Lab Test Aspergillosis
15
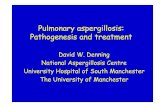
Review Introduction Aspergillus spp are ubiquitous opportunistic moulds that cause both allergic and invasive syndromes. The genus comprises approximately 180 species, of which 33 have been associated with human disease. Most infections are caused by Aspergillus fumigatus, Aspergillus flavus, Aspergillus terreus, and Aspergillus niger; 1 less commonly, Aspergillus nidulans can be implicated as the causative pathogen, especially in the setting of chronic granulomatous disease. 2 An accurate diagnosis of invasive aspergillosis is important for clinical reasons; an earlier diagnosis is associated with improved patient survival 3 and tests with a high negative predictive value may allow expensive and potentially toxic antifungal drugs to be withheld. New drugs—eg, voriconazole—exhibit differential mould activity; the ability to specifically exploit their anti- aspergillus properties requires a rapid and accurate laboratory diagnosis. The epidemiology of invasive aspergillosis is changing; invasive disease is increasingly observed in the non-neutropenic phase of haematopoietic stem cell transplantation 4–6 and in non- classic settings such as critically ill patients in intensive care units. 7 Aspergillus spp other than A fumigatus—some of which demonstrate inherent resistance to antifungal drugs—are increasingly recognised. 8–10 An international collaborative effort recently produced standardised definitions for invasive fungal infections. 11 Thus, a review of the diagnostic modalities and their use in establishing a diagnosis of invasive aspergillosis is timely. Diagnostic tools Direct techniques The advantages of direct techniques over culture include superior sensitivity and a relatively rapid turn around time. The principal disadvantage is the inability to definitively distinguish other filamentous fungi (eg, Penicillium spp and Scedosporium spp) or implicate Aspergillus spp as the causative pathogen in circumstances in which there are atypical or non-specific morphological features. This disadvantage may compromise diagnostic accuracy and hence estimates of therapeutic efficacy if patients are recruited to clinical trials solely on the basis of hyphae that resemble Aspergillus spp. Within tissue sections, Aspergillus spp typically appear as slender septate hyphae that exhibit angular dichotomous branching (figure 1). Lancet Infect Dis 2005; 5: 609–22 DWD and WWH are at the School of Medicine, University of Manchester and Wythenshawe Hospital, Manchester, UK; TJW is at the Pediatric Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA. WWH is also at the Pediatric Oncology Branch, National Cancer Institute. Correspondence to: Professor David W Denning, Education and Research Centre, Wythenshawe Hospital, Southmoor Road, Manchester M23 9LT, UK. Tel +44 (0)161 291 5811; fax +44 (0)161 291 5806; [email protected] http://infection.thelancet.com Vol 5 October 2005 609 Invasive aspergillosis occurs in a wide range of clinical scenarios, is protean in its manifestations, and is still associated with an unacceptably high mortality rate. Early diagnosis is critical to a favourable outcome, but is difficult to achieve with current methods. Deep tissue diagnostic specimens are often difficult to obtain from critically ill patients. Newer antifungal agents exhibit differential mould activity, thus increasing the importance of establishing a specific diagnosis of invasive aspergillosis. For these reasons, a range of alternate diagnostic strategies have been investigated. Most investigative efforts have focused on molecular and serological diagnostic techniques. The detection of metabolites produced by Aspergillus spp and a range of aspergillus-specific antibodies represent additional, but relatively underused, diagnostic avenues. The detection of galactomannan has been incorporated into diagnostic criteria for invasive aspergillosis, reflecting an increased understanding of the performance, utility, and limitations of this technique. Measurement of (1,3)--D glucan in blood may be useful as a preliminary screening tool for invasive aspergillosis, despite the fact that this antigen can be detected in a number of other fungi. There have been extensive efforts directed toward the detection of Aspergillus spp DNA, but a lack of technical standardisation and relatively poor understanding of DNA release and kinetics continues to hamper the broad applicability of this technique. This review considers the application, utility, and limitations of the currently available and investigational diagnostic modalities for invasive aspergillosis. Laboratory diagnosis of invasive aspergillosis W W Hope, T J Walsh, D W Denning Figure 1: The appearance of Aspergillus spp in histological sections (A) Gomori methanamine silver (GMS) stain of rabbit lung in experimental invasive pulmonary aspergillosis (magnification x400). (B) A similar section stained with periodic acid-Schiff (PAS) (magnification x400). (C) and (D) show acute angle dichotomous branching, which is typical of Aspergillus spp (magnification x630).The GMS sections demonstrate the prominent staining and stark appearance of hyphae. By contrast, with PAS there is preservation of background histological detail and hyphal morphology, but hyphae are less conspicuous against the background.
-
Upload
rifka-fadhilah -
Category
Documents
-
view
45 -
download
0
description
Lab test about aspergillosis
Transcript of Lab Test Aspergillosis
-
Review
IntroductionAspergillus spp are ubiquitous opportunistic moulds thatcause both allergic and invasive syndromes. The genuscomprises approximately 180 species, of which 33 havebeen associated with human disease. Most infections arecaused by Aspergillus fumigatus, Aspergillus flavus,Aspergillus terreus, and Aspergillus niger;1 less commonly,Aspergillus nidulans can be implicated as the causativepathogen, especially in the setting of chronicgranulomatous disease.2
An accurate diagnosis of invasive aspergillosis isimportant for clinical reasons; an earlier diagnosis isassociated with improved patient survival3 and tests witha high negative predictive value may allow expensive andpotentially toxic antifungal drugs to be withheld. Newdrugseg, voriconazoleexhibit differential mouldactivity; the ability to specifically exploit their anti-aspergillus properties requires a rapid and accuratelaboratory diagnosis. The epidemiology of invasiveaspergillosis is changing; invasive disease is increasinglyobserved in the non-neutropenic phase ofhaematopoietic stem cell transplantation46 and in non-classic settings such as critically ill patients in intensivecare units.7 Aspergillus spp other than A fumigatussomeof which demonstrate inherent resistance to antifungaldrugsare increasingly recognised.810 An internationalcollaborative effort recently produced standardiseddefinitions for invasive fungal infections.11 Thus, a reviewof the diagnostic modalities and their use in establishinga diagnosis of invasive aspergillosis is timely.
Diagnostic toolsDirect techniquesThe advantages of direct techniques over culture includesuperior sensitivity and a relatively rapid turn aroundtime. The principal disadvantage is the inability todefinitively distinguish other filamentous fungi (eg,
Penicillium spp and Scedosporium spp) or implicateAspergillus spp as the causative pathogen in circumstancesin which there are atypical or non-specific morphologicalfeatures. This disadvantage may compromise diagnosticaccuracy and hence estimates of therapeutic efficacy ifpatients are recruited to clinical trials solely on the basis ofhyphae that resemble Aspergillus spp. Within tissuesections, Aspergillus spp typically appear as slender septatehyphae that exhibit angular dichotomous branching(figure 1).
Lancet Infect Dis 2005; 5: 60922
DWD and WWH are at the Schoolof Medicine, University ofManchester and WythenshaweHospital, Manchester, UK; TJW isat the Pediatric Oncology Branch,National Cancer Institute,National Institutes of Health,Bethesda, MD, USA. WWH is alsoat the Pediatric Oncology Branch,National Cancer Institute.
Correspondence to: Professor David W Denning,Education and Research Centre,Wythenshawe Hospital,Southmoor Road, ManchesterM23 9LT, UK. Tel +44 (0)161 291 5811; fax +44 (0)161 291 5806;[email protected]
http://infection.thelancet.com Vol 5 October 2005 609
Invasive aspergillosis occurs in a wide range of clinical scenarios, is protean in its manifestations, and is still associatedwith an unacceptably high mortality rate. Early diagnosis is critical to a favourable outcome, but is difficult to achievewith current methods. Deep tissue diagnostic specimens are often difficult to obtain from critically ill patients. Newerantifungal agents exhibit differential mould activity, thus increasing the importance of establishing a specific diagnosisof invasive aspergillosis. For these reasons, a range of alternate diagnostic strategies have been investigated. Mostinvestigative efforts have focused on molecular and serological diagnostic techniques. The detection of metabolitesproduced by Aspergillus spp and a range of aspergillus-specific antibodies represent additional, but relatively underused,diagnostic avenues. The detection of galactomannan has been incorporated into diagnostic criteria for invasiveaspergillosis, reflecting an increased understanding of the performance, utility, and limitations of this technique.Measurement of (1,3)--D glucan in blood may be useful as a preliminary screening tool for invasive aspergillosis,despite the fact that this antigen can be detected in a number of other fungi. There have been extensive efforts directedtoward the detection of Aspergillus spp DNA, but a lack of technical standardisation and relatively poor understanding ofDNA release and kinetics continues to hamper the broad applicability of this technique. This review considers theapplication, utility, and limitations of the currently available and investigational diagnostic modalities for invasiveaspergillosis.
Laboratory diagnosis of invasive aspergillosisW W Hope, T J Walsh, D W Denning
Figure 1: The appearance of Aspergillus spp in histological sections(A) Gomori methanamine silver (GMS) stain of rabbit lung in experimental invasive pulmonary aspergillosis(magnification x400). (B) A similar section stained with periodic acid-Schiff (PAS) (magnification x400). (C) and (D)show acute angle dichotomous branching, which is typical of Aspergillus spp (magnification x630).The GMS sectionsdemonstrate the prominent staining and stark appearance of hyphae. By contrast, with PAS there is preservation ofbackground histological detail and hyphal morphology, but hyphae are less conspicuous against the background.
-
Review
Wet mounts, potassium hydroxide preparations, and use ofroutine stainsAll specimens obtained in scenarios in which fungi arepossible aetiological agents should be subject to a series ofroutine direct procedures; these procedures may varyaccording to the specimen, degree of clinical urgency, andthe individual laboratory. Specimens may be examined asa wet mount preparation with or without the addition of10% potassium hydroxide, which aids in the visualisationof hyphal elements through the partial digestion andclearing of proteinaceous material while leaving thefungal cell wall intact.12 Subsequently, a smear is made ona slide, fixed and subjected to a variety of stainingprocedures. A Gram stain should be done as a matter ofroutine, but cytological stains (eg, Papanicolaou stain),fungal stains, and fluorescent stains may improvesensitivity.
Fungal stainsFungal-specific stains should be applied in all cases inwhich invasive aspergillosis is considered a diagnosticpossibility.13 Hyphal elements are stained withhaematoxylin and eosin, although they may be difficultto visualise if sparse, fragmented, or present in thesetting of substantial tissue necrosis. Fungal-specificstainseg, Gomoris methenamine silver stain (GMS)and periodic acid-Schiff (PAS)can be applied tohistological sections and smears (figure 1). On occasion,GMS is referred to as Grocotts stain or the Grocott-Gomori silver stainRobert Grocott demonstrated thatGMS, which was initially designed as a stain forglycogen and mucin, also readily stained fungalelements.14 PAS has the advantage of providing acounter stain that reveals the background host cellulardetail, tissue architecture, and inflammatory response.By contrast, the GMS counter stain removes the finedetails of background host cells and tissues, butprovides a more sensitive stain for detecting smallfragments of cell wall that may be otherwise obscuredby surrounding tissue elements. Thus, for detection ofhyphal elements, the use of the GMS stain may be moresensitive; whereas PAS provides more of the cellulardetail and architecture that may be of help inestablishing relations between the fungus and otherelements of tissue. This may be important in definingthe individual aspergillus-related syndromes that varyaccording to the immunological status of the host. Inthis regard, GMS and PAS are complementary.
Fluorescent techniquesFluorescent dyeseg, Calcofluor white, Uvitex 2B, andBlankophorare water-soluble colourless dyes thatselectively bind to beta-glycosidically linked poly-saccharides within fungal cell walls. They are not specificfor Aspergillus spp, but have the advantages of relativelyhigh sensitivity, rapid turnaround time, and broadapplicability. They may be applied to frozen sections,
paraffin-embedded tissue, and other fresh clinicalspecimenseg, bronchoalveolar lavage fluid (BAL) orcorneal scrapings.15,16
Immunohistochemistry, immunofluorescence, and in-situhybridisationImmunohistochemistry (using the monoclonal antibodyWF-AF-117 or EB-A118,19), immunofluorescence,20 and in-situ hybridisation21,22 have been studied as diagnosticmodalities. Collectively, these techniques have thepotential to provide genus and species specific data, whichmay be important to improve diagnostic certainty whenhyphae are seen invading tissue, but cultures or otheradjunctive diagnostic data are negative. The availability ofthese modalities in routine clinical microbiologylaboratories is variable.
CultureA culture yielding Aspergillus spp, in addition to enabling adiagnosis of invasive aspergillosis, may further definetherapeutic options via susceptibility testing or theisolation of a species possessing inherent antifungalresistance; examples of the latter include A terreus andA nidulans, which are both resistant to amphotericin B.10,23
The main disadvantage of culture is that it is relativelyslow (the process takes days), is relatively insensitive,24 andrequires specialised expertise for species determination.
In common with other pathogenic fungi, the ability togrow at 37C distinguishes Aspergillus spp from other non-pathogenic environmental moulds. Aspergillus spp can berecovered on most routine solid and liquidmicrobiological media (eg, blood agar, chocolate agar,brain heart infusion broth). A fungal-specific mediumeg, Sabouraud dextrose agarshould be included at thetime of initial specimen set-up in clinical scenarios inwhich Aspergillus spp (or other moulds) are consideredpossible pathogens, because of superior yield.25 Theaddition of antibioticseg, chloramphenicol andgentamicinto the medium is required for the recoveryof Aspergillus spp from specimens obtained from non-sterile sites, since they prevent bacterial overgrowth.Cycloheximide, a eukaryotic protein synthesis inhibitor, isfrequently added to fungal media to inhibit theovergrowth of cultures by non-pathogenic environmentalmoulds; however, on occasion, cycloheximide may inhibitthe growth of Aspergillus spp.26
The identity of a laboratory isolate can often be inferredon the basis of colonial morphology and colour. Definitiveidentification, however, is dependent on a detailedinspection of conidial morphology and ontogeny andrequires a microscopic examination of a simple teasedpreparation or a slide culture (a procedure in whichsporulation is induced and the relevant diagnostic featuresare visualised on the under-surface of a cover-slip). Theappearance and diagnostic features of individual species isbeyond the scope of this review and readers are referred todefinitive texts,27 useful guides,28 and excellent websites.
Seehttp://www.aspergillus.man.ac.uk
http://www.mycology.adelaide.edu.au and
http://www.doctorfungus.org
610 http://infection.thelancet.com Vol 5 October 2005
-
Review
Several additional issues pertaining to culture requireemphasis. First, the growth characteristics andmorphological appearances of Aspergillus spp areprotean and in some circumstances quite atypical; inthis regard, Aspergillus spp are great mimics and shouldalways be included in the list of diagnostic possibilitiesfor an unidentified mould. Second, at least on occasion,sporulation may be difficult or impossible to induce,29
and other modalities must be used for the purposes ofidentification. In this circumstance, moleculartechniques are perhaps best placed to enable rapid andaccurate identification.
Serological techniquesGalactomannan Galactomannan is a heat-stable heteropolysaccharidepresent in the cell wall of most Aspergillus and Penicilliumspecies.30 The molecule is comprised of a non-immunogenic mannan core with immunoreactive side-chains of varying lengths containing galactofuranosylunits.30 The composition of galactomannan varies betweengenera and strains, as well as the strain and conditionsused for its production, extraction, and purification.30
There are two commercial assays for the detection ofgalactomannanthe Pastorex kit (Sanofi DiagnosticsPasteur,Marnes-La-Coquette, France) and Platelia ELISA(BioRad, Marnes-La-Coquette, France). Pastorex is nowrarely used, while Platelia has been available in Europe forapproximately 10 years and has recently been licensed inthe USA. There has been a progressive increase in theunderstanding of the diagnostic utility of galactomannanto a point that has enabled its incorporation intodiagnostic criteria.11 However, galactomannan testing isnot universally available to clinicians; the decision to offergalactomannan testing within a hospital microbiologylaboratory depends on resources, the institutionalincidence of invasive aspergillosis, and the hospital case-mix.
Details surrounding the release and kinetics ofcirculating galactomannan remain largely undefined. Thegrowth phase, microenvironment, host immune status,and pathology may all influence galactomannan release.31
An abundance of data supports the notion thatgalactomannan production is proportional to fungal loadin tissue;3234 furthermore, galactomannan levels appear tohave prognostic significance, with high unremitting levelsin the face of antifungal therapy associated with anunfavourable outcome.10,3337
Assays to detect galactomannan have mostly usedserum and BAL fluid. Galactomannan can also bedetected in tissue and a number of bodily fluids includingCSF, peritoneal fluid, urine, and pericardial fluid,although data to support its use at these sites is relativelyscant, and is likely to remain that way.38
Galactomannan assays use EB-A2, a monoclonalantibody derived from rats, which is directed towards the (1,5)-linked galactofuranoside side-chain residues of the
galactomannan molecule.39 Four or more epitopes arerequired for antibody binding.31,39 Detection is achievedusing a sandwich ELISA format, which is made possibleby multiple immunoreactive epitopes on a singlegalactomannan molecule.39
There are a number of important determinants ofanalytical sensitivity of galactomannan assays. First, thebinding of EB-A2 requires four or moregalactofuranoside epitopessensitivity may becompromised by the inability to detect secreted antigensthat bear fewer residues.31 Second, the Platelia assay isdependent on a pretreatment step, the goal of which is toremove complexing antibody that may block EB-A2binding. However, the acid-sensitive galactofuranosideresidues may be degraded by the edetic acid used in thisstep.31 Finally, the limit of detection using the sandwichELISA format is lower (1 ng/L) than that achievableusing latex agglutination (15 ng/L).40 In terms of theanalytical specificity, cross reactivity with otherfilamentous fungi, bacteria, drugs, and cotton swabshave been documented,4145 but whether this is due to(exogenous) galactomannan or unrelated cross-reactivemolecules is unclear.
There have been considerable efforts in establishing theappropriate galactomannan ELISA cut-off to maximiseclinical sensitivity and specificity. The ELISA endpoint is acontinuous variable and the optimal cut-off should bedetermined after defining the receiveroperator curverelation (ie, the relation between sensitivity and1specificity).46 The cut-off level of 15 ng/L initiallyrecommended by BioRad and used in many early studieshas been progressively revised downwards; a cut-off of05 ng/mL is now currently accepted by the US Food andDrug Administration (FDA), while a level of 07 ng/L iscommonly used in Europe.47
The clinical sensitivity of galactomannan ELISA issomewhat variable, with a range of 29100%.31 There are anumber of potential reasons for these disparate results.First, the performance of the assay may differ according tothe host group and therefore the underlying pathologicalprocess. In studies of profoundly immunocompromisedpatients, sensitivity has been generally reported to be inexcess of 90%,48,49 while in other settingseg, chronicgranulomatous disease50 and solid organ transplan-tationsensitivity appears to be somewhat lower.5153
Second, accumulating evidence suggests that concomitantantifungal therapy leads to a decrease in the sensitivity ofgalactomannan.32,36,54 Finally, inadequate samplingstrategies could conceivably compromise clinicalsensitivity; the optimal sampling strategy for screeninghas not been rigorously defined, but the twice weeklydetermination of antigen levels has been generally used inpatients deemed to be at risk of invasive aspergillosis. Bycontrast, galactomannan levels should be determinedimmediately in a host with a constellation of clinicalfeatures indicative of invasive aspergillosis to facilitate adefinitive diagnosis.
http://infection.thelancet.com Vol 5 October 2005 611
PersonalHighlight
-
Review
The clinical specificity of galactomannan is generallyestimated to be greater than 90%.32,36,4749,55 The specificity ofgalactomannan in neonates and children appears to belower, which is possibly due to the ingestion of extraneousgalactomannan (in food and water) and translocationacross a damaged or immature gut wall.45,47,56 Antibioticsrepresent an additional source of extraneousgalactomannan that may compromise clinical specificity.The in-vitro reactivity of a range of antibiotics ingalactomannan assays was originally reported in 1997.57
More recently, positive galactomannan results in patientsreceiving piperacillin-tazobactam have beendocumented.58,59 This phenomenon has been furtherexplored in vitro and in vivo and probably relates to thepresence of galactomannan within the drug itself.60,61 Thisfinding has forced some institutions to change theirantibacterial protocols and the FDA to issue a warning.62
(1,3)--D glucanThere has been an emergence of clinical data pertaining tothe diagnostic utility of the cell wall component, (1,3)--Dglucan.6367 (1,3)--D glucan assays have been developed byWako Pure Chemical Industries (Tokyo, Japan),Seikagaku Kogyo Corporation (Tokyo, Japan), MaruhaCorporation (Tokyo, Japan) and Associates of Cape Code(Falmouth, USA); the assay developed by Associates ofCape CodeFungitellhas been approved by the FDA inthe USA for the diagnosis of invasive fungal infections. -D glucan is present in the cell wall of most fungi; thenotable exceptions are Cryptococcus spp and thezygomycetes.67 The molecule is ubiquitous in theenvironment and has been used as a marker of fungalbiomass.68 The presence of (1,3)--D glucan in fungalspecies other than Aspergillus spp (eg, Candida spp,Fusarium spp, Acremonium spp, and Pneumocystis jiroveci)means that its role in establishing a specific diagnosis ofinvasive aspergillosis is not straightforward.
Assays to detect (1,3)--D glucan typically use serum.The common feature of all of the glucan assays is theability of (1,3)--D glucan to activate a coagulation cascadewithin amoebocytes derived from the haemolymph ofhorseshoe crabs. Horseshoe crab lysate preparations werefirst used to detect endotoxin using the limulus test orlimulus reaction (named after one type of horseshoe crab,Limulus polyphemus). Endotoxin induces clot formation viaa serine protease zymogen named factor C (figure 2).Subsequently, evidence emerged that (1,3)--D glucan-induced clot formation independently of factor C, via asecond serine protease zymogen, factor G, thus providingthe impetus for the development of the current assays.
The analytical sensitivity of the Fungitell assay is in theorder of 1 pg/mL, which is less than the cut-off of60 pg/mL used in a recent clinical study.67 A technicalconsideration pertinent to the analytical sensitivity of (1,3)--D glucan assays is that human plasma contains anumber of inhibitors of serine proteases that need to beremoved in a pretreatment step; this removal can be
achieved by an alkali reagent method (Fungitell), or by theaddition of Triton X-100 and heating to 70C for10 minutes (Wako assay). The alkali pretreatment step inthe Fungitell assay also converts triple-helix glucans intosingle-helix structures, which appear to be more reactive.Since both endotoxin and (1,3)--D glucan activate thehorseshoe crab coagulation pathway, an assay thatspecifically detects (1,3)--D glucan requires removal ofendotoxin from the specimen or the endotoxin-specificpathway from the lysate; correspondingly, endotoxin isinactivated by the addition of polymyxin in thepretreatment step in the Wako assay, while the Fungitellassay uses factor C to deplete limulus lysate. Thepretreatment step also enhances analytical specificity viathe removal of non-specific activators of serine proteasespresent in human serum.
There are no data that address the clinical sensitivity ofthe (1,3)--D glucan assays specifically for Aspergillus spp.The positive cut-off of 60 pg/mL was defined in a non-neutropenic group of patients with candidaemia.69 Theperformance of (1,3)--D glucan in the context ofantifungal therapy has not been rigorously studied. False-positive (1,3)--D glucan results have been documented inhaemodialysis, cardiopulmonary bypass, treatment withimmunoglobulin products, and exposure to glucan-containing gauze (eg, following major surgery).69
Environmental (1,3)--D glucan contamination may alsocompromise specificity.
Antibodies directed toward Aspergillus sppThe demonstration of specific antibody is required toestablish the diagnosis of chronic pulmonaryaspergillosis.69 Traditionally, antibody detection has notbeen considered useful for the diagnosis of acute invasiveaspergillosis, following an early study that failed todocument antibody formation in 15 patients with invasiveaspergillosis.70 Subsequently, antibody has beendocumented in approximately one-third of patients withinvasive aspergillosis.47,71 The detection of antibody may
612 http://infection.thelancet.com Vol 5 October 2005
Endotoxin (1,3)--D glucan
Factor C Activated factor C Activated factor G Factor G
Factor B Activated factor B
Clotting enzymeProclotting enzyme
Clotting enzyme activity detected via cleaving of synthetic chromagenicsubstrate or turbidimetric assay
Figure 2: The pathways for the activation of the amoebocyte lysate byendotoxin and (1,3)--D glucan and the use of this pathway for thedetection of (1,3)--D glucan
PersonalHighlight
-
Review
prove to be the best non-invasive means of establishingthe diagnosis of subacute invasive aspergillosis in non-neutropenic patients with invasive aspergillosis, asillustrated by a recent case report describing invasivepulmonary aspergillosis in an individual with chronicgranulomatous disease.72 Furthermore, antibody detectioncould be useful as a means of establishing a retrospectivediagnosis of invasive aspergillosis in profoundlyimmunocompromised hosts who have undergoneimmunological reconstitution, although more work isrequired in this regard.
The detection of antibodyMany assay formats have been used to detect antibodies toAspergillus spp, including immunodiffusion, counterimmunoelectrophoresis, complement fixation, particle-haemagglutination, indirect-immunofluoresence, radio-immunoassay, and ELISA.73,74 The large number ofepitopes in crude extracts may compromise specificity.The use of recombinant antigenseg, dipeptidyl-peptidases,75 superoxide dismutase,75,76 catalase,75 metallo-protease,75 mitogillin,77 and galactomannoprotein71,78mayrectify this situation. One potential advantage of usingassays with a single antigen is the prospect of studyingprotective epitopes and thereby facilitating the generationof assays that may also confer prognostic information.
MetabolitesAspergillus spp produce a range of extracellular enzymes(eg, metalloproteases, phospholipases) as well asprimary (eg, mannitol)33 and secondary metabolites (eg,gliotoxin),79 all of which at least have the potential toserve as diagnostic markers for invasive aspergillosis.The ability of Aspergillus spp to produce D-mannitol hasbeen known for many years80 and its diagnostic potentialexamined in several experimental models of invasiveaspergillosis,33,81 although it is limited in terms of itsbroad applicability as a diagnostic tool because of thecomplexity of measurements, which are done by gasliquid chromatography and mass spectroscopy. Recentwork suggests that gliotoxin is produced by most Afumigatus strains and the possibility of using it as adiagnostic marker has been entertained.82 Acomprehensive summary of the various secondarymetabolites (mycotoxins) produced by Aspergillus sppcan be found at http://www.aspergillus.man.ac.uk. Thedetection of metabolites represents an under-researchedarea in terms of their possible application as diagnosticmodalities for invasive aspergillosis.
Nucleic acid testsAs far as the amplification of nucleic acid and diagnosis ofinvasive aspergillosis is concerned, PCR technology hasdominated. A limited number of publications have usedthe isothermal technique nucleic acid sequence-basedamplification.83,84 Only PCR will be discussed here. Thelack of standardisation of technical issues has and
continues to represent a considerable barrier for thewidespread application of PCR as a diagnostic modalityfor invasive aspergillosis and this is the focus of thefollowing discussion.85
Clinical specimensMany studies have addressed the detection of nucleicacid from various fractions of blood (serum, plasma,whole blood) to establish a diagnosis of invasiveaspergillosis, but PCR may also be applied to BALspecimens86,87 and tissue,88 including paraffin-embeddedsections.89,90 The optimal blood fraction for the detectionof aspergillus DNA remains unknown. One study, usingquantitative PCR (qPCR), suggested that the yield ofDNA from serum, plasma, and white cell pellet wassimilar,91 while another demonstrated that the(qualitative) PCR signal from whole blood was superiorto plasma.92 Serum has the advantage that it enablesconcomitant antigen testing91 and does not require theaddition of anticoagulants (eg, sodium citrate, edetic acid,or heparin) that may inhibit PCR.93
DNA extractionThere are a multitude of extraction techniques; theprincipal technical issues are summarised in table 1.The chosen extraction method represents acompromise between efficiency, freedom fromexogenous contamination, and applicability to routinehigh-throughput laboratories. The fungal cell wallclearly represents the major hurdle to high-efficiencyextraction of fungal DNA. DNA may be extracted usingin-house methods, commercial kits (eg, Qiagen QIAmpTissue Kit [Hilden, Germany]), and automatedcommercial techniques (eg, MagNA Pure LC [RocheDiagnostics, Basel, Switzerland). Automatedcommercial techniques are probably required to makefungal DNA detection a viable option for routine clinicallaboratories. The efficiency of extraction of fungal DNAmay vary considerably between commercial kits.94 Highspeed cell disruption incorporating chaotropic reagentsand lysing matrices provide efficient and high yields ofDNA from Aspergillus spp and other filamentous fungi.95
Fungal contamination of extraction systems andreagents has been documented.96 Considerabledifferences in DNA extraction protocols andperformance is one aspect of molecular assays thathinders the comparison of studies.
Primer targetFor clinical diagnostic purposes, the detection of a broadrange of fungi is important, as is the ability to ultimatelyidentify the specific pathogen(s). The optimal approach, inthis regard, involves the application of broad-rangingpanfungal primers with post-amplification analysis forspecies determination. Panfungal primers are directedtoward conserved regions, usually within multicopygenes, which flank sequences containing species specific
http://infection.thelancet.com Vol 5 October 2005 613
-
Review
polymorphisms that can be exploited in post-amplificationanalysis.
The ribosomal DNA (rDNA) complex is the mostcommon target. This complex contains both conservedand variable sequences and there is a large volume of datadeposited in public databases for a wide range of generaand species. The recent genome sequencing ofA fumigatus, using strain Af293, revealed 35 repeatingunits;97 the structure of the gene complex is illustrated infigure 3.98 The mitochondrial genes encoding some of thetRNA genes91 and (apo)cytochrome b99 have also been usedas primer targets. Mitochondrial targets can be consideredmulticopy because of a multiple number ofmitochondria per cell nucleus; in Af293, there were12 copies of the mitochondrial genome present for everycopy of the nuclear genome.97
Amplification formatNested PCR formats have been widely used for Aspergillusspp in an attempt to optimise analytical sensitivity, but the
requirement to open reaction tubes means that there isconsiderable risk of contamination and the subsequentgeneration of false-positive results. Real-time formats havebeen increasingly used and are likely to dominate in thenear future.
Post-amplification analysisPost-amplification detection techniques provide genusor species specific data but may also increasesensitivity and specificity.100,101 Real-time detectiontechniques (eg, TaqMan, LightCycler, molecularbeacons) are automated, rapid, and reproducible, thusfacilitating comparisons between studies. Southernblotting has had a valuable role in the evolution of PCRas a diagnostic modality, but is unlikely to have anysubstantial future role in routine clinical assays.Single-strand conformational polymorphism,102,103
restriction fragment length polymorphism digestpattern,104 Line Probes,105 fragment size deter-mination,106 and PCR-ELISA107 may have a limited role
614 http://infection.thelancet.com Vol 5 October 2005
Feature Definitions and goals Specific considerations with respect to invasive aspergillosis
Sample Sample type, volume, transport, and handling Serum and white cell pellet equivalent and possibly superior to plasma as sampleshould be defined Heparin and citrate inhibitory to PCR
Sample handling varies between studies (some have demonstrated stability at room temperature for 48 h, others recommend immediate freezing)
DNA extraction Target is of an adequate concentration and quality Extraction efficiency for fungal DNA is low due to the requirement to break the cell wallfor amplification. PCR inhibitors and DNA nucleases Contamination rate 33% in one series, commercial reagents may be contaminated with removed fungal DNA
Ideally negative and positive extraction controls should be usedRemoval of red and white cells Red cell lysis buffer and white cell lysis bufferDisruption of cell wall Enzymatic methods (eg, lyticase, zymolase)
Chemical (eg, boiling in dilute alkali) Physical (eg, glass bead milling, freeze-thawing, sonication, grinding in liquid nitrogen)
Disruption of cell membrane Usually achieved with lysis buffer (sodium dodecyl sulphate, beta-mercaptoethanol, EDTA)Precipitation of protein and purification of DNA Phenol-chloroform
Silica fibres (eg, Qiagen Tissue Kit) Capture of DNA Alcohol precipitation
Magnetic beads (eg, MagNA Pure)Silica fibres (eg, Qiagen Tissue Kit)
Amplification Nested PCR, real-time formats, PCR-ELISA represent Nested formats potentially allow for optimal analytical sensitivity but are associated withthe commonest formats contamination and are difficult to compare
Real-time formats will probably dominate in the futureAmplification controls Negative and positive controls are required
Analytical The smallest number of target organisms reliably and Multicopy target preferablesensitivity reproducibly detected by the assay Assessed by serial dilution of Aspergillus spp (conidia or purified DNA) using the appropriate
clinical specimen as the diluent Circulating DNA in invasive aspergillosis is typically less than 10 colony forming units per mL or less than 30 fgExtraction method, primer target, and detection method all influence analytical sensitivity
Analytical Does the test detect only what it purports to? Specific primer and probe sequences initially identified from public databasesspecificity Amplicon ideally should be sequenced and a BLAST search done
Cross reactivity studies with a range of fungal and bacterial pathogens as well as human DNA are requiredPost-amplification detection probe(s) may enhance specificity
Inhibition Inhibitors of DNA polymerase (eg, heparin) Spiking with purified aspergillus DNA and analysing in a separate reaction controls Spiking with a plasmid construct containing different size and sequence or label to the target
Amplifying a human housekeeping gene (eg, betaglobin, HLA2), which also allows some determination of specimen adequacy, although the relative dominance of human DNA in clinical samples may mask low levels of inhibitors which could interfere with target amplification
Contamination Uracil-D-glycolase, appropriate number of control negative controls
Table 1: Technical variables required for a robust and reproducible PCR assay
-
Review
in specific instances, such as the identification oflaboratory isolates.
Analytical sensitivity and specificityThe analytical sensitivity of a molecular assay is usuallydetermined by serial dilution of the infectious agent inpooled non-infectious clinical material as the diluent.108
Such a paradigm immediately presents a problem forAspergillus spp or any other mould, since accurate andindeed meaningful dilution of hyphae is not possible.Two commonly used approaches include serial dilutionof conidia or DNA (either purified genomic DNA or aplasmid construct), although neither are ideal; theformer does not mimic a biologically valid scenario,since hyphae rather than conidia are the invasive form,while the latter does not control for issues in extractionefficiency. If it is intended that more than one species isdetectable then DNA from those species should beincluded in the assessment of analytical sensitivity.109
The analytical sensitivity of published assays varies byseveral orders of magnitude; however, most studiesreport detection limits in the order of 110 fg DNA;variability in the detection limit is yet another issue thatcompromises study comparability.
Studies differ considerably in terms of the methods andextent to which analytical specificity is determined; there
are no standard techniques or criteria (table 2). Primertargets are generally identified by aligning sequencesretrieved from public databases. This practice should beviewed as a necessary but insufficient step in establishingthe analytical specificity of an assay and further validationprocedures are required. Ideally, relatively early in assay
http://infection.thelancet.com Vol 5 October 2005 615
IGS
5'
5'
IGS IGSITS1 ITS2
58S18SSSU
28SLSU
3'
3'
IGS
Figure 3: The structure of the ribosomal DNA complexShaded areas denote areas of variability that are present throughout the complex that can be exploited to designassays of varying levels of specificity. IGS=intergenic spacer; ITS=internal transcribed spacer; LSU=long subunit;SSU=short subunit. Adapted from reference 98.
Primer target Assay format Intended BLAST search of primer and probe sequences; isolates Method by which analytical specificity determined and result Referencespecificity with same probability match as intended target
18S rRNA PCR-ELISA Aspergillus spp Aspergillus spp, Penicillium italicum, Penicillium commune, Penicillium Cross-reactivity studies: Einsele chryosogenum, Penicillium brevicompactum, Penicillium phialosporum, Amplification of Aspergillus fumigatus, Aspergillus flavus, Aspergillus et al110
Penicillium tardum, Penicillium allii, Penicillium expansum, Ajellomyces terreus, Aspergillus niger, Aspergillus nidulans, Aspergillus versicolor, capsulatus (telemorph of Histoplasma capsulatum), Paracoccidiodes Histoplasma capsulatumbrasiliensis, Eupenicillium spp, Penicilliopsis spp No amplification of Malassezia furfur (3 strains), Fusarium spp (3 strains),
Trichosporon cutaneum (2 strains), Mucor spp (3 strains), Penicillium spp (2 strains), Pseudallescheria boydii (1 strain), Paecilomyces spp (2 strains), Saccharomyces cerevisiae (2 strains)
18S rRNA TaqMan Aspergillus spp Aspergillus spp, P italicum, Penicillium glabrum, P commune, Cross-reactivity studies: Kami P chryosogenum, P brevicompactum, P phialosporum, Penicillium Ampification of A fumigatus, A niger, A terreus, A flavus, Aspergillus oryzae et al111
purpurogenum, P tardum, Penicillium verruculosum, Penicillium hirsutum, No amplification of Candida albicans, Candida tropicalis, Candida krusei, Penicillium radicum, Penicillium funiculosum, Penicillium siamense, Candida parapsilosis, Candida glabrata, Candida guilliermondiiPenicillium pittii, Penicillium minioluteum, Penicillium pinophilum, Penicillium variabile, Penicillium rugulosum, Penicillium crateriforme, Penicillium variotii, Eupenicillium spp, and others
Mitochondrial Competitive PCR Aspergillus spp A fumigatus Cross-reactivity studies: BretagneDNA (tRNA) with PCR-ELISA Ampification of 30 isolates of A fumigatus, A niger, A terreus, A flavus et al112
No amplification of A nidulans, C albicans, C tropicalis, C krusei, C parapsilosis, C glabrata, Cryptococcus neoformans
Mitochondrial Competitive PCR A fumigatus, No database matches Amplicon sequenced: revealing A fumigatus and A flavus Bretagne DNA (tRNA) with PCR-ELISA A flavus Cross-reactivity studies: et al113
No ampification of A niger, A terreus, A nidulans, Aspergillus ustus, Penicillium purporogenum, Scopulariopsis brevicaulis
Mitochondrial LightCycler A fumigatus A fumigatus None, although clinical specificity assessed using 20 serum samples from Costa DNA (tRNA) healthy individuals et al91
Mitochondrial LightCycler A fumigatus Eupenicillium shearii, Neosartorya fischerii, A fumigatus Cross-reactivity studies: Spiess DNA (cyto- Amplification of A fumigatus, Aspergillus clavatus et al99
chrome b) No amplification of Candida spp, other Aspergillus spp, P chryosegenum, P expansum, P funiculosum, P variotii, Rhizopus oryzae, Fusarium proliferatum
The BLAST searches were done at http://www.ncbi.nlm.nih.gov, using search for short nearly exact matches. The primer and probe sequences were searched simultaneously and were separated by a string of at least ten nucleotides toensure only the specified sequences were matched in the search algorithm. Only matches identical to those of the intended target are displayed.
Table 2: Selected examples of issues in establishing the analytical specificity of PCR assays to detect Aspergillus spp
-
Review
development, the amplicon should be sequenced and aBLAST search done to verify that the intended target hasbeen amplified.109 Subsequently, the assay should bechallenged with organisms that have a high likelihood ofcross-reacting with the target; in the case of Aspergillusspp, genera that are close phylogenetic relationseg,Penicillium spp and Paecilomyces spp114 are especiallyimportant to consider (figure 4). A further considerationis that sequences are being continuously deposited inpublic databases; a unique sequence at the time of primerdesign may subsequently align with a sequence from anunrelated species or genus deposited at a later date. Somehave suggested that BLAST searches are done on anannual basis to ensure there is no cross reactivity withrecently submitted sequence.109 A final consideration isthat false-positive reactions due to carry-overcontamination of amplicon from previous reactions maybe prevented with the addition of uracil-D-glycolase.85
Clinical sensitivity and specificityThere are a number of factors that potentially have animpact upon the clinical sensitivity of PCR. Themagnitude of the quantitative PCR signal falls withantifungal therapy in both experimental models and inclinical contextsthis may account for false-negative PCRresults.110,111,115,116 Patients at risk for invasive aspergillosisare also often prescribed a multitude of drugs and fluids,all of which may act as non-specific inhibitors of PCR; as a
result, inhibition controls are mandatory and may take theform of spiking the sample with aspergillus DNA, aplasmid construct, or amplification of a human gene suchas betaglobin (table 1).
The application of diagnostic modalitiesLaboratory isolatesGiven the distinct differences in disease manifestations,prognosis, and antifungal susceptibility betweendifferent fungal genera and species, a rapid diagnosiswill assume increasing importance. The inherentproblems with identification using culture methods havebeen outlined. An increasing number of studies haveexamined the use of PCR to enable the accurate andrapid detection of laboratory isolates (table 3). The rapididentification of laboratory isolates using microarraytechnology with a panfungal chip is possible and nodoubt the relevant studies will emerge in the near future.
Clinical specimensThe application of diagnostic modalities to tissue,respiratory tract secretions, and blood in the context of thepathophysiology of invasive pulmonary aspergillosis isillustrated in figure 5.
Tissue and sterile fluidsHistological and culture techniques applied to tissue formthe reference diagnostic standard for invasive
616 http://infection.thelancet.com Vol 5 October 2005
005
100
100
100
100
100
58
100
100
Candida krusei
Candida lusitaniaeCandida albicans
Taphrina deformans
Aureobasidium pullulans
Histoplasma capsulatum
Blastomyces dermatitidis
Coccidioides immitis
Trichophyton rubrum
Eremascus albusAscosphaera apis
Penicilllum marneffei
Paecilomyces variotii
Peniclllium chrysogenum
Aspergillus flavusAspergillus fumigatus
Aspergillus terreus
Aspergillus nigerAspergillus nidulans
Eurotium fubrumMonascus purpureus
Neurospora crassa
Colletotrichum gloeosporiodesOphiostoma uimi
Ophiostoma stenoceras
Sporothrix schenckii
Candida viswanathiiCandida tropicalis
Schizosaccharomyces pombe
Endomyces geotrichum
Figure 4: The phylogenetic relations between Aspergillus spp and other fungi based on the 18S rRNA complexAdapted from reference 114.
-
Review
aspergillosis11 and have been, and continue to be, thestandard tools by which tissue invasion and destruction byhyphae is documented. Within this context, the followingpoints specifically deserve emphasis. First, difficulties inobtaining deep tissue specimens in patients who are leastable to tolerate invasive procedures have been exhaustivelydocumented and remain one of the principal factorsdriving the development of new diagnostic techniques.Second, the analytical sensitivity of both histology andculture is relatively low, meaning that invasive disease iswell established by the time that culture and histology arepositive. Third, the specificity of the reference standard forAspergillus spp is optimised with the combination ofhistological and culture data and this rigorous standardhas been used in some recent clinical trials.48,120 Theproblem, however, is that Aspergillus spp can only berecovered from tissue in the context of positive histologyin 3050% of cases.24 Finally, the possibility of accepting apositive PCR result in tissue as the reference standard forinvasive aspergillosis deserves increasing attention.Certainly, data from experimental models suggests thatvalidated PCR is more sensitive than culture for thedetection of Aspergillus spp in tissue, especially in thesetting of substantial tissue necrosis;115,121 the key in thisregard is assay validation.
Non-sterile sitesIn the absence of tissue specimens, samples obtainedfrom contiguous non-sterile siteseg, the upper andlower respiratory tractserve as a surrogate with whichto establish the diagnosis of invasive aspergillosis. Inthe case of invasive pulmonary aspergillosis, viablehyphal elements or related serological or molecularmarkers are shed into the respiratory tract from infectedparenchyma (figure 5). A body of data suggests thisshedding occurs relatively late in the natural history,thus compromising attempts to establish an earlydiagnosis using this approach.25,122,123 The isolation ofAspergillus spp (or related serological, molecular, orbiochemical markers) in the respiratory tract may
represent one of three scenarios: (1) evidence of currentdisease, (2) true colonisation, or (3) a marker for thefuture development of invasive disease. An example ofthe latter is provided by a study that demonstrated that apositive PCR result from BAL at the time of bonemarrow transplant conditioning was predictive of thesubsequent development of invasive pulmonaryaspergillosis.124
There are a number of points to make about usingBAL specimens to secure a diagnosis of invasivepulmonary aspergillosis. First, although BAL is a safeprocedure, even in patients with substantialimmunological impairment, it is not a trivialundertaking and requires a dedicated and competentbronchoscopist and an adequate commitment ofresources. Second, the overall sensitivity (using cultureand microscopy) is relatively low and generally estimatedto be in the order of 50%.122,123,125,126 Variations in BALtechnique,127 the location, size, and type of pulmonarylesions,128130 and the timing of bronchoscopy122 are allimportant determinants of the overall estimate. Theimpact of antifungal therapy in terms of the recovery ofaspergillus and related markers in the respiratory tractremains poorly defined. Third, the specificity of theisolation of Aspergillus spp from the respiratory tract inpatients with substantial immunological impairmenteg, those with allogeneic haematopoietic stem celltransplantation or neutropeniais very high,131 but forother patient groups, the likelihood of underlyinginvasive pulmonary aspergillosis varies enormously.25,131
Fourth, qPCR may prove to be especially useful indetermining the relation between the fungal burden inthe respiratory tract and the probability of underlyinginvasive disease;87,99,115 however, at the current time, thebenefit of PCR over conventional culture remains to befurther defined. Finally, the diagnostic yield from BALfluid is potentially optimised with the application ofmore than one test; a recent study demonstratedsensitivity was improved with the concomitantapplication of galactomannan and PCR.130
http://infection.thelancet.com Vol 5 October 2005 617
Specimen Target Demonstrated specificity PCR format Detection method Reference
Cultures ITS1-58S rRNA-ITS2 Aspergillus fumigatus, Aspergillus flavus, Aspergillus Conventional Sequencing of amplicon Henry et al117
terreus, Aspergillus niger, Aspergillus ustusCultures ITS1-58S rRNA-ITS2 A fumigatus, A flavus, Aspergillus nidulans, Aspergillus
versicolor Conventional Line probe Martin et al105
Cultures ITS1-58S rRNA-ITS2 A fumigatus, A flavus, A terreus, A niger, A nidulans Conventional SSCP Rath et al103
Cultures ITS1-58S rRNA-ITS2 A fumigatus Multiplex PCR Ethidium bromide Luo et al118
Cultures ITS1-58S rRNA-ITS2 A fumigatus Nested Ethidium bromide Zhao et al119
Cultures 58S rRNA-ITS2 region A fumigatus, A flavus, A terreus, A niger Conventional Automated fluorescent capillary electrophoresis (detection of different length of amplicon) Turenne et al106
Cultures 18S rRNA A fumigatus, A terreus Conventional SSCP Walsh et al102
Cultures and ITS2 Aspergillus spp and Penicillium spp, A fumigatus, A flavus, Conventional PCR-ELISA De Aguirre et al107
tissue A terreus, A niger, A nidulans, A ustus, A versicolor
SSCP=single-strand conformational polymorphism
Table 3: The use of PCR in the identification of Aspergillus spp
-
Review
BloodBlood sampling represents the optimal non-invasivediagnostic approach for invasive aspergillosis. Despitetheir propensity for vascular invasion, Aspergillus spp areonly very infrequently isolated from blood usingconventional culture techniques, hence the traditionaldependence on tissue specimens to secure a definitivediagnosis of invasive aspergillosis. There is an extensivebody of literature examining the diagnostic utility ofmolecular and serological techniques in blood.Galactomannan has been incorporated into diagnosticcriteria for invasive aspergillosis and the technical issuesrequired for PCR to be applied in the same manner have
been discussed. However, there remain some additionalpertinent issues. First, specific sampling strategies are yetto be systematically studiedyield is almost certainly afunction of the volume and frequency of sampling, as isthe case with blood cultures. Second, the appropriateinterpretation of a positive galactomannan or validatedPCR result in a patient at risk of invasive aspergillosis, butwithout subsequent evidence of invasive disease, remainsunclear and difficult to resolve; the most conservativeinterpretation in this context is that all single positiveresults are false-positive, but at least on occasion, suchresults may reflect true invasive disease that has abortedor is non-progressive. Third, a body of evidence suggests
618 http://infection.thelancet.com Vol 5 October 2005
Appearance of viable or non-viablehyphal elements or surrogate markers(galactomannan, DNA) in the contiguousrespiratory tract
Pathogenesis of IPA
Respiratory tract
Inhalation of conidia,germination, mucosalsurfaces breached
Blood
Dissemination tonon-contiguous sites
A B
Lung andsinus tissue Tissue
invasionanddamage
Haematogenousdissemination
Compartmental characteristicsand inter-compartmental relations
Appearance of Aspergillus sppand associated markers occurslate in the natural history of IA
Quantitative relation betweenfungal load in tissue and respiratorytract difficult to determine with culture;quantitative PCR may be useful
Positive predictive value dependson underlying disease
Destruction and invasion of tissue byhyphal elements represents the conceptualunderpinning for IA; the demonstration ofAspergillus spp in tissue is the referencestandard for IA
Sensitivity of tissue sampling may be low due to sampling error, prior antifungal therapy, fungal tissue load beneath the analytical sensitivity of histology and culture
Highest specificity achieved with combination of histology and culture
Blood cultures typically negative
Risk factors for haematogenousdissemination remain poorly defined
Clinical samples andsampling strategies
Bronchoalveolar lavageSensitivity ~50%
Sputum examinationPositive sputum culturesoccur relatively late in thenatural history
Fine needle aspiration May be more sensitive than bronchoscopy depending on the radiological pattern of disease
Complications include pneumothorax,haemoptysis, haemorrhagiccomplications, seeding of needle tract
Open biopsySensitivity compromised by infarctionand necrosisIncreased diagnostic certainty may not translate to improved patient outcome
Blood samplingBlood cultures generally not helpfulPCR and galactomannan from blood potentially usefulOptimal sampling strategies yet to berigorously defined
Figure 5: Compartmental characteristics, inter-compartmental relations, and sampling strategies as they relate to the pathogenesis of invasive pulmonaryaspergillosis(A) Hepatosplenic aspergillosis (courtesy of Damon Eisen). (B) Cerebral abscess due to Aspergillus fumigatus. IA=invasive aspergillosis.
-
Review
that both PCR and galactomannan may enable a specificdiagnosis to be established earlier than is possible using aconventional approach.32,49,132 Fourth, the combination ofdifferent diagnostic modalitieseg, concomitant meas-urement of galactomannan and (1,3)--D glucanis astrategy that may optimise diagnostic accuracy.63 Finally, itseems likely that both PCR and galactomannan engenderimportant prognostic information; a falling galacto-mannan titre or a positive-turning-negative PCR signal inthe context of antifungal therapy is usually associated witha successful outcome. However, at the current time,galactomannan and PCR have not been systematicallyused to guide antifungal therapy.
The incorporation of diagnostic data into managementstrategiesGalactomannan (and validated PCR) applied to blood canbe used as screening tools to further improve theidentification of patients at high risk of developinginvasive aspergillosis.133 A positive result may enable thestart of early targeted antifungal chemotherapy, whileexpensive and potentially toxic antifungal drugs can bewithheld with persistently negative results. Testing for(1,3)--D-glucan could be also be useful in this regard.When the assays are used in this manner, a positive resultshould also serve as a trigger for additional diagnosticevaluationeg, a high-resolution computed tomographyscan of the thoraxto investigate the possibility of asubclinical focus of infection. The success of galac-tomannan (and validated PCR) as a screening tool islargely dependent on the underlying prevalence ofinvasive aspergillosis, which varies according to thespecific host group and institution; thus, the requirementand extent of galactomannan screening may varyaccordingly.
An alternate diagnostic strategy is to reservegalactomannan and validated PCR for situations inwhich clinical and radiological data are suggestive ofinvasive aspergillosis; in this scenario, galactomannanand validated PCR applied to serum, and other tissuesand fluids, may enable a definitive diagnosis of invasiveaspergillosis to be secured. Although this approach doesnot facilitate early antifungal therapy, it may minimisethe use of invasive diagnostic modalities. Furthermore, amore definitive diagnosis enables the administration ofspecific anti-aspergillus therapy and would be of
considerable benefit for future diagnostic andtherapeutic research.
Future challengesInvasive aspergillosis continues to pose many challenges.From a diagnostic point of view, improving the testaccuracy remains a priority for patient care, therapeuticresearch, and future diagnostic research. The question, ofcourse, is the manner in which these improvements canbe achieved. The progressive refinement of existingtechniques and development of new diagnostic technolo-gies is clearly a priority. Substantial work remains in areasrelated to cost-effectiveness and whether patients whoundergo intensive diagnostic testing have improvedoutcome. Just as importantly, however, is the generationof a clinical environment and culture that is amenable tohigh quality diagnostic research, the provision of adequatefunding, multicentre participation, international collabo-ration, and rigorous study design.
Conflicts of interestWWH is supported by an unrestricted educational grant from Merck & Coand the Fungal Research Trust. TJW and DWD have no conflicts ofinterest to declare.
AcknowledgmentsWe thank Ruta Petraitiene for the photomicrographs in figure 1.
References1 Perfect JR, Cox GM, Lee JY, et al. The impact of culture isolation of
Aspergillus species: a hospital-based survey of aspergillosis. Clin InfectDis 2001; 33: 182433.
2 Segal BH, DeCarlo ES, Kwon-Chung KJ, Malech HL, Gallin JI,Holland SM. Aspergillus nidulans infection in chronic granulomatousdisease. Medicine (Baltimore) 1998; 77: 34554.
3 von Eiff M, Roos N, Schulten R, Hesse M, Zuhlsdorf M, van de Loo J.Pulmonary aspergillosis: early diagnosis improves survival.Respiration 1995; 62: 34147.
4 Wald A, Leisenring W, van Burik JA, Bowden RA. Epidemiology ofAspergillus infections in a large cohort of patients undergoing bonemarrow transplantation. J Infect Dis 1997; 175: 145966.
5 Grow WB, Moreb JS, Roque D, et al. Late onset of invasive Aspergillusinfection in bone marrow transplant patients at a university hospital.Bone Marrow Transplant 2002; 29: 1519.
6 Alangaden GJ, Wahiduzzaman M, Chandrasekar PH. Aspergillosis:the most common community-acquired pneumonia with gram-negative bacilli as copathogens in stem cell transplant recipients withgraft-versus-host disease. Clin Infect Dis 2002; 35: 65964.
7 Meersseman W, Vandecasteele SJ, Wilmer A, Verbeken E,Peetermans WE, Van Wijngaerden E. Invasive aspergillosis incritically ill patients without malignancy. Am J Respir Crit Care Med2004; 170: 62125.
8 Hachem RY, Kontoyiannis DP, Boktour MR, et al. Aspergillus terreus:an emerging amphotericin B-resistant opportunistic mold in patientswith hematologic malignancies. Cancer 2004; 101: 1594600.
9 Steinbach WJ, Benjamin DK Jr, Kontoyiannis DP, et al. Infectionsdue to Aspergillus terreus: a multicenter retrospective analysis of 83cases. Clin Infect Dis 2004; 39: 19298.
10 Walsh TJ, Petraitis V, Petraitiene R, et al. Experimental pulmonaryaspergillosis due to Aspergillus terreus: pathogenesis and treatment ofan emerging fungal pathogen resistant to amphotericin B. J Infect Dis2003; 188: 30519.
11 Ascioglu S, Rex JH, de Pauw B, et al. Defining opportunistic invasivefungal infections in immunocompromised patients with cancer andhematopoietic stem cell transplants: an international consensus. ClinInfect Dis 2002; 34: 714.
12 Merz WG, Roberts GD. Algorithims for detection and identificationof fungi. In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, YolkenRH, eds. Manual of clinical microbiology, 7th edn. Washington DC:ASM Press, 1999: 116783.
http://infection.thelancet.com Vol 5 October 2005 619
Search strategy and selection criteria
PubMed was searched for English-language literature usingthe following terms: Aspergillus, aspergillosis, diagnosis,fungus, fungal, culture, histology, galactomannan,glucan, serology, antibody, PCR, molecular,metabolite, mannitol, and gliotoxin. Further relevantreferences, not identified by this strategy, were retrievedfrom the primary publications.
-
Review
13 Denning DW, Kibbler CC, Barnes RA. British Society for MedicalMycology proposed standards of care for patients with invasivefungal infections. Lancet Infect Dis 2003; 3: 23040.
14 Grocott RG. A stain for fungi in tissue sections and smears usingGomoris methenamine-silver nitrate technic. Am J Clin Pathol 1955;25: 97579.
15 Ruchel R, Schaffrinski M. Versatile fluorescent staining of fungi inclinical specimens by using the optical brightener Blankophor. J ClinMicrobiol 1999; 37: 269496.
16 Chander J, Chakrabarti A, Sharma A, Saini JS, Panigrahi D.Evaluation of Calcofluor staining in the diagnosis of fungal cornealulcer. Mycoses 1993; 36: 24345.
17 Choi JK, Mauger J, McGowan KL. Immunohistochemical detectionof Aspergillus species in pediatric tissue samples. Am J Clin Pathol2004; 121: 1825.
18 Kaufman L, Standard PG, Jalbert M, Kraft DE. Immunohistologicidentification of Aspergillus spp. and other hyaline fungi by usingpolyclonal fluorescent antibodies. J Clin Microbiol 1997; 35:220609.
19 Verweij PE, Smedts F, Poot T, Bult P, Hoogkamp-Korstanje JA, Meis JF. Immunoperoxidase staining for identification of Aspergillusspecies in routinely processed tissue sections. J Clin Pathol 1996; 49:798801.
20 De Vos MM, Nelis HJ. Detection of Aspergillus fumigatus hyphae bysolid phase cytometry. J Microbiol Methods 2003; 55: 55764.
21 Zimmerman RL, Montone KT, Fogt F, Norris AH. Ultra fastidentification of Aspergillus species in pulmonary cytology specimensby in situ hybridization. Int J Mol Med 2000; 5: 42729.
22 Hayden RT, Isotalo PA, Parrett T, et al. In situ hybridization for thedifferentiation of Aspergillus, Fusarium, and Pseudallescheria species intissue section. Diagn Mol Pathol 2003; 12: 2126.
23 Kontoyiannis DP, Lewis RE, May GS, Osherov N, Rinaldi MG.Aspergillus nidulans is frequently resistant to amphotericin B. Mycoses2002; 45: 40607.
24 Tarrand JJ, Lichterfeld M, Warraich I, et al. Diagnosis of invasiveseptate mold infections. Am J Clin Pathol 2003; 119: 85458.
25 Horvath JA, Dummer S. The use of respiratory-tract cultures in thediagnosis of invasive pulmonary aspergillosis. Am J Med 1996; 100:17178.
26 Sutton DA. Specimen collection, transport, and processing:mycology. In: Murray PR, Baron EJ, Jorgensen JH, Pfaller MA,Yolken RH, eds. Manual of clinical microbiology, 8th edn.Washington DC: ASM Press, 2003: 165967.
27 de Hoog GS, Guarro J, Gene J, Figueras MJ. Atlas of clinicalfungi, 2nd edn. Utrecht: Centraalbureau voor Schimmelcultures,2000.
28 Klich MA. Identification of common Aspergillus species. Utrecht:Centraalbureau voor Schimmelcultures, 2002.
29 Callister ME, Griffiths MJ, Nicholson AG, et al. A fatal case ofdisseminated aspergillosis caused by a non-sporulating strain ofAspergillus fumigatus. J Clin Pathol 2004; 57: 99192.
30 Latge JP, Kobayashi H, Debeaupuis JP, et al. Chemical andimmunological characterization of the extracellulargalactomannan of Aspergillus fumigatus. Infect Immun 1994; 62:542433.
31 Mennink-Kersten MA, Donnelly JP, Verweij PE. Detection ofcirculating galactomannan for the diagnosis and management ofinvasive aspergillosis. Lancet Infect Dis 2004; 4: 34957.
32 Marr KA, Balajee SA, McLaughlin L, Tabouret M, Bentsen C, Walsh TJ. Detection of galactomannan antigenemia by enzymeimmunoassay for the diagnosis of invasive aspergillosis: variablesthat affect performance. J Infect Dis 2004; 190: 64149.
33 Francis P, Lee JW, Hoffman A, et al. Efficacy of unilamellarliposomal amphotericin B in treatment of pulmonary aspergillosis inpersistently granulocytopenic rabbits: the potential role ofbronchoalveolar D-mannitol and serum galactomannan as markersof infection. J Infect Dis 1994; 169: 35668.
34 Bretagne S, Marmorat-Khuong A, Kuentz M, Latge JP, Bart-Delabesse E, Cordonnier C. Serum Aspergillus galactomannanantigen testing by sandwich ELISA: practical use in neutropenicpatients. J Infect 1997; 35: 715.
35 Boutboul F, Alberti C, Leblanc T, et al. Invasive aspergillosis inallogeneic stem cell transplant recipients: increasing antigenemia isassociated with progressive disease. Clin Infect Dis 2002; 34: 93943.
36 Becker MJ, Lugtenburg EJ, Cornelissen JJ, Van Der Schee C,Hoogsteden HC, De Marie S. Galactomannan detection incomputerized tomography-based broncho-alveolar lavage fluid andserum in haematological patients at risk for invasive pulmonaryaspergillosis. Br J Haematol 2003; 121: 44857.
37 Maertens J, Verhaegen J, Lagrou K, Van Eldere J, Boogaerts M.Screening for circulating galactomannan as a noninvasive diagnostictool for invasive aspergillosis in prolonged neutropenic patients andstem cell transplantation recipients: a prospective validation. Blood2001; 97: 160410.
38 Klont RR, Mennink-Kersten MA, Verweij PE. Utility of Aspergillusantigen detection in specimens other than serum specimens. ClinInfect Dis 2004; 39: 146774.
39 Stynen D, Goris A, Sarfati J, Latge JP. A new sensitive sandwichenzyme-linked immunosorbent assay to detect galactofuran inpatients with invasive aspergillosis. J Clin Microbiol 1995; 33:497500.
40 Verweij PE, Stynen D, Rijs AJ, de Pauw BE, Hoogkamp-Korstanje JA,Meis JF. Sandwich enzyme-linked immunosorbent assay comparedwith Pastorex latex agglutination test for diagnosing invasiveaspergillosis in immunocompromised patients. J Clin Microbiol 1995;33: 191214.
41 Dalle F, Lopez J, Caillot D, et al. False-positive results caused by cotton swabs in commercial Aspergillus antigen latex agglutination test. Eur J Clin Microbiol Infect Dis 2002; 21: 13032.
42 Swanink CM, Meis JF, Rijs AJ, Donnelly JP, Verweij PE.Specificity of a sandwich enzyme-linked immunosorbent assay fordetecting Aspergillus galactomannan. J Clin Microbiol 1997; 35:25760.
43 Kappe R, Schulze-Berge A. New cause for false-positive results withthe Pastorex Aspergillus antigen latex agglutination test. J ClinMicrobiol 1993; 31: 248990.
44 Hashiguchi K, Niki Y, Soejima R. Cyclophosphamide induces false-positive results in detection of aspergillus antigen in urine. Chest1994; 105: 97576.
45 Mennink-Kersten MA, Klont RR, Warris A, Op den Camp HJ,Verweij PE. Bifidobacterium lipoteichoic acid and false ELISAreactivity in aspergillus antigen detection. Lancet 2004; 363:32527.
46 Bennett JE, Kauffman C, Walsh T, et al. Forum report: issues in theevaluation of diagnostic tests, use of historical controls, and merits ofthe current multicenter collaborative groups. Clin Infect Dis 2003; 36(suppl 3): S12327.
47 Herbrecht R, Letscher-Bru V, Oprea C, et al. Aspergillusgalactomannan detection in the diagnosis of invasive aspergillosis incancer patients. J Clin Oncol 2002; 20: 1898906.
48 Maertens J, Verhaegen J, Demuynck H, et al. Autopsy-controlledprospective evaluation of serial screening for circulatinggalactomannan by a sandwich enzyme-linked immunosorbent assayfor hematological patients at risk for invasive aspergillosis. J ClinMicrobiol 1999; 37: 322328.
49 Maertens J, Van Eldere J, Verhaegen J, Verbeken E, Verschakelen J,Boogaerts M. Use of circulating galactomannan screening for earlydiagnosis of invasive aspergillosis in allogeneic stem cell transplantrecipients. J Infect Dis 2002; 186: 1297306.
50 Verweij PE, Weemaes CM, Curfs JH, Bretagne S, Meis JF. Failure todetect circulating Aspergillus markers in a patient with chronicgranulomatous disease and invasive aspergillosis. J Clin Microbiol2000; 38: 390001.
51 Husain S, Kwak EJ, Obman A, et al. Prospective assessment ofPlatelia Aspergillus galactomannan antigen for the diagnosis ofinvasive aspergillosis in lung transplant recipients. Am J Transplant2004; 4: 796802.
52 Kwak EJ, Husain S, Obman A, et al. Efficacy of galactomannanantigen in the Platelia Aspergillus enzyme immunoassay for diagnosisof invasive aspergillosis in liver transplant recipients. J Clin Microbiol2004; 42: 43538.
53 Fortun J, Martin-Davila P, Alvarez ME, et al. Aspergillus antigenemiasandwich-enzyme immunoassay test as a serodiagnostic method forinvasive aspergillosis in liver transplant recipients. Transplantation2001; 71: 14549.
54 Marr KA, Laverdiere M, Gugel A, Leisenring W. Antifungal therapydecreases sensitivity of the Aspergillus galactomannan enzymeimmunoassay. Clin Infect Dis 2005; 40: 176269.
620 http://infection.thelancet.com Vol 5 October 2005
-
Review
55 Maertens J, Theunissen K, Verbeken E, et al. Prospective clinicalevaluation of lower cut-offs for galactomannan detection in adultneutropenic cancer patients and haematological stem cell transplantrecipients. Br J Haematol 2004; 126: 85260.
56 Siemann M, Koch-Dorfler M, Gaude M. False-positive results inpremature infants with the Platelia Aspergillus sandwich enzyme-linked immunosorbent assay. Mycoses 1998; 41: 37377.
57 Ansorg R, van den Boom R, Rath PM. Detection of Aspergillusgalactomannan antigen in foods and antibiotics. Mycoses 1997; 40:35357.
58 Viscoli C, Machetti M, Cappellano P, et al. False-positivegalactomannan platelia Aspergillus test results for patients receivingpiperacillin-tazobactam. Clin Infect Dis 2004; 38: 91316.
59 Sulahian A, Touratier S, Ribaud P. False positive test for Aspergillusantigenemia related to concomitant administration of piperacillinand tazobactam. N Engl J Med 2003; 349: 236667.
60 Walsh TJ, Shoham S, Petraitiene R, et al. Detection ofgalactomannan antigenemia in patients receiving piperacillin-tazobactam and correlations between in vitro, in vivo, and clinicalproperties of the drug-antigen interaction. J Clin Microbiol 2004; 42:474448.
61 Singh N, Obman A, Husain S, Aspinall S, Mietzner S, Stout JE.Reactivity of platelia Aspergillus galactomannan antigen withpiperacillin-tazobactam: clinical implications based on achievableconcentrations in serum. Antimicrob Agents Chemother 2004; 48:198992.
62 FDA. Practice Caution in Using Bio-Rad Platelia Aspergillus EIA.http://www.fda.gov/cdrh/oivd/laboratory.html#tip8 (accessed Aug17, 2005).
63 Pazos C, Ponton J, Del Palacio A. Contribution of (1->3)-beta-D-glucan chromogenic assay to diagnosis and therapeutic monitoringof invasive aspergillosis in neutropenic adult patients: a comparisonwith serial screening for circulating galactomannan. J Clin Microbiol2005; 43: 299305.
64 Obayashi T, Yoshida M, Mori T, et al. Plasma (1>3)-beta-D-glucanmeasurement in diagnosis of invasive deep mycosis and fungalfebrile episodes. Lancet 1995; 345: 1720.
65 Mori T, Ikemoto H, Matsumura M, et al. Evaluation of plasma (1-3)-beta-D-glucan measurement by the kinetic turbidimetric Limulustest, for the clinical diagnosis of mycotic infections. Eur J Clin ChemClin Biochem 1997; 35: 55360.
66 Miyazaki T, Kohno S, Mitsutake K, et al. Plasma (1>3)-beta-D-glucan and fungal antigenemia in patients with candidemia,aspergillosis, and cryptococcosis. J Clin Microbiol 1995; 33:311518.
67 Odabasi Z, Mattiuzzi G, Estey E, et al. Beta-D-glucan as a diagnosticadjunct for invasive fungal infections: validation, cutoff,development, and performance in patients with acute myelogenousluekemia and myelodysplastic syndrome. Clin Infect Dis 2004; 39:199205.
68 Rylander R, Norrhall M, Engdahl U, Tunsater A, Holt PG.Airways inflammation, atopy, and (1>3)-beta-D-glucanexposures in two schools. Am J Respir Crit Care Med 1998; 158:168587.
69 Denning DW, Riniotis K, Dobrashian R, Sambatakou H. Chroniccavitary and fibrosing pulmonary and pleural aspergillosis: caseseries, proposed nomenclature change, and review. Clin Infect Dis2003; 37 (suppl 3): S26580.
70 Young RC, Bennett JE. Invasive aspergillosis. Absence of detectableantibody response. Am Rev Respir Dis 1971; 104: 71016.
71 Chan CM, Woo PC, Leung AS, et al. Detection of antibodies specificto an antigenic cell wall galactomannoprotein for serodiagnosis ofAspergillus fumigatus aspergillosis. J Clin Microbiol 2002; 40:204145.
72 Sambatakou H, Guiver M, Denning D. Pulmonary aspergillosis in apatient with chronic granulomatous disease: confirmation bypolymerase chain reaction and serological tests, and successfultreatment with voriconazole. Eur J Clin Microbiol Infect Dis 2003; 22:68185.
73 Kappe R, Schulze-Berge A, Sonntag HG. Evaluation of eight antibodytests and one antigen test for the diagnosis of invasive aspergillosis.Mycoses 1996; 39: 1323.
74 Schonheyder H. Pathogenic and serological aspects of pulmonaryaspergillosis. Scand J Infect Dis Suppl 1987; 51: 162.
75 Centeno-Lima S, de Lacerda JM, do Carmo JA, Abecasis M,Casimiro C, Exposto F. Follow-up of anti-Aspergillus IgG and IgAantibodies in bone marrow transplanted patients with invasiveaspergillosis. J Clin Lab Anal 2002; 16: 15662.
76 Holdom MD, Lechenne B, Hay RJ, Hamilton AJ, Monod M.Production and characterization of recombinant Aspergillusfumigatus Cu,Zn superoxide dismutase and its recognition byimmune human sera. J Clin Microbiol 2000; 38: 55862.
77 Weig M, Frosch M, Tintelnot K, et al. Use of recombinantmitogillin for improved serodiagnosis of Aspergillus fumigatus-associated diseases. J Clin Microbiol 2001; 39: 172130.
78 Yuen KY, Chan CM, Chan KM, et al. Characterization of AFMP1: anovel target for serodiagnosis of aspergillosis. J Clin Microbiol 2001;39: 383037.
79 Latge JP. Aspergillus fumigatus and aspergillosis. Clin Microbiol Rev1999; 12: 31050.
80 Strandberg GW. D-mannitol metabolism by Aspergillus candidus. J Bacteriol 1969; 97: 130509.
81 Wong B, Brauer KL, Tsai RR, Jayasimhulu K. Increased amountsof the Aspergillus metabolite D-mannitol in tissue and serum ofrats with experimental aspergillosis. J Infect Dis 1989; 160:95103.
82 Lewis RE, Wiederhold NP, Chi J, et al. Detection of gliotoxin inexperimental and human aspergillosis. Infect Immun 2005; 73:63537.
83 Yoo JH, Choi JH, Choi SM, et al. Application of nucleic acidsequence-based amplification for diagnosis of and monitoring the clinical course of invasive aspergillosis in patients with hematologic diseases. Clin Infect Dis 2005; 40: 39298.
84 Loeffler J, Hebart H, Cox P, Flues N, Schumacher U, Einsele H.Nucleic acid sequence-based amplification of Aspergillus RNA inblood samples. J Clin Microbiol 2001; 39: 162629.
85 Bretagne S. Molecular diagnostics in clinical parasitology andmycology: limits of the current polymerase chain reaction (PCR)assays and interest of the real-time PCR assays. Clin Microbiol Infect2003; 9: 50511.
86 Sanguinetti M, Posteraro B, Pagano L, et al. Comparison of real-time PCR, conventional PCR, and galactomannan antigendetection by enzyme-linked immunosorbent assay usingbronchoalveolar lavage fluid samples from hematology patients fordiagnosis of invasive pulmonary aspergillosis. J Clin Microbiol2003; 41: 392225.
87 Rantakokko-Jalava K, Laaksonen S, Issakainen J, et al.Semiquantitative detection by real-time PCR of Aspergillusfumigatus in bronchoalveolar lavage fluids and tissue biopsyspecimens from patients with invasive aspergillosis. J ClinMicrobiol 2003; 41: 430411.
88 Hendolin PH, Paulin L, Koukila-Kahkola P, et al. Panfungal PCRand multiplex liquid hybridization for detection of fungi in tissuespecimens. J Clin Microbiol 2000; 38: 418692.
89 Willinger B, Obradovic A, Selitsch B, et al. Detection andidentification of fungi from fungus balls of the maxillary sinus bymolecular techniques. J Clin Microbiol 2003; 41: 58185.
90 Paterson PJ, Seaton S, McLaughlin J, Kibbler CC. Development ofmolecular methods for the identification of aspergillus andemerging moulds in paraffin wax embedded tissue sections. MolPathol 2003; 56: 36870.
91 Costa C, Costa JM, Desterke C, Botterel F, Cordonnier C,Bretagne S. Real-time PCR coupled with automated DNAextraction and detection of galactomannan antigen in serum byenzyme-linked immunosorbent assay for diagnosis of invasiveaspergillosis. J Clin Microbiol 2002; 40: 222427.
92 Loeffler J, Hebart H, Brauchle U, Schumacher U, Einsele H.Comparison between plasma and whole blood specimens fordetection of Aspergillus DNA by PCR. J Clin Microbiol 2000; 38:383033.
93 Garcia ME, Blanco JL, Caballero J, Gargallo-Viola D.Anticoagulants interfere with PCR used to diagnose invasiveaspergillosis. J Clin Microbiol 2002; 40: 156768.
94 Loffler J, Hebart H, Schumacher U, Reitze H, Einsele H.Comparison of different methods for extraction of DNA of fungalpathogens from cultures and blood. J Clin Microbiol 1997; 35:331112.
http://infection.thelancet.com Vol 5 October 2005 621
-
Review
95 Muller FM, Werner KE, Kasai M, Francesconi A, Chanock SJ, Walsh TJ. Rapid extraction of genomic DNA from medicallyimportant yeasts and filamentous fungi by high-speed celldisruption. J Clin Microbiol 1998; 36: 162529.
96 Loeffler J, Hebart H, Bialek R, et al. Contaminations occurring infungal PCR assays. J Clin Microbiol 1999; 37: 120002.
97 Nierman W, Pain A, Anderson MJ, et al. Genomic sequence of thepathogenic and allergenic Aspergillus fumigatus. Nature (in press).
98 Chen SC, Halliday CL, Meyer W. A review of nucleic acid-baseddiagnostic tests for systemic mycoses with an emphasis onpolymerase chain reaction-based assays. Med Mycol 2002; 40: 33357.
99 Spiess B, Buchheidt D, Baust C, et al. Development of a LightCyclerPCR assay for detection and quantification of Aspergillus fumigatusDNA in clinical samples from neutropenic patients. J Clin Microbiol2003; 41: 181118.
100 Melchers WJ, Verweij PE, van den Hurk P, et al. General primer-mediated PCR for detection of Aspergillus species. J Clin Microbiol1994; 32: 171017.
101 Spreadbury C, Holden D, Aufauvre-Brown A, Bainbridge B, Cohen J.Detection of Aspergillus fumigatus by polymerase chain reaction. J Clin Microbiol 1993; 31: 61521.
102 Walsh TJ, Francesconi A, Kasai M, Chanock SJ. PCR and single-strand conformational polymorphism for recognition of medicallyimportant opportunistic fungi. J Clin Microbiol 1995; 33: 321620.
103 Rath PM, Ansorg R. Identification of medically important Aspergillusspecies by single strand conformational polymorphism (SSCP) of thePCR-amplified intergenic spacer region. Mycoses 2000; 43: 38186.
104 Hopfer RL, Walden P, Setterquist S, Highsmith WE. Detection anddifferentiation of fungi in clinical specimens using polymerase chainreaction (PCR) amplification and restriction enzyme analysis. J MedVet Mycol 1993; 31: 6575.
105 Martin C, Roberts D, van Der Weide M, et al. Development of a PCR-based line probe assay for identification of fungal pathogens. J ClinMicrobiol 2000; 38: 373542.
106 Turenne CY, Sanche SE, Hoban DJ, Karlowsky JA, Kabani AM.Rapid identification of fungi by using the ITS2 genetic region and anautomated fluorescent capillary electrophoresis system. J ClinMicrobiol 1999; 37: 184651.
107 de Aguirre L, Hurst SF, Choi JS, Shin JH, Hinrikson HP, Morrison CJ. Rapid differentiation of Aspergillus species from othermedically important opportunistic molds and yeasts by PCR-enzymeimmunoassay. J Clin Microbiol 2004; 42: 3495504.
108 Forbes BA. Introducing a molecular test into the clinicalmicrobiology laboratory: development, evaluation, and validation.Arch Pathol Lab Med 2003; 127: 110611.
109 Dimech W, Bowden S, Brestovac B, et al. Validation of assemblednucleic acid-based tests in diagnostic microbiology laboratories.Pathology 2004; 36: 4550.
110 Einsele H, Hebart H, Roller G, et al. Detection and identification offungal pathogens in blood by using molecular probes. J ClinMicrobiol 1997; 35: 135360.
111 Kami M, Fukui T, Ogawa S, et al. Use of real-time PCR on bloodsamples for diagnosis of invasive aspergillosis. Clin Infect Dis 2001;33: 150412.
112 Bretagne S, Costa JM, Marmorat-Khuong A, et al. Detection ofAspergillus species DNA in bronchoalveolar lavage samples bycompetitive PCR. J Clin Microbiol 1995; 33: 116468.
113 Bretagne S, Costa JM, Bart-Delabesse E, Dhedin N, Rieux C,Cordonnier C. Comparison of serum galactomannan antigendetection and competitive polymerase chain reaction for diagnosinginvasive aspergillosis. Clin Infect Dis 1998; 26: 140712.
114 Verweij PE, Meis JF, van den Hurk P, Zoll J, Samson RA, Melchers WJ. Phylogenetic relationships of five species of Aspergillusand related taxa as deduced by comparison of sequences of smallsubunit ribosomal RNA. J Med Vet Mycol 1995; 33: 18590.
115 OSullivan CE, Kasai M, Francesconi A, et al. Development andvalidation of a quantitative real-time PCR assay using fluorescenceresonance energy transfer technology for detection of Aspergillusfumigatus in experimental invasive pulmonary aspergillosis. J Clin Microbiol 2003; 41: 567682.
116 Bowman JC, Abruzzo GK, Anderson JW, et al. Quantitative PCRassay to measure Aspergillus fumigatus burden in a murine model ofdisseminated aspergillosis: demonstration of efficacy of caspofunginacetate. Antimicrob Agents Chemother 2001; 45: 347481.
117 Henry T, Iwen PC, Hinrichs SH. Identification of Aspergillus speciesusing internal transcribed spacer regions 1 and 2. J Clin Microbiol2000; 38: 151015.
118 Luo G, Mitchell TG. Rapid identification of pathogenic fungi directlyfrom cultures by using multiplex PCR. J Clin Microbiol 2002; 40:286065.
119 Zhao J, Kong F, Li R, Wang X, Wan Z, Wang D. Identification ofAspergillus fumigatus and related species by nested PCR targetingribosomal DNA internal transcribed spacer regions. J Clin Microbiol2001; 39: 226166.
120 Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versusamphotericin B for primary therapy of invasive aspergillosis. N Engl JMed 2002; 347: 40815.
121 Loeffler J, Kloepfer K, Hebart H, et al. Polymerase chain reactiondetection of aspergillus DNA in experimental models of invasiveaspergillosis. J Infect Dis 2002; 185: 120306.
122 Albelda SM, Talbot GH, Gerson SL, Miller WT, Cassileth PA. Role offiberoptic bronchoscopy in the diagnosis of invasive pulmonaryaspergillosis in patients with acute leukemia. Am J Med 1984; 76:102734.
123 Kahn FW, Jones JM, England DM. The role of bronchoalveolarlavage in the diagnosis of invasive pulmonary aspergillosis. Am J ClinPathol 1986; 86: 51823.
124 Einsele H, Quabeck K, Muller KD, et al. Prediction of invasivepulmonary aspergillosis from colonisation of lower respiratory tractbefore marrow transplantation. Lancet 1998; 352: 1443.
125 Levy H, Horak DA, Tegtmeier BR, Yokota SB, Forman SJ. The valueof bronchoalveolar lavage and bronchial washings in the diagnosis ofinvasive pulmonary aspergillosis. Respir Med 1992; 86: 24348.
126 von Eiff M, Zuhlsdorf M, Roos N, Hesse M, Schulten R, van de Loo J.Pulmonary fungal infections in patients with hematologicalmalignanciesdiagnostic approaches. Ann Hematol 1995; 70:13541.
127 Crystal RG, Reynolds HY, Kalica AR. Bronchoalveolar lavage. Thereport of an international conference. Chest 1986; 90: 12231.
128 McWhinney PH, Kibbler CC, Hamon MD, et al. Progress in thediagnosis and management of aspergillosis in bone marrowtransplantation: 13 years experience. Clin Infect Dis 1993; 17:397404.
129 Brown MJ, Worthy SA, Flint JD, Muller NL. Invasive aspergillosis inthe immunocompromised host: utility of computed tomography andbronchoalveolar lavage. Clin Radiol 1998; 53: 25557.
130 Musher B, Fredricks D, Leisenring W, Balajee SA, Smith C, Marr KA. Aspergillus galactomannan enzyme immunoassay andquantitative PCR for diagnosis of invasive aspergillosis withbronchoalveolar lavage fluid. J Clin Microbiol 2004; 42: 551722.
131 Yu VL, Muder RR, Poorsattar A. Significance of isolation ofAspergillus from the respiratory tract in diagnosis of invasivepulmonary aspergillosis. Results from a three-year prospective study.Am J Med 1986; 81: 24954.
132 Hebart H, Loffler J, Meisner C, et al. Early detection of Aspergillusinfection after allogeneic stem cell transplantation by polymerasechain reaction screening. J Infect Dis 2000; 181: 171319.
133 Jones BL, McLintock LA. Impact of diagnostic markers on earlyantifungal therapy. Curr Opin Infect Dis 2003; 16: 52126.
622 http://infection.thelancet.com Vol 5 October 2005
-
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.