Lars Ettarp, President, International Federation of ... · Fast Facts: Psoriasis the best offers...
14
Fast Facts Fast Facts: Psoriasis Alan Menter, Catherine Smith and Jonathan Barker Fourth edition © 2014 Health Press Ltd. www.fastfacts.com
Transcript of Lars Ettarp, President, International Federation of ... · Fast Facts: Psoriasis the best offers...

Fast Facts: Psoriasis
the best offers are on
fastfacts.com
Fast Facts Pso
riasis
Fast Facts
Fourth edition
7 Epidemiology and pathophysiology
15 Clinical presentation
31 Differential diagnosis
38 General management approach
45 Topical therapy
65 Phototherapy and photochemotherapy
74 Systemic therapy
85 Receptor-targeted (biological) therapies
96 Psoriatic arthritis
112 Future trends
“This book reflects well the WHO’s current view of psoriasis as a chronic inflammatory condition with close links to the metabolic condition and a number of comorbidities. It
will be of great benefit in passing on new knowledge of psoriasis to health professionals, administrators and patient representatives around the world.”
Lars Ettarp, President, International Federation of Psoriasis Associations (IFPA) Fast Facts:
PsoriasisAlan Menter, Catherine Smith and Jonathan Barker
Fourth edition
© 2014 Health Press Ltd. www.fastfacts.com

Fast Facts
Fast Facts: Psoriasis Fourth edition
Alan Menter MD
Chair, Psoriasis Research Unit
Baylor Medical Center, Dallas, and
Clinical Professor, University of Texas
Southwestern Medical School
Dallas, USA
Catherine Smith MD FRCP
Professor of Dermatology and Therapeutics
St John’s Institute of Dermatology
Guy’s and St Thomas NHS Foundation Trust
London, UK
Jonathan Barker MD FRCP FRCPath
Professor of Medical Dermatology, and
Head of Department
St John’s Institute of Dermatology
King’s College, London, UK
Declaration of IndependenceThis book is as balanced and as practical as we can make it.Ideas for improvement are always welcome: [email protected]
© 2014 Health Press Ltd. www.fastfacts.com

Fast Facts: Psoriasis First published 2002; second edition 2004; third edition 2008, reprinted 2009, 2010 Fourth edition September 2014
Text © 2014 Alan Menter, Catherine Smith, Jonathan Barker © 2014 in this edition Health Press Limited
Health Press Limited, Elizabeth House, Queen Street, Abingdon, Oxford OX14 3LN, UK Tel: +44 (0)1235 523233 Fax: +44 (0)1235 523238
Book orders can be placed by telephone or via the website. For regional distributors or to order via the website, please go to: fastfacts.com For telephone orders, please call +44 (0)1752 202301 (UK, Europe and Asia–Pacific), 1 800 247 6553 (USA, toll free) or +1 419 281 1802 (Americas).
Fast Facts is a trademark of Health Press Limited.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the express permission of the publisher.
The rights of Alan Menter, Catherine Smith and Jonathan Barker to be identified as the authors of this work have been asserted in accordance with the Copyright, Designs & Patents Act 1988 Sections 77 and 78.
The publisher and the authors have made every effort to ensure the accuracy of this book, but cannot accept responsibility for any errors or omissions.
For all drugs, please consult the product labeling approved in your country for prescribing information.
Registered names, trademarks, etc. used in this book, even when not marked as such, are not to be considered unprotected by law.
A CIP record for this title is available from the British Library.
ISBN 978-1-908541-74-1
Menter A (Alan) Fast Facts: Psoriasis/ Alan Menter, Catherine Smith, Jonathan Barker
Medical illustrations by Dee McLean, London, UK. Typesetting by Thomas Bohm, User Design, UK. Printed by Latimer Trend & Company Limited, Plymouth, UK.
Text printed on biodegradable and recyclable paper manufactured using elemental chlorine free (ECF) wood pulp from well-managed forests.
© 2014 Health Press Ltd. www.fastfacts.com

Introduction 5
List of abbreviations 4
Epidemiology and pathophysiology 7
Clinical presentation 15
Differential diagnosis 31
General management approach 38
Topical therapy 45
Phototherapy and photochemotherapy 65
Systemic therapy 74
Receptor-targeted (biological) therapies 85
Psoriatic arthritis 96
Future trends 112
Useful resources 114
Index 116
© 2014 Health Press Ltd. www.fastfacts.com
4
List of abbreviations
APC: antigen-presenting cell
cAMP: cyclic adenosine monophosphate
COX: cyclooxygenase (inhibitor)
CRP: C-reactive protein
ESR: erythrocyte sedimentation rate
HIV: human immunodeficiency virus
HLA: human leukocyte antigen
ICAM1: intercellular adhesion molecule 1
Ig: immunoglobulin
IL: interleukin
LFA1: lymphocyte function-associated antigen 1
MED: minimal erythema dose; amount of radiation required to produce faint, but definite, erythema
NASH: non-alcoholic steatohepatitis
NSAID: non-steroidal anti-inflammatory drug
PASI: Psoriasis Area and Severity Index
PDE4: phosphodiesterase 4 (inhibitor)
PSORS1: psoriasis susceptibility locus
PUVA: photochemotherapy; combination of methoxsalen (psoralen), a photosensitizing drug, and long-wave ultraviolet A radiation
Th cell: T helper cell
TNFα: tumor necrosis factor α
TPMT: thiopurine methyltransferase
UV: ultraviolet (A and B) radiation
© 2014 Health Press Ltd. www.fastfacts.com
5
Introduction
Psoriasis is a common, chronic and disfiguring skin disease with
significant quality of life issues for every individual affected worldwide
(over 120 million). The significant growth in the number of patient
organizations around the world and the development of major new
biological agents are testimony to the increasing importance being
given to this common disorder.
Given the advances in genetics and immunology that have
furthered our understanding of the condition and resulted in
dramatically effective new treatments, psoriasis can no longer be
considered a mere ‘skin disease’. The disease called ‘Psoriasis’ has
a host of phenotypic variants, and multiple medical conditions have
been shown to be associated with the disease (see Chapter 2).
Cardiovascular disease is now more readily recognized as a
comorbidity of psoriasis, as are the consequences that this may have
for therapeutic intervention. An ongoing major issue of debate is
whether it is just patients with more extensive forms of psoriasis,
i.e. moderate to severe, who develop these comorbidities and a
potential shorter life span, or whether these comorbidities reach across
the whole spectrum of the disease.
We also need to answer the vexing questions as to why psoriatic
arthritis, which affects up to 30% of the psoriatic population, has its
onset approximately 10 years later than that of the skin manifestations
and why it has genetic, immunologic and therapeutic differences to
psoriasis.
Since the third edition, the main area of therapeutic advance
remains the receptor-targeted (biological) therapies, and the chapter
on these therapies has been updated to provide the latest developments
in this important area.
Receptor-targeted treatments have had a dramatic beneficial effect
on many patients with moderate and severe disease. These treatments
also have a key role in managing individuals with comorbidities such
as arthritis, cardiovascular disease and inflammatory bowel disease,
and in the future may have a role in switching off the systemic
© 2014 Health Press Ltd. www.fastfacts.com

6
Fast Facts: Psoriasis
inflammation associated with the disease that may in turn cause other
comorbidities.
Thus, looking forward – and of significant interest to researchers
and our readership – there is the potential to significantly improve the
quality of life of our patients and to reduce the full range of
comorbidities associated with psoriasis. It is thus essential that
dermatologists work closely with their primary care colleagues, as well
as specialists in cardiology, gastroenterology, rheumatology and
others, and maintain a central role in elucidating the complexity of
psoriasis.
This fourth edition of Fast Facts: Psoriasis is a well-illustrated, easy-
to-read yet comprehensive synopsis of the state of the art in psoriasis,
its pathogenesis and its management. We believe it is a valuable
resource for all health professionals involved in the care and treatment
of individuals with this problematic but increasingly treatable disease.
Acknowledgments. The authors thank Professor Philip Mease, Head
of Seattle Rheumatology Associates; Chief of Rheumatology Research,
Swedish Medical Center; and Clinical Professor, University of
Washington, Seattle, USA, for his chapter on psoriatic arthritis
(page 96).
© 2014 Health Press Ltd. www.fastfacts.com

7
EpidemiologyPsoriasis is a common chronic, disfiguring inflammatory skin disease
that affects up to 3% of the population. Several clinical variants exist
(see Chapter 2) of which chronic plaque psoriasis (psoriasis vulgaris) is
the most common form (85–90% of all cases).
Effects of ethnicity. Although all races are affected, there is
considerable interracial variation. For example, psoriasis is relatively
common in white people but appears to be very uncommon in
American Indians and in Japanese people. Prevalence appears to be
highest in Scandinavian countries and northern Europe.
Effects of gender and age. Men and women are affected equally. The
usual age of onset is 20–35 years, with 75% of all cases occurring for
the first time before 40 years of age. However, psoriasis can occur at
any age, including childhood (often signifying a more severe clinical
course) and old age.
Types of psoriasis. Two types of chronic plaque psoriasis have been
described, based on age of onset, association with human leukocyte
antigen (HLA) and disease course.
• TypeI,thecommonestform,occursinyoungadultswithahigh
probability of a positive family history. Affected individuals tend to
have more severe disease that runs a more irregular course.
• TypeIIhasapeakincidencebetween50and60yearsofage.In
these individuals, a positive family history is very uncommon and
the disease tends to be mild and localized.
Socioeconomic burden. Psoriasis severely affects a patient’s quality of
life in terms of both psychological and physical well-being. Studies
comparing psoriasis with other important chronic diseases have shown
that the impact of psoriasis on the patient’s quality of life is at least as
1 Epidemiology and pathophysiology
© 2014 Health Press Ltd. www.fastfacts.com
8
Fast Facts: Psoriasis
great as that of ischemic heart disease, diabetes and chronic
obstructive pulmonary disease. Psoriasis is therefore a disease of major
socioeconomic importance; in the USA alone, the annual cost to
society has been estimated at US$3.5 billion. Furthermore, there is
increasing evidence of an association between psoriasis and important
comorbidities including cardiovascular and psychiatric disease;
evidence suggests that patients with moderate and severe disease have
a high mortality due to cardiovascular events (see Chapter 2).
In the UK, although most patients with psoriasis have relatively
mild disease, evidence suggests that 30% require second-line treatment
(phototherapy or systemic medication) that involves referral to a
dermatologist and that perhaps 40% of all dermatology inpatients
have psoriasis. In the USA, where inpatient dermatology care is rarely
available, and at many institutions in the UK, specialized psoriasis day
centers have evolved for patients with moderate-to-severe disease. The
advent of new treatments has greatly improved the outlook for many
patients, particularly those with severe disease. Consequently, inpatient
episodes have been dramatically cut, with clear economic benefit.
Pathogenesis and pathophysiologyThe pathogenesis of psoriasis can be described in terms of three
inter-related phases (Figure 1.1):
• theinterplaybetweenenvironmentalandgeneticfactors
• theinteractionbetweeninnate/adaptiveimmunityandkey
inflammatory and epidermal cells
• changesintheepidermisanddermis,suchasexcessivegrowthand
failure of proper differentiation and proliferation and dilatation of
blood vessels, which lead to the development of the clinical
psoriatic plaque.
Genetics. In 1963, Gunnar Lomholt, a pioneer in the epidemiology of
psoriasis, stated in his classic thesis that the disease ‘is capricious and
refuses to part with its innermost secret’, but also wrote: ‘that psoriasis
is genetically conditioned is beyond doubt’. The validity of this
statement has been borne out by population and family studies and
research in twins, all of which suggest an important genetic
© 2014 Health Press Ltd. www.fastfacts.com

9
Epidemiology and pathophysiology
component to the disease. For example, in terms of types I and II
psoriasis (see page 7), approximately 80% of patients with type I
psoriasis are positive for the HLA-Cw6 gene, compared with only
20% of those with type II psoriasis. Approximately 30% of patients
with psoriasis will have a known family history of the disease.
In some families, psoriasis appears to behave like a Mendelian
autosomal dominant disease, whereas in other cases there is little or
no family history. It has been suggested that psoriasis may represent a
spectrum of diseases in which different genes, working either alone or
in concert (polygenic disease), are important in different families.
There have been a number of key genetic advances in recent years:
first, the chromosomal localization (on 6p21.3) of the major psoriasis
genetic locus, psoriasis susceptibility 1 (PSORS1), which contributes
up to 50% of the genetic risk; and secondly, the discovery of several
genes that, while conferring a low genetic risk, point to specific
biological pathways for the disease. To date, approximately 35 genetic
loci have been associated with psoriasis. Interesting candidate genes at
each of these loci cluster around specific biological pathways involved
in the epidermal barrier, innate immunity and adaptive immune
response. They suggest a key role for host defenses against microbes,
Primary event PBMCDC
Th1Th17
Environmental trigger
Innateimmunity
IL-12IL-23
Acquiredimmunity
PSORIASIS
PSORS1 TNFα
Figure 1.1 The interplay between environmental, genetic and
immunologic factors in lesional skin. Antigens may be environmental
antigens, superantigens or autoantigens. DC, dendritic cell; IL, interleukin;
PBMC, peripheral blood mononuclear cell; PSORS1, psoriasis susceptibility 1
gene; Th1/Th17, type 1/type 17 T helper cell; TNFα, tumor necrosis factor α.
© 2014 Health Press Ltd. www.fastfacts.com

10
Fast Facts: Psoriasis
which involve interferon. Intriguingly, these genetic findings indicate a
key role for tumor necrosis factor (TNF)α in disease pathogenesis,
thus supporting therapy targeted at TNF. Furthermore, when
combined with immunologic studies, they define the key T-cell subset
in psoriasis pathogenesis as T helper (Th)-17 cells (see below). This
explains the highly effective treatments designed to block Th17 cells or
prevent their differentiation through inhibition of interleukin (IL)-23
(see Chapter 8).
Environmental factors also play a key etiologic role. For example, in
60% of patients with guttate psoriasis (see page 18), the disease is
precipitated by systemic, usually upper respiratory tract, streptococcal
infection. Other important environmental factors include drugs,
particularly lithium and antimalarials, and physical or psychological
stress. Excessive alcohol intake is also associated with disease
deterioration and makes management more difficult.
Immunologic changes. Evidence that psoriasis is primarily an
immunologic disease comes from many different sources. In evolving
lesions, lymphocytes infiltrate the skin early, before epidermal and
other changes. Psoriasis is associated with certain HLA antigens,
particularly HLA-Cw6, which are cell-surface molecules critical to the
regulation of T-lymphocyte function. Experimentally, psoriasis can be
induced in non-lesional skin transplanted onto mice by injection of
lymphocytes from the same patient. Finally, psoriasis responds rapidly
to treatments designed to inhibit T-lymphocyte function, such as
ciclosporin (cyclosporine), as well as to specific biological agents
targeting key cytokines (IL17, TNFα, etc.) involved in its
immunopathogenesis.
Considerable progress has been made in identifying the precise
lymphocytes that cause the disease (see Genetics above). The antigens
– foreign or auto – to which these lymphocytes respond are currently
unknown, although potentially important lessons can be learnt from
Streptococcus-induced eruptive guttate psoriasis.
There has been an explosion of knowledge about immunopathogenetic
events in psoriasis. In great part, this has been led by advances in
© 2014 Health Press Ltd. www.fastfacts.com

31
3 Differential diagnosis
Although diagnosis is relatively straightforward, a number of other
dermatological entities may be confused with psoriasis (Table 3.1). A
careful medical and family history and physical examination, together
with laboratory findings, will usually reveal the correct diagnosis.
InfectionCandidiasis. In flexural areas, peripheral pustules are characteristic of
Candida infection. The presence of yeast and pseudohyphae in
Gram-stained microscopy specimens will confirm infection.
Tinea, or ringworm, is an infection caused by a dermatophyte fungus
and may sometimes be mistaken for psoriasis. Where diagnostic doubt
exists, appropriate mycological specimens (skin, hair and/or nail)
should be taken.
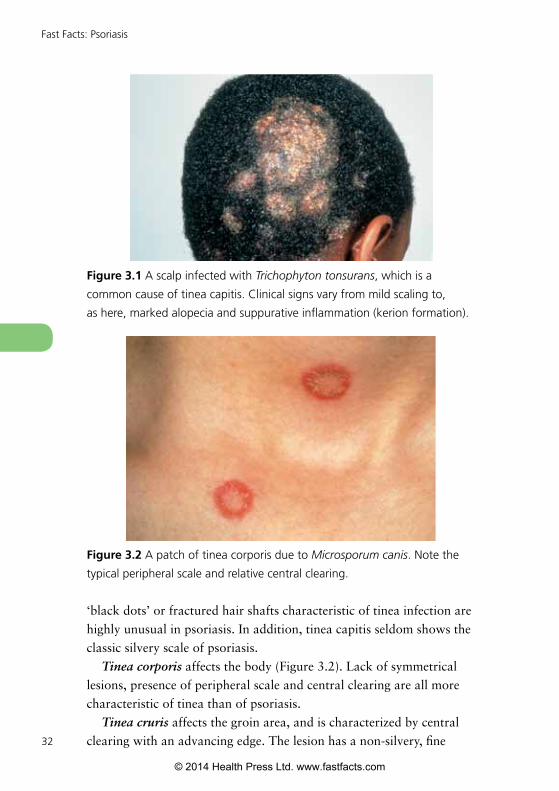
Tinea capitis is ringworm of the head. Although a minor degree of
hair thinning is not uncommon in established cases of psoriasis,
well-demarcated areas of hair loss (Figure 3.1) and signs such as the
TABLE 3.1
Differential diagnosis of psoriasis
• Candidiasis
• Tineainfection
• Syphilis(secondary)
• Eczema(atopicornummular)
• Contactdermatitis
• Drug-inducedrashes
• Lichenplanus
• SuperficialbasalcellcarcinomaandBowen’sdisease
• CutaneousT-celllymphoma(mycosisfungoides)
• Pityriasisrosea
© 2014 Health Press Ltd. www.fastfacts.com
32
Fast Facts: Psoriasis
‘black dots’ or fractured hair shafts characteristic of tinea infection are
highly unusual in psoriasis. In addition, tinea capitis seldom shows the
classic silvery scale of psoriasis.
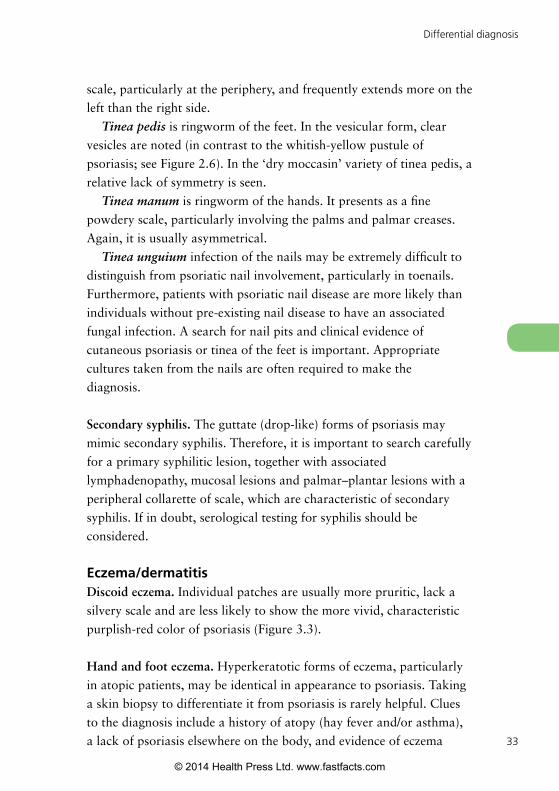
Tinea corporis affects the body (Figure 3.2). Lack of symmetrical
lesions, presence of peripheral scale and central clearing are all more
characteristic of tinea than of psoriasis.
Tinea cruris affects the groin area, and is characterized by central
clearing with an advancing edge. The lesion has a non-silvery, fine
Figure 3.2 A patch of tinea corporis due to Microsporum canis. Note the
typical peripheral scale and relative central clearing.
Figure 3.1 A scalp infected with Trichophyton tonsurans, which is a
common cause of tinea capitis. Clinical signs vary from mild scaling to,
as here, marked alopecia and suppurative inflammation (kerion formation).
© 2014 Health Press Ltd. www.fastfacts.com
33
Differential diagnosis
scale, particularly at the periphery, and frequently extends more on the
left than the right side.
Tinea pedis is ringworm of the feet. In the vesicular form, clear
vesicles are noted (in contrast to the whitish-yellow pustule of
psoriasis; see Figure 2.6). In the ‘dry moccasin’ variety of tinea pedis, a
relative lack of symmetry is seen.
Tinea manum is ringworm of the hands. It presents as a fine
powdery scale, particularly involving the palms and palmar creases.
Again, it is usually asymmetrical.
Tinea unguium infection of the nails may be extremely difficult to
distinguish from psoriatic nail involvement, particularly in toenails.
Furthermore, patients with psoriatic nail disease are more likely than
individuals without pre-existing nail disease to have an associated
fungal infection. A search for nail pits and clinical evidence of
cutaneous psoriasis or tinea of the feet is important. Appropriate
cultures taken from the nails are often required to make the
diagnosis.
Secondary syphilis. The guttate (drop-like) forms of psoriasis may
mimic secondary syphilis. Therefore, it is important to search carefully
for a primary syphilitic lesion, together with associated
lymphadenopathy, mucosal lesions and palmar–plantar lesions with a
peripheral collarette of scale, which are characteristic of secondary
syphilis. If in doubt, serological testing for syphilis should be
considered.
Eczema/dermatitisDiscoid eczema. Individual patches are usually more pruritic, lack a
silvery scale and are less likely to show the more vivid, characteristic
purplish-red color of psoriasis (Figure 3.3).
Hand and foot eczema. Hyperkeratotic forms of eczema, particularly
in atopic patients, may be identical in appearance to psoriasis. Taking
a skin biopsy to differentiate it from psoriasis is rarely helpful. Clues
to the diagnosis include a history of atopy (hay fever and/or asthma),
a lack of psoriasis elsewhere on the body, and evidence of eczema
© 2014 Health Press Ltd. www.fastfacts.com