Laparoscopic radical right hemicolectomy for cecal cancer ...
Laparoscopic Colorectal Surgery
Part I. Colon Surgery
A.D’Hoore MD PhD, A. Wolthuis MD F. Penninckx MD,PhD
Department of abdominal SurgeryUniversity Hospital Leuven
Q. I personally performed
1. 0 laparoscopic colorectal resections
2. < 10
3. < 20
4. > 20

Q. my personal exposureduring training
1. 0 laparoscopic colorectal resections
2. < 20
3. < 50
4. > 50
Laparoscopic assistedright hemicolectomy Schlinkert RTDis Colon Rectum 1991 ; 34 : 1030 - 1031

A complex journeyfacilitated – gasless – hand assisted
later to medial , medial to lateral
Q. Laparoscopy for colonic cancer
1. Is still investigational ( performed in PRT )
2. Oncologic outcome beter than open
3. Same oncologic outcome but short-term outcome is better
4. Only a cosmetic benefit

Hazard Ratio : disease free survival at 3 years
Ration
Kuhry et aL. Lapsc. Surgery for colonic cancer - PhDThesis
Morbidity (meta-analysis)
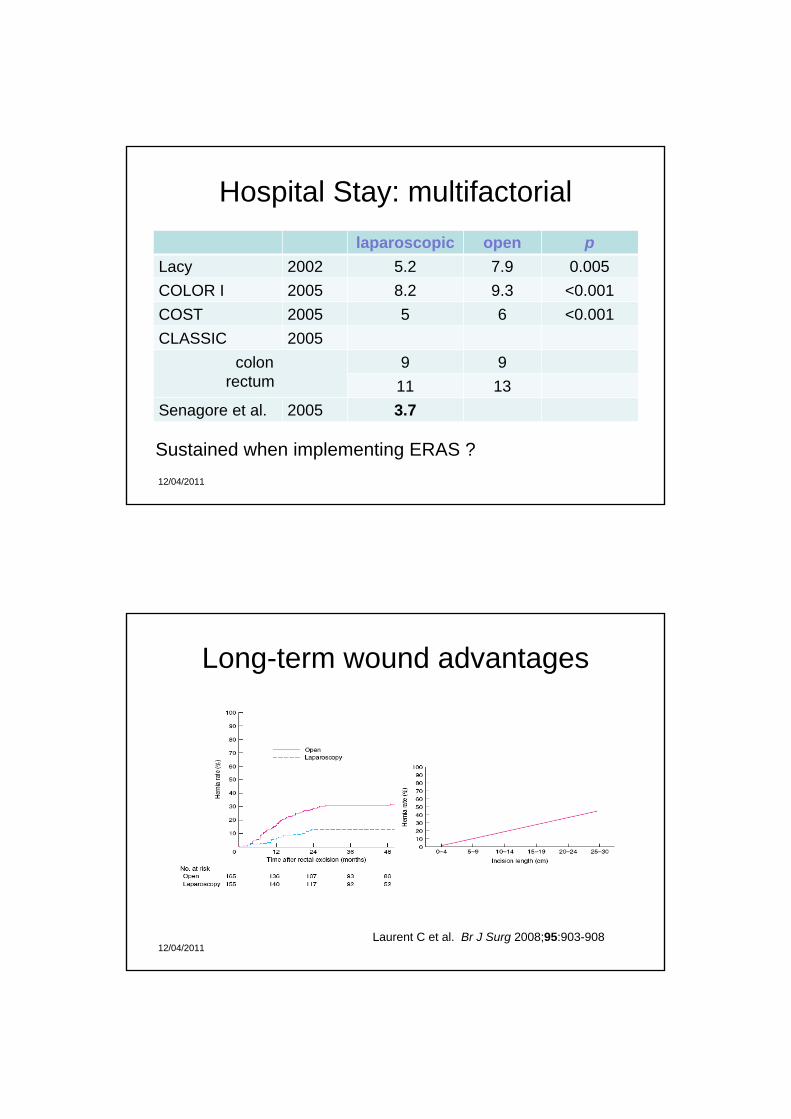
Hospital Stay: multifactoriallaparoscopic open p
Lacy 2002 5.2 7.9 0.005COLOR I 2005 8.2 9.3 <0.001COST 2005 5 6 <0.001CLASSIC 2005
colon rectum
9 911 13
Senagore et al. 2005 3.7
12/04/2011
Sustained when implementing ERAS ?
Long-term wound advantages
Laurent C et al. Br J Surg 2008;95:903-90812/04/2011
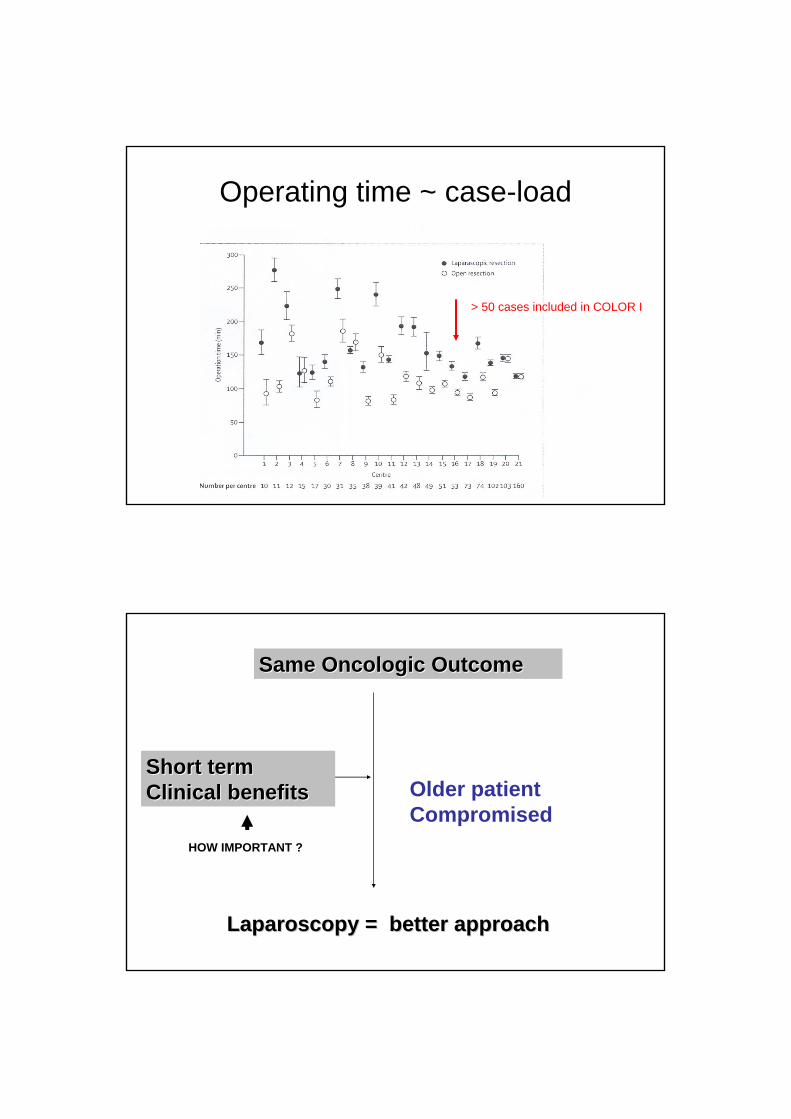
Operating time ~ case-load
> 50 cases included in COLOR I
Same Oncologic OutcomeSame Oncologic Outcome
Short termShort termClinical benefitsClinical benefits
Laparoscopy = better approachLaparoscopy = better approach
Older patientCompromised
HOW IMPORTANT ?

Port – site Metastasis : learning curve - effect
< 1995 : 0.6 – 21 %>1995 / n = 1.769 0.85 %recent n = 1.114 1 %
Called for a temporary moratorium ( 1994-1999)
Surgical Technique
1. Left colon- approach in benign disease- splenic flexure mobilisation- approach in cancer (cfr. rectal cancer)
2. Right colon- lap-assisted- approach in cancer

Laparoscopic colorectal surgery
Modified Lloyd – DavisArms along the bodyMoldable bean bag
Pelvic exposure
- Trendelenburg
- Temporary hysteropexy
° trans fundic° round ligament

Anatomical landmarks
Medial to Lateral approachThe left Colon
Final release
Laparoscopic approach medial to lateral

Diverticular disease
- Recurrent diverticulitis ( > 2 attacks )
- Internal fistulae (15%)
- Diagnostic doubt (ca)
- (recurrent bleeding)
Trend toward a more conservative approach

Common fistulas
-BladderFoley cathether 5-7 d
-Vagina
-Small bowel
resection margins in diverticular disease
Benn PL,Wolff BC,et al. Level of anastomosis and recurrent diverticulitis.Am J Surg 1986;269-271.
Wolff BC, Ready RL, MacCarty RL Dis Colon Rectum 1984;27:645-647
Importance distal resection margin : colo-rectal anastomosis12.5 % (distal sigmoid) vs 6.7 % rectum (p<0.03)
Proximal resection margin : no correlation with recurrence

Surgeon 1
Surgeon 2
TrendelenburgRight sided tilt
Pelvic diverticulitis

Vascular control
1. SRA -sparing
2. LCA - sparing
SRA-sparing vascular control
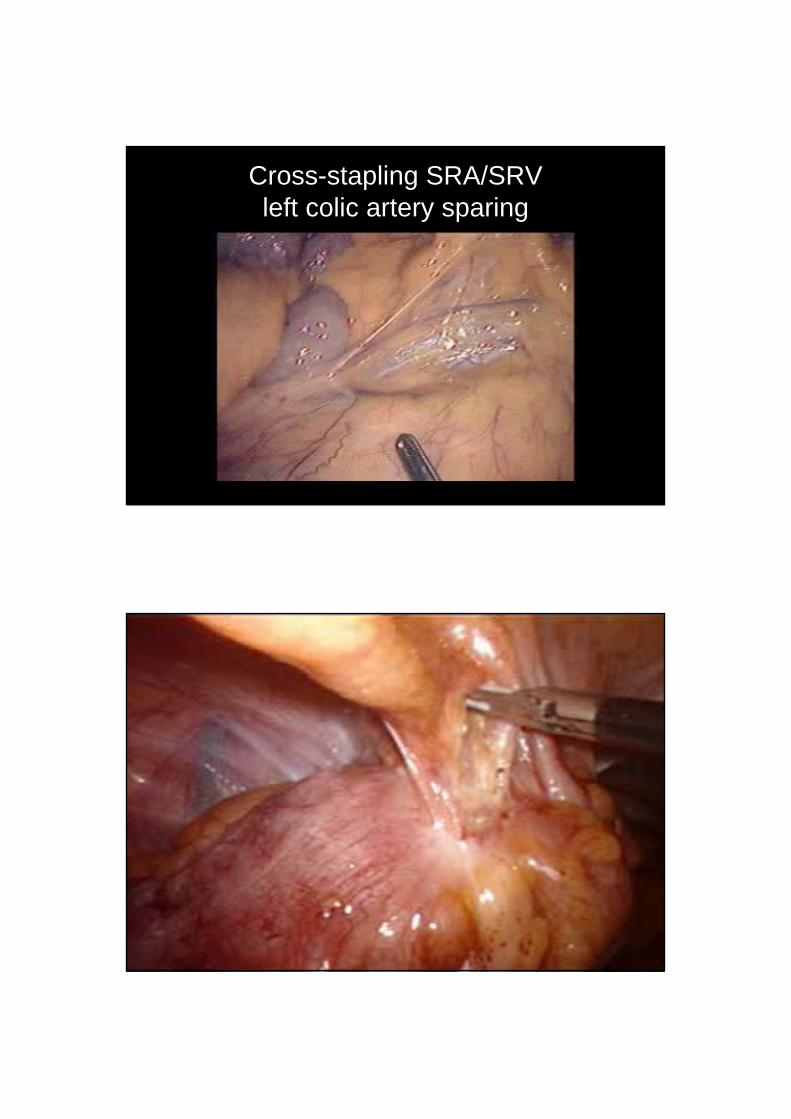
Cross-stapling SRA/SRV left colic artery sparing

double stapling (Knight & Griffen 1984)
double stapled anastomosis

difficulty : the high anastomosis
- Anastomosis on the rectum ? ( circular muscle coat)
- Further mobilize the rectum- Use the sizers to straighten the rectum (flatten Houston valves)- Insufflate the rectum - More distal recoupe- ( lateral anastomosis on the anterior aspect of the rectum )
Benign lesions: location
- RX Colon contrast
- Preoperative staining : not always accurate
- Peroperative colonoscopy : left colon


IMA – High Ligation
Surgeon 1 Surgeon 2
monitor
Trendelenburg
Right sided tilt

11
22
SRALCA

Splenic flexurePreserve arterial blood
Mobilisation Bowel
Release- lateral attachments (Toldt)- superior (splenocolic ligament)- omentum- adhesions lesser sac
Level of vascular ligation- high/low tie (left colic preservation)- high venous ligation

Griffith’s point
Sudeck’s point
Low tie + High venous ligation providesfull mobility

Surgeon 1
Surgeon 2
monitor
reversed – Trendelenburg
right sided tilt

Step I : exposure
- reversed Trendelenburg
- flip-over the omentum
- incision Treitz’s ligament
- first jejunal loop to the right

II. Ligation IMVOpening lesser sac
lateral to the middle colic vessels

III. omental release

predictable difficultiesfused mesentery transverse / descending colon / omentum
TCDC
Splenic flexure avoid medial to lateral dissection
“en bloc” exteriorization
disssection will eventuallyyeopardise blood supply DC

extraction
- Site- supra pubic - left flank- NOSE
- use a woud – protector- wound infections- tumour implants
Transrectal specimen retrieval ?
Akamatsu H et al. Surg Endosc. 2009 Mar 6. [Epub ahead of print]Totally laparoscopic sigmoid colectomy: a simple and safe technique for intracorporeal anastomosis.
12/04/2011

Surgery for Crohn’s disease
laparoscopic ileocaecal resection
stricture plasty
natural history of Crohn’s disease
Cosnes J et al. Inflamm Bowel Dis 2002;8(4):244-50Beaugerie et al. Gastroeneterology 2006;130:650-656
medical therapy
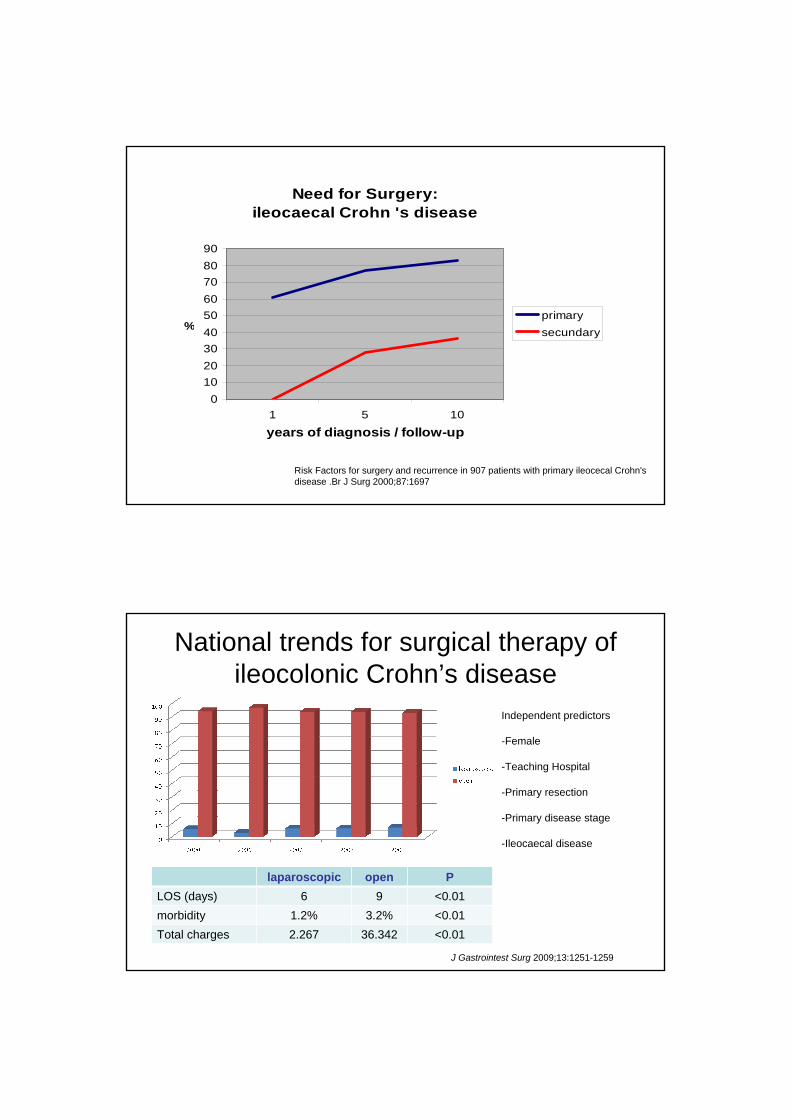
Need for Surgery:ileocaecal Crohn 's disease
0102030405060708090
1 5 10
years of diagnosis / follow-up
%primarysecundary
Risk Factors for surgery and recurrence in 907 patients with primary ileocecal Crohn's disease .Br J Surg 2000;87:1697
National trends for surgical therapy of ileocolonic Crohn’s disease
Independent predictors
-Female
-Teaching Hospital
-Primary resection
-Primary disease stage
-Ileocaecal disease
laparoscopic open PLOS (days) 6 9 <0.01morbidity 1.2% 3.2% <0.01Total charges 2.267 36.342 <0.01
J Gastrointest Surg 2009;13:1251-1259

Surgical technique = lapsc assisted
1. Complete SB – colonic exploration
2. Take down internal fistulae
3. Mobilisation Right Colon / terminal ileum
Vascular controlAnastomosis through Utility incision
Surgeon 2
Surgeon 1
monitor
TrendelenburgLeft sided tilt
Exploration – hepatic flexure
Dissection

associated surgery in 20 %
Lap.ass.[n=117] Open[n =125]
strictureplasty 7 pts [ 27 ] 3 pts [ 12 ] segm. enter. 6 3 sigmoid resection 5 anterior resection 4 wedge rectosigmoid wedge transverse wedge duodenum
9 1
9 1 1
CCE 1 drainage abscess 4 rectopexy 1

Ileosigmoidal fistula (10-15%)sensitivity of diagnostic tests
Melton G et al. Cleveland Clinic experience J Gastrointest Surg 2009;13:839-845
Colonoscopy (fistula) 11%Colonoscopy (fistula- erythema) 54%CT-scan (fistula) 41%CT-scan (indirect) 78%Fluoroscopic contrast 53%
Important information
1. State of the sigmoid
2. Anal stricture ?
3. Sphincters ?

SILS ileocaecal for complexe Crohn
Aspects of Quality in colonic ca resection
1. Margins
2. Integrity mesocolon
3. Vascular pedicle ligation
4. Extent lymphadenectomy

Arterial Supply determines resection margins
colonic flexure and transverse colon tumours
more complexe lymphatic drainage
Extended Right Hemicolectomy vs Left Hemicolectomy
middle colic vessels
excluded from randomised trials (COLOR I, COST)

meso-colic dissection
West NP, Lancet Oncol 2008; 9: 857-865
Supraduodenal window delineates
D2 resection
D3
D3

medial to lateral approach= ideal surgical strategy for cancer
1. Vascular ligation first (Turnbull ‘no-touch’)
2. Broad mesenteric dissection
3. Controls the retroperitoneum ureter, duodenum, autonomic nerves
4. Lateral attachments - tumor mobilisation last step
°1965, male

monitor
Surgeon 2
Surgeon 1optic
Ports for lapsc Right Hemicolectomy for cancer
stapler
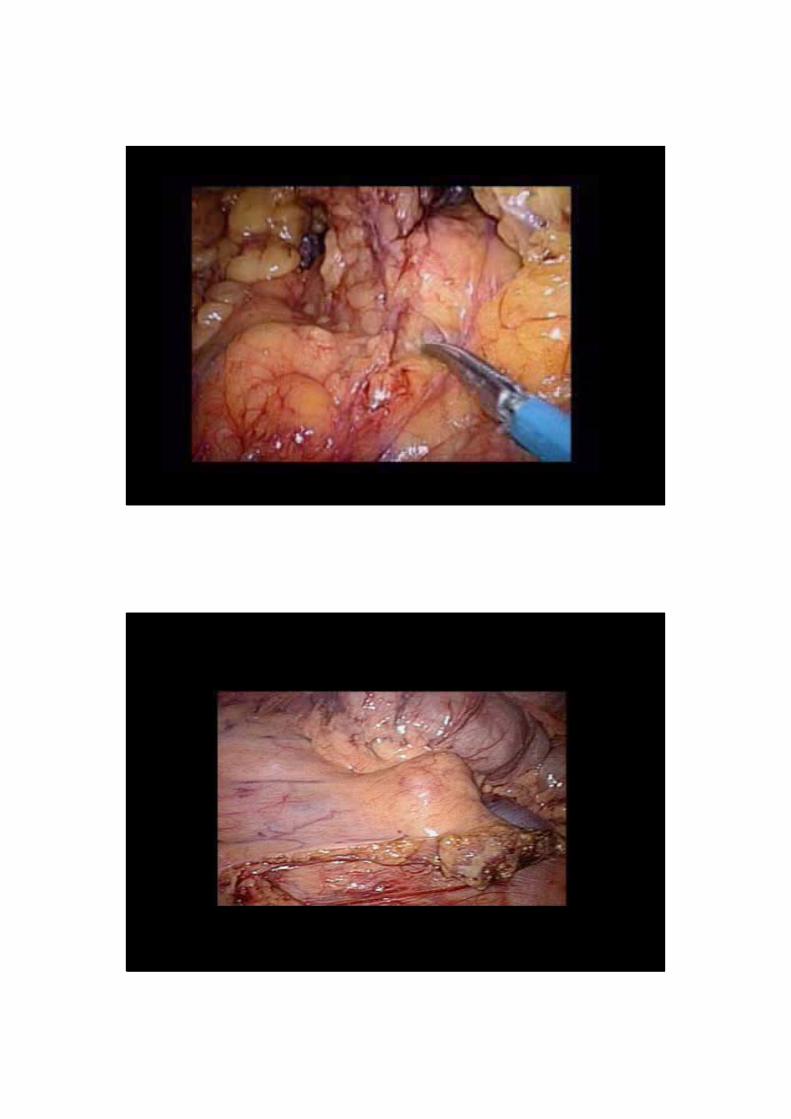
Submesocolic dissection

Difficulty : branches middle colics
- anatomic variability
- ‘troublesome’ venous bleeding
- exposure

VMSMCV
sGDVGEV
Henle venous confluens

Laparoscopic approach
SMV
gastro-epiploics

Anastomosis
1. Through extraction site
- manual
- stapled : functional end-to end ( Barcelona )
Caveat !!! : mesenteric twist
Close the mesenteric window ?

2. Laparoscopic anastomosis
Preop - perop assesment
OPEN expl LAPAROSCOPY
lapsc. assisted resection
5 %
conv :5 %
35-40%

Laparoscopyfor colorectal disease
is not the end of the futureSo, remain alert !
SILSTransrectal specimen delivery
The future will probably be far less invasive