
Lasers in Dentistry (2) / orthodontic courses by Indian dental academy
58
LASERS IN DENTISTRY Introduction Laser is an acronym, which stands for light amplification by stimulated emission of radiation. Several decades ago, the laser was a death ray, the ultimate weapon of destruction, something you would only find in a science fiction story. Then lasers were developed and actually used, among other places, in light shows. The beam sparkled, it showed pure, vibrant and intense colors. Today the laser is used in the scanners at the grocery store, in compact disc players, and as a pointer for lecturer and above all in medical and dental field. The image of the laser has changed significantly over the past several years. With dentistry in the high tech era, we are fortunate to have many technological innovations to enhance treatment, including intraoral video 1
-
Upload
indian-dental-academy -
Category
Documents
-
view
214 -
download
0
Transcript of Lasers in Dentistry (2) / orthodontic courses by Indian dental academy
LASERS IN DENTISTRY
Introduction
Laser is an acronym, which stands for light amplification by
stimulated emission of radiation. Several decades ago, the laser was a
death ray, the ultimate weapon of destruction, something you would
only find in a science fiction story. Then lasers were developed and
actually used, among other places, in light shows. The beam sparkled, it
showed pure, vibrant and intense colors. Today the laser is used in the
scanners at the grocery store, in compact disc players, and as a pointer
for lecturer and above all in medical and dental field. The image of the
laser has changed significantly over the past several years.
With dentistry in the high tech era, we are fortunate to have many
technological innovations to enhance treatment, including intraoral
video cameras, CAD-CAM units, RVGs and air-abrasive units.
However, no instrument is more representative of the term high-tech
than, the laser. Dental procedures performed today with the laser are so
effective that they should set a new standard of care.
This presentation intends to discuss the role of lasers in dentistry.
1

History of Lasers
Approximately, the history of lasers begins similarly to much of
modern physics, with Einstein. In 1917, his paper in Physikialische
Zeil, “Zur Quantern Theorie der Strahlung”, was the first discussion
of stimulated emission.
In 1954 Townes and Gordon built the first microwave laser or better
known as ‘MASER’ which is the acronym for ‘Microwave
Amplification by stimulated Emission of Radiation’
In 1958, Townes, working with Schawlow at Bell Laboratories,
published the first theoretic calculations for a visible light maser –
or what was then called a LASER.
In May 1960, Theodore Maimen at Hughes Aircraft company made
the first laser. He used a ruby as the laser medium.
One of the first reports of laser light interacting with tissue was from
Zaret; he measured the damage caused by lasers incident upon rabbit
retina and iris.
The first gas laser was developed by Javan et al in 1961. This was
the first continuous laser and used helium – neon.
2
The Nobel Prize for the development of the laser was awarded to
Townes, Basor and Prokhovov in 1964.
The neodymium – doped (Nd): glass laser was developed in 1961 by
Snitzer.
In 1964 Nd: YAG was developed by Geusic.
The CO2 laser was invented by Patel et al in 1965.
In 1968 Polanyi developed articulating arms to deliver CO2 laser to
remote areas.
Polanyi in 1970 applied CO2 laser clinically.
In 1990 Ball suggested opthalmologic application of ruby laser.
Laser Physics
Laser is a device that converts electrical or chemical energy into
light energy.
In contrast to ordinary light that is emitted spontaneously by
excited atoms or molecules, the light emitted by laser occurs when an
atom or molecule retains excess energy until it is stimulated to emit it.
3

The radiation emitted by lasers including both visible and invisible light
is more generally termed as electromagnetic radiation. The concept of
stimulated emission of light was first proposed in 1917 by Albert
Einstein.
He described three processes:
1. Absorption
2. Spontaneous emission
3. Stimulated emission.
Einstein considered the model of a basic atom to describe the
production of laser. An atom consists of centrally placed nucleus which
contains +vely charged particles known as protons, around which the
negatively charged particles. i.e. electrons are revolving.
When an atom is struck by a photon, there is an energy transfer
causing increase in energy of the atom. This process is termed as
absorption. The photon then ceases to exist, and an electron within the
atom pumps to a higher energy level. This atom is thus pumped up to an
excited state from the ground state.
In the excited state, the atom is unstable and will soon
spontaneously decay back to the ground state, releasing the stored
4

energy in the form of an emitted photon. This process is called
spontaneous emission.
If an atom in the excited state is struck by a photon of identical
energy as the photon to be emitted, the emission could be stimulated to
occur earlier than would occur spontaneously. This stimulated
interaction causes two photons that are identical in frequency and
wavelength to leave the atom. This is a process of stimulated emission.
If a collection of atoms includes, more that are pumped into the
excited state that remain in the resting state, a population inversion
exists. This is necessary condition for lasing. Now, the spontaneous
emission of a photon by one atom will stimulate the release of a second
photon in a second atom, and these two photon will trigger the release of
two more photons. These four than yield eight, eight yield sixteen and so
on. In a small space at the speed of light, this photon chain reaction
produces a brief intense flash of monochromatic and coherent light
which is termed as ‘laser’.
Properties of Laser
1. Coherent: Coherence of light means that all waves are in certain
phase relationship to each other both in space and time
5
2. Mono- chromatic: Characterized by radiation in which all waves are
of same frequency and wavelength.
3. Collimated: That means all the emitted waves are parallel and the
beam divergence is very low. This property is important for good
transmission through delivery systems.
4. Excellent concentration of energy: When a calcified tissue for eg.
dentin is exposed to the laser of high energy density, the beam is
concentrated at a particular point without damaging the adjacent
tissues even though a lot of temperature is produced ie 800-900oC.
5. Zero entropy.
Laser Design
The laser consist of following components.
1. A laser medium or active medium: This can be a solid, liquid or
gas. This lasing medium determines the wavelength of the light
emitted from the laser and the laser is named after the medium.
2. Housing tube or optical cavity:
Made up of metal, ceramic or both.
6
This structure encapsulates the laser medium.
Consists of two mirrors, one fully reflective and
the other partially transmittive, which are
located at either end of the optical cavity.
3. Some form of an external power source: This external power
source excites or “pumps” the atom in the laser medium to their
higher energy levels. A population inversion happens when there are
more atoms in the excited state rather than a non-excited state.
Atoms in the excited state spontaneously emit photons of light which
bounce back and forth between the two mirrors in the laser tube, they
strike other atoms, stimulating more spontaneous emission. Photons
of energy of the same wavelength and frequency escape through the
transmittive mirror as the laser beam. An extremely small intense
beam of energy that has the ability to vaporize, coagulate, and cut
can be obtained if a lens is placed in front of the beam. This lens
concentrates the emitted energy and allows for focussing to a small
spot size.
7
Laser Light Delivery
Light can be delivered by a numbered of different mechanisms.
Several years ago a hand held laser meant holding a larger, several
hundred pound laser usually the size of desk above a patient. Although
the idea was comical at the time, it is becoming more feasible as laser
technology is producing smaller and lighter weight lasers. In the more
future it is probable that hand held lasers will be used routinly in
dentistry.
1. Articulated arms
Laser light can be delivered by articulated arms, which are very
simple but elegant. Mirrors are placed at 45o angles to tubes carrying the
laser light. The tubes can rotate about the normal axis of the mirrors.
This results in a tremendous amount of flexibility in the arm and in
delivery of the laser light. This is typically used with CO2 laser. The arm
does have some disadvantages that include the arm counter weight and
the limited ability to move in straight line.
2. Optical Fiber
Laser light can be delivered by an optical fiber, which is
frequently used with near infrared and visible lasers. The light is trapped
8
in the glass and propagates down through the fiber in a process called
total internal reflection.
Optical fibers can be very small. They can be either tenths of
micros or greater than hundreds of microns in diameter. Advantages of
optical fiber is that they provide easy access and transmit high intensities
of light with almost no loss but have two disadvantages, one the beam is
no longer collimated and coherent when emitted from the fiber which
limits the focal spot size and second disadvantage is that the light is no
longer coherent.
Patient to laser
Another method of delivering laser light to the patient is actually
to bring the patient up to the laser. Eg: Slit lamp used in the
ophthalmologist gist has been doing this for quite some time. The
ophthalmic laser microscope is simply a slit lamp with a laser built into
it. The doctor simply images what he wants on the cornea or retina and
then pushes the foot pedal to deliver laser beam to the target.
Once the laser is produced, its output power may be delivered in
the following modes.
9

1. Continuous wave: When laser machine is set in a continuous wave
mode the amplitude of the output beam is expressed in terms of
watts. In this mode the laser emits radiation continuously at a
constant power levels of 10 to 100 w. Eg: CO2 laser
2. Gated: The output of a continuous wave can be interrupted by a
shutter that “chops” the beam into trains of short pulses. The speed
of the shutter is 100 to 500ms.
3. Pulsed: Lasers can be gated or pulsed electronically. This type of
gating permits the duration of the pulses to be compressed producing
a corresponding increase in peak power, that is much higher than in
commonly available continuous wave mode.
4. Super pulsed: The duration of pulse is one hundredth of
microseconds.
5. Ultra pulsed: This mode produces an output pulse of high peak
power that is maintained for a longer time and delivers more energy.
6. Q-scotched: Even shorter and more intense pulse can be obtained
with this mode.
10

Focussing
Lasers can be used in either a focussed mode or in a defocused
mode.
A focussed mode is when the laser beam hits the tissue at its focal
points or smallest diameter. This diameter is dependent on the size of
lens used. This mode can also be referred as cut mode. Eg. While
performing biopsies.
The other method is the defocused mode. By defocusing the laser
beam or moving the focal spot away from the tissue plane, this beam
size that hits the tissue has a greater diameter, thus causing a wider area
of tissue to be vaporized. However, laser intensity / power density is
reduced. This method is also known as ablation mode. Eg. In
Frenectomies. In removal of inflammatory papillary hyperplasias.
Contact and Non contact modes
In contact mode, the fiber tip is placed in contact with the tissue.
The charred tissue formed on the fiber tip or on the tissue outline
increases the absorption of laser energy and resultant tissue effects. Char
can be eliminated with a water spray and then slightly more energy will
be required to provide time efficient results. Advantage is that there is
control feed back for the operator.
11
Non contact mode: Fiber tip is placed away from the target tissue.
The clinician operates with visual control with the aid of an aiming
beam or by observing the tissue effect being created.
So generally laser can be classified as
Dental Lasers
Those work in
both
Solely in the non Contact & focussed Non contacted
contact mode &
defocused
Eg: CO2 Eg: Agon, HO : YAG,
Nd:YAG
Laser Types
I. Based on wavelength.
1. Soft lasers
2. Hard lasers
II.
12

Based on the type of active / lasing medium used
1. ArF excimer
2. KrF excimer
3. XeCl excimer
4. Argon ion
5. KTP
6. Ruby
7. Nd: YAG
8. HO: YAG
9. YSGG
10. Er: YAG
11. CO2
13
I.
1. Soft Lasers: With a wave length around 632mm Soft lasers are
lower power lasers.
Eg: He Ne, Gallium arsenide laser.
These are employed to relieve pain and promote healing eg. In
Apthous ulcers.
2. Hard lasers: Lasers with well known laser systems for possible
surgical application are called as hard lasers.
Eg: CO2, Nd: YAG, Argon, Er:YAG etc.
CO2 Lasers
The CO2 laser first developed by Palet et al in 1964 is a gas laser
and has a wavelength of 10,600 nanometers or 10.6 deep in the
infrared range of the electromagnetic opectrum.
CO2 lasers have an affinity for wet tissues regardless of tissue color.
14
The laser energy weakens rapidly in most tissues because it is
absorbed by water. Because of the water absorption, the CO2 laser
generates a lot of heat, which readily carbonizes tissues. Since this
carbonized or charred layer acts as a biological dressing, it should
not be removed.
They are highly absorbed in oral mucosa, which is more than 90%
water, although their penetration depth is only about 0.2 to 0.1mm.
There is no scattering, reflection, or transmission in oral mucosa.
Hence, what you see is what you get.
CO2 lasers reflect off mirrors, allowing access to difficult areas.
Unfortunately, they also reflect off dental instruments, making
accidental reflection to non-target tissue a concern.
CO2 lasers cannot be delivered fiber optically Advances in
articulated arms and hollow wave guide technologies, now provide
easy access to all areas of the mouth.
Regardless of the delivery method used, all CO2 lasers work in a non-
contact mode.
Of all the lasers for oral use, CO2 is the fastest in removing tissue.
15
As CO2 lasers are invisible, an aiming helium – neon (He Ne) beam
must be used in conjunction with this laser.
Nd: YAG Laser: Here a crystal of Yttrium – aluminum – garnet is
doped with neodymium. Nd: YAG laser, has wavelength of 1,064 nm
(0.106 ) placing it in the near infrared range of the magnetic spectrum.
It is not well absorbed by water but are attracted to pigmented tissue.
Eg: hemoglobin and melanin. Therefore various degrees of optical
scattering and penetration to the tissue, minimal absorption and no
reflection.
Nd: YAG lasers work either by a contact or non-contact mode. When
working on tissue, however, the contact mode in highly
recommended.
The Nd: YAG wavelength is delivered fiber optically and many sizes
of contact fibers are available. Carbonized tissue remains often build
of on the tip of the contact fiber, creating a ‘hot tip’. This increased
temperature enhances the effect of the Nd:YAG laser, and it is not
necessary to rinse the build up away. Special tips, the coated
sapphire tip, can be used to limit lateral thermal damage. A helium-
neon-aiming beam is generally used with Nd: YAG wavelength.
16
Penetration depth is ~ 2 to 4m, and can be varied by upto 0.5-4mm in
oral tissues by various methods.
A black enhancer can be used to speed the action.
Most dental Nd: YAG lasers work in a pulsed mode. At higher
powers and pulsing, a super heated gas called a plasma can form on
the tissue surface. It is the plasma that can be responsible for the
effects of either coagulation, vaporization or cutting. If not cooled
(e.g. by running a water stream down the fiber) the plasma can cause
damage to the surrounding tissues.
Suffer from dragability
The Nd:YAG beam is readily absorbed by amalgam, titanium and
non-precious metals, requiring careful operation in the presence of
these dental materials.
Argon Lasers
Argon lasers are those lasers in the blue-green visible spectrum.
They operate at 488nm or 514.5nm, are gas like CO2 lasers and are
easily delivered fiber optically like Nd:YAG.
17

Argon lasers have an affinity for darker colored tissues and also a
high affinity for hemoglobin, making them excellent coagulators. It
is not absorbed well by hard tissue, and no particular care is needed
to protect the teeth during surgery.
In oral tissues there is no reflection, some absorption and some
scattering and transmission.
Argon lasers work both in the contact and non contact mode
Like, Nd: YAG lasers, at low powers argon lasers suffer from
‘dragability’ and need sweeping motion to avoid tissue from
accumulating on the tip.
Enhances are not needed with Argon lasers.
Argon lasers also have the ability to cure composite resin, a feature
shared by none of the other lasers.
The blue wavelength of 488 nm is used mainly for composite curing,
while the green wavelength of 510nm is mainly for soft tissue
procedures and coagulation.
18
Er: YAG laser
Have a wavelength of 2.94 m.
A number of researchers have demonstrated the Er: YAG lasers
ability to cut, or ablate, dental hard tissue effectively and efficiently.
The Er: YAG laser is absorbed by water and hydroxyapatite, which
particularly accounts for its efficiency in cutting enamel and dentin.
Pulpal response to cavity preparation with an Er: YAG laser was
minimal, reversible and comparable with pulpal response created by
a high-speed drill.
Ho: YAG laser [Holmium YAG lasers]
Has a wavelength of 2,100 nm and is a crystal
Delivered through a fiber optic carrier.
A He-Ne laser is used as an aiming light
Dragability is less compared to Nd: YAG and argon lasers
Like Nd: YAG, can be used in both the contact and non-contact
modes and are pulsed lasers.
19
Ho: YAG laser has an affinity for white tissue and has ability to pass
through water and acts as a good coagulator.
Laser interaction with biologic tissues
Light can interact with tissues in four different mechanisms
1. Reflected
2. Scattered
3. Absorbed
4. Transmitted
Reflection: Reflected light bounces off the tissue surface and is
directed outward. Energy dissipates after reflection, so that there is little
danger of damage to other parts of mouth and it limits the amount of
energy that enters the tissue.
Scattering: occurs when the light energy bounces from molecule to
molecule within the tissue. It distributes the energy over a larger volume
of tissue, dissipating the thermal effects.
Absorption: occurs after a characteristic amount of scattering and is
responsible for the thermal effects within the tissue. It converts light
energy to heat energy The absorption properties of tissue and cells
20
depends on the type and amount of absorbing pigments or
chromophores. Eg. Hemoglobin, water, Melanin, Cytochromes etc.
Transmission: Light can also travel beyond a given tissue boundary.
This is called transmission. Transmission irradiates the surrounding
tissue and must be quantified. Its effects should be considered before
laser treatment can be justified.
Tissue effects on laser irradiation
When radiant energy is absorbed by tissue 4 basic types of
interactions occurs.
Laser effects on Dental Hard Tissues
The absorption and transmission of laser light in human teeth is
mainly dependent on the wavelength of the laser light.
For eg. – Ultraviolet laser light is well absorbed by teeth.
In water and in hydroxyapatite, there is a very low absorption at a
wavelength of 2m in comparison to high absorption of laser energy at
3m and 10m.
The laser effects can be grouped as:
1. Thermal effects:
21
The best known laser effect in dentistry is the thermal
vaporization of tissue by absorbing laser light i.e. the laser energy is
converted into thermal energy or heat that destroys the tissues.
From 45o – 60 o denaturation occurs
>60 o coagulation and necrosis
At 100 o C water inside tissue vaporizes
>300 o C carbonization and later phyrolysis
with vaporization of bulky
tissues.
2. Mechanical effects:
High energetic and short pulsed laser light can lead to a fast
heating of the dental tissues in a very small area. The energy dissipates
explosively in a volume expansion that may be accompanied by fast
shock waves. These shock waves lead to mechanical damage of the
irradiated tissue.
3. Chemical effects:
Here molecules can be associated directly with laser light of high
photon energies.
Histologic Results:
22
With continuous wave and pulsed CO2 lasers.
When continuous wave and pulsed CO2 lasers were used,
structural changes and damage in dental hard tissue were reported.
Microcracks and zones of necrosis and carbonization are unavoidable.
Because of drying effects, the microhardnes of dentin increases. The
crystalline structure of hydroxyapatite changes and a transformation of
apatite to tricalcium phosphate takes place.
Nd: YAG Lasers:
The Nd: YAG laser shows low absorption in water as well as in
hydroxyapatite. Therefore the laser power diffuses deeply through the
enamel and dentin and finally heats the pulp. In dentin, at the laser
impact, zones of debris and carbonization are surrounded by an area of
necrosis can be seen. Microcracks appear when energies above a
threshold of 100mj / pulse are used. But the appearance and the extent of
the side effects are not predictable.
Er: YAG Laser:
In dentin, shallow cavities were surrounded by a zone of necrosis
of 1-3m thickness when water-cooling systems were used. In deeper
23

cavities areas of carbonization and microcracks were observed. Ablating
enamel always cracked and deep zones of debris appeared.
Excimer Lasers:
No pathologic changes in the tissue layers adjacent to the
dissected areas were found after the ablation.
The ablation effects of dental hard tissues are predictable.
Compared to conventional diamond and burs, however, the effectiveness
is low. Thermal side effects increase as photon energies of excimer
lasers decrease.
Laser Effects On Dental Pulp:
Recent histologic evidence suggests that a normal odontoblasts
layer, stroma and viable epithelial root sheath can be retained following
laser radiation provided damage threshold energy densities are not
exceeded. If pulp temperatures are raised beyond the 5°C level, research
has shown that the odontoblasts layer may not be present.
Characteristics of the dentinogenesis process related to root
development, predentin and reparative dentin formation, dentinal bridge
presence, typically reflect the overall trauma that has been induced in
the odontoblasts.
24

Application of Lasers in Dentistry:
Application Possible Laser Types
Basic research
Laser tissue interaction
Technical development of applications
of lasers in dentistry
All types
All types
Measurement and diagnosis
Holography
Laser Doppler fowmetry
Spectroscopy (caries diagnosis)
He Ne, diodes
He Ne, diodes
Various types
Oral and Maxillofacial Surgery
Cutting and Coagulation
Photodynamic therapy
CO2, Nd: YAG, Ar, dye
Dye, Au-Cu vapour
Conservative dentistry
Preventive dentistry (fissure sealing)
Caries treatment
Composite resin light Curing
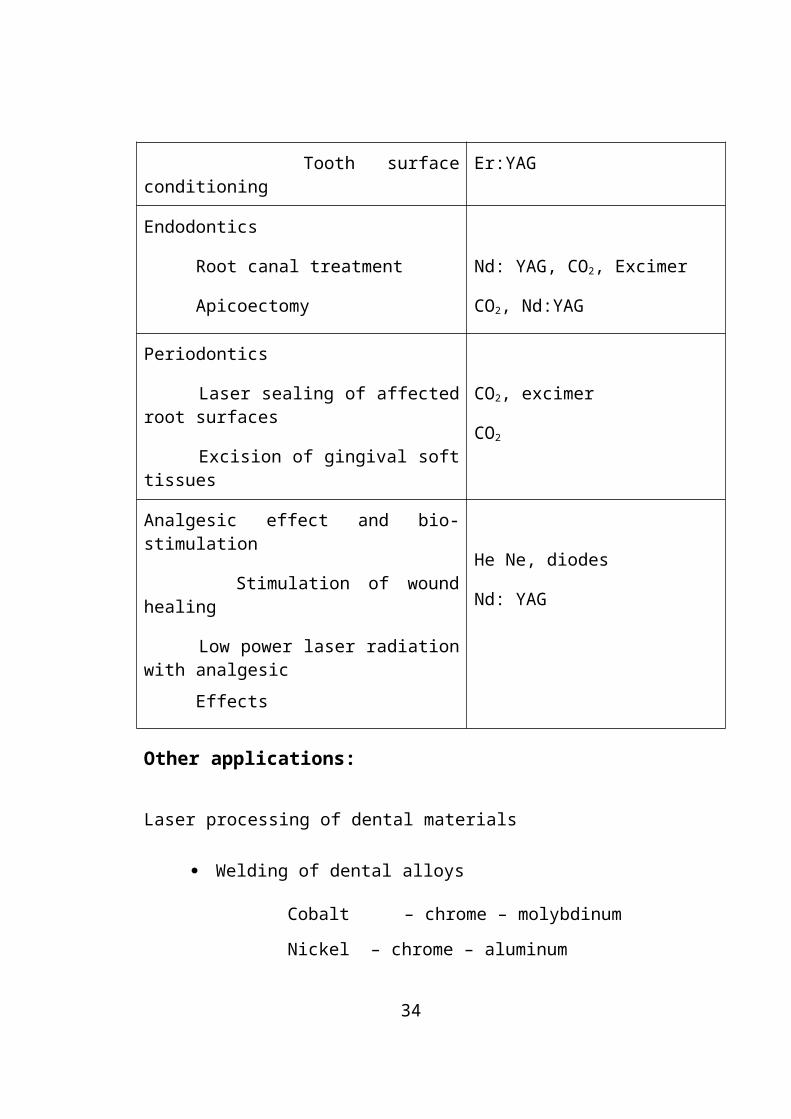
Tooth surface conditioning
CO2, Nd:YAG, ruby
CO2, Nd:YAG, Er: YAG, Excimer
Ar, dye, HeCd
Excimer, CO2, Nd:YAG, Er:YAG
Endodontics
Root canal treatment
Apicoectomy
Nd: YAG, CO2, Excimer
CO2, Nd:YAG
Periodontics
25
Laser sealing of affected root surfaces
Excision of gingival soft tissues
CO2, excimer
CO2
Analgesic effect and bio-stimulation
Stimulation of wound healing
Low power laser radiation with analgesic
Effects
He Ne, diodes
Nd: YAG
Other applications:
Laser processing of dental materials
Welding of dental alloys
Cobalt – chrome – molybdinum
Nickel – chrome – aluminum
Silver Palladium
Titanium alloys
Welding of ceramic materials
Still under investigation
Advantages of laser welding:
1. High bond strength and corrosion resistance since laser welding is a
form of sweating that does not use solders of different materials.
2. Reduced oxidation when argon gas is used for welding.
26

3. Decreased thermal influence and greater precision in processing than
with soldering or other techniques.
Laser in Restorative Dentistry and Endodontics
Lasers find numerous applications in restorative dentistry and
endodontics ranging from prevention of caries to antibacterial action in
root canals.
1. Prevention of carries:
Yamamoto and Oaya used as YAG laser at energy
densities of 10 to 20 J/cm³ and demonstrated that the lased
enamel surface was more resistant to in vitro
demineralization than non lased enamel.
Stern and Sognnaes demonstrated in vivo that enamel
subjected to 10 to 15 J/cm² showed a greater resistance to
dental caries than the controls.
Stern concluded that energy levels below 250 J/cm² did
not permanently alter the pulp but necrosis could occur
when energy level, reached 1800 J/cm² or higher.
27

Lobene and Collogues in their experiment with CO2 laser,
observed that CO2 irradiation to tooth enamel caused small
amounts of hydroxyapatite to be converted to more
insoluble calcium orthophosphate apatite. This paved the
way for widespread use laser in prevention of caries.
Lasers can be used for removal of incipient caries, sealing
pits and fissures. The CO2 and Nd:YAG lasers can remove
the organic and inorganic debris found in pits and fissures.
Following the removal a synthetic hydorxyapatite
compound is attached to enamel using the laser. Power
densities used are low and it did not alter the health of
pulp tissue.
In 1985 Terry Myers used Nd:YAG laser for debrident of
incipient caries.
When a topical fluoride treatment was performed after
argon laser conditioning of enamel, an even more dramatic
reduction in enamel acid demineralization was observed.
2. Diagnosis: Lasers can be used to detect incipient carious lesion
which cannot be diagnosed clinically and radiographically.
28

Transilliumination using lasers is used for this purpose. The lesion
appears as a distinct dark red area easily differentiated from the rest
of the sound tooth structure. Decalcified area appears as a dull,
opaque, orange color. Also enamel fractures and recurrent decay
around metallic and resin restoration can be diagnosed.
3. Laser Doppler Flowmetry: Pulpal blood flow can be assessed using
laser doppler flowmentry. He Ne and diodes can be used.
Cavity preparation:
The use of lasers for cavity preparation has been under scrutiny
for 20yrs as many investigators found that pulpal necrosis would occur
with use of lasers.
The reasons for necrosis are:
1. The heat produced
2. Total power output (J/cm²)
The search for laser that can be used to cut hard tissues begun in
1964 by Dr. Leo Goldman who used laser on his brother Bernard’s
teeth. The subsequent search included many laser wavelengths such as
29

CO2 but its disadvantages include cracking with flaking of enamel
surface.
Nd:YAG 10 J/cm² has shown to inhibit incipient carious lesions
but at higher densities it causes irreversible pulpal damage. Other lasers
such as Ho: YAG, ArF, Nd:YLF and Er: YAG have been investigated.
Er: YAG at the wavelength of 2.94m has shown most promising
results. A number of researchers have demonstrated the Er:YAG laser’s
ability to cut or ablate dental hard tissues effectively and efficiently. The
Er:YAG laser is absorbed by water and hydroxyapatite, which partially
accounts for its efficiency in cutting enamel and dentin.
It has generally been assumed that if pulpal temperature
rises less than 5.5°C, the procedure would be safe and
would not cause irreversible histologic damage to the
pulpal tissues. Researchers who conducted in vivo animal
studies reported that the pulpal response to cavity
preparation with an Er:YAG laser was minimal, reversible
and comparable with the pulpal response created by a high
speed drill.
30

The temperature rise with these type of laser was less than
3°C.
Moreover, a water coolent can be used which not only
cools the tooth during ablation but also increase the
efficiency of ablation.
In a study by Timothy Smith, patients reported little or no
pain during the treatment with dental laser. With many
people reporting fear of pain as then chief reason for not
seeking dental care, lasers may offer a more acceptable
treatment technique.
Etching the Enamel:
The laser absorbed by enamel causes the enamel surface to be
heated to a high temperature, generating micro cracks in the surface and
this aids in enhancing adhesion of composite to the tooth structure. The
surfaces appear similar to acid etched surfaces.
The Nd:YAG laser is not readily absorbed but absorption can be
increased by using a dye on enamel surface.
31

Curing of Composites and GIC:
Currently, photoactivated dental resins employ a diketone, such
as camphoroquinone, and a tertiary amine reducing agent to initiate
polymerization. This photoinitiator system is sensitive to light in blue
region of the visible spectrum with broad peak activity in the 480nm
region. The argon laser’s monochromatic wavelengths of 488nm and
514.5nm have been shown to be effective in the initiation of
polymerization of dental resins.
Advantages:
Enhanced physical properties like increased tensile
strength due to enhanced or more thorough
polymerization.
Improved adhesion
Reduced microleakage
Reduced exposure time. Argon laser polymerization
requires a 10sec cure cycle while visible light activation
usually takes approximately 40sec.
32

The polymerization of light activated bases and or liners
can also be accomplished with the argon laser.
Advantages : A wide verity of fiber sizes provides access to all location
of cavity preparation.
Pit and Fissure Sealant Therapy:
Advantages are similar to those offered for curing composite
resins.
Desensitization:
Lasers are effective tool in the treatment of hypersensitivity.
Mode of action is by blocking the dentinal tubules resulting in change in
hydraulic conductance.
Bleaching:
Lasers also find use in bleaching of vital and non-vital teeth.
Treatment of fractured teeth:
Lasers have the potential to fuse the segments of fractured teeth.
33
Pulpotomy:
Recent development
Removal of Old restoration:
Composites and cements can be ablated.
Gold crowns and cast fillings cannot be removal as laser beam
is reflected.
Ceramics cannot be ablated.
In endodontics:
For root canal preparation.
1. For Root Canal Preparation: Based on the SEM investigation of
prepared teeth, root canals appeared to be free of soft tissue and
debris. There was no smear layer detectable and there were no cases
of straightening or over instrumentation of the canals. The dentinal
tubules appeared to be open. These were no detectable thermal or
mechanical alteration to the root canal walls. There was a significant
reduction in bacterial growth (disinfection).
2. For sterilization of Files & Reamers
34

3. Apicoectomies:
for soft tissue procedures
for curing the retrograde filling materials.
Lasers in Surgical Systems:
Lasers are an alternative to conventional surgical systems. Stated
best by Apfelberg in 1987, lasers are a “new and different scalpel”
(optical knife, light scalpel).
Advantages:
Easy access to the anatomic site
Possess inherent hemostatic properties.
Capable of ablation of lesions in proximity to normal
structures, with minimal damage to normal structures.
Reduced pain during surgical procedures and less post
operative pain.
Enhanced healing
35
Bactericidal and virucidal effects of laser result in
decreased rates of wound infection.
Certain proven uses for dental soft tissue procedures using
lasers are:
1. Frenectomy
Maxillary midline
Lingual (Tongue tie)
2. Incisional and exasional biopsies.
3. Removal of benign lesions
Fibrous
Papillous
Pyogenic granuloma
Lichen Planus
Erosive lichen planus
Nicotinic stomatites
Verruca vulgaris
Inflammatory papillary hyperplasia
Epuli
4. Gingivoplasty
36

5. Soft tissue tuberosity reduction.
6. Soft tissue distal wedge procedure.
7. Gingivectomy
A. Removal of hyperplasias
1. Dilantin etc
2. Idopathic
B. Crown trough.
8. Aphthous ulcer
9. Operculectomy
10. Removal of hyperkeratotic lesions
11. Removal of malignant lesions
12. Soft tissue crown lengthening
13. Coagulation.
A. Graft donor sites.
B. Seepage around crown preparation.
14. Vestibuloplasty
15. Removal of granulation tissue – periodontal clean out
16. Removal of vascular lesions
A. Hemangioms
B. Pyogenic granuloma
37
17. Removal of lesion in patients with hemorrhagic disorders.A. Hemophelia etc.
18. Implants – Stage II – at the time of recovery.
A. Soft tissue removal
Bio-stimulation and Photodynamic Therapy:
Photodynamic therapy is an experimental cancer treatment that is
based on a cytotoxic photochemical reaction. This reaction requires
molecular oxygen, the photoactive drug dihematoporphyrin ether, a
hematophorphyrin derivative and intense light, which is typically
delivered by a laser. Dihematoporphyrin which is relatively retained in
malignant tissue after several days, is given intravenously to a patient.
Laser light at a wavelength corresponding to the absorption peak of the
drug is used to activate the drug to an excited state. The drug then reacts
with molecular oxygen to produce singlet oxygen, a highly reactive free
radical which ultimately leads to tissue necrosis.
Laser Hazards and Laser Safety:
The subject of dental laser safety is broad in scope, including not
only an awareness of the potential risks and hazards related to how
38

lasers are used, but also a recognition of existing standards of care and a
thorough understanding of safety control measures.
Laser Hazard Class for according to ANSI and OSHA Standards:
Class I - Low powered lasers that are safe to view
Class IIa - Low powered visible lasers that are hazards only when
viewed directly for longer than 1000 sec.
Class II - Low powered visible lasers that are hazardous when
viewed for longer than 0.25 sec.
Class IIIa - Medium powered lasers or systems that are normally not
hazardous if viewed for less than 0.25 sec without
magnifying optics.
Class IIIb - Medium powered lasers (0.5w max) that can be
hazardous if viewed directly.
Class IV - High powered lasers (>0.5W) that produce ocular, skin
and fire hazards.
39
The types of hazards can be grouped as follows:
1. Ocular injury
2. Tissue damage
3. Respiratory hazards
4. Fire and explosion
5. Electrical shock
1. Ocular Injury:
Potential injury to the eye can occur either by direct emission
from the laser or by reflection from a specular (mirror like) surface or
high polished, convex curvatured instruments. Damage can manifested
as injury to sclera, cornea, retina and aqueous humor and also as cataract
formation. The use of carbonized and non-reflective instruments has
been recommended.
2. Tissue Hazards:
Laser induced damage to skin and others non target tissues can
result from the thermal interaction of radiant energy with tissue proteins.
Temperature elevation of 21°C above normal body temp (37°C) can
produce cell destruction by denaturation of cellular enzymes and
structural proteins. Tissue damage can also occur due to cumulative
40
effects of radiant exposure. Although there have been no reports of laser
induced caroinogenesis to date, the potential for mutagenic changes,
possibly by the direct alteration of cellular DNA through breathing of
molecular bonds, has been questioned.
The terms photodisruption and photoplasmolysis have been
applied to describe these type of tissue damage.
3. Respiratory:
Another class of hazards involves the potential inhalation of
airborne biohazardous materials that may be released as a result of the
surgical application of lasers. Toxic gases and chemical used in lasers
are also responsible to some extent.
During ablation or incision of oral soft tissue, cellular products
are vaporized due to the rapid heating of the liquid component in the
tissue. In the process, extremely small fragments of carbonized, partially
carbonized, and relatively intact tissue elements are violently projected
into the area, creating airborne contaminants that are observed clinically
as smoke or what is commonly called the ‘laser plume’. Standard
surgical masks are able to filter out particles down to 5m in size.
41

Particle from laser plume however may be as small as 0.3m in
diameters. Therefore, evacuation of laser plume is always indicated.
4. Fire and Explosion
Flammable solids, liquids and gases used within the clinical
setting can be easily ignited if exposed to the laser beam. The use of
flame-resistant materials and other precautions therefore is
recommended.
Flammable materials found in dental treatment areas.
Solids Liquids Gases
Clothing
Paper products
Plastics
Waxes and resins
Ethanol
Acetone
Methylmethacrylate
Solvents
Oxygen
Nitrous oxide
General anesthetics
Aromatic vapors
5. Electrical Hazards:
These can be:
- Electrical shock hazards
- Electrical fire or explosion hazards
42
Summary of laser safely control measures recommended by
ANSI
Engineering controls:
- Protective housing
- Interlocks
- Beam enclosures
- Shutters
- Service panels
- Equipment tables
- Warning systems
- Key switch
Administrative controls:
- Laser safety officer
- Standard operating procedures
- Output limitations
- Training and education
- Medical surveillance
Personal protective equipment:
- Eye wear
- Clothing
- Screens and curtains
43
Special controls:
- Fire and explosion
- Repair and maintenance
Conclusion:
Laser has become a ray of hope in dentistry. When used
efficaciously and ethically, lasers are an exceptional modality of
treatment for many clinical conditions that dentists treat on daily basis.
But laser has never been the “magic wand” that many people have
hoped for. It has got its own limitations. However, the futures of dental
laser is bright with some of the newest ongoing researches.
44


















