Lab Values Relevant to the Radiologist - Nova Scotia...
34
Lab Values Relevant to the Radiologist Gillian Shiau Swiped from Jim Henson’s Muppets
Transcript of Lab Values Relevant to the Radiologist - Nova Scotia...

Lab Values Relevant to the
RadiologistGillian Shiau
Swiped from Jim Henson’s Muppets

Disclosures
• Nothing to disclose

Outline1) Coagulation:
• High-level review of the clotting cascade
• Review of commonly encountered anticoagulants and antiplatelet agents and hemostatic agents
• Review of guidelines for percutaneous image-guided procedures
2) Renal function:
• Review of creatinine and GFR calculations
• Classic teaching regarding contrast-induced nephropathy (CIN)
• Emerging evidence on CIN
• Management of renal functionhttp://www.arizonatransplantassociates.com/
http://myhomegarden.xyz/

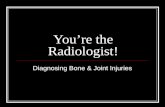
Recall the Coagulation Cascade…
Oral anticoagulants for Asian patients with atrial fibrillation Sabir I et al. Nature Reviews Cardiology 11, 290–
303 (2014) doi:10.1038/nrcardio.2014.22
*Measured using PT/INR
*Measured using PTT

Coagulopathy Workup
• INR: 0.9-1.1– Reflects the extrinsic pathway (I, II, V, VII, X)
– Elevated if on PO anticoagulant therapy;
– Liver dysfunction – synthesis of Vitamin K dependent II, VII, IX, and X; also proteins C and S)
– Also elevated if: Vit K deficiency; lupus anticoagulants; DIC, bile duct obstruction, malabsorption, malnutrition)
• aPTT: 25-35s– Reflects intrinsic pathway (VIII, IX, XI, XII)
– Elevated if on heparin (usu 1.5-2.5 times for therapeutic)
– Also elevated if: liver disease, DIC, Vit K deficiency, use of therapeutic anticoagulants (eg. hirudin, argatroban)
• CBC:– Hgb: 135-170g/L (also can look at MCV: normal 83-98fL)
– Platelets: 150-450 x 109/L (beware HIT – heparin induced thrombocytopenia)
• TT: < 20s

Commonly Used Anticoagulants Agent Half-Life Test Reversal Agent
Warfarin 40 hours INR FFP
Unfractionated
heparin
1.5 hrs aPTT Protamine (1mg/100IU)
LMWH (Lovenox,
Enoxaparin)
4.5-7 hours Anti-Xa Incomplete. Protamine – can
repeat ½ dose PRN
LMWH (Dalteparin,
Fragmin)
2.5 hrs Anti-Xa Incomplete. Protamine – can
repeat ½ dose PRN
LMWH (Tinzaparin,
INNOHEP)
3-4 hrs Anti-Xa Incomplete. Protamine – can
repeat ½ dose PRN
Fondaparinux
(Arixtra)
17 hrs Anti-Xa None. Consider recombinant
factor VIIa
Bivalirudin
(Angiomax)
25 minutes aPTT None. Consider recombinant
factor VIIa
Argatroban 45 minutes aPTT None. Consider recombinant
factor VIIa
Cook. Anticoagulation Management. Semin Intervent Radiol. 2010 Dec; 27(4): 360–367. doi: 10.1055/s-0030-1267849

Anticoagulants – Warfarin
• Oral vitamin K antagonist
• MOA: affects clotting factors II, VII, IX, X and proteins C and S
• t1/2 of 37hrs but dependent on amount of circulating clotting factors – II – prothrombin is most important with t1/2 of 96hrs;
– VII has shortest t1/2 of 6 hrs
• Monitored using INR
• Indications: afib; DVT/PE; hypercoagulable states; mechanical heart valves
• Antithrombotic effect: delayed onset and transient HYPERcoagulability � heparinization indicated when initiating treatment
http://www.phassociation.uk.com/treatment_for_ph/warfarin.php
St Jude Medical. http://www.mechanicalheartvalve.co.uk/

Anticoagulants – WarfarinTime til procedure Reversal Management
> 5 days Hold warfarin x 5 days
1-5 days Hold warfarin; check INR 24hrs preprocedure
1 day Hold warfarin, check INR
- If INR > 1.9 � 2 mg vit K PO
- If INR 1.5-1.9 � 1 mg vit K PO
< 24hrs or emergent Hold warfarin; check INR
- If INR > 3 � FFP and consider factor concentrates
- If INR 1.5-3 � 2 units of FFP and recheck INR
Cook. Anticoagulation Management. Semin Intervent Radiol. 2010 Dec; 27(4): 360–367. doi: 10.1055/s-0030-1267849

Anticoagulants – Heparin (UFH)
• IV or subcutaneous medication of mixture of large and small heparin fractions
• MOA: forms complex with antithrombin (III) which inhibits activation of factors II and X
• t1/2 of 60-90minutes (nonlinear)
• Monitored using aPTT (full anticoagulation = 1.5-2.5x normal); can use ACT (activated clotting time, normal <150s)
• Reversal agent – protamine t1/2 7 minutes (1mg neutralizes ~100units heparin)– Only need to reverse last 1-2 hrs (d/t short t1/2 of heparin)
– Beware of inducing bradycardia and hypotension (avoid by slow administration)
• Complications: – HIT (4-5% incidence; develops day 5-14 of continuous
therapy)
– Osteoporosis (up to 15% incidence; develops if on long-term therapy)

Anticoagulants – Heparin (LMWH)
• Multiple formulations (enoxaparin; tinzaparin; dalteparin; nadroparin) derived from UFH – uniform size
• MOA – forms complex with antithrombin (III) which inhibits activation of thrombin – *reduced bridging of antithrombin �
inhibition of other factors is more important than with UFH (aPTTunderestimates the anticoagulation d/t LMWH)
• t1/2 is ~4x that of UFH (~4.5hrs)
• Reversal – protamine (less effective and predictable than with UFH) – can give an additional half dose PRN
• Complications: reduced incidence of HIT and osteopenia
Enoxaparain training. Iyer BK.

Anticoagulants – Direct Thrombin
Inhibitors • Aptly named – directly inhibit thrombin
• Bivalent (Hirudin; bivalirudin; lepirudin) – binds at active site and exosite 1
• Univalent (Argatroban) – binds only at active site
• Does not require monitoring (only test could do would be a clotting time)
• Indication: contraindication to heparin (eg. HIT)
• Reversal: no specific agent – factor concentrates and recombinant factors induce partial reversal

New Kid on the Block: Dabigatran• Also known as Pradaxa
• MOA: directly inhibits both free and clot-bound thrombin; renally cleared
• Indications: VTE prevention; afib pts for prevention of stroke and systemic arterial thromboembolism
• Monitoring: INR and PTT relatively insensitive (often normal); thrombin time is quite sensitive
• Reversal: studies in progress. Early studies show that Idarucizumab complete rerversethe anticoagulant effects within minutes (in Clinical Trials)

New Kids on the Block: Direct Xa
Inhibitors• Rivaroxaban (Xarelto); Apixaban
• Rivaroxaban: – ~50% hepatically cleared; and 66% excreted in urine
– Indications: VTE prevention in ortho pts; afib pts for prevention of stroke and systemic arterial thromboembolism; also approved for acute tx and secondary prevention of DVT and PE
• Apixaban: – Metabolized by CYP3A4; partly eliminated by kidneys
• Reversal strategies: NO agent currently (some synthetic molecules in the works – Andexanet alpha and aripazine) Laulicht2012.

Antiplatelet – Aspirin
• MOA: inhibits platelet cyclooxygenase (enzyme that contributes to production of thromboxane A2), thereby inhibiting platelet aggregation and activation
• Platelet lifespan is 10days so withholding x 5 days �30-50% of platelets will have normal function
• Indication: coronary artery disease
The Awkard Yeti

Antiplatelet – Thienopyridines• Multiple formulations: clopidogrel, ticlopidine,
prasugrel
• MOA: inhibit adenosine diphosphate (ADP) dependent binding to platelet receptors �inhibit activation of glycoprotein Iib/IIIa
• Duration of action – lifespane of platelet (7-10days) but effective t1/2 is ~4 hours
• Reversal: partial restoration of hemostatic function if administer exogenous platelets 6-8 hours post last dose as newly transfused platelets do not undergo inhibition

Antiplatelets – NSAIDs • Nonsteroidal antiinflammatory
drugs – usually do not cause significant problems unless patient has underlying coagulopathy
• MOA: inhibit platelet aggregation
• Reversal: reversible – decays with clearance from blood (specific NSAID dependent for duration)
• *Paradoxical: diminish antiplatelet effect of ASA if given concomitantly
http://rccatalyst.com/?p=26277

Antiplatelets – Glycoprotein IIb/IIIa
Inhibitors • Abciximab; eptifibatide; tirofiban
• MOA: antagonist to integrin complex glycoprotein IIb/IIIa found on platelets inhibiting platelet aggregation
• Reversal: specific formulation dependent
– Abciximab – stop 24hrs preprocedure (at least 12 hrs)
– Tirofiban – can stop at moment of incision without increased bleeding risk

Hemostatic Agents
• FFP– contains plasma proteins (including coagulation factors) – effects are variable d/t vitamin K
dependent clotting factors (sometimes need to concomitantly use vitamin K)
• Platelets– Fractionated blood product dose in increments of 4-6 units
• Protamine– Rapid onsent within 10 minutes of administration with SHORT half life � paradoxic” repeat
anticoagulation after protamine administration
– Side effects: bradycardia; hypotension; pulmonary arterial hypertension; decreased O2 consumption; anaphylactoid
• Vitamin K– If stable, elective case, PO (5-10mg) administration preferred
– IV administration associated w/ risk of anaphylactoid reaction
• Cryoprecipitate– Used if acquired or hereditary deficiency of fibrinogen
• Recombinant Factor VIIa– Used in hemophilia patients + factor VIII inhibitors OR non-hemophilia patients with SEVERE
bleeding and acute trauma
• Desmopressin– Synthetic analogu of ADH – unclear MOA to enhance plasma levels of factor VIII and vWF
(dosed at 0.3µg/k IV diluted in 100cc of NS in a 20-30 minute infusion)
– Side effects: mild hyponatremia; tachyphylaxis. Case reports: vascular thrombosis, MI

Guidelines for Anticoagulation Rx Pre-
Procedure – LOW RISK• If LOW risk of bleeding that is EASILY DETECTED AND CONTROLLABLE:
• Vascular procedures: – dialysis access; venography; central line removal; IVC filter placement; PICC line insertion
• Nonvascular procedures: – Drainage catheters exchange (biliary, nephrostomy, abscess); thora-/paracentesis; superficial aspiration and
bx (excluding intrathoracic/intraabdominal) such as thyroid, superficial LNs; superficial abscess drainage
• Preprocedure labs: – INR (if on warfarin; liver dz) – if > 2.0 � tx with FFP, Vit K
– PTT (if on IV unfractionated heparin) – NO CONSENSUS
– Plts (NOT recommended) – trx if < 50
– Hct (NOT recommended) – no threshold for trx
• Medications:– Warfarin: withhold 3-5days (want INR < 2.0)
– ASA: do NOT withhold
– Heparin: check the PTT
– LMWH( therapeutic dose): withhold ONE DOSE pre-procedure
– Fondaparinux: do NOT withhold
– Plavix: withhold x 5 days pre-procedure
– Ticlopidine: withhold for 0-5days pre-procedure
– NSAIDs (short, intermediate and long-acting): do NOT withhold
– Direct thrombin inhibitors (Argatroban; Angiomax; Dabigatran): do NOT withhold
Patel et al. Consensus Guidelines for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous Image-guided
Interventions. CIRSE. J Vasc Interv Radiol 2012; 23:727–736. DOI: 10.1016/j.jvir.2012.02.012; Addendum of Newer Anticoagulants to the
Conesnsus Guidelines. J Vasc Interv Radiol 2013; 24:641-645. DOI: 10.1016/j.jvir.2012.02.012

Guidelines for Anticoagulation Rx Pre-
Procedure – MODERATE RISK• If MODERATE risk of bleeding
• Vascular procedures: – Angiography; arterial interventions with access up to 7French; venous interventions; chemoembolization; UFEs; transjugular
liver bx; tunneled CVC; subcutaneous port insertion
• Nonvascular procedures: – Intraabdominal, chest wall, or retroperitoneal abscess drainage or bx; lung bx, transabdominal liver bx (core); perc chole;
gastrostomy tube insertion; RFA (straightforward); spine procedures (vertebroplasty, kyphoplasty, LP, epidural injections; facet blocks)
• Preprocedure labs: – INR (recommended): correct to < 1.5
– PTT: recommended if on IV unfractionated heparin: NO CONSENSUS but trend with 73% consensus for correcting if > 1.5x control)
– Plts (NOT recommended) – trx if < 50
– Hct (NOT recommended) – no threshold for trx
• Medications:– Warfarin: withhold for 5days (INR < 1.5)
– ASA: do NOT withhold
– Heparin: check the PTT – trend towards correcting if > 1.5x control
– LMWH( therapeutic dose): withhold ONE dose or 12 hours pre-procedure
– Fondaparinux: withhold (2-3days if Cr > 50cc/min; 3-5 days if < 50cc/min)
– Plavix: withhold x 5 days pre-procedure
– Ticlopidine: withhold x 7days pre-procedure
– NSAIDs (short, intermediate and long-acting): do NOT withhold
– Direct thrombin inhibitors (Argatroban; Angiomax; Dabigatran): defer procedure until medication is off; • If emergent � withhold Argatroban x 4 hrs preprocedure
• if emergent and Cr Cl > 50cc/min � wait 2-3 hours for Angiomax; 2-3days for Dabigatran
• if emergent and Cr Cl > 50cc/min � wait 3-5 hours for Angiomax; 3-5days for Dabigatran
Patel et al. Consensus Guidelines for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous Image-guided
Interventions. CIRSE. J Vasc Interv Radiol 2012; 23:727–736. DOI: 10.1016/j.jvir.2012.02.012; Addendum of Newer Anticoagulants to the
Conesnsus Guidelines. J Vasc Interv Radiol 2013; 24:641-645. DOI: 10.1016/j.jvir.2012.02.012

Guidelines for Anticoagulation Rx Pre-
Procedure – HIGH RISK• If SIGNIFICANT risk of bleeding (could be DIFFICULT TO DETECT OR CONTROL):
• Vascular procedures: – TIPS
• Nonvascular procedures: – Renal bx; biliary interventions (new); nephrostomy tube placement; RFA (complex)
• Preprocedure labs: – INR (recommended) – if > 2.0 � tx with FFP, Vit K
– PTT (recommended on IV unfractionated heparin) – stop or reverse heparin values if > 1.5x control)
– Plts (IS recommended) – trx if < 50
– Hct (IS recommended) – no threshold for trx
• Medications:– Warfarin: withhold for 5days (INR < 1.5)
– ASA: withhold 5 days preprocedure
– Heparin: withhold 2-4hrs preprocedure (want aPTT < 1.5x control)
– LMWH( therapeutic dose): withhold TWO doses or 24 hours pre-procedure
– Fondaparinux: withhold (2-3days if Cr > 50cc/min; 3-5 days if < 50cc/min)
– Plavix: withhold x 5 days pre-procedure
– Ticlopidine: withhold x 7days pre-procedure
– NSAIDs: withhold short-acting (t1/2 2-6hrs) x 24 hrs; intermediate acting (t1/2 7-15hrs) x 2-3days; long-acting (t1/2 > 20hrs) x 10days
– Direct thrombin inhibitors (Argatroban; Angiomax; Dabigatran): defer procedure until medication is off; • If emergent � withhold Argatroban x 4 hrs preprocedure
• if emergent and Cr Cl > 50cc/min � wait 2-3 hours for Angiomax; 2-3days for Dabigatran
• if emergent and Cr Cl > 50cc/min � wait 3-5 hours for Angiomax; 3-5days for Dabigatran
Patel et al. Consensus Guidelines for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous Image-guided
Interventions. CIRSE. J Vasc Interv Radiol 2012; 23:727–736. DOI: 10.1016/j.jvir.2012.02.012; Addendum of Newer Anticoagulants to the
Conesnsus Guidelines. J Vasc Interv Radiol 2013; 24:641-645. DOI: 10.1016/j.jvir.2012.02.012


Creatinine (serum)
• Breakdown product of creatine phosphate produced at an approximately constant rate and then removed by the kidneys by BOTH glomerular filtration AND proximal tubular secretion (little tubular resorption)– There is correlation between creatinine clearance (CrCl) and GFR BUT CrCl can
overestimate GFR (d/t tubular secretion)
• Multiple GFR calculators (incorporate age, sex, race – weight is no longer included as normalized to BSA)– IDMS-traceable MDRD study equation (estimates slightly lower)
• GFR (mL/min/1.73m2) = 175 x (Scr/88.4)-1.154 x (Age)-0.203 x (0.742 if female) x (1.212 if African American) (SI units)
– CKD-EPI equation (estimates slightly higher)• GFR = 141 × min (Scr /κ, 1)α × max(Scr /κ, 1)-1.209 × 0.993Age × 1.018 [if female] × 1.159 [if
black]where: Scr is serum creatinine in µmol/L, κ is 61.9 for females and 79.6 for males, α is -0.329 for females and -0.411 for males, min indicates the minimum of Scr /κ or 1, and max indicates the maximum of Scr /κ or 1.
– Calculators are a dime a dozen online or via a smartphone app – no need to memorize!

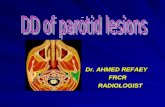
Glomerular Filtration
Rate (GFR)
Age (years) Mean eGFR (cc/min/1.73m2)
20-29 116
30-39 107
40-49 99
50-59 93
60-69 85
70+ 75
Coresh J, Astor BC, Greene T, Eknoyan G, et al. Prevalence of chronic kidney disease and
decreased kidney function in the adult US population: Third national health and nutrition
examination survey. American Journal of Kidney Disease. 2003; 41 (1): 1-12.
General CrCl guidelines for adults (> 18yo) for CT contrast administration:
Men < 120µmol/L (GFR range of 75 @ 20yo to 46 @ 90yo)
Women < 100µmol/L (GFR range of 70 @ 20yo to 43 @ 90yo)

Nephrotoxicity
• Kidneys receive ~1/4 of resting cardiac output (~1.3 L/min); GFR = 125 cc/min (180 L/day); urine volume ~ 1 L/day �kidneys reabsorb ~99% of glomerular filtrate– Contrast agents easily pass through glomeruli being filtered out
– Pathogenesis:• Vascular changes
• Tubular injury
• Tubular obstruction
– No universal agreement regarding what constitutes contrast-induced nephropathy (CIN) (generally development of ARF after radiocontrast administration in absence of an alternative identifiable cause)• ?increase in serum Cr by 25-50% above baseline
• ?absolute elevation of 0.5-2.0 mg/dL from baseline (44.2 µmol/L)

Classic Teaching: CIN Risk Factors
• Renal insufficiency– Cutoffs: Cr of 120 (M); 100 (F)
• DM
• Dehydration
• Cardiovascular disease
• Diuretic usage
• Multiple myeloma
• Hypertension
• Hyperuricemia
• Multiple iodinated contrast doses
in a short time interval (< 24 hrs)

Classic Teaching: CIN – Clinical Course
• It depends
– Baseline renal fxn; other risk factors; degree of hydration
– Usual course = transient asymptomatic elevation in serum creatinine rising @ 24 hrs and peaking within 4 days, returning to baseline by 7-10 days
– Atypical to develop permanent renal dysfxn
• Why do we care?
– Longer hospital stays; higher mortality; higher incidence of cardiac/neurologic events

Classic Teaching: CIN
• Actual incidence:– Controversial
– Lack of control groups in literature (important to have a baseline for comparison – how many patients who do NOT receive contrast have a serum creatinine change anyway)
– Bruce et al AJR 2009 showed frequency + magnitude of post-CT serum creatinine elevation equivalent regardless of receiving dose of iodinated contrast
• Insufficient data to prescribe a threshold for CIN BUT increased risk in pts with pt with stable chronic renal insufficiency of 2.0 mg/dL(176 µmol/L)
• CAUTION in pts with AKI – no great data
• ESRD – not at risk for CIN, okay to receive contrast
• ?Time interval for measuring Cr – 30 days generally accepted but prudent to shorten if inpatient

CIN – myth?
• Does CIN actually exist?
• Retrospective study from 2000-2010 of all contrast-enhanced and unenhanced CTs of the chest, abdomen, and/or pelvis (157,140 scans in 53,439 unique patients with 1,510,001 serum creatinine values)
• Patients stratified into low, medium, and high-risk groups (based on CrCl) for developing CIN
• Incidence of AKI (as defined by increase of serum Cr 44.2µmol/L or 0.5mg/dL) after propensity matching patients
• AKI risk was NOT significantly different between the two groups (those receiving contrast and those who did not receive contrast)

CIN – Management
• Because okay, you probably shouldn’t give contrast to *some* patients still
• ESRD
– Okay to receive iodinated IV contrast b/c no further risk of renal damage because kidneys no longer functioning
– ?risk of osmotic load � pulmonary edema and anasarca
• Unless using a LARGE volume of contrast or underlying cardiac dysfunction, no need for urgent dialysis (47)*** (ACR)
– Theoretical risk of converting an OLIGURIC patient to an ANURIC patient if administer contrast

CIN - Management
• Prevention:– Alternative imaging strategies
– Appropriate screening
– Repeat injections: recall half-life of 2 hours � takes ~20 hrs to excrete entire dose (scan again > 24 hours) unless urgent
• Choice of contrast agent:– Literature supports LOCM > HOCM (less nephrotoxic in pts with underlying
renal dysfunction); data of LOCM v. IOCM is less clear
• HYDRATION– ***MAJOR*** PREVENTATIVE MEASURE
– Exact rate/volume uncertain – use isotonic• Variable protocols: 0.9% NS IV @ 100 cc/hr for 6-12 hrs prior
to study and for 4 hrs post-contrast administration
• Oral hydration less effective
• ?sodium bicarb; NAC
• Not endorsed: diuretics (mannitol, furosemide); theophylline;
endothelin-1; fenoldopam

Sidenote
• Metformin does NOT increase risk of CIN
• Rarely, it may cause lactic acidosis in a patient
with renal failure.
Image courtesy of Diabetes Daily.

References
• ACR manual on contrast media. Version 9, 2013 [Internet] Reston, VA: American College of Radiology, ACR Committee on Drugs and Contrast Media; c2013. [cited 2014 Nov3]. Available from:http://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/2013_Contrast_Media.pdf.
• Cook BW. Anticoagulation Management. Semin Intervent Radiol. 2010 Dec; 27(4): 360–367. doi: 10.1055/s-0030-1267849
• Coresh J, Astor BC, Greene T, Eknoyan G, et al. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third national health and nutrition examination survey. American Journal of Kidney Disease. 2003; 41 (1): 1-12.
• Katzberg RW, Newhouse JH. Intravenous Contrast Medium–induced Nephrotoxicity: Is the Medical Risk Really as Great as We Have Come to Believe? Radiology. 2007 Jun;243(3):622-8. Epub 2007 Apr 19. Small molecule antidote for anticoagulants. Circulation 2012, 126:A11395.
• Macdonald RJ, McDonald JS, Bida JP, Carter RE, Fleming CJ, Misra S, Williamson EE, Kallmes DF. Intravenous Contrast Material–induced Nephropathy: Causal or Coincident Phenomenon? Radiology 2013 267:1, 106-118.
• Pollack CV, Reilly PA, Eikelboom J, Glund S, Verhamme P, Bernstein RA, Dubiel R, Huisman MV, HylekEM, Kamphuisen PW, Kruezer J, Levy JH, Selke FW, Stangier J, Steiner T, Wang B, Kam CW, Weitz JI. Idarucizumab for Dabigatran Reversal. N Engl J Med 2015; 373:511-520August 6, 2015DOI: 10.1056/NEJMoa1502000
• Younathan CM, Kaude JV, Cook MD, Shaw GS, Peterson JC. Dialysis is not indicated immediately after administration of nonionic contrast agents in patients with end-stage renal disease treated by maintenance dialysis. AJR Am J Roentgenol 1994; 163:969-971.