus arteriosus and coarctation of theaorta. This clinical diagnosis was confirmed at theage of 5 years. At the first operation in March 1968,a 5 mm ductus was ligated, the coarctation was re-sected, and continuity of the aorta was restored byend-to-end anastomosis using continuous and inter-rupted 5/0 sutures. Opinions varied about the stateof the femoral pulses after operation but 18 monthslater they were clearly diminished and delayed, anda shadow had developed in the left upper mediastinumwhich was noticeably widened in the early postopera-tive chest films. The shadow was continuous with theaortic shadow and soon developed evidence of calci-fication (Figs 3a and b). A calcified false aneurysm atthe coarctation site was confirmed at aortography in1972. There was also a gradient of 40 mmHg betweenthe aorta proximal and distal to the aneurysm. Theblood pressure was 130/85 mmHg in both arms andthere was loud systolic bruit to be heard both at theback and the front of the left upper chest. Plain chestradiography at this time showed that the aneurysmwas static in size. Review of the aortograms suggestedthat the aneurysm did not involve the origin of theleft common carotid artery and that it had becomesecondarily adherent to the left subclavian arterywhose lumen was also intact. Collateral vessels were
FIG. 1. Case 1. (a) Ascending aortogram showingcomplete aortic occlusion at the level of the origin ofthe left subclavian artery. (b) Large collateral vesselsshown on aortography in a later film in the series.
32
i"
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
Late complications of surgery for coarctation of the aorta
0
2
cm
(a)
(b)FIG. 2. Case 1. (a, b) The resected occluded Teflonprosthesis. A black ligature marks the point of attach-nient of the ligamentum arteriosum. The appearances
seen end-on suggest that some of the original coarcta-tion is still present.
seen to be well developed, and it appeared possiblethat the aneurysm itself could have been partly re-
sponsible for the aortic narrowing by compressionfrom without.Reoperation (October 1973, JKR). At left thorac-otomy the lung was mobilized off the aneurysm andcontrol of the distal arch, left subclavian, and des-cending aorta was obtained. Preparations had beenmade for left atrial-femoral bypass but on trialclamping of the aorta and left subclavian artery prox-imal to the aneurysm the mean pressure only fell from80 to 60 mmHg in the distal aorta. This was con-
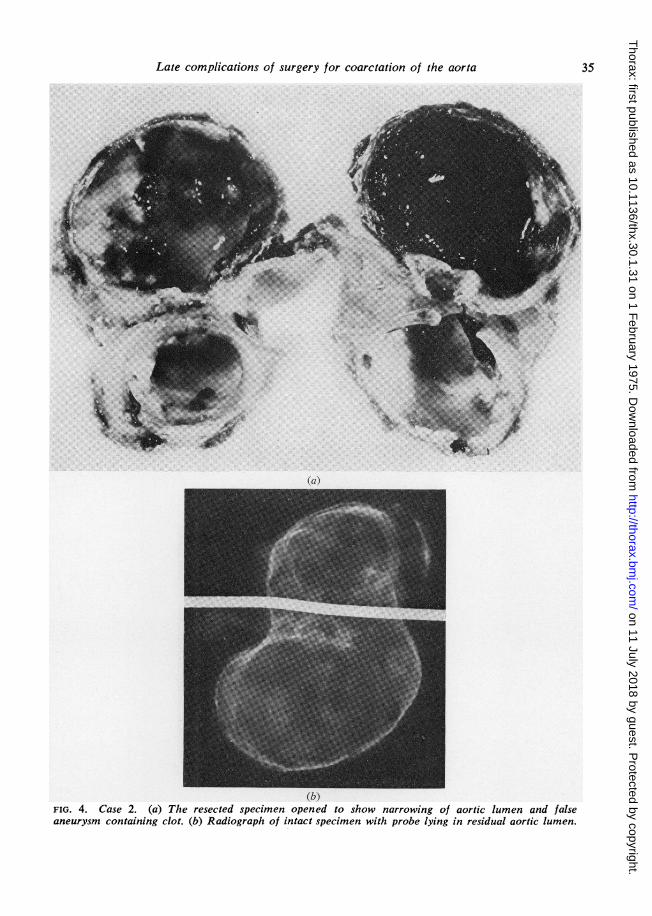
sidered sufficient to proceed without bypass and theaneurysm was uneventfully resected (Figs 4a and b)and aortic continuity restored using a 3 cm lengthof 18 mm diameter crimped woven Dacron tube.Postoperative recovery was uneventful with return ofnormal femoral pulses.
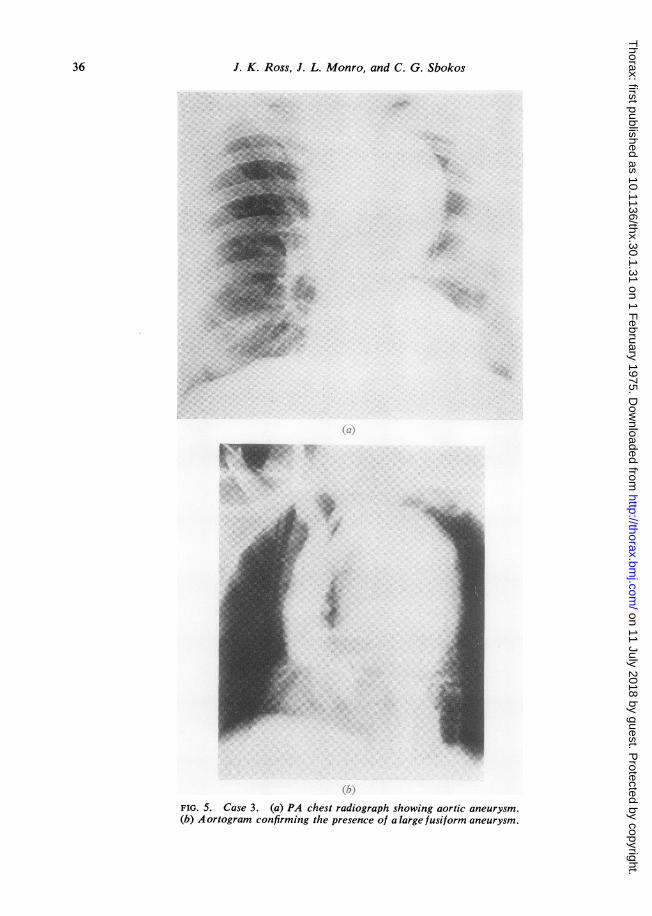
CASE 3 A. D. aged 43. Seventeen years before admis-sion to the Cardiothoracic Unit at Southampton thispatient had undergone surgery for coarctation of theaorta at another hospital. Six months before admissionhe had begun to develop hoarseness. A small polypwas removed from one vocal cord but the hoarsenesspersisted and a subsequent chest radiograph showedan aortic aneurysm (Fig. Sa). At this time his bloodpressure was 140/90 mmHg, he had no murmurs, andhis femoral pulses were normal. Aortography con-firmed the diagnosis although the exact way in whichthe aneurysm communicated with the aortic lumenwas not clear (Fig. 5b).Reoperation (January 1974, JLM) At left thorac-otomy the aneurysm was exposed by dividing vascularadhesions and mobilizing the lung. Proximal and distalcontrol was obtained by passing tapes round theaorta above and below the aneurysm. Femoral vein tofemoral artery perfusion (with a Temptrol oxygenatorin the circuit) was then started and a flow of 1-7 1/minwas maintained in the lower half of the body while theaorta was cross-clamped. The aneurysm proved to bea fusiform dilatation of the whole area without adiscrete neck. It was incised longitudinally and a16 mm crimped woven Dacron tube prosthesis wasput in, after which the residual aneurysm wall wassutured over it. The postoperative recovery was com-plicated only by slow re-aeration of the left lung, andthe patient left hospital on the eleventh day followingsurgery. After operation an account of the first pro-cedure was received which stated that a piece ofhomograft aorta had been used to reconstruct theaorta after resection of the coarctation. The homo-graft had been sterilized with beta propiolactone andfreeze-dried.
DISCUSSION
Reasons for reoperation in our three patientsneed not cause much debate. In the first case atubular prosthesis became blocked immediatelyafter it was put in and the evidence suggests thatthe original coarctation was incompletely excised.It is reasonable to suppose that this causedreduced flow through the Teflon tube, whichthen rapidly thrombosed. It is interesting thatthrombotic occlusion of the aorta had beendescribed after resection of a coarctation(Cerilli and Lauridsen, 1965) without prostheticreconstruction.
In our second case there is little doubt that asuture line leak led to a peri-aortic haematomawhich then became organized into a falseaneurysmal sac. Infection, although not a likelycause, cannot be entirely excluded. The calcifica-tion in the aneurysmal wall may have helped toprevent the aneurysm from growing larger.
33
3
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
J. K. Ross, J. L. Monro, and C. G. Sbokos
= .-_.... '5°.:>' . #.wi-_12';::: .... s$-*: b:. .*_b |. _t.6.}t_j 6: :a:
'F PaP.
i_L@. 1@|3.. ;s 0s.
s. _._l _.#:. '_. :: _¢. F ................. -z.;:
a F
..:a-W;_i w ..'....2..:.!:.
r_E ,Eg.=,.'_...W'' _ |
r l_F 1_EL.... _|- _.F 11N 1...... 1 , ' .......... ]! 1 .jo .j1
......... .
._ I
.|_ ,l
FIG. 3. Case 2. (a) PA and (b) lateral chest radiographs showingcalcified multilocular false aneurysm at site of previous coarctationresection.
34
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
Late complications of surgery for coarctation of the aorta
(a)
(b)FIG. 4. Case 2. (a) The resected specimen opened to show narrowing of aortic lumen and falseaneurysnm containing clot. (b) Radiograph of intact specimen with probe lying in residual aortic lumen.
35
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
J. K. Ross, J. L. Monro, and C. G. Sbokos
t.,.....*, ..
.
, #.oNf :_ :
.: _
.- .;: :i3_
_*i3._
.'._BB.! . ........ . s:. ::.- ': :>
_11' £w° ..:w_
..S.:X.' '.:
: *_*.....
1/
FIG. 5. Case 3. (a) PA chest radiograph showing aortic aneurysm.(b) Aortogram confirming the presence of alarge fusiform aneurysm.
36
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
Late complications of surgery for coarctation of the aorta
In the third case, the fusiform aneurysm wasdue to degenerative change in the segment ofchemically sterilized, freeze-dried homograft aortainserted at the primary operation. Aneurysmaldilatation of a Dacron graft has also been re-ported (Stankowiak and Soots, 1973).Aneurysms can occur in the region of a coarcta-
tion repair due to infection on the suture line(Martin et al., 1956; Roesch and Bond, 1960;Davis, Fell, and Taylor, 1965) when the prob-lems of management have much in common withthe spontaneously occurring mycotic aneurysm(Khazei and Cowley, 1967; Oldham et al., 1973)although the unpredictable early regression ofcollaterals should influence the surgical tactics inthe postoperative variety. Aneurysms can alsooccur at the site where a clamp was applied to theaorta (Gazzaniga, 1966) or can involve the areaof the suture line without identifiable aetiology(Blickman, 1949; Frederiksen, Poulsen, andDavidsen, 1961).The presence of an aneurysm, provided that it
is not infected, is less important than the problemof the reliability of the collateral circulation whena second operation is needed, and this in turndepends on the degree of aortic obstructionpresent. If, following any type of operation forcoarctation, complete obstruction of the aorticlumen remains (as in case 1), there can be nodoubt that if it was considered safe to clamp theaorta at the first operation it will be so at thesecond. Any collaterals that had to be divided atthe first procedure represent the only differencebetween the two preoperative situations. Con-versely, if there is no aortic obstruction (as incase 3), it must be assumed that there are noeffective collaterals. It is the intermediate type ofcase that represents the real problem, when therecurrent or residual obstruction is incomplete (asin case 2). This is typified by the patient whoseprimary repair was in infancy (Parsons andAstley, 1966; Khoury and Hawes, 1968; Ibarra-Perez et al., 1969; Tawes et al., 1969; Eshaghpourand Olley, 1972) but the uncertainty about howmuch regression and re-establishment of the col-lateral circulation has occurred applies to allindividuals in this category regardless of their ageat the primary procedure.
PREOPERATIVE ASSESSMENT OF COLLATERAL CIRCU-LATION Clinical assessment of a collateral circula-tion may be difficult or misleading unless there areobviously palpable chest wall vessels combinedwith diminished and delayed or absent femoralpulses. Conversely, easily felt femoral pulses and a
loud coarctation bruit, indicating less importantaortic obstruction, must raise doubts about thestate of the collateral supply.
Radiological assessment is more valuable butdemands high quality aortography with sufficienttime lapse during the study for the collateralvessels to fill and be clearly demonstrated.The velocity of flow in superficial collaterals
may be measured by the Doppler method (Ben-chimol, Baldi, and Desser, 1973) but this tech-nique has not yet been used enough for one to besure of its usefulness.A study of the records of the first operation
and the patient's postoperative course can givesome indication of both the duration and theseverity of any residual or recurrent aortic ob-struction and, therefore indirectly, of the likelystate of the collateral circulation.
ASSESSMENT OF COLLATERAL CIRCULATION AT OPERA-TION An estimate of the size and number of col-lateral vessels may be made as the chest is opened,and failure to encounter the characteristic vesselsin the chest wall may be the first indication thatthe collateral circulation is poor. If, as is likely,the chest is being reopened in the line of the pre-vious incision, this may not be a valid sign.
Trial clamping of the aorta with measurementof intra-aortic pressure proximal and distal to theclamp (Hughes and Reemtsma, 1971) is acceptedas a method of judging the efficiency of the col-lateral circulation. A mean pressure of 50 mmHgdistal to the clamp is regarded as the criticalpressure below which some form of circulatorysupport is needed for the lower half of the body.Ideally, this manoeuvre should be combined withestimates of blood flow in the descending aorta,and this would be a logical extension of the flowstudies reported by Schenk, McDonald, andAndersen (1965). We agree that trial clamping isa valuable manoeuvre and that a pressure of50 mmHg (mean) is an acceptable arbitrary levelto set, but the method should routinely includeocclusion of the left subclavian artery and also ofany particularly large collaterals entering closeto the coarctation distally which would have tobe ligated or clamped during the subsequent re-pair. We also feel that although trial clampingmay be regarded as the most precise way ofassessing the adequacy of the collateral circula-tion, it is dangerous to base the judgement of thesafety of aortic cross-clamping on a single para-meter. The final decision must therefore take intoaccount all the available clinical and radiological
37
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
J. K. Ross, J. L. Monro, and C. G. Sbokos
evidence and must always err on the side ofsafety if there is the slightest doubt, although thispoint of view would not be shared by Crawfordand Rubio (1973), who advocate aortic cross-clamping at normal temperature without the useof shunts or circulatory support when treatinganeurysms of the descending thoracic aorta.There are various methods available for pro-
tecting the tissues distal to the site of aorticclamping, assuming that preservation of inter-costal and other collateral vessels is an integralpart of the surgical technique. Here the tech-nique of plastic reconstruction of the aorta des-cribed by Vosschulte (1961) has much torecommend it as the need for extensive mobiliza-tion of the aorta, and therefore the threat tocollateral vessels, is much reduced. Some favourhypothermia (Dubost, cited by Brewer et al.,1972) as a routine adjunct to all secondary pro-cedures. Others use temporary or permanent by-pass shunts electively in such instances (Lam andArciniegas, 1973; Skagseth and Froysaker, 1973;Weldon et al., 1973), and in difficult cases thetechnique described by Weldon, which does notinvolve aortic cross-clamping, is attractive. It ispossible, however, that the abnormal thinning ofthe aortic wall which may be found at secondaryprocedures make these methods difficult to applyuniversally with safety.
In common with many other authors, we favourthe use of a perfusion technique, either left atrial-femoral bypass (Gerbode et al., 1957; Braim-bridge, 1963) or veno-arterial femoral bypass(Neville et al., 1968), not only as a safe and flexiblemethod which ensures an adequate and measur-able blood supply to the lower half of the bodybut as a means of decompressing the proximalcirculation when the aorta is cross-clamped. Fur-ther, we would agree with the opinion expressedby others (Hughes and Reemtsma, 1971) that suchfacilities should always be available when surgeryof this kind is undertaken.
Spinal cord complications with coarctation ofthe aorta have recently been well reviewed(Brewer et al., 1972) together with the vagaries ofthe spinal cord's blood supply and the factorsconsidered important in causing and preventingspinal cord damage. It is clear that no methodfor protecting the spinal cord at primary orsecondary operation can be regarded as totallysafe, and the fact that coarctation can be associ-ated with spontaneous cord lesions without sur-gery emphasizes the unpredictable nature of thedisease complex. Perfusion support for the distalcirculation represents the most reliable method
available for protection of the tissues beyond thelevel of aortic cross-clamping. Temporary or per-manent local bypass shunt procedures, which canbe made without aortic clamping, also have aplace, particularly when mobilization of the aortaproximally and distally is likely to be moredangerous than the introduction of the shunt.
REFERENCES
Benchimol, A., Baldi, J., and Desser, K. B. (1973).Measurement of phasic scapular and intercostalcollateral arterial blood velocity in coarctation ofthe aorta. Chest, 63, 1015.
Blickman, J. R. (1949). A case of aneurysm of theaorta after resection for coarctation (cured byexcision). Archivum Chirurgicum Neerlandicum,1, 50.
Braimbridge, M. V. (1963). Surgery of the descendingthoracic aorta. Annals of Royal College of Sur-geons of England, 33, 344.
Brewer, L. A., Fosburg, R. G., Mulder, G. A., andVerska, J. J. (1972). Spinal cord complicationsfollowing surgery for coarctation of the aorta.Journal of Thoracic and Cardiovascular Surgery,64, 368.
Cerilli, J. and Lauridsen, P. (1965). Reoperation forcoarctation of the aorta. Acta Chirurgica Scan-dinavica, 129, 391.
Crawford, E. S. and Rubio, P. A. (1973). Reappraisalof adjuncts to avoid ischemia in the treatment ofaneurysms of descending thoracic aorta. Journalof Thoracic and Cardiovascular Surgery, 66, 693.
Davis, C. B., Fell, E. H., and Taylor, C. B. (1965).Postoperative aneurysm following surgery forcoarctation of aorta. Surgery, Gynaecology andObstetrics, 121, 1043.
Eshaghpour, E. and Olley, P. M. (1972). Recoarcta-tion of the aorta following coarctectomy in thefirst year of life: a follow-up study. Journal ofPediatrics, 80, 809.
Frederiksen, T., Poulsen, T., and Davidsen, H. G.(1961). True aortic aneurysm following resectionof coarctation of the aorta. A cta Chirurgica Scan-dinavica, Supplement, 283, p. 188.
Gazzaniga, A. B. (1966). Complications of coarctationresection: pseudoaneurysm following total aorticdistraction. Annals of Thoracic Surgery, 2, 840.
Gerbode, F., Braimbridge, M., Osborn, J. J., Hood,M., and French, S. (1957). Traumatic thoracicaneurysms: treatment by resection and graftingwith the use of an extracorporeal bypass. Surgery,42, 975.
Hughes, R. K. and Reemtsma, K. (1971). Correctionof coarctation of the aorta; manometric deter-mination of safety during test occlusion. Journalof Thoracic and Cardiovascular Surgery, 62, 31.
Ibarra-P6rez, C., Castafieda, A. R., Varco, R. L., andLillehei, C. W. (1969). Recoarctation of the aorta.Nineteen year clinical experience. AmericanJournal of Cardiology, 23, 778.
38
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from
Late complications of surgery for coarctation of the aorta
Khazei, A. H. and Cowley, R. A. (1967). Mycoticaneurysm associated with coarctation of theaorta. American Surgeon, 33, 325.
Khoury, G. H. and Hawes, C. R. (1968). Recurrentcoarctation of the aorta in infancy and child-hood. Journal of Pediatrics, 72, 801.
Lam, C. R. and Arciniegas, E. (1973). Surgicalmanagement of coarctation of the aorta withminimal collateral circulation. A nnals of Surgery,178, 693.
Martin, W. J., Kirklin, J. W., and Dushane, J. W.(1956). Aortic aneurysm and aneurysmal endar-teritis after resection for coarctation. Journal ofthe American Medical Association, 160, 871.
Neville, W. E., Cox, W. D., Leininger, B., and Pifarr6,R. (1968). Resection of the descending thoracicaorta with femoral vein to femoral artery oxygen-ation perfusion. Journal of Thoracic and Cardio-vascular Surgery, 56, 39.
Oldham, H. N., Phillips. J. F., Jewett, P. H., andChen, J. T. (1973). Surgical treatment of mycoticaneurysm associated with coarctation of the aorta.Annals of Thoracic Surgery, 15, 411.
Owens, J. C. and Swan, H. (1963). Complications inthe repair of coarctation of the aorta. Journal ofCardiovascular Surgery, 4, 816.
Parsons, C. G. and Astley, R. (1966). Recurrence ofaortic coarctation after operation in childhood.British Medical Journal, 1, 573.
Roesch, C. B. and Bond, J. W. (1960). False aneurysmdue to an infccted aortic anastomosis. AmericanJournal of Surgery, 99, 90.
Schenk, W. G., McDonald, K. E., and Andersen,M. N. (1965). Blood flow measurements in humancoarctation. Studies on descending aorta and leftsubclavian and intercostal arteries before andafter excision with repair. Journal of Thoracicand Cardiovascular Surgery, 50, 26.
Skagseth, E. and Froysaker, T. (1973). Temporary andpermanent bypass prostheses in the treatment ofaortic coarctation. Scandinavian Journal ofThoracic and Cardiovascular Surgery, 7, 249.
Stankowiak, C. and Soots, G. (1973). Faux aneurisme12 ans apres resection-greffe par prosthese endacron pour coarctation de l'aorte. Annales deChirurgie Thoracique et Cardiovasculaire, 11, 377.
Tawes, R. L., Aberdeen, E., Waterston, D. J., andBonham-Carter, R. E. (1969). Coarctation of theaorta in infants and children. A review of 333operative cases, including 179 infants. Circulation,39 and 40, Supplement 1, p. 173.
Vosschulte, K. (1961). Surgical correction of coarcta-tion of the aorta by an 'isthmusplastic' operation.Thorax, 16, 338.
Weldon, C. S., Hartmann, A. F., Steinhoff, N. G., andMorrissey, J. D. (1973). A simple, safe, and rapidtechnique for the management of recurrent co-arctation of the aorta. Annals of Thoracic Sur-gery, 15, 510.
Requests for reprints to: J. K. Ross, F.R.C.S.,Wessex Cardiac and Thoracic Centre, SouthamptonWestern Hospital, Southampton, S09 4WQ.
39
on 11 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.31 on 1 February 1975. D
ownloaded from