Kuliah Fisiologi Faring Dan Laring - Dr Ratna Kusumawati
28
Physiology of Pharynx Ratna Kusumawati
-
Upload
anindityap -
Category
Documents
-
view
45 -
download
6
description
Fisiologi Blok THT
Transcript of Kuliah Fisiologi Faring Dan Laring - Dr Ratna Kusumawati

Physiology of PharynxRatna Kusumawati




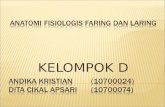
PHARYNX
- Pharynx is a conical fibromuscular tube forming upper part of air and food passages.
- Divisions: -Nasopharynx
- Oropharynx
- laryngopharynx.
- Structure of Pharyngeal wall from outwards 4 layers :
Mucous membrane
Pharyngeal aponeurosis
Muscular coat
Buccopharyngeal fascia.

Functions
• As a conduit for passage of food and air.
• Helps in the pharyngeal phase of deglutition.
• Helps in appreciation of taste:taste bubs present on the base of tongue,soft palate,anterior pillars &post pharyngeal walls.
• Provides local defence & immunity.
• Drainage mucus from nasopharynx
• Reflex action


Nerve supply: lesser palatine branches of sphenopalatine ganglion(5th CN) & glossopharyngeal nerve provide sensory nerve supply.

Enlarged tonsils

Functions
• Protective role & act as sentinels at the portal of air & food passages.
• Crypts : increase the srface area for contact with the foreign substances.
• Removed when themselves become seat of infection.



Basic Functions
•Protection
•Respiration
•Phonation
•Closure of glottis
7/15/2012 www.nayyarENT.com 15
Closure of glottis – helps to increase intrathoracic and intraabdominalpressure and aids in lifting, digging, defecation, vomiting, urination orchildbirth

Protection
• Acts as a sphincter• Closure of the laryngeal • Closure of the glottis• Cessation of respiration• Cough relfex, expulsion of secretions and foreign
bodies
• 3 Sphincteric tiers of airway protection:• Contraction of superior division of the thyroarytenoid
muscles• Contraction of middle thyroarytenoid fibers• Contraction of inferior division of thyroarytenoid
7/15/2012 www.nayyarENT.com 16
Prevents entrance of ANYTHING but AIR into the lung

Protection
7/15/2012 www.nayyarENT.com 17
Unilateral SLN paralysis may lead to aspiration (failure of ipsilateral cord closure) despite integrity of both RLNs*(one SLN DOES NOT produce simultaneous activation of the contralateral adductor musculature)3 Sphincteric tiers of airway protection:1.Contraction of superior division of the thyroarytenoid muscles contained in the aryepiglottic folds 2.Contraction of middle thyroarytenoid fibers in false cords 3.Contraction of inf. Division of thyroarytenoid at the level of true cord (MOST SIGNIFICANT barrier to aspiration owing to the upturned border of the cord margin)SLN stimulation – produces strong laryngeal ADDUCTOR response and inhibition of laryngeal abductor activity, resulting in various degrees of reflex apnea.Laryngeal spasm – mediated solely by SLN

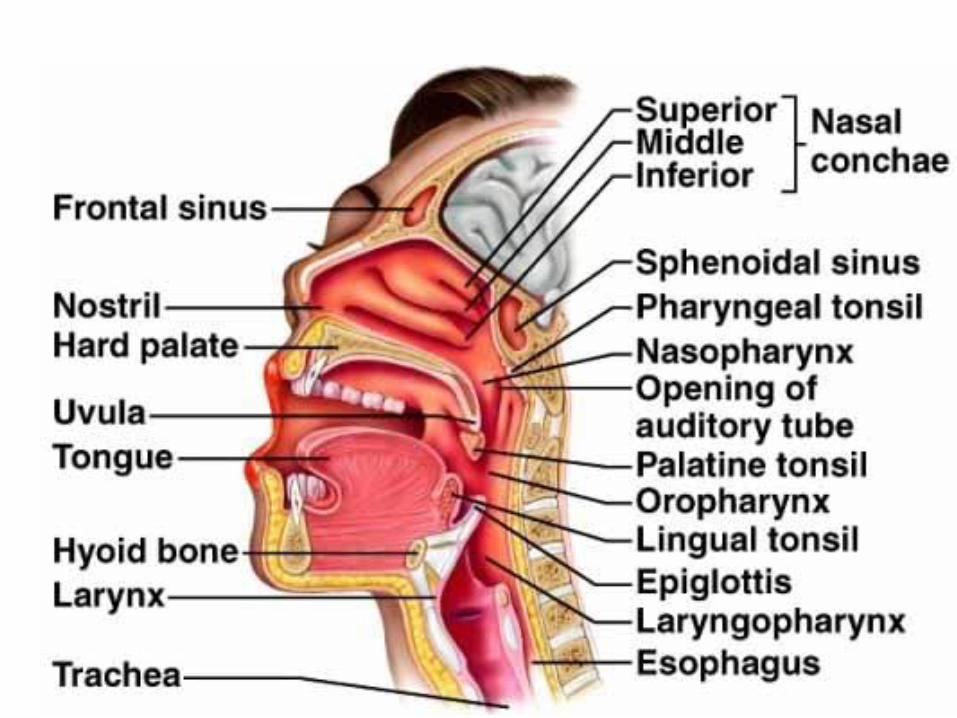
Phonation in brief
• Voice produced by vibration of the vocal cords
• Fundamental tone produced at the larynx
• Modified by resonating chambers of the upper aerodigestive tract
7/15/2012 www.nayyarENT.com 18


Anatomy and Physiology of Normal Swallowing
Phases of Swallowing• Oral Phase
• Pharyngeal Phase
• Esophageal Phase
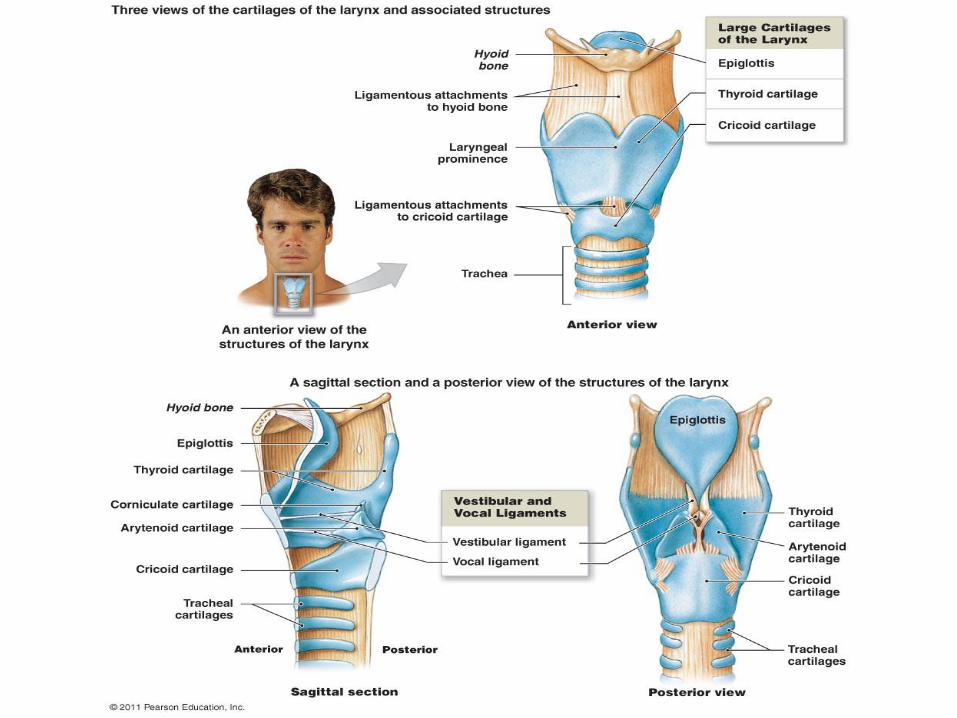
Moving bolus from mouth to stomach
• Three phases• Facilitated by saliva,
mucous secretions• Involves mouth, pharynx,
esophagus
1. Buccal phase Voluntary Moves bolus to
oropharynx

2. Pharyngeal phase
- Involuntary
- Receptors in oropharynx stimulate medulla and pons to:
1. Block mouth with tongue2. Block nasopharynx with
soft palate
3. Raise larynx to seal epiglottis, blocking airways
4. Relax upper esophageal sphincter
• Bolus is moved through pharynx into esophagus

3. Esophageal stage• Upper esophageal
sphincter closes• Gastroesopaheal sphincter
opens• Esophagus controls
involuntary peristaltic movement
• Epiglottis reopens• Bolus moves from
esophagus to stomach

A=voluntary initialion of the swallow by tongueB=triggering of the pharyngeal swallowC=arrival of the bolus in the valleculae- valleculae - where base of tongue, epiglottis, and aryepiglottic folds joinD=tongue base retraction to the anteriorly moving pharyngeal wallE=bolus in the cervical esophagus and cricopharyngeal regionLogemann, 1998



Anatomy and Physiology of Normal Swallowing
Abnormal Swallowing
Dysphagia - difficulty in swallowing
Abnormal Swallowing- dysphagia - difficulty in swallowing - occurs only during act of swallowing- generally results from neuromuscular or structural changes in oral cavity, pharynx, or larynx-most frequent causes include developmental or traumatic neuromotordisorders and congenital anatomical defects-in adults, most commonly associated with strokes, neurologic disease, head and neck cancer surgery, radiation Rx for head and neck cancer, traumatic brain injury- of interest to mote that many of these causes are also causes or communication disorders- not surprising since using same structures

CAUSES OF DYSPHAGIA
• Structural abnormalities• Oesophageal neoplasm• Peptic stricture• Incarcerated hiatal hernia
• Motility disorders• Achalasiaetc