
Laboratory Challenges in Screening and Monitoring of...
61
Transcript of Laboratory Challenges in Screening and Monitoring of...


Ch ll i L b tChallenges in Laboratory Tests for CKD
Hassan Argani
Professor of NephrologyProfessor of Nephrology,
Shahid Beheshti University of Medical Sciences

ddIntroductionIntroduction
ChallengeChallenge‐‐11: Who should be screened for CKD: Who should be screened for CKD
ChallengeChallenge‐‐22: Which method is better for : Which method is better for ggscreening and follow up for CKDscreening and follow up for CKD
ChallengeChallenge‐‐33: The biases of each method: The biases of each method

ddIntroductionIntroduction
ChallengeChallenge‐‐11: Who should be screened for CKD: Who should be screened for CKD
ChallengeChallenge‐‐22: Which method is better for : Which method is better for ggscreening and follow up for CKDscreening and follow up for CKD
ChallengeChallenge‐‐33: The biases of each method: The biases of each method

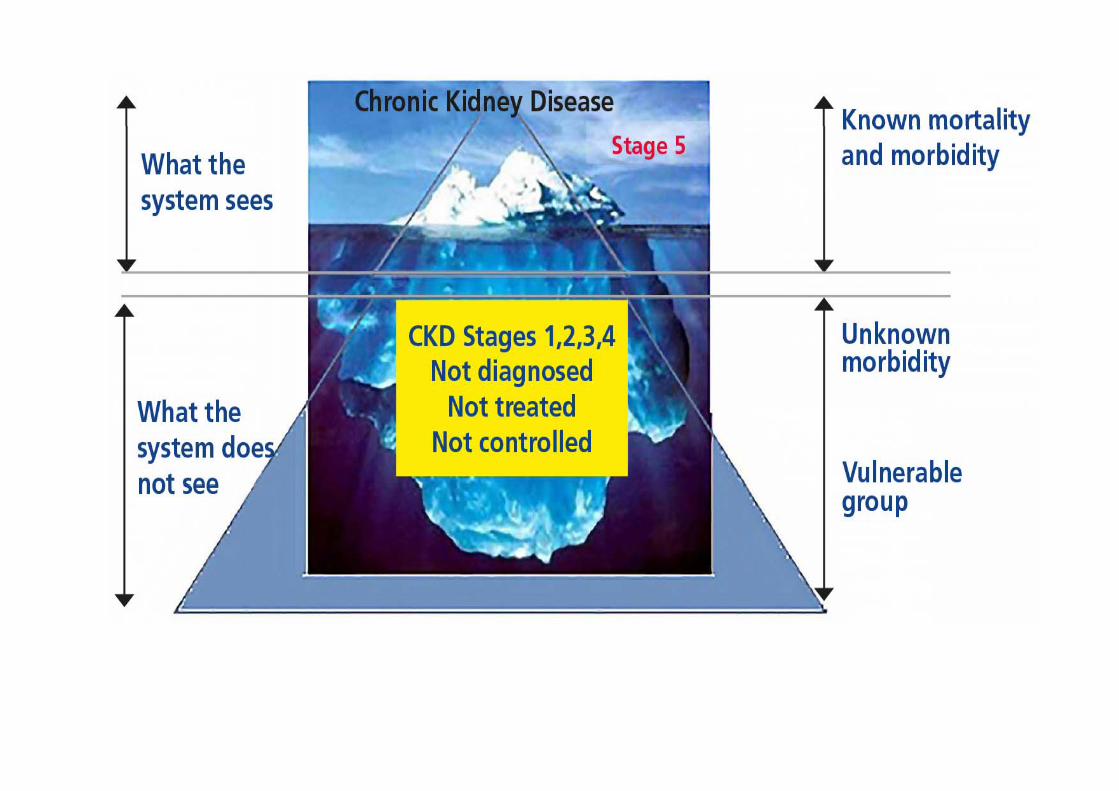
Revised chronic kidney disease classification based upon glomerular filtration rate and albuminuria
GFR stages GFR(mL/min/1.73 m2) Terms
G1 >90 Normal or highgG2 60 to 89 Mildly decreasedG3a 45 to 59 Mildly to moderately decreasedG3b 30 44 M d l l d dG3b 30 to 44 Moderately to severely decreasedG4 15 to 29 Severely decreased
G5 <15 Kidney failure (add D if treated by dialysis)G5 <15 Kidney failure (add D if treated by dialysis)
Albuminuria stages
AER(mg/day) Terms
A1 <30 Normal to mildly increased (may be subdivided for risk prediction)
A2 30 to 300 Moderately increased
A3 >300Severely increased (may be subdivided into nephrotic and non‐nephrotic for differential diagnosis, management, and risk prediction)g , g , p )


ddIntroductionIntroduction
ChallengeChallenge‐‐11: Who should be screened for CKD: Who should be screened for CKD
ChallengeChallenge‐‐22: Which method is better for : Which method is better for ggscreening and follow up for CKDscreening and follow up for CKD
ChallengeChallenge‐‐33: The biases of each method: The biases of each method

Who needs screening for CKD?The ACP recommendations,
October 2013The ASN in response to the ACP recommendations
Asymptomatic adults without risk f f CKD h ld b
CKD screening even in patients i h i k f f CKDfactors for CKD should not be
screened for the disease (Grade: weak recommendation, low‐quality
without risk factors for CKD
weak recommendation, low quality evidence
Adults with or without diabetes Disagreed. Present or absent who are currently taking an angiotensin‐converting enzyme (ACE) inhibitor or an angiotensin II
Diabetes in adults taking an ACE inhibitor or an ARB, should be tested for proteinuria (G d k(ACE) inhibitor or an angiotensin II‐
receptor blocker (ARB) should not be tested for proteinuria (Grade:
tested for proteinuria (Grade: weak recommendation, low‐quality evidence)
be tested for proteinuria (Grade: weak recommendation, low‐quality evidence)

Flowchart for diagnosing CKD
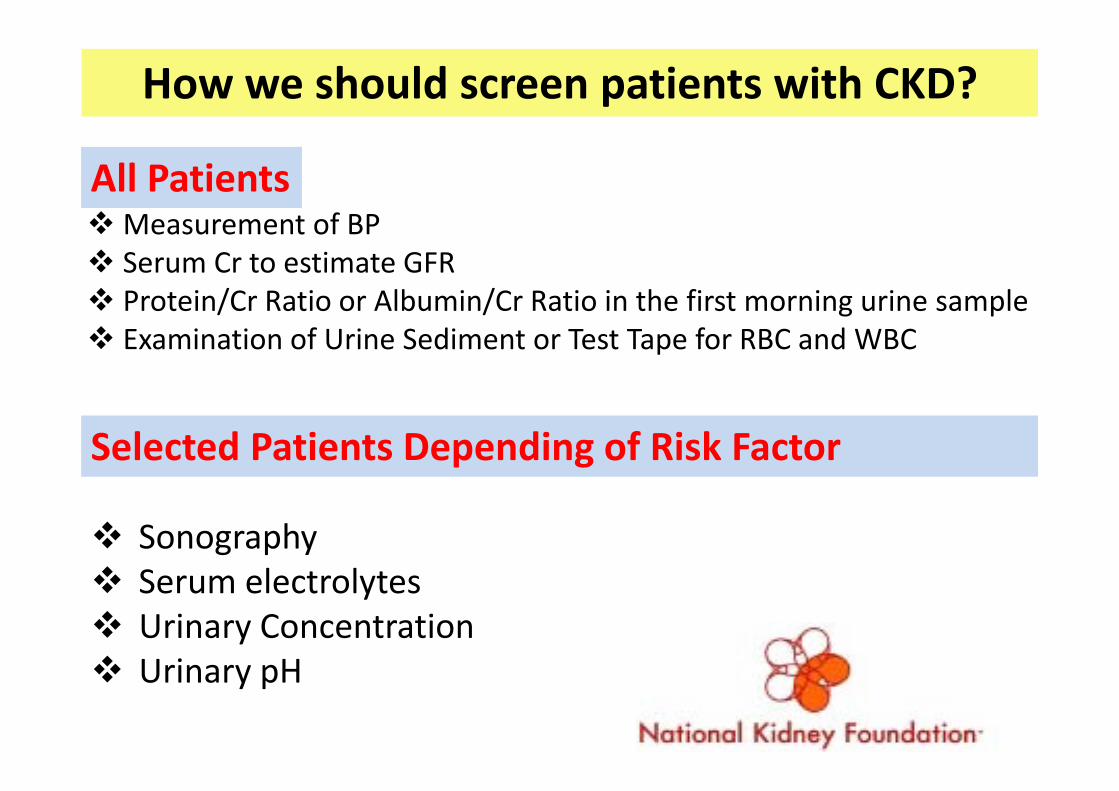
How we should screen patients with CKD?
M t f BPAll PatientsMeasurement of BP Serum Cr to estimate GFR Protein/Cr Ratio or Albumin/Cr Ratio in the first morning urine sample Protein/Cr Ratio or Albumin/Cr Ratio in the first morning urine sample Examination of Urine Sediment or Test Tape for RBC and WBC
Selected Patients Depending of Risk Factor
Sonography S l t l t Serum electrolytes Urinary Concentration Urinar pH Urinary pH

Diagnostic Evaluation in Chronic Kidney Disease-1
CLINICAL URINE PROTEIN/CRDISORDER
CLINICAL CLUES
URINE SEDIMENT
PROTEIN/CR RATIO ADDITIONAL TESTS
Diabetes mellitus Diabetes for > 15 years,
Benign > 30 to > 3,500 mg of protein
Fasting blood sugar, A1C
retinopathy per g of creatinine
Essential hypertension
LVH, retinopathy
Benign > 30 to 3,000 mg of protein per
No additional testshypertension retinopathy of protein per
gram of creatinine
Glomerulonephritis History and Dysmorphic > 30 to > 3,500 C3 and C4 for all physical examination: infections; rash arthritis;
RBCs or RBC casts
mg of protein per g of creatinine
patientsTests for infections: anti-ASO, ASK, HIV, HBsAg, HCV RPR bloodrash, arthritis;
Old ageHCV, RPR, blood culturesTests if there is rash or arthritis: ANA, ANCA, cryoglobulin, anti-GBMTests if patient is older than 40 years: SPEP, UPEPUPEP

Diagnostic Evaluation in Chronic Kidney Disease-2URINE PROTEIN/CR
DISORDER CLINICAL CLUES SEDIMENT RATIO ADDITIONAL TESTSLow flow
statesVolume depletion,
hypotension, ti h t
Hyaline casts, eosinophils
< 200 mg of protein per g of creatinine
FENa: < 1 percent;
congestive heart failure, cirrhosis, atherosclerosis
Urinary tract Urinary symptoms Benign, or None KUB radiography,Urinary tract obstruction
Urinary symptoms Benign, or RBCs
None KUB radiography, intravenous
pyelography, spiral CT scanning, renal lt hultrasonography
Chronic urinary tract
infection
Urinary symptoms WBCs, RBCs < 2,000 mg of protein per g of creatinine
Pelvic examination, urine culture, voiding cystourethrography,infection cystourethrography,
renal ultrasonography, CT scanning
Neoplasm, Old ages, RBCs, RBC False-negative result SPEP, UPEP, calcium Sparaproteine
miaconstitutional
symptoms, anemiacasts,
granular castsor > 30 to > 3,500 mg
of protein per g of creatinine
level, ESR
Interstitial Medications fever WBCs WBC 30 to 3 000 mg of ACE level; SS–A SS–BInterstitial nephritis
Medications, fever, rash, eosinophilia
WBCs, WBC casts,
eosinophils
30 to 3,000 mg of protein per g of
creatinine
ACE level; SS A, SS Beosinophilia

Diagnostic Evaluation in Chronic Kidney Disease-3URINE
SEDIME PROTEIN/CRDISORDER CLINICAL CLUES
SEDIMENT
PROTEIN/CRRATIO ADDITIONAL TESTS
Cystic kidney disease
Palpable kidneys with or without
RBCs 30 to 3,000 mg of protein per g of
Renal ultrasonography or CT scanning if there isdisease with or without
family history of cystic kidney disease, flank pain
protein per g of creatinine
or CT scanning if there is a complex kidney cyst or mass
Renovascular disease
Late-onset or refractory hypertension, sudden onset of
Benign < 200 mg of protein per g of creatinine
Renal Doppler ultrasonography, radioisotope renal scanning MRA renalsudden onset of
hypertension in young woman, smoking history,
scanning, MRA, renal angiography
abdominal bruitVasculitis Constitutionalsympt
oms, peripheral neuropathy rash
RBCs; granular casts
> 30 to > 3,500 mg of protein per g of creatinine
C3, C4, ANA, ANCA; HBsAg, HCV, cryoglobulins ESR RFneuropathy, rash,
respiratory symptoms
casts creatinine cryoglobulins, ESR, RF, SS–A, SS–B, HIV

Screening for Complications in CKD(Stages 3 and 4*)
TEST COMPLICATIONS DETECTEDHemoglobin concentration Anemia
Red blood cell indexes, reticulocyte count, iron studies, fecal occult
blood test
For ruling out other causes of anemia before erythropoietin
therapy is startedblood test therapy is started
Serum electrolyte levels Hyperkalemia, hyponatremia, id iacidosis
Calcium, phosphorus, and parathyroid hormone levels
Hypocalcemia, hyperphosphatemia secondaryparathyroid hormone levels hyperphosphatemia, secondary
hyperparathyroidism
Serum albumin and total protein Hypoalbuminemia decreasedSerum albumin and total protein levels
Hypoalbuminemia, decreased levels of immunoglobulins in
patients with nephritic levels of p pproteinuria or signs of
malnutrition

Evaluation of Intrinsic Renal Failure
Glomerular Vascular Interstitial
RBC castUrinalysis RBC cast,OFB, fatty cast RBC cast None
24 h protein24‐h protein excretion
(g/d/1.73 m2)>3.5 1‐5 <2
Hypertension 50% 75% RareHypertension 50% 75% Rare

ddIntroductionIntroduction
ChallengeChallenge‐‐11: Who should be screened for CKD: Who should be screened for CKD
ChallengeChallenge‐‐22: Which method is better for : Which method is better for ggscreening and follow up for CKDscreening and follow up for CKD
ChallengeChallenge‐‐33: The biases of each method: The biases of each method

Minimal initial diagnostic tests for patients with CKD
• Estimation of GFRMinimal initial diagnostic tests for patients with CKD
• Urinalysis• Quantification of proteinuria Quantification of proteinuria• Renal ultrasound
Additional diagnostic tests, depending on the clinical situation
• Serologies for autoimmune diseases• Serologies for chronic infections (hepatitis B and C, HIV, and others)g f f ( p , , )• Serum and urine protein electrophoresis and immunofixation• Blood and urine cultures
d f l• Imaging studies for malignancy• Kidney biopsy??

Minimal initial diagnostic tests for patients with CKD
• Estimation of GFRMinimal initial diagnostic tests for patients with CKD
• Urinalysis• Quantification of proteinuria Quantification of proteinuria• Renal ultrasound
Additional diagnostic tests, depending on the clinical situation
• Serologies for autoimmune diseases• Serologies for chronic infections (hepatitis B and C, HIV, and others)g f f ( p , , )• Serum and urine protein electrophoresis and immunofixation• Blood and urine cultures
d f l• Imaging studies for malignancy• Kidney biopsy??

Minimal initial diagnostic tests for patients with CKD
• Estimation of GFRMinimal initial diagnostic tests for patients with CKD
• Urinalysis• Quantification of proteinuria Quantification of proteinuria• Renal ultrasound
Additional diagnostic tests, depending on the clinical situation
• Serologies for autoimmune diseases• Serologies for chronic infections (hepatitis B and C, HIV, and others)g f f ( p , , )• Serum and urine protein electrophoresis and immunofixation• Blood and urine cultures
d f l• Imaging studies for malignancy• Kidney biopsy??

Sensitivity and specificity of each equation to Diagnosis and classify patients with CKDDiagnosis and classify patients with CKD
‐EPI
CG: Cockcroft‐Gault equation; CGi: Cockcroft‐Gault equation (calculated with ideal weight); CKD‐EPI: the Chronic Kidney Disease Epidemiology Collaboration equation; CrCl: Creatinine l MCQ M Cli i Q d i E i MDRD i lifi d MDRD d iclearance; MCQ: Mayo Clinic Quadratic Equation; sMDRD: simplified MDRD study equation.

Preferred Methods for Assessing Kidney FunctionMETHOD SITUATIONS FOR USE
MDRD study equation for estimating GFR
Patients with diabetic kidney disease
Patients with chronic kidney disease in middle age (average age: 51 years)middle-age (average age: 51 years)
Black patients with hypertensive chronic kidney diseasekidney disease
Patients with a kidney transplant
Cockcroft Gault equation for Older patients (performs better than theCockcroft-Gault equation for estimating creatinine clearance
Older patients (performs better than the MDRD study equation)
24-hour urine collection for Pregnant womencreatinine clearance Patients with extremes of age and weight
Patients with malnutritionPatients with skeletal muscle diseases
Patients with paraplegia or quadriplegia
Patients with a vegetarian diet and rapidly changing kidney function

Formulas to Estimate Creatinine Clearance as an Estimate of GFR
Cockroft‐Gault formula (mL/minute) (Cockroft, 1976):
([140−Age] × [IBW])/(72×SCr)× 0.85 if female.the CG formula overestimates the measured GFR at levels lower 60 mL/min/1.73 m2.
The modified MDRD formula , 2000
GFR=175×Cr−1.154×Age−0.203×1.212(for black)×0.742(for women)the MDRD underestimates the measured GFR at levels above 60 mL/min/1.73 m2.
Males: IBW= 50kg+0.9 kg/Cm over 150 cm
F l IBW 45 5k 9 k /C 150Females: IBW= 45.5kg+o.9 kg/Cm over 150 cm

The formulas for estimating creatinine clearance for children
Schwartz Formula 1976:GFR 0 55 h i h ( )/ i i ( /dL)GFR=0.55× height(cm)/serum creatinine(mg/dL)
Counahan‐Barrett Formula 1976:Counahan‐Barrett Formula 1976:GFR=40× height(cm)/serum creatinine(μmol/L)
Modified Schwartz Formula in 2009:GFR(mL/min/1.73m2)=39.1[height(m)/Cr(mg/dL)]0.516×[1.8/cystatin C( /L)] 0 294[30/BUN( /dL)]0 169[1 099] l [h i ht( )/1 4]0 188C(mg/L)] 0.294[30/BUN(mg/dL)]0.169[1.099]male[height(m)/1.4]0.188
Most recently, a new formula, known as the CKD‐EPI (Chronic Kidney Disease Epidemiology Collaboration) equation, was reported to give improved performance over the widely used MDRD equation.



ddIntroductionIntroduction
ChallengeChallenge‐‐11: Who should be screened for CKD: Who should be screened for CKD
ChallengeChallenge‐‐22: Which method is better for : Which method is better for ggscreening and follow up for CKDscreening and follow up for CKD
ChallengeChallenge‐‐33: The biases of each method: The biases of each method


TionsInfection,D i t i tiDrug intoxicationDehydrationObstructionSevere hypertensionSevere hypertension
1.5mg/dL


Cr production in male (mg/Kg)=Cr production in male (mg/Kg)=2828‐‐00..2 2 ageage
Cr production in Cr production in female female (mg/Kg)=(mg/Kg)=2323..88‐‐00..17 17 ageage


Common causes of false estimates of elevated creatinine

Urea as Measure of Renal Function
Urea is the main waste product of nitrogen‐containing chemicals in the body.the body.
It has a molecular weight of 60 Da.
The concentration of urea is expressed only by the nitrogen t t fcontent of urea.
Each molecule of urea contains 2 nitrogen atoms, the molecular Each molecule of urea contains 2 nitrogen atoms, the molecular weight of urea nitrogen is 28 Da.
Serum urea is widely used as a measure of renal dysfunction, but its value as a measure of GFR is not very good for several reasons.

Causes of Prerenal Azotemia
Low cardiac output• Acute myocardial infarction• Chronic heart failure• Valvular heart disease• Valvular heart disease• Diarrhea• Vomiting
Decreasedplasma volume
• Sweating• Nasogastric suction• Burns• Diuretics
Decreasedhemoglobin levels • Bleedinghemoglobin levels
Endocrinedysfunction
• Uncontrolled diabetes mellitus(polyuria) • Diabetes insipidusdysfunction • Addison disease
Renal dysfunction • Salt‐wasting nephropathy• S i dVasodilation • Sepsis syndrome• Endotoxemia
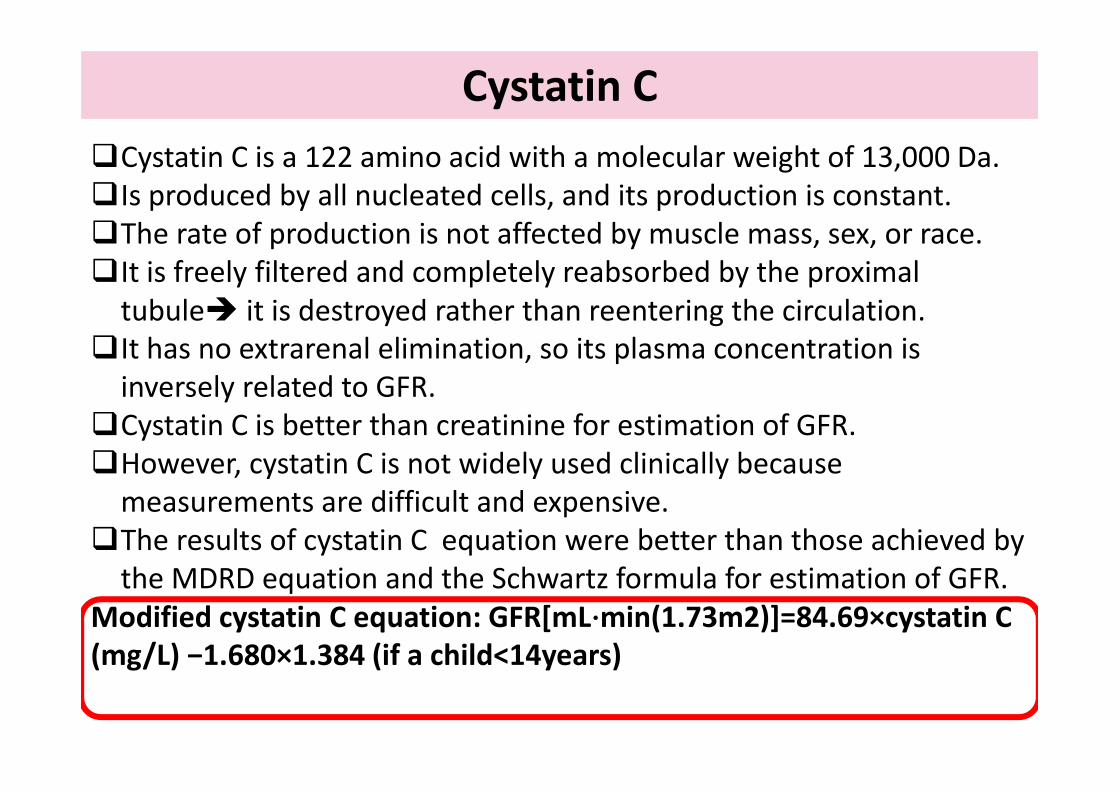
Cystatin CCystatin C is a 122 amino acid with a molecular weight of 13,000 Da.Is produced by all nucleated cells, and its production is constant. The rate of production is not affected by muscle mass, sex, or race.It is freely filtered and completely reabsorbed by the proximal tubule it is destroyed rather than reentering the circulationtubule it is destroyed rather than reentering the circulation.
It has no extrarenal elimination, so its plasma concentration is inversely related to GFR.inversely related to GFR.
Cystatin C is better than creatinine for estimation of GFR. However, cystatin C is not widely used clinically because measurements are difficult and expensive.
The results of cystatin C equation were better than those achieved by the MDRD equation and the Schwartz formula for estimation of GFRthe MDRD equation and the Schwartz formula for estimation of GFR.
Modified cystatin C equation: GFR[mL⋅min(1.73m2)]=84.69×cystatin C (mg/L) −1.680×1.384 (if a child<14years)(mg/ ) .680 .384 (if a child 4years)

Level of Cystatin C is alteredIncreased Level Decreased Level
Hyperthyroidism HypothyroidismHyperthyroidism Hypothyroidism
Peripheral arterial diseases Glucocorticostroidsb l d h lMetabolic syndrome Atherosclerosis
Alzheimer Aorta AneurysmCigarette smoking
CHF MI StrokeCHF, MI, Stroke
Malignancy
HIV infection
Increased CRPIncreased CRP


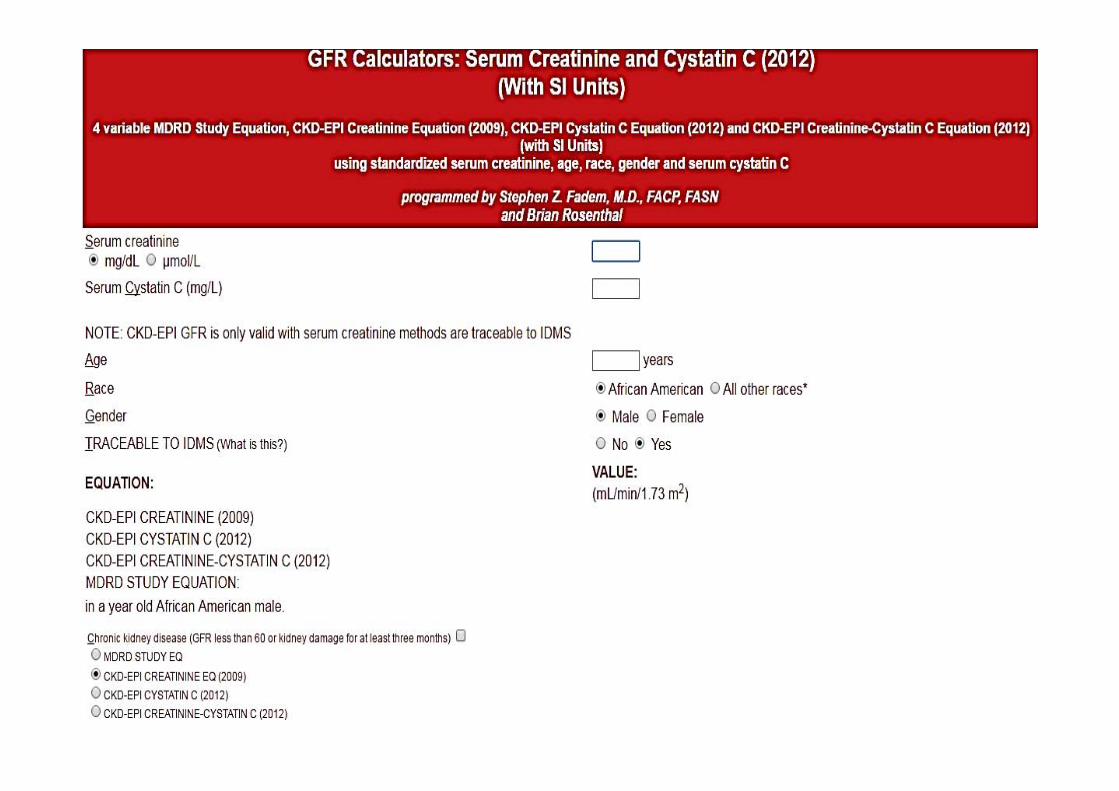

Methods for GFR Estimation

Equations developed by the MDRD Study Group and CKD‐EPI, based on serum Cr.
Filtration Marker
eGFR Research Group
Number of
Assays Equation
Advantages References
CKD EPI, based on serum Cr.
subjectsMDRD Study 1628
CKDNon-
standardizedMDRD Study
ti i
Recommended by NKF-KDOQI
2002
Levey et al. Ann
I t M dcreatinine 1999
2002 Intern Med 1999; 130:
461-70;MDRD Study Same as Re-expressed MDRD Appropriate for Levey et y
abovepfor
standardized assay
Study creatinin
e 2006
pp puse with
standardized assays
yal. Ann
Intern Med 2006; 145:
247-54
CKD-EPI 12,150 Standardized CKD-EPI creatinin
Lesser bias ateGFR >60.
Levey et al. Ann Int
e 2009 Recommended by KDIGO 2013
Med 2009; 150: 604-
12

Equations developed by the MDRD Study Group and CKD‐EPI, based on serum Cystatin‐C
Filtration Marker
eGFR Research Group
Number of
subjects
Assays Equation Advantages References
CKD EPI, based on serum Cystatin C
subjects
CKD-EPI CKD3418
Non-standardized
CKD-EPI cystatin C
2008
eGFRcr-cys more precise
Stevens et al. Am J
Kidney Dis CKD-EPI
creatinine-cystatin C
2008
than eGFRcroreGFR cys
2008; 51:395-406
CKD-EPI Same as above
Re-expressed for standardized
assay
CKD-EPI cystatin C
2011CKD-EPI
Appropriate for use with standardize
d assays
Inker et al. Am J Kidney Dis 2011; 58:
682-684CKD-EPI creatinine-cystatin C
2011
d assays 682-684
CKD-EPI Diverse6471
Standardized CKD-EPI cystatin C
2012CKD-EPI
Lesser bias ateGFR >60.Recommend
ed by
Inker et al. N Engl J
Med 2012; 367: 20-9
creatinine-cystatin C
2012
yKDIGO 2013

β‐2‐Microglobulin
β ‐2‐microglobulin, a polypeptide with molecular weight of 11.6 kDaand length of 99 amino acidsand length of 99 amino acids.
Is a component of the MHA class I molecule.It is present in all nucleated cells, and is needed for production ofIt is present in all nucleated cells, and is needed for production of CD8 cells.
Its production is increased in multiple myeloma and lymphoma. β‐2 microglobulin is freely filtered at the glomerulus, and then is reabsorbed and metabolized completely by the proximal tubule.
Similar to cystatin C the plasma level increases in renal failureSimilar to cystatin C the plasma level increases in renal failure. The protein appears in the urine when reabsorption is incomplete because of proximal tubular damage, as in acute kidney injury. p g , y j y

β Trace Protein
BTP is a low molecular weight glycoprotein with 168 amino acids. The molecular weight varies between 23 000 and 29 000 DaThe molecular weight varies between 23 000 and 29 000 Da, depending on the degree of glycosylation.
BTP belongs to the lipocalin protein family and functions as prostaglandin D synthase.
Plasma BTP originates from the brain and is freely filtered at the l l th i b b d l t l b th i l t b lglomerulus, then is reabsorbed completely by the proximal tubule and is catabolized there.
The plasma level is increased in patients with renal disease because ofThe plasma level is increased in patients with renal disease because of reduced filtration in the presence of constant production.
Estimated GFR by B Trace Protein is better than those obtained by the MDRD equation and serum cystatin C measurements. However, others showed that BTP was less sensitive than cystatin C.
GFR=112.1×BTP−0.662×urea−0.280×(0.880 if female)

Tryptophan Glycoconjugate
Is a substance normally produced in the body by glycoconjugation of tryptophan.
It is filtered at the glomerulus freely and is not reabsorbed. A strong linear correlation exists between clearances of TG and inulin. TG increases progressively with declining renal function but unlike TG increases progressively with declining renal function, but unlike
creatinine, it is not affected by muscle mass. The current limitation: it can be measured only by the HPLC. The current limitation: it can be measured only by the HPLC. It is not known whether dietary intake of tryptophan affects the
serum concentration.

The soluble urokinase‐type plasminogen activator receptor
The soluble urokinase‐type plasminogen activator receptor (suPAR) may be a marker of CKDmay be a marker of CKD.
suPAR is a membrane protein that has been implicated in the p ppathogenesis of glomerular diseases including focal segmental glomerulosclerosis (FSGS) and diabetic nephropathy.

Minimal initial diagnostic tests for patients with CKD
• Estimation of GFRMinimal initial diagnostic tests for patients with CKD
• Urinalysis• Quantification of proteinuria Quantification of proteinuria• Renal ultrasound
Additional diagnostic tests, depending on the clinical situation
• Serologies for autoimmune diseases• Serologies for chronic infections (hepatitis B and C, HIV, and others)g f f ( p , , )• Serum and urine protein electrophoresis and immunofixation• Blood and urine cultures
d f l• Imaging studies for malignancy• Kidney biopsy??

C l it f U i t tC l it f U i t tComplexity of Urinary testComplexity of Urinary test
CollectionCollectionStorage AnalysisAnalysis


APPEARANCE CAUSEMilky Acid urine: urate crystals
Alk li i i l bl
APPEARANCE CAUSEOrange Drugs: anthraquinones
(l ti ) if i iAlkaline urine: insoluble phosphatesInfection: pus
(laxatives), rifampicin
UrobilinogenuriaYellow Mepacrine
SpermatozoaChyluria
Smoky pink Hematuria (>0.54 mL blood/L
pConjugated bilirubinPhenacetinRib fl iurine)
Foamy ProteinuriaBlue or green Pseudomonas urinary tract
RiboflavinBrown or black Melanin (on standing)
Myoglobin (on standing)g yinfectionBilirubinMethylene blue
y g ( g)Alkaptonuria
Green or black PhenolL lMethylene blue
Pink or red Aniline dyes in sweetsPorphyrins (on standing)Blood hemoglobin myoglobin
LysolBrown Drugs: phenazopyridine,
furazolidone, l ‐dopa, Blood, hemoglobin, myoglobinDrugs: phenindione, phenolphthaleinA th i i (b t t
niridazole
Hemoglobin and myoglobin (on standing)Anthocyaninuria (beetroot,
“beeturia”)
( g)
Bilirubin

The main causes of false negative and positive testing from use of urine dipsticksp
Discounting contamination from menstrual – or other – bleeding, and exercise induced haematuria and proteinuriaexercise‐induced haematuria and proteinuria

Urinary protein Urinary protein excretion of < 150 mg/day is normal (~30
mg of this is albumin and about 70 100 mg is Tamm
y pmg of this is albumin and about 70–100 mg is Tamm‐Horsfall (muco)protein, derived from the proximal renal tubule)tubule).
Protein excretion can rise transiently with fever, acute illness UTI and orthostaticallyillness, UTI and orthostatically.
In pregnancy, the upper limit of normal protein excretion is around 300 mg/dayaround 300 mg/day.
Persistent elevation of albumin excretion (microalbuminuria) and other proteins can indicate renal(microalbuminuria) and other proteins can indicate renal or systemic illness.

Microalbuminuria is an early sign of renal and cardiovascularMicroalbuminuria is an early sign of renal and cardiovasculardysfunction with adverse prognostic significance.

AMAM
PM

Albuminuria in the Detection of Renal Lesions
• Method of measurement (of choice): albumin/creatinine ratio (mg/g creatinine)
• Definition of albuminuria: >30 mg/g in spot urine sample
Gi t i bilit 2 t f 3 iti d d 3 6• Given measurement variability, 2 out of 3 positive measures are needed over 3‐6 months to consider it pathologic
• Valid samples: first morning, mid‐morning and mid‐afternoon urine samples
• Situations that increase albuminuria: intense physical exercise, fever, infection, Situations that increase albuminuria: intense physical exercise, fever, infection, heart failure, hyperglycemic decompensation
• False positives: hematuria pyuria highly concentrated urine• False positives: hematuria, pyuria, highly concentrated urine
• Less accurate albumin/creatinine ratio in extreme values of creatinine: overestimated in reduced muscle mass and underestimated in muscular patients

The main causes of differently colored urine

Microscopic haematuria isMicroscopic haematuria is present in around 4% of
the adultl ti f h tpopulation – of whom at
least 50% have glomerular disease

ConclusionConclusion

Summary of screening Summary of screening recommendationsrecommendations for CKDfor CKD
Screen four groups of Use two tests for g ppatients with screening
Diabetes Urine albumin to creatinine ratio in 2 to 3 spot urine
Hypertension p
samples (mg/g)
Cardiovascular disease Serum creatinine and eGFR
Age over 55 yr



![superficial mycoses2 [Read-Only]iacld.ir/DL/workshop/superficialmycosesdrhashemi.pdf · Superficial MycosesSuperficial Mycoses PityriasisversicolorPityriasis versicolor Pityrosporosis](https://static.fdocuments.net/doc/165x107/5f0fe88d7e708231d4467c62/superficial-mycoses2-read-onlyiacldirdlworkshopsuperfi-superficial-mycosessuperficial.jpg)






![Mycology - Dr. Hashemi.ppt - iacld.ir · A yeastA yeast--like dematiaceus fungus, ... Erythrasma Definition: ... Mycology - Dr. Hashemi.ppt [Compatibility Mode] Author: bathaei](https://static.fdocuments.net/doc/165x107/5ad803fa7f8b9ab8378cd5eb/mycology-dr-iacldir-yeasta-yeast-like-dematiaceus-fungus-erythrasma.jpg)






