INTRODUCTION TO PROSTHODONTICS INTRODUCTION TO PROSTHODONTICS.
Upload
ragi-al-emamCategory
view
382download
2
Laser in prosthodontics

Advances in technology are increasing and changing the ways that the patient experience dental treatment.
One of the milestones in technological advancements in dentistry is the use of lasers.
The term laser is the acronym for” Light Amplification by Stimulated Emission of Radiation”
They provide more efficient , more comfortable and more predictable outcomes of the patient.

Theory of stimulated emission1917-Einsteen
Laser principle1958-Townes&Schawlow
Ruby laser1960-Maiman
Neodymium ion doped yttrium aluminum garnet rod
1961-Johnson
Co2 laser1964-Patel
First documented case in OMFS using laser
1977-Shafir
First dental laser ND:YAG1989-Terr Myers
History

Fundmentals of laser

Components
1. Active component (lasing medium)
2. Pumping mechanism
3. Optical resonators

Basic laser components.


Classifications of laser

The main differentiating characterstics of laser is wavelength which depends on the laser medium and the excitation mode .

Classification based on light spectrum
Not used in dentistry 100 nm - 400 nm UV Light
Most commonly used in dentistry ( Argon & Diagnodent Lasers)
400 nm to 750 nm Visible light
Most dental lasers are in this spectrum
750 nm to 10000 nm Infrared light

The following four laser instruments emitt
visible light:. Aragon laser :blue wave length of 488nm..Aragon laser: blue-green wavelength of 514nm.frequency doubled laser ND:YAG also called potassium titanyl phosphate(KTP) : green wavelength of 530nm.low level lasers red non surgical wavelength of 600to 635 nm for photomodulation and 655nm for caries detection

These include photomodulation devices.Diode lasers various wavelengths between 800 and 1064nm.ND:YAG laser 1064nm.Erbium ,chromium doped ytrium scandium gallium garner (Er:Gr:Ysgg)2780nm.Co2 laser :9300nm and 10,600nm
Other dental lasers emitt invisible laser light

Classification according to the materials used
solidliquidgas
Diodes Nd:YAG, Er:YAG, Er:Cr:YSGG, Ho :YAG
Not so far in clinical use
Argon Carbon dioxide

Lasers are also classified as soft lasers and hard lasers.

Delivery systems

Shorter wavelength instruments, such as Ar, diode, and Nd:YAG lasers, have small, flexible fiber-opticsystems with bare glass fibers that deliver the laser energy to the target tissue.


Because the Erbium and Co2 are absorped by water which is a major component of coventional glass fibers, these wavelengths cannot pass through these fibers

Erbium and co2 laser devices are therefore constructed with special fibers capable of transmitting these wavelengths with semiflexible hollow waveguides or articulator arms.

The Er family of dental lasers provides a cooling water spray for hard tissue procedures that can be switched off for soft tissue surgeries.

In the noncontact use the beam is aimed at the target some distance away, with the loss of tactile sensation the surgeon must pay attention to the tissue interaction with the laser energy.

Emission mode

There are two basic modes of wavelength emission for dental lasers:
Continuous wave emission
• means that laser energy is emitted continuously produces constant tissue interaction.
• CO2, Ar, and diode lasers operate in this manner
Free-running pulse emission
• occurs with very short bursts of laser energy
• KTP, Nd:YAG, Er:YAG, and Er,Cr:YSGG devices operate as free-running pulsed lasers.

Continuous wave emission Free-running pulse emission
• provides target tissue withthermal relaxation time to cool
•They are equipped with a mechanical shutter with a time circuit to produce gated or super-pulsed energy.
•To minimize some of the undesirable residual thermal damage.

Regardless of the emission mode, all lasers produce a thermal effect on target tissues, and the operator must
pay strict attention to the temperature of the surgical site and ensure that the laser energy is correctly
controlled

Laser Effects on Tissue

Depending on the optical properties of the tissue, laser may have four different interactions with the target tissue.
1. Reflection2.Transmission3.Scattering4.Absorption

The primary and beneficial goal of laser energy is therefore
absorption of the laser light by the intended biological tissue.

The principal laser-tissue interaction is photothermal

Three primary photothermal laser-tissue interactions
Incision/excision
Ablation/vaporization
Hemostasis/coagulation
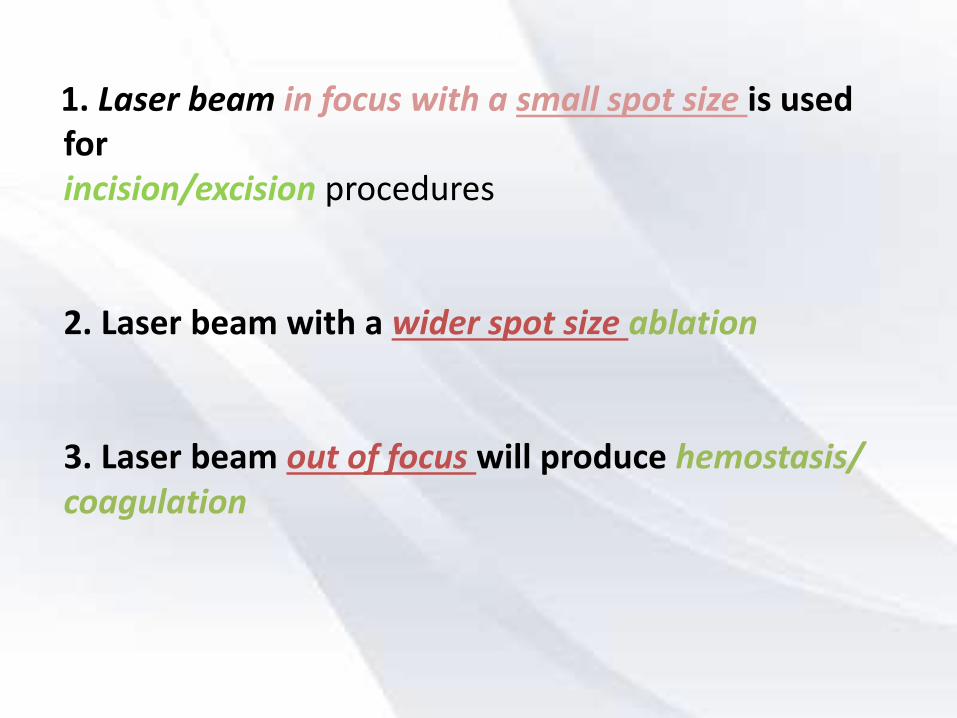
1. Laser beam in focus with a small spot size is used forincision/excision procedures
2. Laser beam with a wider spot size ablation
3. Laser beam out of focus will produce hemostasis/coagulation

Deep effect on tissue
Superficial effect on tissue
Small spot size Large spot size

Laser excisional biopsy.

Laser ablation of gingivalhyperplasia.

Laser coagulation of an aphthous ulcuer

Photochemical effects occur when the laser is used tostimulate chemical reactions, such as the curing ofcomposite resin.
A laser can be used in a nonsurgical mode forbiostimulation for more rapid wound healing, pain relief.
The pulse of laser energy on hard dentinal tissues canproduce a shock wave, which is an example of the photoacoustic effect of laser light. This process is often calledspallation.
Certain biologic pigments, when absorbing laser light of aspecific wavelength, can fluoresce, which can be used forcaries detection on occlusal surfaces of teeth.

Application of laser in prosthodontics

Removable prosethsis

The successful construction of removable full and partial dentures mainly depends on the preoperative evaluation of the supporting hard and soft tissue structures and their proper preparation.
A comprehensive prosthodontic treatment plan may need to incorporate surgery to maximize this support.

removal of a torus vestibuloplasty
contouring of irregular ridge
anatomy
removal of hyperplastic or redundant soft
tissue
reduction of a hard or soft tissue
tuberosity
Surgery of healthy tissues may include

Dental lasers can be successfully used for all of these procedures because laser energy :
1. reduces bacteria at the surgical site2. coagulates blood vessels.
3. minimizes scar formation.4. reduces swelling and postoperative pain.5. facilitates the overall treatment of prosthodontic patients.

All dental wavelengths can perform soft tissue surgeries, but the erbium (Er) family of lasers is the
only group of lasers indicated for treatment of osseous tissue.
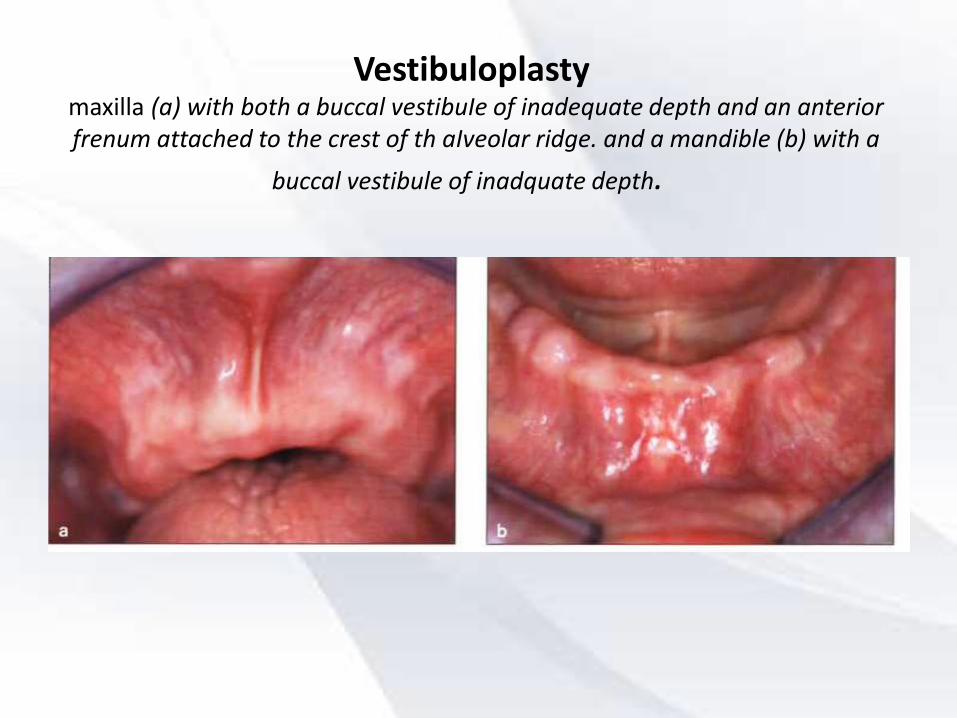
Vestibuloplastymaxilla (a) with both a buccal vestibuIe of inadequate depth and an anterior frenum attached to the crest of th aIveolar ridge. and a mandible (b) with a
buccal vestibule of inadquate depth.

Immediate postoperative views of the maxilla (c) following the frenectomy and vistibuloplasty and the mandible
(d) following vistibuloplasty.

Tuberosity reduction in the posterior maxilla

Any laser can be used to reduce soft tissue tuberosities. For hard tissue tuberosity reduction, the Er family of lasers is
necessary to ablate bone.

Removal of a mandibular torus
An Er laser cuts the osseous protuberance Large torus on the lingual aspect of the left mandible

Reflection of the soft tissue flap and hemostasis can be accomplished using any wavelength. However, the osseous
reduction can only be performed with Er family lasers.
Torus removal with a hemostat. Immediate postoperative view.

Contouring of the maxillary denture base
Preoperative view showing a partially edentulous maxilla immediately following extraction of the anterior dentition.
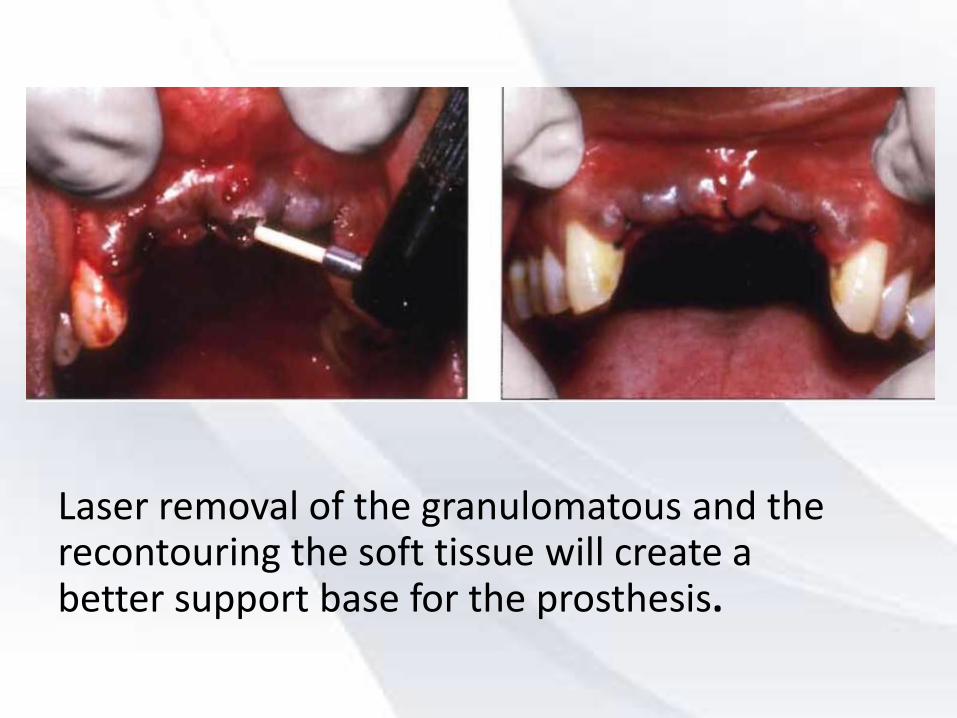
Laser removal of the granulomatous and the recontouring the soft tissue will create a better support base for the prosthesis.

Although any dental laser will work, a wavelength with superior hemostatic ability (ie, CO2, diode, or Nd:YAG) will ensure that blood clots formed in the coagulated
extraction sockets will not be displaced and cause new bleeding.

Chronically inflamed hyperplastic tissue on the mandibular ridge
Soft tissue laser ablation.

Immediate postoperative view of the soft tissue denture base.
The l month postoperative view shows complete healing.
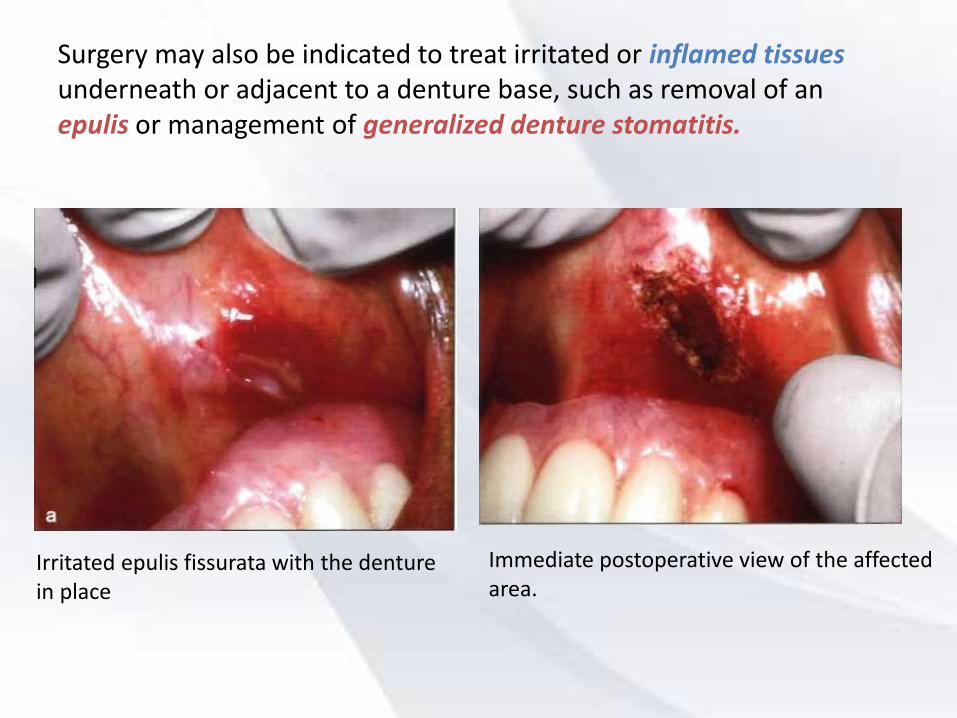
Surgery may also be indicated to treat irritated or inflamed tissues underneath or adjacent to a denture base, such as removal of an epulis or management of generalized denture stomatitis.
Irritated epulis fissurata with the denture in place
Immediate postoperative view of the affected area.

Denture sore on the right mandibular ridge

Treatment of undercut alveolar ridges
• Naturally occurring undercuts such those found in the lower anterior alveolus or where a prominent pre-maxilla is present.
• This causes soft tissue trauma, ulceration, and pain when prosthesis is placed on such a ridge.
• Soft tissue surgery may be performed with any of the soft tissue lasers. Osseous surgery may be performed with the erbium family of lasers

Application of laser in Implant dentistry

Why use laser technology in implant dentistry?
The advantages of using lasers in implant dentistry are the same as for any other soft tissue dental procedure.
Increased visibilty due
to hemostasis
Reduced swelling and
infection
Reduced pain
Minimal damage to
the surrounding
tissue

Impressions for restorative procedures can be taken immediately after second-stage surgery because the surgical field
will be clean and dry.

The erbium (Er) family of lasers, with its capacity for osseous ablation, can be used in osteotomy
preparation and for removal of diseased osseous tissue around areas of inflammation."

Although Nd:YAG has been a particularly popular wavelength to use for soft tissue second-stage surgery, several investigators contend that it is contraindicated to use with implants.
Due to1. the transmission of heat to the bone from the heated implant surface.2. the potential for pitting and melting, and the porosity of the implant surface.

whereas the diode, Er family, and carbon dioxide (C02) lasers can be used .
Because they are reflected away from metal surfaces, they interact only minimally with the implant.

Peri-implantitis case
Preoperative swelling around implants. Radiographic view showing radiolucency between
implants.
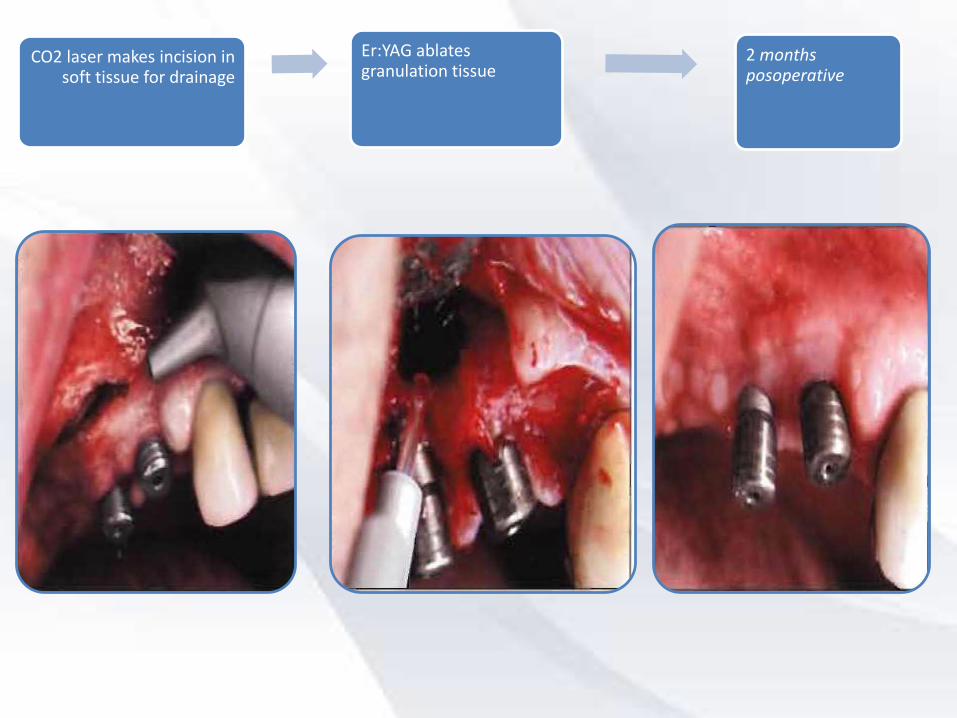
CO2 laser makes incision in soft tissue for drainage
Er:YAG ablates granulation tissue
2 months posoperative

Periimplantitis
Inflamed hyperplastic tissue surrounding implant abutments.
Immediate postoperative view following laser ablation.
Excellent soft tissue tone. contour, and health are restored 6 months after laser treatment.
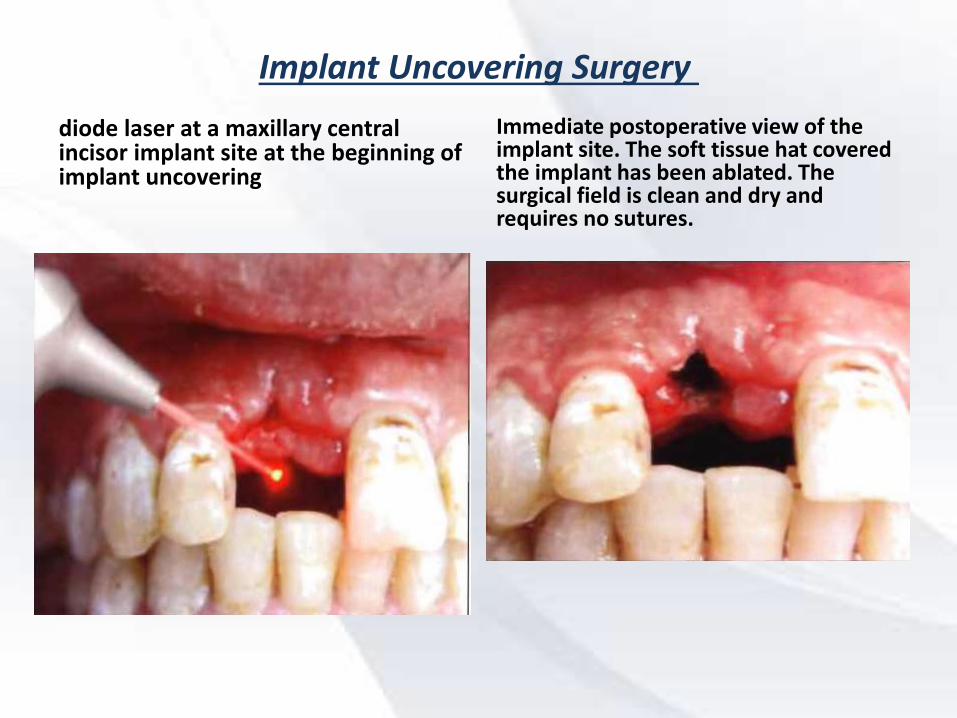
Implant Uncovering Surgery
diode laser at a maxillary central incisor implant site at the beginning of implant uncovering
Immediate postoperative view of the implant site. The soft tissue hat covered the implant has been ablated. The surgical field is clean and dry and requires no sutures.

CO2 laser removing soft tissue during second-stage implant surgery.
Immediate postoperative view showing three uncovered Implants

Implant Placement
Partially edentulous posterior maxilla.
The Er:YAG laser begins soft tissue preparation.
After soft tissue ablation is completed the surgical site is ready for pilot holes.

The Er:YAG laser begins osseous pr eparation.
Implant placement with supragingival healing caps.
Three months postoperative view of implants

Implant problem solvingSoft tissue growth over an implant

One of the most interesting uses of lasers in implant dentistry is the possibility of salvaging ailing implants by decontaminating their surfaces with laser energy.
Diode, ER:YAG, CO2 lasers can be used for this purpose
Nd:YAG wavelength did not sterilize dental implants. In addition,melting, loss of porosity, and other surface alterations.

In some clinical sitiuations using laser may be the best choice
A patient with potential bleeding problems could betreated with a laser to provide essentially bloodless surgery in the bone. This practice could be particularly
useful in the placement of mini-implants

Sinus lift procedure
• The procedure can be done by making the lateral osteotomy with a decreased incidence of sinus membrane perforation.
• The yttrium-scandium-gallium-garnet (YSGG) laser is the optimal choice for not cutting the sinus membrane

Bone grafts done with lasers have been demonstrated to decrease the amount of bone necrosis from the donor site and the osteotomy cuts are narrower, resulting in less postoperative pain and edema

The impact laser use have on the prostheses that are manufactured for
implant restoration
One of the hallmarks of the osseointegrationtechnique is a passive fit of the prosthesis on the implants.
one of the ways to obtain a true passive fit is by the elimination of the casting technique.
The expansion and contraction during casting can lead to a nonpassive fit of the implant prosthesis when placed onto multiple implants

To that end, the proposed
laser welding of titanium components has been advocated and used with some mixed success.

One of the issues was the learning curve for the technicians and that as familiarity with the procedure
increased, success rates improved

LASER APPLICATION IN DENTAL LABORATORY
• Laser holographic imaging is a well established method for storing topographic information, such as crown preparations, occlusal tables, and facial forms for maxillofacial prosethsis.
• Holography is the science of recording the reflected light waves from an object onto a hologram and subsequently reconstructing the stored image of the object in the space where the original object had been. The terms holo, meaning complete, and gram, meaning message, give rise to the hologram or complete message.
• The three-dimensional aspect of the hologram image is unique.

Ultraviolet (helium-cadmium) laser-initated polymerization of liquid resin in a chamber, to create surgical templates for
implant surgery and major reconstructive oral surgery

Laser scanning of casts can be linked to computerized milling equipment for fabrication of restorations from porcelain and
other materials


Safety regulations
•.Using high volume plum
evacuaton system
wearing wavelength-specific protective eyewear,
Restricting access to the laser surgery area, minimizing reflective surfaces and normal
protocol for infection control