
LABORATORY QUALITY CONTROL Course Code RIT 2.2 Revision C.
63
LABORATORY QUALITY CONTROL Course Code RIT 2.2 Revision C
-
Upload
adam-spencer-wilkinson -
Category
Documents
-
view
244 -
download
3
Transcript of LABORATORY QUALITY CONTROL Course Code RIT 2.2 Revision C.

LABORATORY QUALITY CONTROL
Course Code RIT 2.2 Revision C

Definitions:
• Quality Control:-
– the process of detecting errors
– the systems or procedures in place to avoid errors occurring
• Quality Assurance:-

… to ensure the reliability of the test results to give the best patient care !

Unreliable Performance ?
• Potential consequences include:-– patient misdiagnosis– delays in treatment– increased costs
• avoidable retests cost US 200million USD per year
• Even a small calibration bias can effect treatment rates:– 1% +ve bias in cholesterol result
5% increase in patients exceeding the treatment cut-off
– 3% +ve bias 15% increase in patient treatment.

Error Classification..
• Pre-analytical:-
– errors before the sample reaches the laboratory
• Analytical:-
– errors during the analysis of the sample
• Post-analytical:-
– errors occurring after the analysis

Pre - Analytical Errors..
• Improper preparation of the patient:-
– patient fasting
• glucose test
– stress and anxiety• urinary protein

Pre - Analytical Errors..
• Improper preparation of the patient• Improper collection of the blood
sample:-
– sample haemolysis• LDH, potassium or inorganic phosphate
– insufficient sample volume• unable to carry out all requested tests
– collection timing• 24 hour urine

Pre - Analytical Errors..
• Improper preparation of the patient• Improper collection of the blood
sample• Incorrect specimen container:-
– serum or plasma– fluoride tubes for glucose
• to inhibit glycolysis
– EDTA unsuitable anti-coagulant for calcium

• Improper preparation of the patient• Improper collection of the blood sample• Incorrect specimen container• Incorrect specimen storage:-
– sample left overnight at room temperature• falsely elevated K, Pi and red cell enzymes
– delay in sample delivery• falsely lowered levels of unstable analytes
Pre - Analytical Errors..

• The sex of the patient– male or female
• The age of the patient– new born / juvenile / adult / geriatric
• Dietary effects– low carbohydrate / fat– high protein / fat
• When the sample was taken– early morning urine collection pregnancy testing
• Patient posture– urinary protein in bed-ridden patients
Other Factors..

• Effects of exercise
– creatine kinase / CRP
• Medical history
– heart disease / diabetes / existing medication
• Pregnancy
– hormonal effects
• Effects of drugs and alcohol
– liver enzymes / dehydration
Other Factors..

• The sample:
Analytical Errors..
– labelling• barcoding / aliquoting
– preparation• centrifugation / aspiration
– storage temperature• short –term refrigeration• medium term freezing at –20oC• long term freezing at -80oC
– correct test selection• Laboratory Information Management System (LIMS)

• The sample:• Glassware / pipettes / balances:
Analytical Errors..
– used incorrectly– contaminated– poorly calibrated– reuse of pipette tips

• The sample:• Glassware / pipettes / balances:• Reagents / calibrators / controls:
Analytical Errors..
– poor quality– inappropriate storage
• correct temperature • badly maintained fridges or freezers
– stability• shelf-life / working reagent
– incorrect preparation

• The sample:• Glassware / pipettes / balances:• Reagents / calibrators / controls:• The application:
Analytical Errors..
– incorrect analytical procedures– poorly optimised instrument settings

• The sample:• Glassware / pipettes / balances:• Reagents / calibrators / controls:• The application:• The instrument:
Analytical Errors..
– operational limitations• temperature control/read times/mixing/carry-over
– lack of maintenance• worn tubing / optics / cuvettes / probes

Other Factors..• Calculation errors:
– incorrect factor / wrong calibration values
• Transcription errors:• Dilutions errors:
– incorrect dilution or dilution factor used
• Lack of training:• The human factor:
– tiredness / carelessness / stress

• The prompt and correct delivery of the correct report on the correct patient to the correct Doctor.
• How the Clinician interprets the data to the full benefit of the patient.
Post - Analytical Errors..

Accuracy ?
How correct your result is.

Precision ?
The reproducibility of your results.

Accurate and Precise..

Imprecise but Accurate !

Precise but Inaccurate !
Specificity ?
• The ability of a method to measure solely the component of interest.
• A lack of specificity will affect accuracy– falsely elevated values
• hormones and drugs
– falsely low values• BCP method with bovine albumin

• The ability to detect small quantities of a measured component.
Sensitivity ?
– will affect both precision and accuracy at the bottom end of the assay range.

Normal Distribution..
Values fall randomly about a mean value.
Fre
qu
en
cy
Measured value
Mean value (x)

Precision ?
• How disperse the values are.
• Quantified by measuring the Standard Deviation (SD) of the set of results.

Standard Deviation (SD)..
The lower the SD the better the Precision.
)1-n
x)-(xi ( = SD
2

Example:
Mean result (x) = 100 mmol/L
Standard deviation (SD) = 1.0 mmol/L
Number of results (n) = 100

Mean +/- 1SD..
Values fall randomly about a mean value.
Fre
qu
en
cy
x-1SD +1SD
99 100 101
68%

Mean +/- 2SD..
Values fall randomly about a mean value.
Fre
qu
en
cy
x-2SD +2SD
98 100 102
95%

Which is more Precise ?
Potassium SD = 0.1 mmol/L
Sodium SD = 2.0 mmol/L

Coefficient of Variation..
A %CV takes into consideration the magnitude of the overall result.
100% x (x) Mean
SD = CV

Example:
Sodium has the better CV and in this example is performing better
than potassium.
Potassium %CV = (0.1 / 5.0) x 100% = 2.0%
Sodium %CV = (2.0 / 140) x 100% = 1.4%

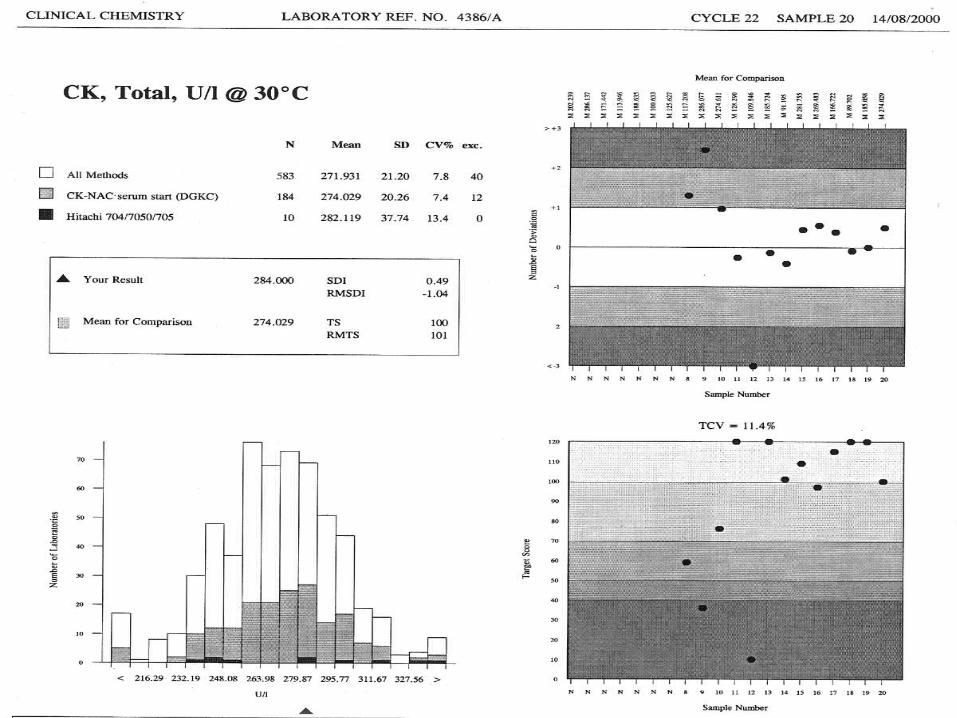
Interpretation..
10 40 unacceptable performance 41 50 need for improvement 51 70 acceptable 71 100 good101 120 excellent

TS Calculations
V = (Result - Mean for Comparison) x 100
Mean for Comparison
The mean for comparison could be either:
– the all method mean
– your method mean
– your instrument mean

TS = Log10 (3.16 x TCV) x 100
V
TCV is Target Coefficient of Variation
TS Calculations

3.16 is selected as a constant because:– the log10 of 3.16 is 0.5
– so if V = TCV, then the target score will be 50
TS Calculations
TS = Log10 (3.16 x TCV) x 100
V

TS = log10 3.16 x TCV x 100 V
= log10 3.16 x 3.7 x 100 3.7
= log10 (3.16) x 100
= 50

How can Analytical Quality be
Controlled ?

• Internal Quality Control (IQC).– daily monitoring of quality control sera
• External Quality Assessment (EQA).– comparing of performance to other laboratories.

Internal Quality Control..
• Daily monitoring – precision – accuracy
• Quality control sera– results within control limits indicates
that analytical system is running satisfactorily

What is Acceptable ?
A sodium control has a target value of 140 mmol/L
139 mmol/L
140 mmol/L
141 mmol/L
120 mmol/L
160 mmol/L
180 mmol/L

What is Acceptable ?
• A range of acceptable values is established
• Sodium Control:- 137 143mmol/L.

What are the Options ?• Unassayed serum:
– the cheaper option !• but the laboratory must establish its own ranges
– cannot be used to assess accuracy !• no externally assigned target values
• Assayed serum:– with predetermined targets and ranges
• established by the manufacturer.

Unassayed Serum..
• Analysed extensively by the laboratory. – a minimum of 20 sets of data generated– a mean +/- 2SD range established
• 95% of results acceptable
– some laboratories may adopt tighter ranges

Assayed Serum..
• Targets and ranges generated by the manufacturer:– utilises RIQAS
• database of 5,000 laboratories• method / instrument / temperature specific values


Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
X
XX
X
X
X
X
X
X
X
X
X
X
X
X
X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
XX
X
X
X
X
XX
X
X
X
X
X
X
X
X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
X
XX
X
X
X
X
X
X
XX
X
X
XX
X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
X
X
XX
X
X
XX
X
XX
X
X
XX
X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
X
XX
X X
X
X
XX
XX
XX
X
X X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
X
X
X
X
X
X
X
X
X
X
X
X
X
XX
X
X

Levey Jennings Chart
-2SD
-1SD
Mean
+1SD
+2SD
140
137
138.5
141.5
143
XX
X
X
X
X
XX
X
XX
X
X
XX
XX

Westgard Rules..
• Decision criteria is dependent on the precision of the method or analyser– the less precise the method the more
difficult the decision.
• Westgard provides multiple QC rules:-– defines acceptability
• minimises false rejections• maintains high error detection

Westgard Flowchart..Control data
1 point
outside 2 SD
1 point
outside 3 SD
2 consecutive
values outside
the same 2 SD
Difference between
2 controls within
a run
exceeds 4 SD
4 consecutive control
values on one side
of the mean and
further than
1 SD from the mean
10 consecutive
values
on one side of
the mean
In control – report data
Out of control – reject analytical run
Yes
Yes
No
No
No NoNo No
YesYes
YesYes

External Quality Assessment..
.. the main objective of EQA is not to bring about day to day consistency but to establish inter-laboratory
comparability

EQA Options..• International / National / Regional
• International schemes provide:-– a larger database of results– a wider range of analytical methods– a global representation of diagnostic
manufacturers
• Compulsory or Voluntary

A Typical EQA Scheme..
• Participants receive unknown samples.– these are analysed ‘blind’– the results returned to scheme
organiser– they are statistically analysed– to generate a comparative report – report sent to participant

RIQAS•
International Quality Assessment Scheme– launched in 1988– 5000 participants
• Management tool– to assess, review and improve performance

RIQAS..• Annual subscription
– two six monthly cycles
• Weekly samples– one vial reconstituted per week
– tested blind as if a patient sample
• Results reported back to – statistically analysed
• Weekly Report generated




![First Revision No. 34-NFPA 450-2014 [ Section No. 2.2 ]](https://static.fdocuments.net/doc/165x107/62944781c3b38c06595402b3/first-revision-no-34-nfpa-450-2014-section-no-22-.jpg)



![Second Revision No. 11-NFPA 30-2013 [ Section No. 2.2 ]€¦ · · 2013-08-14Second Revision No. 11-NFPA 30-2013 [ Section No. 2.2 ] ... NFPA 96, Standard for Ventilation Control](https://static.fdocuments.net/doc/165x107/5b053b107f8b9abf568b62fc/second-revision-no-11-nfpa-30-2013-section-no-22-2013-08-14second-revision.jpg)

![First Revision No. 49-NFPA 17A-2015 [ Detail ]€¦ · First Revision No. 12-NFPA 17A-2015 [ Section No. 2.2 ] 2.2 NFPA Publications. National Fire Protection Association, 1 Batterymarch](https://static.fdocuments.net/doc/165x107/5f81326cfdb6e6131b21892d/first-revision-no-49-nfpa-17a-2015-detail-first-revision-no-12-nfpa-17a-2015.jpg)




![Second Revision No. 11-NFPA 302-2013 [ Section No. … Revision No. 11-NFPA 302-2013 [ Section No. 2.2 ] 2.2 NFPA Publications. National Fire Protection Association, 1 Batterymarch](https://static.fdocuments.net/doc/165x107/5b0b2f5a7f8b9a45518d94cc/second-revision-no-11-nfpa-302-2013-section-no-revision-no-11-nfpa-302-2013.jpg)

