Laparoscopic Low Anterior Resection for Cancer : “Pursued or just Permitted?” - Dimitris P....
40
LAPAROSCOPIC LOW ANTERIOR RESECTION FOR CANCER: “Pursued or just Permitted?” DIMITRIS P. KORKOLIS, MD, PhD. Senior Consultant Surgeon “St Savvas” Anticancer – Oncological Hospital Athens, GREECE
-
Upload
dimitris-p-korkolis -
Category
Health & Medicine
-
view
35 -
download
0
Transcript of Laparoscopic Low Anterior Resection for Cancer : “Pursued or just Permitted?” - Dimitris P....

LAPAROSCOPIC LOW ANTERIOR
RESECTION FOR CANCER:
“Pursued or just Permitted?”
DIMITRIS P. KORKOLIS, MD, PhD.
Senior Consultant Surgeon
“St Savvas” Anticancer – Oncological Hospital
Athens, GREECE

Laparoscopic TME
2

3
Potential Advantages of Lap TME
• Less blood loss• Faster recovery• Earlier return of gut function• Lower morbidity and mortality• Magnified view allows precise dissection
(pelvic autonomics)• Earlier hospital discharge

4
Potential Advantages of Lap TME
• Reduced pain• Decreased need for analgesics• Improved cosmetic result• Decreased adhesions• Decreased wound complications• Reduced immunosuppressive effect

5
Potential Disadvantages
• Steep learning curve• Longer operating times • Cost– Instruments / equipment
• Port-site recurrence? (Initial reports 21%!!!)
• Oncological safety compared with open TME?

6
Potential Disadvantages
• Practical and technical limitations
– Crowding of instruments in the pelvis– Plume can obscure vision– Retraction of the rectum can be very difficult– Division of the rectum can be difficult– Pneumoperitoneum• Gas embolism / decreased venous return

7
Technical Difficulties in Rectal Surgery
- Narrow confines of the bony pelvis
- Angling limitations of the stapling devices
- Identification of tumor site can be difficult
- High BMI
- Level of rectal tumor from anal verge
- Stage of disease
- Higher anastomotic complications

8
Patients Excluded
• Morbid Obesity• Adjacent organ invasion• Metastatic disease• Cardiovascular, pulmonary or hepatic disease• Inflammatory bowel disease• Need for emergency surgery

9
Critical Points in Rectal Surgery
• TME as “the gold standard” • CRM• Distal resection margins• Adequate lymphadenectomy• MRI-guided use of neoadjuvant chemoradiotherapy• Need for autonomic nerve preservation• Sphincter preservation• “Experienced Surgeon”

10

Randomized TrialsSpecimen Quality
6% vs 12% LAR
11

Short – Term Outcomes
12

13

14Mizrahi I, et al. Role of Laparoscopy in Rectal Cancer: A Review. World J Gastroenterol 2014

15
Long – Term Results in Rectal Cancer
Lai JH, et al. Br Med Bull 2012

16Mizrahi I, et al. Role of Laparoscopy in Rectal Cancer: A Review. World J Gastroenterol 2014
Meta – Analyses of Oncological Outcomes (2006-2011)
17
N= 16 Clinical Trials3528 rectal CA patients
18
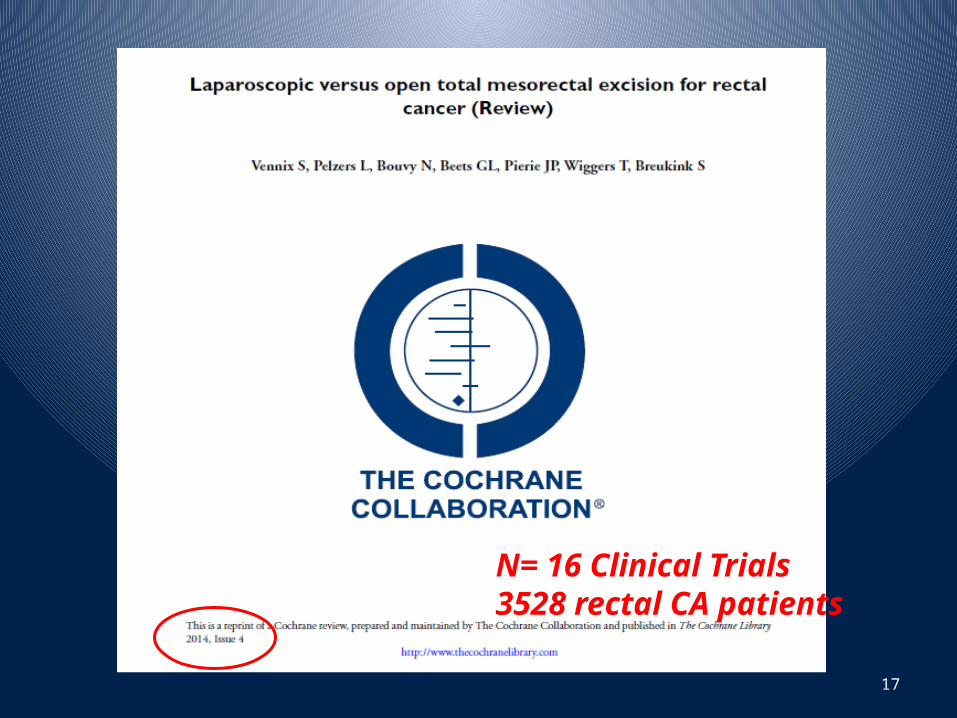
Disease – Free and Overall Survival

19
Local and Distant Recurrence
20
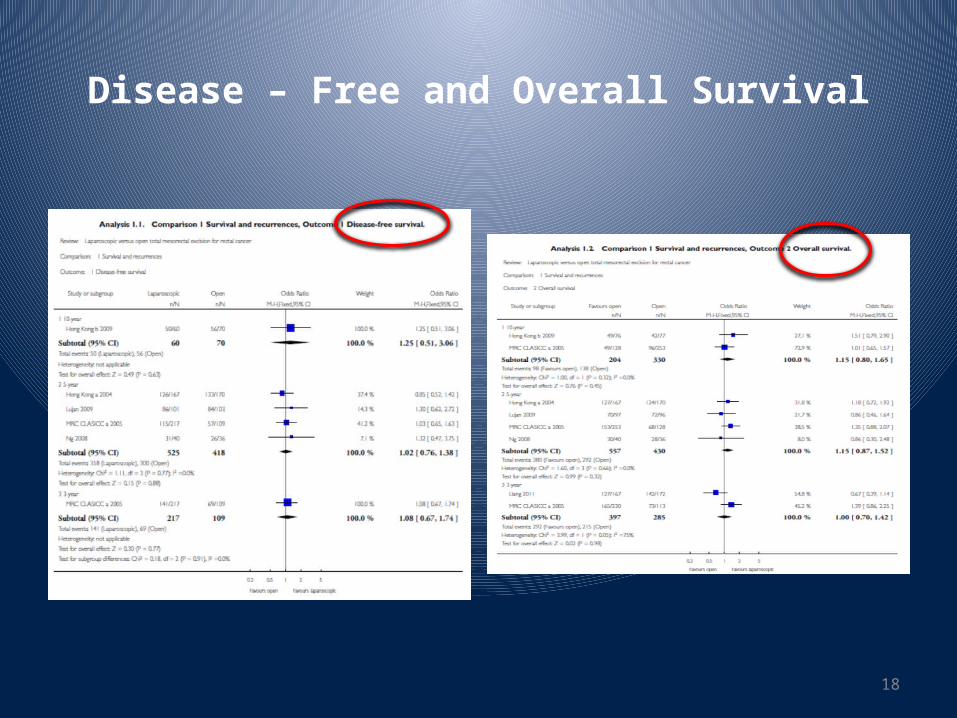
LNs Retrieved and CRM Positivity

21
Postoperative Pain and Hospital Stay

Post - Operative Complications
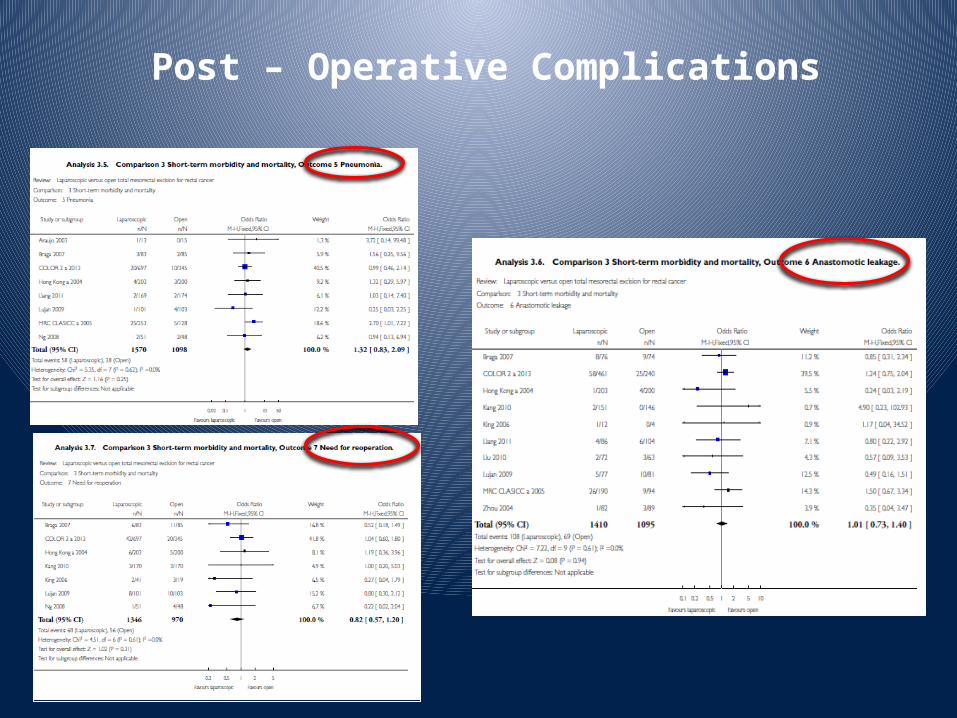
Post – Operative Complications

24

25

26

27BJS 2014; 101: 1272–1279

28
MRC CLASSIC:Financial Results
• Cost – intention to treat (mean)
Open Lap
• Theatre £ 1448 £ 1816• Hospital £ 3713 £ 3359• Others £ 2659
£ 3085
• Total £ 7820 £ 8260Br J Cancer 2006 95:6-12

Lap vs Open Surgery for Rectal CA - USA
• Local recurrence 2% Lap vs 4.2% Open (p=0.42)
Baik, Fleshman, DCR 2011
• Lap & HALS: Conversion 2.9%; LR 5%
Milsom, Sonoda, DCR 2009
• Laparoscopic 26 nodes; open 21. Otherwise identical outcomes
Boutros and Berho, DCR 2013
• Reduces cost $4283, cost-effective per QALY
Jensen and Abcarian, DCR 2012
29

Laparoscopic Resection for Rectal Cancer: What is the Evidence?
Dedrick Kok HC, et al. Biomed Res Int 2014
4 vs 5
30

Laparoscopic Resection for Rectal Cancer: What is the Evidence?
Dedrick Kok HC, et al. Biomed Res Int 2014
31

Open versus Laparoscopic surgery for mid-rectal or low-rectal cancer after
neoadjuvant chemoradiotherapy (COREAN trial): Survival Outcomes.
340 patients with locally advanced resectable rectal cancerIntention to treat analysisAll had neoadjuvant chemoradiotherapyLAP: 170 OPEN: 170
3-year Disease-Free Survival:
72·5% (95% CI 65·0–78·6) for the open surgery group 79·2% (72·3–84·6) for the laparoscopic surgery group
Jeong SY, et al. Gastrointestinal Cancer 201432

33

A Randomized Trial of Laparoscopic versus Open Surgery for Rectal Cancer
H. Jaap Bonjer, M.D., Ph.D, et al, for the COLOR II Study GroupN Engl J Med 2015; 372:1324-1332
• 30 hospitals 1044 patients• Rectal adenocarcinoma <15 cm from anal verge - no invasion• Intention to treat analysis 2:1• LAP 699 – OPEN 345• 3-yr RR L: 5% - O: 5%• 3-yr DFS L: 74.8% - O: 70.8%• 3-yr OS L: 86.7% - O: 83.6% NS• Laparoscopic surgery in patients with rectal cancer was associated
with rates of locoregional recurrence and disease-free and overall survival similar to those for open surgery.
34

35

36

37

Large Scale Ongoing RCTs
a. COLOR II trial in Europe
b. ACOSOG-Z6051 trial in the USA
c. JCOG 0404 trial in Japan
38

Conclusion
• Current data suggests that laparoscopic rectal cancer resection in experienced hands may benefit patients because of:
a. reduced blood loss
b. earlier return of bowel function
c. less postoperative pain
d. shorter hospital length of stay
• Short- and Long-term Oncological outcomes are, at least, equivalent with open surgery.
• There is a slight paucity of data concerning long-term outcome and conversion or other complications, such as bladder and sexual dysfunction after LAP TME.
39

40
“…is laparoscopy permitted for the curative
treatment of rectal cancer…?”
…but rather…
“…who should pursue laparoscopic
rectal cancer resections?…”