
Larynx, Thyroid and Parathyroid Glands II. Parathyroid and Thyroid
14
PARATHYROID IMAGING Imaging ofthe parathyroid glands revolves around the detec- tionof parathyroid adenomas and hypelplastic parathyroid glands in the set- ting of primary hy- perparathyroidism. Arguments for and against imaging and aboutwhich imagingmodality to usehavebeen hotly debated in the radiologyand surgery literature. I Anatomy The lower par- athyroidglands are derived from the third pharyngeal pouchandthe up- per parathyroid glands from the fourth pharyngeal pouchof the bran- chial apparatus. Most people have four glands (a pair at the upper and lower polesof the thyroid gland), however 25Vo of individualshave more thanfour (1,2). Theparathy- roid glands may be aberrantly located anywhere from the carotidbifurcation to the anterior me- diastinum, with in- ferior migration occuring most fre- quently(3). The vascular supply to the parathyroid glands is usuallythroughthe superior and inferior thyroidal arteries, with drainage to thyroidal veins.The glandsare innervated throughthe cervical sympathetic plexus. I Hyperparathyroidism Hyperparathyroidism hasan incidence of 0.031Vo per year in the United States (4). Patients may present with the classic RSNA Special Course in Head and Neck Imaging 1996; pp 95-107 l From the Department of Radiology, llospital of the University of Pennsylvania, 3400 Spruce St, Philadelphia, PA lglM. Portions of this article and all figures were reprinted or adapted from Yousem DM, Scheff A. Thyroid and parathyroid gland pathology: role of im- aging. Otolaryngol Clin North Am 1995; 28621450 and Yousem DM. Thyroid and parathyroid glands. Neuroimaging Clin North Am 1996:6:68-112. findings of bones(demineralization or arthritis), stones (re- nal calculi), groans (abdominal pain), or moans(psychiatric disturbances). Primary hyperparathyroidism is caused by a solitary parathyroid adenoma in80Vo-85Vo ofcases (5-9). The remaining lSVo-ZAVo of pa- tients with hy- perparathyroid- ism haveeither hyperplastic par- athyroid glands (l2Vo-l5%o), multiple adeno- mas(2Vo-jvo), or parathyroid carcinoma (<2Vo) (5-9). Parathyroid ad- enomas areec- topic (not around the thy- roid bed) in l0%o-20Vo of cases (6-8,10). Optionsfor imaging the par- athyroid glands are many andin- clude ultrasound (US), computed tomography (CT), magnetic resonance (MR) imaging,an- giography, and nuclear medi- cine scintigra- phy. The advan- tages anddisad- vantages of the variouscross- sectional imag- ing techniques are summarized in Table 1 (3,11-14). The choices for scintigraphic localiza- tion of parathyroid adenomas includethallium-2O l-techne- tium-99m pertechnetate subtraction scanning, Tc-99m sestamibi (hexakis-2-methoxy-isobutyl-isonitrile) subtrac- tion imaging with iodine-123 or Tc-99m pertechnetate, and Tc-99m sestamibi imaging without subtraction. The subtrac- tion techniques allow tracers that areconcentrated in the thyroid gland (pertechnetate and iodine)to be subtracted from ones (thallium and sestamibi) that accumulate in both thyroid glandsand parathyroid adenomas. Thallium is a po- tassium analog that may concentrate in parathyroid adeno- masdue to changes in potassium turnoverin activecells. Thallium emits low-energy, low-penetrating, 80-keV pho- tons that makepenetration from the mediastinum variable. In addition,thallium washes out of adenomas relatively rap- idly. The mechanism for sestamibi uptake is not well under- stoodbut may relateto mitochondrial densityin oxyphil celts, blood flow within adenomas, or potassiumturnover 95
Transcript of Larynx, Thyroid and Parathyroid Glands II. Parathyroid and Thyroid

PARATHYROID IMAGINGImaging ofthe parathyroid glands revolves around the detec-tion of parathyroid adenomas and hypelplastic parathyroidglands in the set-ting of primary hy-perparathyroidism.Arguments for andagainst imagingand about whichimaging modalityto use have beenhotly debated inthe radiology andsurgery literature.
I AnatomyThe lower par-
athyroid glands arederived from thethird pharyngealpouch and the up-per parathyroidglands from thefourth pharyngealpouch of the bran-chial apparatus.Most people havefour glands (a pairat the upper andlower poles of thethyroid gland),however 25Vo ofindividuals havemore than four(1,2). The parathy-roid glands may beaberrantly locatedanywhere from thecarotid bifurcationto the anterior me-diastinum, with in-ferior migrationoccuring most fre-quently (3). The vascular supply to the parathyroid glands is
usually through the superior and inferior thyroidal arteries,with drainage to thyroidal veins. The glands are innervatedthrough the cervical sympathetic plexus.
I HyperparathyroidismHyperparathyroidism has an incidence of 0.031Vo per year
in the United States (4). Patients may present with the classic
RSNA Special Course in Head and Neck Imaging 1996; pp 95-107
l From the Department of Radiology, llospital of the University of
Pennsylvania, 3400 Spruce St, Philadelphia, PA lglM. Portions of
this article and all figures were reprinted or adapted from Yousem
DM, Scheff A. Thyroid and parathyroid gland pathology: role of im-
aging. Otolaryngol Clin North Am 1995; 28621450 and Yousem
DM. Thyroid and parathyroid glands. Neuroimaging Clin North Am
1996:6:68-112.
findings of bones (demineralization or arthritis), stones (re-
nal calculi), groans (abdominal pain), or moans (psychiatric
disturbances). Primary hyperparathyroidism is caused by asolitary parathyroid adenoma in80Vo-85Vo ofcases (5-9).
The remaininglSVo-ZAVo of pa-tients with hy-perparathyroid-ism have eitherhyperplastic par-athyroid glands(l2Vo-l5%o),multiple adeno-mas (2Vo-jvo),or parathyroidcarcinoma(<2Vo) (5-9).Parathyroid ad-enomas are ec-topic (notaround the thy-roid bed) inl0%o-20Vo ofcases (6-8,10).
Options forimaging the par-athyroid glandsare many and in-clude ultrasound(US), computedtomography(CT), magneticresonance (MR)imaging, an-giography, andnuclear medi-cine scintigra-phy. The advan-tages and disad-vantages of thevarious cross-sectional imag-ing techniquesare summarized
in Table 1 (3,11-14). The choices for scintigraphic localiza-tion of parathyroid adenomas include thallium-2O l-techne-
tium-99m pertechnetate subtraction scanning, Tc-99msestamibi (hexakis-2-methoxy-isobutyl-isonitrile) subtrac-
tion imaging with iodine-123 or Tc-99m pertechnetate, and
Tc-99m sestamibi imaging without subtraction. The subtrac-tion techniques allow tracers that are concentrated in thethyroid gland (pertechnetate and iodine) to be subtractedfrom ones (thallium and sestamibi) that accumulate in both
thyroid glands and parathyroid adenomas. Thallium is a po-
tassium analog that may concentrate in parathyroid adeno-mas due to changes in potassium turnover in active cells.Thallium emits low-energy, low-penetrating, 80-keV pho-
tons that make penetration from the mediastinum variable.
In addition, thallium washes out of adenomas relatively rap-
idly. The mechanism for sestamibi uptake is not well under-
stood but may relate to mitochondrial density in oxyphilcelts, blood flow within adenomas, or potassium turnover
95

(15,16). Tc-99m sestamibi has 140-keV photons that penetrate the anteriorneck and mediastinal soft tissues betterand is concentrated at a higher rate andfor a longer time within an adenomathan thallium. Because sestamibi up-take in parathyroid adenomas persistsafter thyroid gland wash-out, it can beused without subtraction techniques ifone performs delayed imaging. Thedifficult task of patient immobilizationand accurate superimposition of sub-tracted images, required with thallium-pertechnetate studies, is obviated withdelayed sestamibi imaging. Singlephoton-emission CT (SPECT) scan-ning can also be combined with high-dose Tc-99m sestamibi scintigraphyfor more accurate localization of par-athyroid adenomas (15).
In most institutions, preoperative lo-calization of the parathyroid glandswith imaging is not performed beforethe first surgery (for patients who havepreviously undergone surgery, see be-low). This stems from the early surgi-cal literature that suggests that surgicaltime, morbidity, and mortality are notsubstantially influenced by preopera-tive localization of parathyroid ad-enomas for hyperparathyroidism (17-l9). Surgical exploration entails bilat-eral dissection of the perithyroidal re-gion, emphasizing the inferior poleswhere most parathyroid adenomas oc-cur. In experienced hands, this surgicalprocedure can be performed quicklyand accurately with success rates ofmore than 904o (8,19-22).
Proponents of preoperative localiza-tion of parathyroid adenomas even inpreviously unoperated cases cite(a) the need for only unilateral dissec-tion when an adenoma is evident at im-aging: (b) the identification of ectopicadenomas preoperatively, allowingbetter planning and patient education;(c) detection of other head and neckmasses that may require treatment atthe same time (eg, thyroid masses);and (d) the reduction in operatingroom time, recurrent laryngeal nerveparalysis, and postoperative hypopar-athyroidism when preoperative imag-ing is performed (22-26).In studies byRussell et al (25) and Casas etal(27),the difference between mean operatingtimes with 0l and 135 minutes. re-spectively) and without (97 and 180minutes, respectively) preoperative im-aging justified the expense of thestudy. The operative success rate also
96 I Yousem
improved from9Uvo to lNTo with pre-operative imaging (27). Uden et al (28)also noted that the time for surgery andanesthesia decreased with preoperativeimaging; however, when a cost-benefitanalysis was performed, they foundthat the cost of the imaging procedureoutweighed its benefit. A reduction of28 minutes of operating room time inthe study by Roe et al (19) did notjus-tify the $901.00 mean cost of localiza-tion. Other surgeons take a centrist po-sition regarding bilateral or unilateralneck explorations. They will performunilateral neck dissection if imagingstudies are definitive, but convert tobilateral surgery if (a) imaging isequivocal or shows a multifocal abnor-mality, (b) more than one enlargedgland is identified at surgery, (c) thepatient has a multiple endocrine neo-plasia (MEN) syndrome (often associ-ated with parathyroid hyperplasia), or(d) a unilateral exploration isunrevealing (25).
When a parathyroid adenoma is notidentified in a stereotypical perithy-roidal location, the surgeon may em-pirically explore the anterior mediasti-num, deep cervical space, periesoph-ageal grooves, or carotid sheath re-gion. The yield of surgery in this sce-nario is much lower (less than 707osuccessful) than that expected for thoseadenomas in a perithyroidal location,and the surgical complication rate in-creases with such blind explorations(20). The intrathyroidal parathyroid
adenoma (which accounts for a smallpercentage ofcases) cannot be readilydistinguished from thyroid adenomasand poses a particularly difficult prob-lem (8,29). To make matters more con-fusing, thyroidal abnormalities occurin up to 40Vo48Vo of patients with hy-perparathyroidism (2 1,30). These fac-tors have led less experienced surgeonsand those who have had a less $uccess-ful track record to opt for preoperativelocalization of all parathyroid ad-enomas.
It is fairly well accepted that therisks associated with surgery in a pa-tient who has previously undergonesurgery outweigh the cost of preopera-tive imaging. In those patients who un-dergo repeat surgery, the risk of vocalcord injury due to damage to the recur-rent laryngeal nerve or vagus nerve isapproximately j%o, cofipared with theinitial operating room risk of 1.37o(18). When imaging is not performedbefore repeat surgery for hyperparathy-roidism, surgery is approximately 60Vosuccessful; when imaging is performedbefore repeat surgery, the success rateincreases to80%o-907o (7). At repeatsurgery of previously operated cases,30Vo-75Vo of abnormal parathyroidglands are found in a perithyroidal lo-cation, overlooked or missed at thetime of initial operation (18,20,29,31).In patients in whom the initial surgeryfails, parathyroid adenomas are locatedin the anterior mediastinum in20Vo-38%o,in a paraesophageal or deep cer-
Table 1Advantages and Disadvantages of Varlous lmaging Modalities for DetectlngParathyroid Adenomas
Modality Advantages Disadvanlages
CT Examines head, neck, andchest; easy deteclion ofcalcification; biopsy ca-pable
Examines head, neck, andchest; no iodinated con-trast material required;excellent soft tissue dis-crimination
Examines head and neckwell: functional, not ana-tomic, imaging; helps dis-tinguish nodes from ad-enomas; reasonable cost
Examines neck well: inex-pensive; noninvasive;real-time, biopsy capable
Requires iodinated contrast material;iodinated conlrast affects thyroidimaging with scintigraphy; shoulderartifacts; ditficult to differentiatenodes from adenomas; expensive
Dilficult to dillerentiate nodes fromadenomas; intravenous gadoliniumagent employed; requires Patientcooperation, no claustrophobia; ex-pensive
Lower yield for eclopic glands, espe-cially in the chest; intrathyroidmasses indistinguishable lrom ad-enomas; smaller lesions easilymissed
Examines head and chest poorly;cannot help difterentiate nodesfrom adenomas
MRimaging
Nuclearmedicine
US

{ Figure 1. Para-thyroid adenoma.Tl-weighted MRimage demon-strates a parathy-roid adenoma (ar-row) on the rightside of the tracheajust behind the ca-rotid artery. Thecontralateral "nod-ule" (*) is theesophagus.
Figure 2. Initial and delayed Tc-99m sestamibi scans ofparathyroid adenoma.(a) Initial lS-minute scan shows tracer accumulation both in the thyroid gland (T) and
a nodule (arrow) below the right lobe of the thyroid gland. (b) Two-hour delayed im-
age shows that the tracer accumulation in the thyroid gland has largely cleared; theparathyroid adenoma (arow) remains evident.
vical location in about 20Vo,in anintrathyroidal location in 87o, and in aparathymic location in 2Vo (18,29,31).Supernumerary adenomatous glandsare present in 157o of cases. Of thoselocated in the chest, posterior mediasti-nal ectopic adenomas are one-fifth ascommon as anterior ones (32).
I Parathyroid AdenomasAt US, parathyroid adenomas appear
as oval, oblong, or bulbous lesionswith an echogenicity less than that ofthe thyroid gland (21,33). With high-resolution US, sensitivities of 607o-70Vo and specificities of9OVo-96Vohave been achieved for adenomas(5,6,11,21,33). Of those glands greaterthan I g in size, US has a detectionmte of 95Vo (21), When Stark et al (33)compared the accuracies of high-reso-lution CT and US in the detection ofparathyroid adenomas, they found thesensitivitv of CT to be70Vo with a
specificity of 90Vo, an improvementfrom their experience with US. Som-mer et al (34) also found CT to bemore accurate than US by more thanl07o; combining the studies yields adetection rate of 89Vo in patients whohave not previously undergone sur-gery.
Spritzeret al (14) were one ofthefirst groups to report on the accuracyof MR imaging in the detection of par-athyroid adenomas. Seventeen patientshad adenomas; MR imaging correctlydepicted 14 of them (82.3Vo).Twofalse-positive and three false-negativestudies for adenomas were reported;given the possibility of72 glands, thisyields an accuracy of 92Vo for MR im-aging of adenomas (Fig l).
Currently, most centers have em-braced Tc-99m sestamibi imagingwithout subtraction as the technique ofchoice for nuclear scintigraphy of theparathyroid glands. Ten to 30 mCi of
Tc-99m sestamibi is injected, withscanning at l5-minute intervals up to2-4 hours after injection (35). Becausethe agent washes out of the thyroidgland rapidly but is retained by par-athyroid (and thyroid) adenomas, de-layed images are the most useful forlocalization (Fig 2). One need not sac-rifice accuracy with the simpler sesta-mibi study. The overall sensitivity ofTl-Tc-99m pertechnetate subtractionscintigraphy for parathyroid adenomadetection (757o-857o) (36,37) is sub-stantially less than that of Tc-99msestamibi, which is about 9OVo-ljUVo(16,3740). A recent article by Lee etal (41) has shown a specificity of 98Vofor double-phase sestamibi imaging.
When Price (7) reviewed the pre-sestamibi literature up to 1993, hefound that MR imaging had the highestsensitivity for the detection of ad-enoma (74Vo), followed by nuclearmedicine studies (727o), CT (65Vo),and US (63Vo). The false-positive rateof nuclear medicine (117o) was lowerthan that of MR imaging(l4%o),CT(167o), and US (187o). Sestamibi dataover the past 3 years suggest that itsurpasses all other techniques in sensi-tivity and accuracy. Unfortunately, thehigh rate of thyroid abnormalities(40Vo48Vo) that coexist with parathy-roid adenomas may lead to false-posi-tive scintigrams because some thyroidlesions may concentrate radiotracers tothe same degree as parathyroid ad-enomas (16,29,37). Reports of Tc-99msestamibi in thyroid cancers and theirnodal and distant metastases signal thepossibility for false-positive studies(42).
More invasive studies have a highyield, but are more demanding. Thestudy by Miller et al (43) found par-athyroid venous sampling (807o), intra-operative US (7870), and arteriography(49Vo40Vo) to have higher sensitivi-ties than the noninvasive imaging stud-ies. The expense and technical diffi-culty in performing these invasive ex-aminations preclude their routine utili-zation, but they may be held in abey-ance for cases with equivocal or non-revealing noninvasive studies.
In the patient in whom prior surgeryfor a parathyroid adenoma has failed,both imaging and surgery must con-tend with scar tissue in and around thethyroid glands, loss oftissue planes,postoperative inflammation, lymphad-enopathy simulating parathyroid
Parathyroid and Thyroid lmaglng I 97

Table 2MEN Syndromes
Feature MEN I (Werner Syndrome)MEN IIA
(Sipple Syndrome)MEN llB (Mucosal
Neuroma Syndrome)
Parathyroid abnormality
Thyroid lesion
Pituitary lesionsPheochromocytomaOther manifestations
Chromosomal linkage
Hyperparathyroidism (90%) due tohyperplasia more commonly thanadenoma
Goiter, adenomas, thyroiditis arerare
Adenomas (2Oe/"-30%)NoPancreatic islet cell adenomas (insulinoma
or gastrinoma) in 30%-35"/o; adrenal cor'tex adenomas or carcinomas; rarely glu-cagonomas, VlPomas, carcinoid; Zollin-ger-Ellison syndrome
A-D, chromosome 11
Parathyroid hyperplasiain 2Oo/"-3O7o
Medullary thyroidcarcinoma
NoYes
A-D, chromosome 10
Very rare
Medullary thyroidcarcinoma
NoYesMucocutaneous neuromas;
marfanoid facies; cafe aulait spots
A-D, unknown chromosome
adenomas, and distortion of land-marks. False-negative images (due toobscured anatomy) tend to occur in theperithymic or perithyroidal operativebeds. The frequency of false-positiveexaminations (usually due to lymphad-enopathy) is lowest with nuclear medi-cine studies, followed by MR imaging,US, and CT (29).In patients who haveundergone repeat surgery, the sensi-tivities of US (36Vo-76Vo) (7,29,33,44), scintigraphy (26Vo-9OVo) ('7,12,29,44), CT (46%o437o) (7 '29,33,44), andMR imaging (50Vo-9 lVo) (3,7,12,29,44) have ranged widely. Price (7) con-cluded in a review of the literature thatMR imaging was the best cross-sec-tional imaging study to perform in thisscenario and nuclear scintigraphy thebest functional examination. The latestfigures on sestamibi scintigraphy haveshown sensitivities and accuracies inthe 80Eo-90Eo range (45,46). Sestamibiscintigraphy is therefore probably themost accurate and affordable study; itsdisadvantage is that the surroundinganatomy is not visualized for surgicalorientation. When combined with US.the accuracy does not increase; how-ever, the accuracy of sestamibi andMR imaging combined rcaches92%o(47). Alternatively, one can performthe most accurate (although most ex-pensive) cross-sectional imaging tech-nique, MR imaging, which providesgood anatomic detail, while runningthe small risk of mistaking a lymphnode for an adenoma. Because a thirdsurgery is an anathema to the surgeon,multiple studies are not uncommonlyperformed if one is not definitive. Theidea of using a morphologic test (CT,US, or MR imaging) as well as a func-
98 I Yousem
tional test (Tc-99m sestamibi) is ap-pealing. Use of this algorithm will in-crease the success rate of repeat sur-gery by more than 30Vo (18).
I Parathyroid HyperplasiaAbout 307o of patients with parathy-
roid hyperplasia have familial hyper-parathyroidism, including variants ofthe MEN syndrome (Table 2). Asnoted earlier, L2Vo-l5Vo of patientswith hyperparathyroidism have hyper-plasia. CT is reported to have a sensi-uvity of 45Vo-88Vo (7 ,33), US 307o-69Vo (5-1,33,47), and MR imaging409o439o (7,14) for detecting hyper-plastic glands. Parathyroid hyperplasiais detected in 43Vo45Vo of cases withthallium subtraction and in 55Vo-:7 5Voof cases with technetium sestamibi (5-7,37,48). The added accuracy in identi-fying hyperplastic glands has led agrowing consensus in support of theuse of Tc-99m sestamibi as the optimalagent for parathyroid adenoma and hy-perplasia localization (16,37,4O).
I Parathyroid GarcinomaIn all patients with hyperparathy-
roidism, the frequency of parathyroidcarcinoma is only l%o-2vo; however,parathyroid carcinoma causes hyper-parathyroidism in 85Vo-90Vo of cases(1,2). Metastases to lymph nodes occurin one-third of cases, and distant me-tastases occur in 2lVo-287o ofpatients.Men and women are affected equally.Edmonson et ̂ l (49) noted that a par-athyroid carcinoma may have the samesonographic appearance as a benignlarge adenoma (hypoechoic with orwithout heterogeneity); only the pres-ence of local invasion into the thyroid
gland, muscles, or vessels or nodal me-tastases would suggest this diagnosis.Parathyroid carcinomas have been re-ported to accumulate Tc-99m sesta-mibi (45,50).
I Secondary and TertlaryHyperparathyroidism
The evaluation of patients with sec-ondary or tertiary hyperparathyroidismis rarely centered around the parathy-roid glands because the kidneys are thesource of the abnormality in these dis-eases. Parathyroid glandular hyperpla-sia usually occurs in association withchronic renal failure and renal osteo-dystrophy. Tc-99m sestamibi has beenable to help identify bilateral uptake inhyperplastic glands and residual par-athyroid tissue in those individualstreated surgically in the neck for sec-ondary hyperparathyroidism (48).
THYROID IMAGINGI Anatomy
The thyroid gland sits anterolateraland superficial to the larynx and tra-chea and is fixed to the airway by fi-brous septa. Although no true lobes ofthe gland exist, it is enveloped by por-tions of the deep cervical fascia. Thethyroid isthmus is the midline portionof the gland, and from it may arise apyramidal "lobe" (in 50Vo-80Vo ofpa-tients) lying superficial to the thyroidcartilage (51). The vascular supply tothe thyroid gland is derived frompaired superior thyroidal arteries(branches of the external carotid arter-ies) and inferior thyroidal arteries(branches of the thyrocervical trunksof the subclavian arteries). The incon-

Figure 3. US scan shows a calcifiedthyroid mass. Note the acoustic shadow-ing (r<) behind the echogenic focus (ar-row), signifying calcification within thisthyroid gland. Unfortunately, the pres-ence or absence ofcalcification is not veryuseful for distinguishing benign frommalignant thyroid lesions.
stant arteria thyroidea ima arises di-rectly from the aortic arch and suppliesa small inferior portion of the gland.The thyroid gland drains into superior,middle, and inferior thyroidal veins,which pass to internal jugular and bra-chiocephalic veins. Vagal and sympa-thetic plexus branches provide inner-vation.
I lmaging of Masse$US.-The main role of cross-sec-
tional thyroid imaging (US, CT, MRimaging) is to evaluate thyroid massesfor potential malignancy. US, becauseof its simplicity, low cost, and abilityto help distinguish cystic from solid le-sions is often the first modality em-ployed to evaluate a thyroid mass inthe euthyroid patient. When a solid le-sion is hyperechoic, the frequency ofmalignancy is only 4Vo (52). If a solidlesion is isoechoic, the frequency ofmalignancy increases to 26Vo and, ifhypoechoic, malignancy occurs in
63Vo (52). Papillary carcinoma mostcommonly is seen as a solid hypo-echoic (77Vo) or isoechoic (147o) masswith or without calcification (calcifica-tions are hyperechoic but cause acous-tic shadowing that is hypoechoic [Fig3l) (52). If a cancer is hyperechoic atUS, it is usually due to the sclerosingform of papillary carcinoma (10).
If one looks at the margins of tumorsat US, one finds that 167o of malignantlesions have sharply marginated, well-defined borders whereas irregular orill-defined borders occur in approxi-mately 60Vo of cancers (52). Unfonu-nately, irregular or ill-defined bordersalso occur in approximately 457o ofbenign lesions (52). When a mass hasa complete halo of echopenia aroundit, the lesion is 12 times more likely tobe benign than malignant. If the halo isincomplete, a benign origin is still ap-proximately four times more likelythan a malignant one (52). Lesionsmeeting the absolute criteria for cysts(well-demarcated, smooth-walled,anechoic, and demonstrating enhancedthrough-transmission) are usually be-nign (10). A cystic lesion with punc-tate, calcified mural nodules is worri-some for papillary carcinoma.
Nucle ar m e di c ine.- T}:,e commonagents used for thyroid imaging in-clude I-123, I-131, and Tc-99m per-technetate. Because the radiation en-ergy ofI-131 is so high (364 keV), it isthe preferred agent for imaging sub-stemal thyroid glands or for perform-ing whole-body imaging after thyroidablation in order to detect metastaticfoci ofthyroid cancer. The otheragents have energies of 140 keV (Tc-99m) and 159 keV (I-123) (53). Themajor role of scintigraphy in the evalu-ation of a thyroid mass is the determi-nation of whether the lesion is hot(more uptake than the normal thyroidgland), warm (some activity but not asmuch as the normal gland), or cold(little to no uptake). The risk of canceris l%o4Vo for a hot nodule, 9%o-l0%ofor a warm nodule, and 15Vo-25Vo fora cold nodule (7 ,54,55).In a patientwith a prior history of head and neckirradiation, the risk of malignancy in acold nodule doubles to 30Eo-50Eo (7).Cold nodules in men have a higher rateof malignancy because women have agreater frequency of benign cold nod-ules from degenerated adenomas. Ifone performs dynamic injection Tc-99m pertechnetate scintigraphy, one
may find that hypoperfused lesions(less vascularity than that of the nativethyroid gland) are virtually never can-cers whereas most malignancies are"euperfused" or hyperperfused (55).Rarely, a lesion is cold at I-123 scin-tigraphy but hot or warm at Tc-99mpertechnetate scanning (a "discordantnodule"). It is believed that this phe-nomenon is caused by a lesion thattraps iodine (assessed with pertechne-tate) but does not organify it. The dif-ferential diagnosis includes malig-nancy, goiter, or follicular adenoma.Often a biopsy is required in this situa-tion.
C7.- Enhanced CT has a majordrawback in the evaluation of thyroidlesions. Because of the iodine uptakefrom the contrast agent, thyroid local-ization with nuclear scintigraphy andradioactive iodine treatment must bedelayed 4-8 weeks after administrationofiodinated contrast agents. The pres-ence of calcification, cysts, hemor-rhage, hypo- or hyperattenuation, orwell-defined borders in a solitary massat CT does not exclude a carcinoma.Peripheral eggshell-like calcifi cationand large multiple chunks of calciumare suggestive of benignity, whereasfine punctate calcifications are moreworrisome for malignancy (Fig a) (56).Calcification occurs in 137o of all thy-roid lesions, including lTVo of allma-lignancies and ll4o ofall benign pro-cesses (52). In a similar fashion, cysticareas occur in many thyroid masses:38Vo of malignancies have cystic com-ponents md62vo of benign massesmay be wholly or partly cystic (52).Hemorrhage may be found in papillarycarcinomas or goiters. Multiplicity ofnodules in an enlarged thyroid glandusually is suggestive of a benign pro-cess (or metastases).
The presence of lymphadenopathyor infiltration of adjacent tissues sug-gests malignancy. More than 507o ofpatients with papillary carcinoma havenodal spread at presentation , and 227ohave occult thyroid tumors (57). Curi-ously, the lymph nodes of thyroid pap-illary carcinoma may themselves showcalcification, cyst formation, colloidaccumulation, hemorrhage, or necrosis(Fig 5) (58,59). Sometimes the wall ofa cystic node may be unidentifiable,thereby simulating a branchial cleftcyst. Papillary carcinoma of the thy-roid may metastasize to posterior tri-angle, submandibular, retropharyngeal,
Parathyroid and Thyroid lmaging I 99
orjugular chain lymph nodes (58,59).The nodes may enhance uniformly anddramatically or, as in the case of cysticor calcified nodes, not at all (58,59).Any lymph node seen in a patient withpapillary carcinoma is suspected of be-ing malignant, no matter the size, be-cause of the relatively high rate oflymphatic spread.
MR imaging.-Histologic specific-ity of thyroid lesions is not improvedwith MR imaging. The key to the diag-nosis of thyroid cancer at MR imagingis the presence of malignant lymphad-enopathy. Irregular margination andclustered nodularity is characteristic,but not specific, for carcinoma (60).Lesions that have an intact and sym-metric pseudocapsule are usually be-nign, whereas those with pseudocap-sules that are penetrated or destroyedare usually cancers (Fig 6) (60,61). Le-sions that have capsules with irregularthicknesses may be malignant or be-nign. At MR imaging, the nodes ofpapillary carcinoma may have high orlow signal intensity on T1- and T2-weighted images, possibly related tothe presence of intranodal hemorrhageor colloid accumulation (Fig 7).
Postoperatively, thyroid carcinomarecurences usually have medium tohigh signal intensity on T2-weightedimages, whereas scars in the operativebed usually have low signal intensity(62). Postoperative edema, infection,or hemorrhage may simulate recurrenttumor. I- 13 I scintigraphy is the bestmodality to evaluate the operative bedand to screen for distant metastases af-ter thyroidectomy. MR imaging, inconjunction with I-131 radioisotopescanning, has been recommended forconfusing postoperative cases (63).
F ine -ne edle aspiration (FNA).-In-timately associated with any imagingtechnique is FNA cytology. Many pal-pable lesions of the thyroid gland maybe aspirated without imaging guid-ance, but US is the most common mo-dality used to guide aspirations be-cause it images in real time. Aspirationcytology in good hands shows out-standing results. In a series of I 1,000guided and unguided samples obtainedat the Mayo Clinic, Rochester, Minne-sota, the sensitivity of the techniquewas found to be 98Vo with a 997o posi-tive predictive value for cancer (64).Nondiagnostic specimens were presentin 2lVo of cases, however. With US-guided FNA, sensitivity approaches
IOO I Yousem
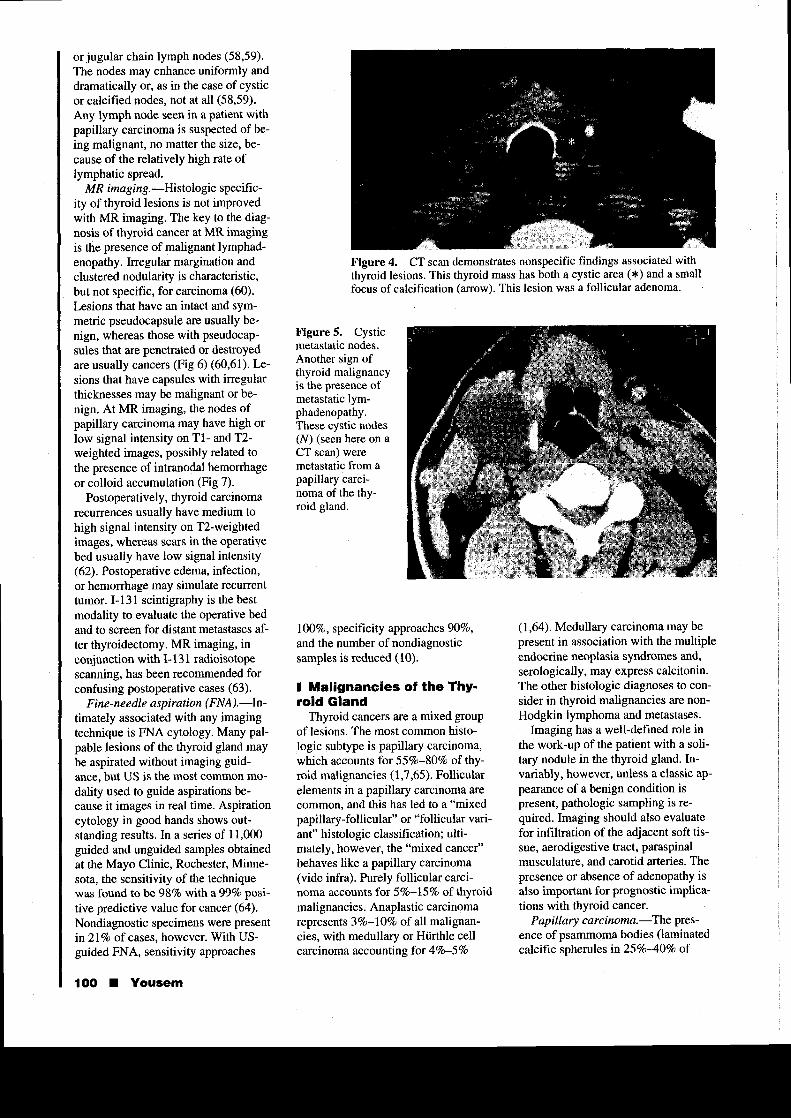
Figure 4. CT scan demonstrates nonspecific findings associated withthyroid lesions. This thyroid mass has both a cystic area (*) and a smallfocus of calcification (arrow). This lesion was a follicular adenoma.
Figure 5. Cysticmetastatic nodes.Another sign ofthyroid malignancyis the presence ofmetastatic lym-phadenopathy.These cystic nodes(N) (seen here on aCT scan) weremetastatic from apapillary carcinoma of the thy-roid gland.
1007o, specificity approaches 90Vo,and the number of nondiagnosticsamples is reduced (10).
I Malignancies of the Thy-roid Gland
Thyroid cancers are a mixed groupof lesions. The most common histo-logic subtype is papillary carcinoma,which accounts for 557o-80Vo of thy-roid malignancies (1,7,65). Follicularelements in a papillary carcinoma arecommon, and this has led to a "mixedpapillary-follicular" or "follicular vari-ant" histologic classification; ulti-mately, however, the "mixed cancer"behaves like a papillary carcinoma(vide infra). Purely follicular carci-noma accounts for S%o-l5%o of thyroidmalignancies. Anaplastic carci nomarepresents 3%o-l0Vo of all malignan-cies, with medullary or Hiirthle cellcarcinoma accounting for 4Vo-5Vo
(1,64). Medullary carcinoma may bepresent in association with the multipleendocrine neoplasia syndromes and,serologically, may express calcitonin.The other histologic diagnoses to con-sider in thyroid malignancies tue non-Hodgkin lymphoma and metastases.
Imaging has a well-defined role inthe work-up of the patient with a soli-tary nodule in the thyroid gland. In-variably, however, unless a classic ap-pearance of a benign condition ispresent, pathologic sampling is re-quired. Imaging should also evaluatefor infiltration of the adjacent soft tis-sue, aerodigestive tract, paraspinalmusculature, and carotid arteries. Thepresence or absence of adenopathy isalso important for prognostic implica-tions with thyroid cancer.
P ap illary c arc inoma. -The pres-ence of psammoma bodies (laminatedcalcific spherules in25%o40Vo of
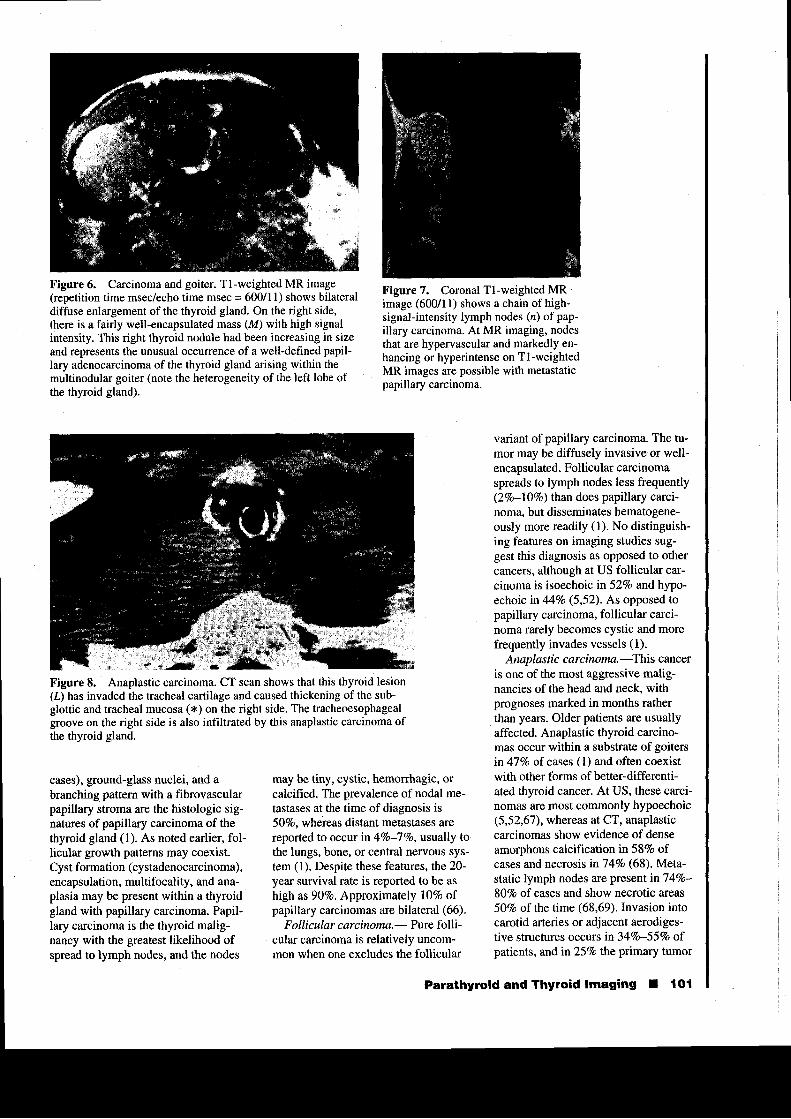
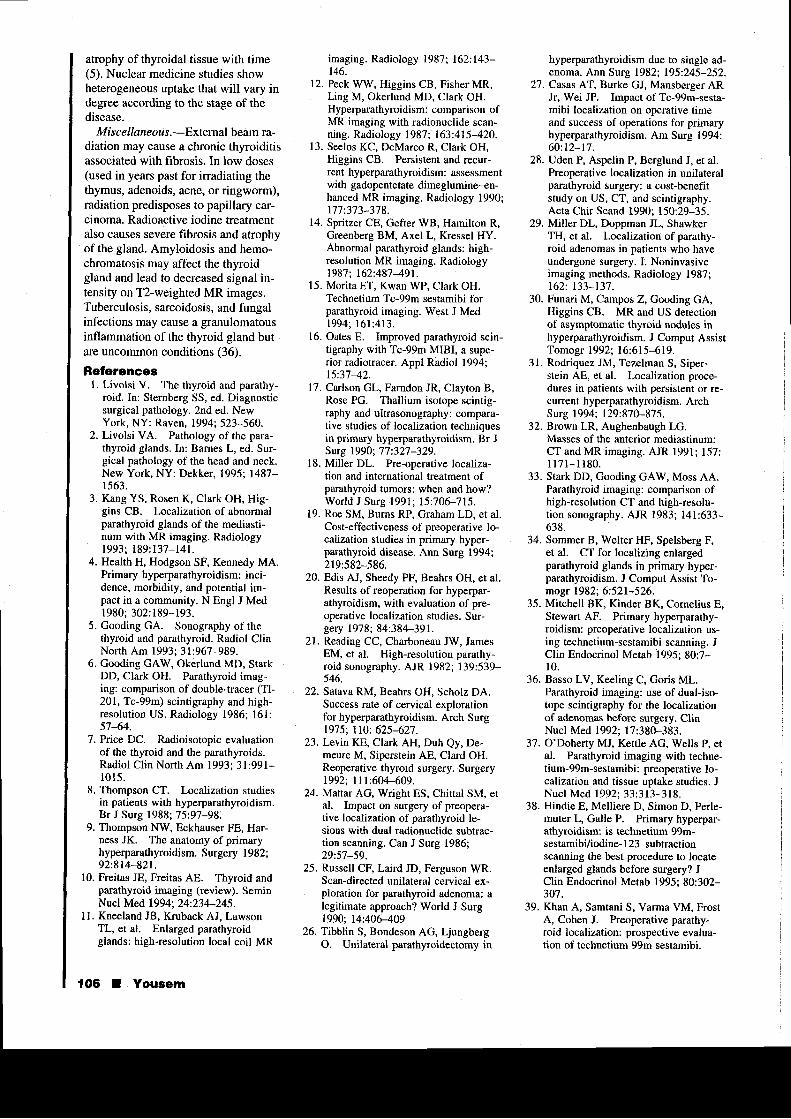
Figure 6. Carcinoma and goiter. Tl-weighted MR image(repetition time msec/echo time msec = 600/11) shows bilateraldiffuse enlargement ofthe thyroid gland. On the right side,there is a fairly w€ll-encapsulated mass (M) with high signalintensity. This right thyroid nodule had been increasing in sizeand represents the unusual occurence of a well-defined papil-Iary adenocarcinoma of the thyroid gland arising within themultinodular goiter (note the heterogeneity of the left lobe ofthe thyroid gland).
Figure 8. Anaplastic carcinoma. CT scan shows that this thyroid lesion(t) has invaded the tracheal cartilage and caused thickening of the sub-glottic and tracheal mucosa (*) on the right side. The tracheoesophagealgroove on the right side is also infiltrated by this anaplastic carcinoma ofthe thyroid gland.
Figure 7. Coronal Tl-weighted MRimage (600/11) shows a chain of high-signal-intensity lymph nodes (n) of pap-illary carcinoma. At MR imaging, nodesthat are hypervascular and markedly en-hancing or hyperintense on Tl-weightedMR images are possible with metastaticpapillary carcinoma.
cases), ground-glass nuclei, and abranching pattern with a fibrovascularpapillary sffoma are the histologic sig-natures of papillary carcinoma of thethyroid gland (1). As noted earlier, fol-licular growth patterns may coexist.Cyst formation (cystadenocarcinoma),encapsulation, multifocality, and ana-plasia may be present within a thyroidgland with papillary carcinoma. Papil-lary carcinoma is the thyroid malig-nancy with the greatest likelihood ofspread to lymph nodes, and the nodes
may be tiny, cystic, hemorrhagic, orcalcified. The prevalence ofnodal me-tastases at the time of diagnosis is507o, whereas distant metastases arereported to occur in %o-:l Vo, usually tothe lungs, bone, or central nervous sys-tem (l). Despite these features,the20-year survival rate is reported to be ashigh as 907o, Approximately llVo ofpapillary carcinomas are bilateral (66).
Follicular carcinoma.- Pure folli-cular carcinoma is relatively uncom-mon when one excludes the follicular
variant of papillary carcinoma. The tu-mor may be diffusely invasive or well-encapsulated. Follicular carcinomaspreads to lymph nodes less frequently(2Vo-l0Vo) than does papillary carci-noma, but disseminates hematogene-ously more readily (1). No distinguish-ing features on imaging studies sug-gest this diagnosis as opposed to othercancers, although at US follicular car-cinoma is isoechoic in 52Vo and hypo-echoic in 44Vo (5,52). As opposed topapillary carcinoma, follicular carci-noma rarely becomes cystic and morefrequent\ invades vessels (1).
Anaplastic carcinoma.:fhis canceris one of the most aggressive malig-nancies of the head and neck, withprognoses marked in months ratherthan years. Older patients are usuallyaffected. Anaplastic thyroid carcino-mas occur within a substrate of goitersin47Vo ofcases (l) and often coexistwith other forms of better-differenti-ated thyroid cancer. At US, these carci-nomas are most commonly hypoechoic(5,52,67), whereas at CT, anaplasticcarcinomas show evidence of denseamorphous calcification in58Vo ofcases and necrosis in74/o (68). Meta-static lymph nodes are present inl4Vo-807o of cases and show necrotic areas50Vo of the time (68,69). Invasion intocarotid arteries or adjacent aerodiges-tive structures occurs in 34Vo-55Vo ofpatients, andin25%o the primary tumor
Parathyroid and Thyroid lmaging I tOl

extends into the mediastinum (Fig 8)(68,69). Rapid growth and obliterationof adjacent tissue planes are hallmarksof this deadly tumor, with a mediansurvival of about 7 months.
Me dullary c arc inoma.-Medullarycarcinoma originates in the parafollicu-lar or C cells of the thyroid gland, cellsderived from neural crest tissue in theultimobranchial bodies of the branchialpouch system. These cells normally se-crete thyrocalcitonin, which decreasesserum calcium. Eighty to 90Vo of med-ullary carcinomas express calcitonin.Medullary carcinomas are usuallyhypoechoic at US (5,52,67). However,echogenic foci due to deposits ofcal-cium may be seen within these tumorsand metastatic lymph nodes whenpresent (67). These tumors do not usu-ally take up iodine, but may be thal-lium or gallium avid. Somatostatin re-ceptor scintigraphy may also depictmedullary carcinoma (67). The tumoris solid at CT and MR imaging andspreads to lymph nodes in more than507o of cases. Medullary carcinoma isa familial in l0vo-20Vo. Sipple syn-drome (MEN IIa) is the association ofmedullary carcinoma with pheochro-mocytoma and parathyroid adenomaand/or hyperplasia. When mucosalneuromas and marfanoid facies coex-ist, MEN IIb is said to be present. Bothsyndromes have been localized to anabnormal gene on the l0th chromo-some.
Lymphoma. -lhyroid lymphomamay be seen as a solitary mass (807o)or as multiple nodules (20Vo) (70). Anantecedent history of Hashimoto thy-roiditis in an elderly woman with arapidly enlarging, compressive, and in-filtrative mass is suggestive of lym-phoma. Most are B-cell neoplasms (1).The response to chemotherapy and ra-diation therapy is variable; some pa-tients do very well. Lymphomas areusually hypoechoic at sonography(5,52,67). Lymphoma is cold on tech-netium or iodine nuclear medicinestudies; however, gallium scans mayshow increased activity. Other lym-phoproliferative (leukemia) and granu-lomatous (eg, sarcoidosis) diseasesmay also be gallium avid and are in thedifferential diagnosis. The tumor ishypoattenuating on unenhanced andenhanced CT scans and shows necrosisor calcification in only 1Vo of cases(70). Invasion ofthe carotid sheath(l9%o-5l%o) or metastases to lymph
1O2 I Yousem
nodes (l4%o44%o) are not uncommon(70), The absence ofcalcification andnecrosis, the rarity ofinvasion into sur-rounding soft tissues, and the lowerfrequency of nodal dissemination helpdistinguish lymphoma from anaplasticcarcinoma. Lymphoma is usually ho-mogeneously hyperintense on T2-weighted MR images. Although somehave found Hashimoto thyroiditis tohave low signal intensity on T2-weighted images and, therefore, distin-guishable from lymphoma (which hashigh signal intensity) (71), most inves-tigators have found their signal intensi-ties to overlap (60,72,73).
Metastas e s.-Metastases to the thy-roid gland are often clinically occult.Pathologically, metastases to the glandmay be present in 2Vo4Vo of patientsdying from malignant disease (51).The two most common primary tumorsto metastasize to the thyroid gland arebronchogenic carcinoma and renal cellcarcinoma. Multifocality is the norm.Hemonhage is not uncommon with re-nal metastases.
Hiirthle cell tumors.-lnitially con-sidered a benign entity, this tumorbridges the gap between benign andmalignant thyroid masses. They maybehave aggressively and spread to theIymph nodes or to the lungs or theymay remain well encapsulated withoutwall or vascular invasion. Hiirthle celladenomas are variable in size andshape and have less well-defined bor-ders. These neoplasms tend to concen-trate sestamibi and are a source offalse-positive parathyroid adenomascans. They are not avid for radioio-dine.
I Benign MassesFunctioning thyroid adenomas.-
Ninety percent of solitary hot nodulesseen at scintigraphy are benign, usu-ally adenomashyperplasias that areexpressing thyroid hormone. Plummerdisease is hyperthyroidism due to asolitary, autonomous hot nodule (7).The difference between an autono-mous versus a hypertrophic function-ing hot nodule depends on the re-sponse to a thyroid suppression test.After a diagnostic course of thyroidhormone administration (with confir-mation of depressed thyroid stimulat-ing hormone ITSHI), a lesion that ispersistently hot at Tc-99m pertechne-tate scanning is considered an autono-mous lesion. whereas one that be-
Figure 9. Goiter. Nuclear medicineTc-99m pertechnetate thyroid scanshows multiple areas of decreased traceruptake with some areas of avid traceractivity. The gland appears enlarged.This is the characteristic appearance of amultinodular goiter. The differential di-agnosis could be an active phase of thy-roiditis.
Figure 10. Multinodular goiter. USscan shows multiple echopenic masses(x) in the left and right lobes of an en-larged thyroid gland.
comes cold is considered hypertrophic(54). Other sources ofhot nodules in-clude thyroiditis, normal variation inthyroid function, and ectopic tissue(7). "Toxic" adenomas rarely causeclinically apparent hyperthyroidismuntil they exceed 2.5 cm in size (10).The patient usually presents with aslowly growing neck mass. The imag-ing features of toxic adenomas arenonspecific at nonscintigraphic mo-dalities. The lesions are usually solidand enhancing.
Nonfunctionin g thyroid adeno -
mas.-A cold (nonfunctioning) noduleis approached more aggressively than ahot nodule because of the higher rateof malignancy, especially in young

Figure 11. Graves disease. Nuclearmedicine scan shows the uptake of thisthyroid gland was markedly elevated.The gland is enlarged with homoge-neous tracer uptake. Note also the en-larged pyramidal lobe (arrow).
women and men of all ages. Biopsy oraspiration is often required early in thediagnostic algorithm. Most cold nod-ules are due to degenerated (follicular)adenomas, nodular hemorrhage, cysts,goiters, inflammatory conditions (seebelow), or amyloid deposition (54).Follicular adenomas occur in all agegroups, in women more than men, andare usually smaller than 3 cm in diam-eter. As adenomas outgrow their bloodsupply, they may involute or encyst.Altematively, they may develop intra-lesional hemorrhage (and acutely ex-pand), necrosis, calcification, and/orscarring. Malignant degeneration is notthought to occur in adenomas.
Occasionally, one will find a hyper-plastic adenoma that is responsive toTSH in a patient with Graves disease.This will appear as a cold nodule be-cause the hyperthyroidism of Gravesdisease will suppress TSH, which inturn suppresses the adenoma on anuclear medicine study. This entity iscalled Marine-Lenhart syndrome (54).
Cysrs.*Most thyroid cysts actuallyrepresent degeneration of adenomas.Cysts of any kind are anechoic orechopenic at US, show a distinct backwall, and demonstrate enhancedthrough-transmission. They have lowattenuation at CT unless hemorrhagicor infected. The attenuation and signalintensity of the cyst will often not ex-actly simulate that of cerebrospinalfluid at CT and MR imaging due to thepresence of hyperproteinaceous colloid
within the cyst. Colloid cysts are char-acteized by homogeneous high signalintensity at Tl-weighted examinations(54). However, this finding is not spe-cific to colloid cysts because areas ofhemorrhage, which also have high sig-nal intensity on Tl-weighted images,can be seen in goiters, adenomas, andtraumatized cysts. Even thyroglossalduct cysts (vide infra) may be hyper-intense due to high protein content.
T eratomas.--:leratomas are rareneoplasms of the thyroid gland. As inother locations in the body, thyroid ter-atomas may demonstrate fluid, fat, cal-cification. and osseo-dental densitiesin various combinations. They usuallyoccur in the midline.
M ul t in o dul ar g o i t e r. - Anothercommon palpable thyroid abnormalityis the multinodular goiter. A goiter issimply an enlarged thyroid gland thatmay be seen with hyper- or hypothy-roidism. In the United States, the com-mon vernacular is to imply a nontoxicgoiter when the term is used. A euthy-roid or hypothyroid goiter is the mostcommon thyroid lesion in this country.In rare instances, a previously non-functioning multinodular goiter mayevolve into one with hyperfunctioningnodules and cause hyperthyroidism.Patients, usually older women, presentbecause of hypothyroidism, neckmasses, or tracheal-esophageal com-pression. The frequency of carcinomain a multinodular goiter is very low(less than 3Vo\, and the characteristicappearance of multiple cold areas in-terspersed with hot areas in a largegland will usually obviate the need foraggressive biopsy of a palpable nodule(Fig 9) (54). A large, dominant, hard,or growing mass amidst a goitershould probably still be sampled forbiopsy (74).
Nontoxic multinodular thyroidglands show minimal to moderate het-erogeneity with nodularity and mildlyincreased signal intensity at Tl-weighted MR examinations (60,61).Hemorrhagic foci are noted in 60Vo ofcases, and the lesions are often hetero-geneous at T2-weighted examination(61). Goiters usually do not havepseudocapsules (61). At CT and US,mixed solid and cystic zones within anenlarged, nodular thyroid gland with orwithout calcification is the characteris-tic appearance of a multinodular goiter(Fie 10).
Hyp e rthy roi dlsn.-The three most
common causes of hyperthyroidism areGraves disease (diffuse toxic goiter),toxic multinodular goiter, and toxic ad-enomas. The toxic adenomas (seeabove) are separated into those that areTSH responsive or TSH independent(autonomous). Occasionally, inflam-mation of the thyroid gland (thyroidi-tis) may produce a transient state ofhyperthyroidism. On rare occasions,ectopic thyroid tissue (lingual or ova-rian) may cause hyperthyroidism,
Intenzo et al (75) have proposed aunique algorithm for evaluating a hy-perthyroid patient. If thyroid functiontest (TFT) results are elevated alongwith the 24-hour radioactive iodine up-rake (RAIU) level (normal, <35Vo),thedifferential diagnosis is Graves diseaseor Marine-Lenhardt disease (Gravesdisease with coexistent TSH-depen-dent nodules). The latter will appear atscintigraphy as a gland with diffuse in-creased trapping of the radiotracer withsuperimposed cold nodules. If the TFTresults are elevated but the RAIU levelis normal. one should consider Plum-mer disease (hyperthyroidism due to asolitary autonomous hot nodule thatsuppresses the remainder of the gland),Graves disease with rapid iodine tum-over, or a laboratory error (75). IfTFTresults are elevated but the RAIU levelis depressed, the possibilities includesubacute granulomatous thyroiditis,subacute lymphocytic thyroiditis, post-partum thyroiditis, and struma ovarii.With thyroiditides, thyroid hormonemay escape ruptured follicles leadingto ffansient hyperthyroidism, but thedamaged gland cannot concentrate io-dine so the RAIU and thyroid scansshow depressed uptake (75).
Graves disease,-4raves disease isthe most common cause of hyperthy-roidism. This disease affects womenmuch more commonly than men, and afamilial tendency is present. Patientsmay have heat intolerance, weight loss,fatigue, insomnia, tremors, palpita-tions, increased thirst and hunger, andagitation. Exophthalmos may be pres-ent, but thyroid eye disease need notoccurjust in the setting ofhyperthy-roidism; it may be present after therapywhen the patient is euthyroid or evenhypothyroid. Thyroid-stimulating im-munoglobulins such as long-actingthyroid stimulator simulate the func-tion of TSH and cause hyperthyroid-ism. In a patient with hyperthyroidism,scintigraphy may be very useful in dis-
Parathyroid and Thyroid lmaging I lO3

tinguishing Graves disease, whichshows homogeneous diffuse intenseuptake (7OVo-85Vo) rn a large gland,from the thyroiditides (Fig I l). Thy-roiditis is less homogeneous and theuptake may be normal, high, or lowdepending on the state of the inflam-fnatory process. Because some thY-roiditides (see below) may revert toeuthyroid activity with time, the im-plications for therapy are important:Graves disease requires antithyroidmedication, radioactive iodine oblit-eration ofthe gland, or surgery.Thyroiditides are treated conserva-tively. Diffuse glandular enlargementwith avid enhancement may be notedat CT and MR imaging in patientswith Graves disease. A large pyrami-dal lobe often coexists. Carcinoma ofthe thyroid gland in a patient withGraves disease is rare, reported inO.l57o4.5Vo of patients (76).
Hypothyroidism.-Patients with hy-pothyroidism have cold intolerance,fatigue, apathy, weight gain, bradycar-dia, constipation, edema, macroglos-sia, and poor condition of the hair,nails, and skin. Women are affectedmore frequently than men. The re-sponse to thyroid hormone replace-ment is excellent. Hashimoto thyroidi-tis is the most common cause of hY-pothyroidism in the United States (seebelow). Worldwide, iodine deficiency(endemic goiter) is another cause ofhypothyroidism but is infrequentlyseen in developed countries. Othercauses include the other chronicthyroiditides. Postoperative andpostradiation therapy (be it I-131 orextemal beam irradiation) patientsalso account for a great number of hy-pothyroid patients. It is common forpatients treated with radioactive io-dine for hyperthyroidism to develophypothyroidism after several years.
Congenital hypothyroidism occursmore commonly in the Japanese popu-lation (one in 5,500 newborns) (77).Possible causes include thyroid apla-sia, hemiaplasia (the left gland is ab-sent more commonly than the right),ectopia, dyshormonogenesis, pifuitaryor hypothalamic deficiency, and au-toimmune diseases. Prompt replace-ment of thyroid hormone is crucial be-cause mental retardation is a possiblecomplication of undiagnosed neonatalhypothyroidism (77). Both US andscintigraphy are used to identify thy-roid tissue in this population.
1O4 I Yousem
Figure 12. Thy-roglosssal ductcyst. T2-weightedMR image (3,000/80) shows that thecyst (+) is off mid-line and infrahy-oid, yet embeddedin the strap mus-cles. A tract to themidline (arrows) isevident.
I Gongenital LesionsThyro glo s sal duct cy st s.--The thy-
roglossal duct cyst is a congenital le-sion in which the tract of migration ofthe thyroid gland from the foramencecum of the tongue (located in themidline at the circumvallate papillaelevel) to the normal position of thethyroid gland is persistent. Although acongenital lesion, 507o of cases presentafter age 10 years. One sees a midlinecystic mass that is located in an infra-hyoid level in657o, hyoid level in151o, and suprahyoid level in 20Vo ofcases (78). It may occur in a paramed-ian position in25vo of cases, usually inthe infrahyoid compartment. The ste-reotypical locations of the thyroglossalduct cyst are embedded in the strapmuscles below the hyoid bone or at themidline junction of the hyoid boneabove the strap muscle insertions (Fig12).
Because the fluid in the thyroglossalduct cyst may have a high protein con-tent, it may appear cystic with someinternal echoes at US. It moves withswallowing or when sticking thetongue out. At CT, the noninfectedthyroglossal duct cyst varies in inten-sity from markedly hypoattenuating(with no protein content) to slightlyhyperattenuating (with high protein orhemorrhage within). At MR imaging,the thyroglossal duct cyst may have ei-ther low or high signal intensity on T1-weighted images but is typicallyhyperintense on T2-weighted images.Enhancement is uncommon in thyro-glossal duct cysts unless the lesion hasbeen traumatized or infected. In thoseinstances, peripheral rim enhancementmay occur.
Ectopic thyroid tissue is found inroughly 25Vo-33Vo of thyroglossal
duct cysts (78,79). The incidence ofcarcinoma within the thyroid tissue ofa thyroglossal duct cyst is less than 17o(78,79). When it occurs, it is usuallypapillary carcinoma. Rarely the tract ofthe thyroglossal duct may serve asconduit for acute suppurative thyroidi-ris (79).
Lin g ual thy r oid glands. -Lingual
thyroid tissue occurs in one in 3,000patients with thyroid disease and repre-sents the most common form of func-tioning ectopic thyroid tissue (51). It isalso the most common benign massfound at the circumvallate papillae.The lingual thyroid gland representsarrest of migration of the thyroid tissuewithin the tongue, usually in the mid-line between the circumvallate papillaeand the epiglottis. This may be a com-plete arest or incomplete arrest of mi-gration. Lingual thyroid glands are as-sociated with absence of thyroid tissuein the neck in70Vo-80Vo ofcases andare much more commonly seen inwomen (51,63,80). Patients oftenpresent in puberty, during which timethe tissue may expand rapidly. Varia-tion in size may occur with menstrua-tion.
The primary role of imaging is toidentify whether thete is normal thy-roidal tissue in the lower neck so thatcomplete excision or transplantation ofthe lingual thyroid tissue may be con-templated. If no other thyroid tissue ispresent, the patient is consigned tolife-long thyroid replacement therapyif the lingual thyroid gland is totallyremoved. A nuclear medicine study todetermine whether a lingual mass rep-resents thyroid tissue, as well as tosearch for other (ectopic) thyroid tis-sue. is favored over cross-sectional im-aging. A malignancy arising within a

lingual thyroid gland is more commonthan one in a thyroglossal duct cyst. Atleast one report noted a frequency of2.8Vo (81).
Ab e rrant thy roid msze.-Thyroidtissue lateral to the jugular vein unas-sociated with lymphadenopathy mayoccur due to anomalous developmentand is termed lateral aberrant thyroidtissue. This phrase is rarely used nowa-days, since most cases of "lateral aber-rant thyroid tissue" actually repre-sented thyroid carcinoma metastases tolymph nodes. Nonetheless, in rare in-stances, thyroid tissue may be "seeded"to this location by trauma, surgery, thy-roiditis, or goiters but must be distin-guished from metastatic thyroid cancer.
Undescended thyroid tissue maysometimes be seen in the anterior necksuperficial to the hyoid bone. Aberrantthyroid tissue may also be found in thetrachea. In this site, women are af-fected more commonly than men andthe thyroid tissue may respond to hor-monal influences. Struma ovarii, thepresence of functioning thyroid tissuein the ovaries or in an ovarian ter-atoma/dermoid, is rare.
Substernal thyroid tissue is not un-common but usually occurs in associa-tion with a goitrous gland extendingdownward rather than as isolated tis-sue. Tracheal or esophageal compres-sion at chest radiography may be thepresenting finding. Imaging to distin-guish a goiter from mediastinal ad-enopathy, thymoma, lymphoma, ter-atoma, carcinoma, or an unusual bron-chogenic cyst is usually pursued withCT.
I Inflammatory LesionsThere are no specific scintigraphic,
sonographic, CT, or MR imaging ap-pearances that enable differentiationamong the various inflammatory pro-cesses involving the thyroid gland. Thevalue of imaging studies pales in com-parison to that of serologic tests fordistinguishing among the various in-flammatory lesions of the thyroidgland. Conversely, if imaging is to beused as a map for surgical correction orresection of the thyroid gland, then MRimaging and US seem to be of particu-lar benefit. In some instances, the ad-ministration of iodine at contrast-en-hanced CT might precipitate thyroidstorm (acute outpouring of thyroid hor-mone), so CT is usually avoided.
S up p u r at iv e t hy ro i dit i s. -P atients
with acute suppurative thyroiditispresent with acute onset ofpain andswelling in the thyroid gland associ-ated with fever, odynophagia, and dys-phagia (8 l). The role of imaging is toexclude a pyriform sinus or thyroglos-sal duct fistula as a cause for the acutesuppurative thyroiditis. This entitymay occur in association with a fourthbranchial cleft anomaly and has a left-sided predominance (81). Imaging maydepict leakage from the pyriform sinusto the lateral neck at the thyroid glandlevel. Acute suppurative thyroiditis isthe rarest form of thyroiditis but hasthe most fulminant clinical presenta-tion.
H a s himo to thy ro idit i s. -Most ofthe other forms of thyroiditis are sub-acute or chronic diseases. Hashimoto(chronic lymphocytic) thyroiditis is themost common of the chronic thyroidi-tides, being five to l0 times more fre-quent than subacute thyroiditis (7). Itis the most common thyroiditis in chil-dren. The diagnosis is based on sero-logic tests because the disease is an au-toimmune process with antigenicstimulation to thyroglobulin, colloid,and other thyroid cell antigens. SerumIevels of antimicrosomal antibodies areelevated, and FNA may reveal a pre-ponderance of lymphocytes, centro-blasts, and Hiirthle cells (82). Womenare affected almost 20 times more fre-quently than men, and the chief com-plaint is usually enlargement and ten-derness of the thyroid gland. Hypothy-roidism is present at presentation ordevelops later in 507o ofcases.
With Hashimoto thyroiditis, thegland is enlarged and shows multinod-ularity and heterogeneous increased ordecreased uptake of radiotracers. Al-though there may be increased uptakeof iodine on nuclear medicine studiesearly in the disease, the usual responseis diminished or normal thyroid uptakeat imaging (82). Patients who trapmore tracer have a greater chance ofreturning to a euthyroid state thanthose who do not. At US, the thyroidgland is symmetrically enlarged andhypoechoic but may have noduleswithin it. Calcification is seen in thechronic stages. On T2-weighted MRimages, the gland has shown increasedsignal intensity, sometimes with linearlow intensity bands thought to repre-sent fibrosis (60,73). Hashimoto thy-roiditis shows no greater risk for carci-noma but seems to predispose to non-
Hodgkin lymphoma (70). Hashimotothyroiditis in the presence of thyroidlymphoma is seen in 25%o-6lvo ofcases (69,70). Hashimoto disease hasalso been associated with other au-toimmune entities such as perniciousanemia, Sjcigren syndrome, lupus,rheumatoid arthritis, Addison disease,and Graves disease.
Rie del thy roidiris.-Riedel thyroidi-tis (struma thyroiditis) is an uncom-mon chronic inflammatory lesion ofthe thyroid gland and neck. The dis-ease may be bilateral or unilateral andis more common in women than men.Patients present with evidence of masseffect with compression of the trachea,hoarseness, and difficulty in swallow-ing. Usually, the patients have hy-pothyroidism. At imaging, Riedel thy-roiditis is homogeneously hypoechoicat US and is usually hypoattenuatingto normal thyroid tissue at CT (5,73).The lesion may be isoattenuating tomuscle at unenhanced CT. Riedel thy-roiditis may spread outside the thyroidgland, infiltrating and obliterating ad-jacent tissue planes. The characteristicfinding on MR images is hypointensityat T1- and T2-weighted imaging, withinfiltration of adjacent structures of theneck (73). The low signal intensity atMR imaging is thought to be due tothe fibrotic nature of the disorder. Thislesion may be associated with retro-peritoneal fibrosis, mediastinal fibro-sis, sclerosing cholangitis, and orbitalpseudotumor. It is distinguished fromHashimoto thyroiditis, which has highsignal intensity on T2-weighted MRimages.
de Quervain thyroiditis.- e Quer-vain thyroiditis (subacute thyroiditis)is a disease of middle age occurringmost commonly in women after an up-per respiratory infection. Coxsackie,ECHO, and mumps viruses have beenimplicated (1). Pain, fever, and fatigueare cornmon presenting symptoms. Pa-tients with subacute thyroiditis maypresent (507o ofcases) with acute toxichyperthyroidism, with subsequent re-turn to an euthyroid state after l-2months (5 1). Hypothyroidism occursapproximately 2-4 months after onsetand, typically, the patient reverts to eu-thyroidism within 6 months of theacute onset (7). Patients are typicallytreated medically, as the prognosis isgood for return of normal thyroid func-tion. Subacute thyroiditis is hypo-echoic at US, although there may be
Parathyroid and Thyroid lmaging I l05
latrophy of thyroidal tissue with time(5). Nuclear medicine studies showheterogeneous uptake that will vary indegree according to the stage of thedisease.
M i s c e llane ous.-External beam ra-diation may cause a chronic thyroiditisassociated with fibrosis. In low doses(used in years past for irradiating thethymus, adenoids, acne, or ringworm),radiation predisposes to papillary car-cinoma. Radioactive iodine treatmentalso causes severe fibrosis and atrophyof the gland. Amyloidosis and hemo-chromatosis may affect the thyroidgland and lead to decreased signal in-tensity on T2-weighted MR images.Tuberculosis, sarcoidosis, and fungalinfections may cause a granulomatousinflammation of the thyroid gland butare uncommon conditions (36).
References|. Livolsi V. The thyroid and parathy-
roid. In: Sternberg SS, ed. Diagnosticsurgical pathology. 2nd ed. NewYork, NY: Raven, 1994; 523-560.
2. Livolsi VA. Pathology of the para-thyroid glands. In: Barnes L, ed. Sur-gical pathology of the head and neck.New York, NY: Dekker, 1995;1487-1563.
3. Kang YS, Rosen K, Clark OH, Hig-gins CB. Localization of abnormalparathyroid glands of the mediasti-num with MR imaging. Radiology1 9 9 3 ; 1 8 9 : 1 3 7 - 1 4 1 .
4. Health H, Hodgson SF, Kennedy MA.Primary hyperparathyroidism: inci-dence, morbidity, and potential im-pact in a community. N Engl J Med1980:302:189-193.
5. Gooding GA. Sonography of thethyroid and parathyroid. Radiol ClinNorth Am 1993; 31967 -989.
6. Gooding GAW, Okerlund MD, StarkDD, Clark OH. Parathyroid imag-ing: comparison of double-tracer (Tl-201, Tc-99m) scintigraphy and high-resolution US. Radiology 1986; 161:57-64.
7. Price DC. Radioisotopic evaluationof the thyroid and the parathyroids.Radiol Clin North Am 1993t 3l:991-1015.
8. Thompson CT. Localization studiesin patients with hyperparathyroidism.Br J Surg 1988; 75:97-98.
9. Thompson NW, Eckhauser FE, Har-ness JK. The anatomy of primaryhyperparathyroidism. Surgery 1982;92:814-821.
10. Freitas JE, Freitas AE. Thyroid andparathyroid imaging (review). SeminNucl Med 1994; 24:234-245.
11. Kneeland JB, Kruback AJ, LawsonTL, et al. Enlarged parathyroidglands: high-resolution local coil MR
106 I Yousem
imaging. Radiology 198'l : 162:143-146.
12. Peck WW, Higgins CB, Fisher MR,Ling M, Okerlund MD, Clark OH.Hyperparathyroidism: comparison ofMR imaging with radionuclide scan-ning. Radiology 198'7 ; 163:415420.
13. Seelos KC, DeMarco R, Clark OH,Higgins CB. Persistent and recur-rent hyperparathyroidism: assessmentwith gadopentetate dimeglumine-en-hanced MR imaging. Radiology 1990;177:373-378.
14. Spritzer CE, Gefter WB, Hamilton R,Greenberg BM, Axel L, Kressel HY.Abnormal parathyroid glands: high-resolution MR imaging. Radiology1987: 162:487-491.
15. Morita ET, Kwan WP, Clark OH.Technetium Tc-99m sestamibi forparathyroid imaging. West J Med1994r 161:413.
16. Oates E. Improved parathyroid scin-tigraphy with Tc-99m MIBI, a supe-rior radiotracer. Appl Radiol 1994;l5:37-42.
17. Carlson GL, Farndon JR, Clayton B,Rose PG. Thallium isotope scintig-raphy and ultrasonography: compara-tive studies of localization techniquesin primary hyperparathyroidism. Br JSurg 1990;77:327-329.
18. Miller DL. Pre-operative localiza-tion and international treatment ofparathyroid tumors: when and how?World J Surg 1991; 15:706*715.
19. Roe SM, Burns RP, Graham LD, et al.Cost-effectiveness of preoperative lo-calization studies in primary hyper-parathyroid disease. Ann Surg 1994;219:582-586.
20. Edis AJ, Sheedy PF, Beahrs OH, et al.Results of reoperation for hyperpar-athyroidism, with evaluation of pre-operative localization studies. Sur-gery 1978;84 :384-391.
21. Reading CC, Charboneau JW, JamesEM, et al. High-resolution parathy-roid sonography. AJR 1982; 139:539-546.
22. Satava RM, Beahrs OH, Scholz DA.Success rate of cervical explorationfor hyperparathyroidism. Arch Surg1975: 110: 625427.
23. Levin KE, Clark AH, Duh Qy, De-meure M, Siperstein AE, Clard OH.Reoperative thyroid surgery. Surgery1992'. lll:604-609.
24. Mattar AG, Wright ES, Chittal SM, etal. Impact on surgery of preopera-tive localization of parathyroid le-sions with dual radionuclide subtrac-tion scanning. Can J Surg 1986;29:57-59.
25. Russell CF, Laird JD, Ferguson WR.Scan-directed unilateral cervical ex-ploration for parathyroid adenoma: alegitimate approach? World J Surg1990; 14:406409.
26. Tibblin S, Bondeson AG, LjungbergO. Unilateral parathyroidectomy in
hyperparathyroidism due to single ad-enoma. Ann Surg 1982; 195:245-252.
27. Casas AT, Burke GJ, Mansberger ARJr, Wei JP. Impact of Tc-99m-sesta-mibi localization on operative timeand success of operations for primaryhyperparathyroidism. Am Surg 1994:6O:12-17.
28. Uden P, Aspelin P, Berglund J, et al.Preoperative localization in unilateralparathyroid surgery: a cost-benefitstudy on US, CT, and scintigraphy.Acta Chir Scand 1990; 150:29-35.
29. Miller DL, Doppman JL, ShawkerTH, et al. Localization ofparathy-roid adenomas in patients who haveundergone surgery. I. Noninvasiveimaging methods. Radiology 1987;162:133-137.
30. Funari M, Campos Z, Gooding GA,Higgins CB. MR and US detectionof asymptomatic thyroid nodules inhyperparathyroidism. J Comput AssistTomogr 1992; 16:615-619.
31. Rodriquez JM, Tezelman S, Siper-stein AE, et al. Localization proce-dures in patients with persistent or re-current hyperparathyroidisrn. ArchSurg 1994; 129:870-87 5.
32. Brown LR, Aughenbaugh LG.Masses of the anterior mediastinum:CT and MR imaging. AJR l99l; 157:1 t7 l - l 180 .
33. Stark DD, Gooding GAW, Moss AA.Parathyroid imaging: comparison ofhigh-resolution CT and high-resolu-tion sonography. AJR 1983; 14l:633-638.
34. Sommer B, Welter HF, Spelsberg F,et al. CT for localizing enlargedparathyroid glands in primary hyper-parathyroidism. J Comput Assist To-mogr 1982; 6:521-526.
35. Mitchell BK, Kinder BK, Cornelius E,Stewart AF. Primary hyperparathy-roidism: preoperative localization us-ing technetium-sestamibi scanning. JClin Endocrinol Metab 1995; 80:7-10 .
36. Basso LV, Keeling C, Goris ML.Parathyroid imaging: use of dual-iso-tope scintigraphy for the localizationof adenomas before surgery. ClinNucl Med 1992: 17:380-383.
37. O'Doherty MJ, Kettle AG, Wells P, etal. Parathyroid imaging with techne-tium-99m-sestamibi: preoperative lo-calization and tissue uptake studies. JNucl Med 1992: 33:313-318.
38. Hindie E, Melliere D, Simon D, Perle-muter L, Galle P. Primary hyperpar-athyroidism: is technetium 99m-sestamibi./iodine- I 23 subtractionscanning the best procedure to locateenlarged glands before surgery? JClin Endocrinol Metab 1995: 80:302-307.
39. Khan A, Samtani S, Varma VM, FrostA, Cohen J. Preoperative parathy-roid localization: prospective evalua-tion of technetium 99m sestamibi.

Otolaryngol Head Neck Surg 1994;llI:467472.
40. Taillefer R, Boucher Y, Potvin C,Lambert L. Detection and localiza-tion of parathyroid adenomas in pa-tients with hyperparathyroidism usinga single radionuclide imaging proce-dure with technetium-99m-sestamibi(double phase study). J Nucl Med1992; 33: I 801-1807.
41. Lee VS, Wilkinson RH, Leight GS Jr,et al. Hyperparathyroidism in high-risk surgical patients: evaluation withdouble-phase Tc-99m sestamibi im-aging. Radiology 1995; 197 : 627-633.
42. Yen TC, Lin HD, Lee CH, Chang SL,Yeh SH. The role of technetium-99m sestamibi whole-body scans indiagnosing metastatic Hurthle cellcarcinoma of the thyroid gland aftertotal thyroidectomy: a comparisonwith iodine-l31 and thallium-20lwhole-body scans. Eur J Nucl Med1994: 2l:980-983.
43. Miller DL, Doppman JL, Krudy AG,et al. Localization of parathyroidadenomas in patients who have un-dergone surgery. ll. Invasive proce-dures. Radiolo gy 1987 ; 162:138-141.
44. Hamilton R, Greenburg BM, GefterW, Kressel H, Spritzer C. Success-ful localization of parathyroid ad-enomas by magnetic resonance imag-ing. Am J Surg 1988; 129:.370-373.
45. Majors JD, Burke GJ, MansbergerAR Jr, Wei JP. Technetium Tc-99msestamibi scan for localizing abnor-mal parathyroid glands after previousneck operations: preliminary experi-ence in reoperative cases. South MedJ 1995: 88:327-330.
46. Weber CJ, Vansant J, Alazraki N, etal. Value oftechnetium 99m sesta-mibi iodine 123 imaging in reopera-tive parathyroid surgery. Surgery1993; I14 :1011-1018.
47. Numerow LM, Morita ET, Clark OH,Higgins CB, Persistent/recurrenthyperparathyroidism: a comparisonof sestamibi scintigraphy, MR imag-ing, and US. JMRI 1995;5:702--708.
48. Wei JP, Burke GJ, Mansberger AR Jr.Preoperative imaging of abnormalparathyroid glands in patients withhyperparathyroid disease using com-bination Tc-99m-pertechnetate andTc-99m-sestamibi radionuclide scans.Ann Surg 1994: ?19:568-572.
49. Edmonson GR, Charboneau JW,James EM, Reading CC, Grant CS.Parathyroid carcinoma: high-fre-quency sonographic features. Radiol-ogy 1986; 16l:65-67.
50. Kitapci MT, Tastekin G, Turgut M; etal. Preoperative localization ofparathyroid carcinoma using Tc-99mMIBI. Clin Nucl Med 1993; 18''217-219.
5 1. Schwartz SI, Shires GT, Spencer FC,
Storer EH. Principles of surgery.3rd ed. New York, NY: McGrawHill, 1979; 1547.
52. Solbiati L, Volterani L, Rizzatto G,et al. The thyroid gland with lowuptake lesions: evaluation by US. Ra-diology 1985; 155: 187-191.
53. Walker JM, Margouleff D. A clini-cal manual of nuclear medicine. Nor-walk, Conn: Appleton-Century-Crofts, 1984.
54. Sandler MP, Patton JA, Ossoff RH.Recent advances in thyroid imaging.Otolaryngol Clin North Am 1990;23:251-27O.
55. Klieger PS, Wilson GA, GreenspanBS. The usefulness of the dynamicphase in pertechnetate thyroid imag-ing for solitary hypofunctioning nod-ules. Clin Nucl Med 1992; 17:617-622.
56. Reading CC, Gorman CA. Thyroidimaging techniques. Clin Lab Med1993; l3:7ll-724.
57. Beahrs OH, Kiernan PD, Hubert JPJr. Cancer of the thyroid gland. In:Suen JY, Myers E, eds. Cancer of thehead and neck. New York, NY:Churchill Livingstone, 1981; 599-632.
58. Som PM, Brandwein M, Lidov M,Lawson W, Biller HF. The variedappearance of papillary carcinomacervical nodal disease: CT and MRfindings. AJNR 1994; 15:1 129-1138.
59. Som PM. Lymph nodes of the neck.Radiology 1987; 165:593-600.
60. Gefter WB, Spritzer CE, LiVolsi VA,et al. Thyroid imaging with high-field-strength surface-coil MR. Radi-ology 1987; 164:483-490.Noma S, Kanaoka M, Minami S, etal. Thyroid masses: MR imagingand pathologic correlation. Radiol-ogy 1988; 168:759-764.
62. Auffermann W, Clark OH, ThurnherS, Galante M, Higgins CB. Recur-rent thyroid carcinoma: characteris-tics on MR images. Radiology 1988;168:753-757.
63. Burman KD, Anderson JH, Wartof-sky L, Mong DP, Jelinek JJ. Man-agement of patients with thyroid car-cinoma: application of thallium-201scintigraphy and magnetic resonanceimaging. J Nucl Med 1990; 31:1958-1964.
64. Gharib H, Goellner JR, Johnson DA.FNA cytology of rhe thyroid: a 12-year experience with I 1,000 biopsies.Clin Lab Med 1995; 13:699-71O.
65. Sutton RT, Reading CC, CharboneauJW, et al. US-guided biopsy ofneck masses in postoperative man-agement of patients with thyroid can-cer. Radiology 1988;' 168:769-772.
66. Woolner LB, Beahs OH, Black BM,et al. Classification and prognosisof thyroid cancer. Am J Surg 196l;lO2:354-387.
67. Gorman B, Charboneau JW, James
EM, et al. Medullary thyroid carci-noma: role of high-resolution US. Ra-diology 1987 ; 162:147 -15O.
68. Takashima S, Morimoto S, Ikezoe J,et al. CT evaluation of anaplasticthyroid carcinoma. AJR 1990; 154:1079-1085.
69. Compagno J, Oertel JE. Malignantlymphoma and other lymphoprolifera-tive disorders of the thyroid gland:clinicopathologic study of 245 cases.Am J Clin Pathol 1980; 74:l-ll.
70. Takashima S, Ikezoe J, Morimoto S,et al. Primary thyroid lymphoma:evaluation with CT. Radiology 1988;168:765-'168.
71. Shibata T, Noma S, Nakano Y, Ko-nishi J. Primary thyroid lymphoma:MR appearance. J Comput AssistTomogr l99l; 15:629-633.
72. Ohnishi T, Noguchi S, Murakami N,et al. MR imaging in patients withprimary thyroid lymphoma. AJNR1992: 13:1196-1198.
73. Perez FFJ, Cordido CF, Pombo FF,Mosquera OJ, Villalba MC. Riedelthyroiditis: US, CT, and MR evalua-tion. J Comput Assist Tomogr 1993;17:324-325.
74. Shulkin BL, Shapiro B. The role ofimaging tests in the diagnosis of thy-roid carcinoma. Endocrinol MetabClin North Am 1990; 19:523*543.
75.lntenzo CM, Park CH, Kim SM.Thyroid scintigraphy of hyperthyroxi-nemia. Clin Nucl Med 1993; 18:981-985.
76. Compagno J. Diseases of the thy-roid. In: Barnes L, ed. Surgical pa-thology ofthe head and neck. NewYork, NY: Dekker, 1995;1435-1486.
77. Takashima S, Nomura N, Tanaka H,et al. Congenital hypothyroidism:assessment with US. AJNR 1995:16:ll17-1123.
78. Batsakis JG. Tumors of the headand neck: clinical and pathologicalconsiderations. Baltimore, Md: Will-iams & Wilkins, 1979.
79. Hays LL, Marlow SF Jr. Papillarycarcinoma arising in a thyroglossalduct cyst. Laryngoscope 1968; 78:2189-2193.
80. Kawanaka M, Sugimoto Y, SuehiroM, Fukuchi M. Thyroid imaging ina typical case of acute suppurativethyroiditis with abscess formation dueto infection from a persistent thyro-glossal duct. Ann Nucl Med 1994;8:159-162.
81. Guneri A, Ceryan K, Igci E, Kovanli-kaya A. Lingual thyroid: the diag-nostic value of magnetic resonanceimaging. J Laryngol Otol l99l; 105:493-495.
82. Montgomery ML. Lingual thyroid:comprehensive review. West J Surg1935:43:661471.
Parathyroid and Thyroid lmaging I 1O7

NOTES


















