KNOWLEDGE AND PRRACTICE OF TRADITIONAL MEDICINE …
84
KNOWLEDGE AND PRRACTICE OF TRADITIONAL MEDICINE AMONG PREGNANT MOTHERS ATTENDING KIBAGABAGA DISTRICT HOSPITAL, RWANDA Eric Nyankieya Kinara MPH/0313/13 A Thesis Submitted in Partial Fulfillment for the Award of a Degree in Master of Public Health (International Health Option) of Mount Kenya University MARCH 2017
Transcript of KNOWLEDGE AND PRRACTICE OF TRADITIONAL MEDICINE …
KNOWLEDGE AND PRRACTICE OF TRADITIONAL MEDICINEAMONG PREGNANT MOTHERS ATTENDING KIBAGABAGA
DISTRICT HOSPITAL, RWANDA
Eric Nyankieya Kinara
MPH/0313/13
A Thesis Submitted in Partial Fulfillment for the Award of a Degree inMaster of Public Health (International Health Option) of Mount Kenya
University
MARCH 2017

DECLARATION
This thesis is my original work and has not been presented for a degree in any other
University or for any other award.
Eric Nyankieya Kinara
MPH/0313/13
Sign ____________________ Date ___/_____/_____
I confirm that the work reported in this thesis was carried out by the candidate under mysupervision.
Dr Raymond Muganga, M PHARM, PhD
Sign ____________________ Date ___/_____/_____
2

DEDICATION
This piece of work is dedicated to my wife Olper Kerubo and my daughter Bilha Keza
Nyanckoka.
3

ACKNOWLEDGEMENT
I thank Dr Raymond Muganga and Dr Cathie Kansiime and for their support during the
research and all participants’ nurses, students and the midwives at the Antenatal Clinic and all
the pregnant women for their time and sharing their knowledge and ideas with us.
4

ABSTRACT
The main purpose of this study is to assess the knowledge and practice of traditionalmedicine among pregnant women. It is thus guided by the following specific objectives: todetermine the prevalence of pregnant mothers using traditional medicine at Kibagabagahospital, to determine the level of knowledge of traditional medicine by pregnant women atKibagabaga hospital, to identify the purpose of traditional medicines used by pregnantwomen at Kibagabaga hospital. This study’s finding will to promoting rational use of herbalmedicines among mothers, Community mobilization should include the husbands,community and religious leaders in order to change the orientation of the community andcreate awareness on the risks involved in indiscriminate use of herbal medicines duringpregnancy and the need to get herbal drug use information from health practitioners. Theresearcher was therefore being guided by a descriptive cross sectional study design where atarget population of 179 pregnant women from whom a sample of 123 women wererandomly selected by the use of Solvin’s formula. A structured questionnaire and In Depthinterview were used get quantitative and qualitative information in regarding to knowledgeand practice about traditional medicine in pregnancy. Data was categorized, coded and thenentered into excel, and then imported into SPSS Version 21 to perform statistical analyses.The study findings indicated that the prevalence of traditional medicine usage among thepregnant women was 31%.additionally the findings indicated that the level of knowledge andpractice among the respondents were good. The study therefore recommended that healthcareproviders should be aware of the common traditional medicines used and the need to knowwith evidence-based research regarding potential benefits or harmful side effects of themedications. Community mobilization is needed to ensure that information on the risks andsafety of traditional medicines to the fetus and mother in pregnancy are well known by thewomen.
5

TABLE OF CONTENTS
DECLARATION.......................................................................................................................ii
DEDICATION..........................................................................................................................iii
ACKNOWLEDGEMENT........................................................................................................iv
ABSTRACT..............................................................................................................................v
TABLE OF CONTENTS..........................................................................................................vi
LIST OF FIGURES..................................................................................................................ix
LIST OF TABLES.....................................................................................................................x
LIST OF ACRONYMS AND ABBREVIATIONS.................................................................xii
DEFINITION OF KEY TERMS............................................................................................xiii
CHAPTER ONE: INTRODUCTION........................................................................................1
1.0 Introduction......................................................................................................................1
1.1 Background of the study..................................................................................................1
1.2 Problem statement............................................................................................................2
1.3 Objectives of the Study....................................................................................................3
1.3.1 General Objectives....................................................................................................3
1.3.2 Specific Objectives....................................................................................................5
1.4 Research Questions..........................................................................................................5
1.5 Significance of the Study.................................................................................................5
1.6. Limitations of the Study..................................................................................................7
1.7. Scope of the Study..........................................................................................................7
1.7.1 Geographical scope...................................................................................................7
6

1.7.2 Time scope.................................................................................................................8
1.7.3 Content scope............................................................................................................8
1.8 Organization of the Study................................................................................................8
CHAPTER TWO: LITERATURE REVIEW..........................................................................10
2.0 Introduction....................................................................................................................10
2.1 Theoretical Literature Review.......................................................................................10
2.1.1 Complementary and Alternative Medicine (CAM).................................................10
2.1.2 Traditional Medical Practitioner..............................................................................11
2.1.3 Advantages of TM...................................................................................................12
2.1.4 Disadvantages of TM..............................................................................................13
2.1.4 Traditional Medicine Usage....................................................................................15
2.1.5 Herbal Remedies Efficacy, Safety, and Regulation.................................................17
2.2 Empirical Literature Review..........................................................................................22
2.3 Critical Literature and Gap Identification......................................................................25
2.4 Theoretical Framework..................................................................................................27
2.4.1 Monopolistic Health Care Model............................................................................27
2.4.2 Tolerant (Co-existence) Health Care Model............................................................28
2.4.3 Parallel (inclusive) or Dual Health Care Model......................................................28
2.4.4 Integrative Health Care Model................................................................................29
2.4.5 Traditional Model of Health....................................................................................29
2.5 Conceptual Framework..................................................................................................32
2.6 Summary........................................................................................................................33
CHAPTER THREE: RESEARCH METHODOLOGY..........................................................34
7

3.0 Introduction....................................................................................................................34
3.1 Research design..............................................................................................................34
3.2Target Population............................................................................................................34
3.3 Sample Design...............................................................................................................34
3.3.1 Sample size..............................................................................................................35
3.3.2 Sampling Technique................................................................................................35
3.4 Data Collection Methods...............................................................................................36
3.4.1 Data Collection Instruments....................................................................................36
3.4.2 Administration of Data Collection Instruments.......................................................37
3.4.3 Reliability and validity............................................................................................37
3.5 Data analysis Procedure.................................................................................................38
3.6 Ethical Consideration.....................................................................................................39
CHAPTER FOUR: RESEARCH FINDINGS AND DISCUSSION.......................................40
4.0 Introduction....................................................................................................................40
4.1 Demographic Characteristics of Respondents...............................................................40
4.1.1 Socio-Demographic Characteristic of Respondents................................................41
4.2 Presentation of Findings.................................................................................................42
4.2.1 Prevalence of TM usage among pregnant women..................................................42
4.2.2 Knowledge of TM among pregnant women............................................................43
4.2.3 Practice of Traditional medicine among pregnant women......................................45
4.2.4 Sources of herbal medicines....................................................................................46
4.2.5 Source of information regarding traditional medicine............................................47
4.2.6 Factors influencing pregnant women knowledge and practice regarding TM........49
8

4.2.7 Correlation between socio-demographic, Social-cultural, Social economic
characteristics and TM use among pregnant women.......................................................51
Qualitative Analysis Results................................................................................................52
4.2.8 Level of practice among pregnant women who used Traditional medicine............52
4.2.9 Reasons for traditional medicine usage during pregnancy......................................53
4.2.10 Stage of pregnancy at which women mostly use TM............................................54
4.2.11 Risk of using Traditional medicine........................................................................55
4.2.11 Suggestions for reducing TM use during pregnancy.............................................55
4.2.12 Herbal medicine used by pregnant women...........................................................56
CHAPTER FIVE: SUMMARY, CONCLUSION AND RECOMMENDATIONS.................57
5.0 Introduction....................................................................................................................57
5.1 Summary of Findings.....................................................................................................57
5.1.1 Objective i: Prevalence of Traditional medicine usage among pregnant women. . .57
5.1.2 Objective ii: Level of Knowledge regarding TM by pregnant women...................57
5.1.3 Objective iii: Level of practice regarding TM by pregnant women........................58
5.2 Conclusion.....................................................................................................................58
5.3 Recommendations..........................................................................................................59
5.4 Suggestions for further study.........................................................................................59
REFERENCES........................................................................................................................61
APPENDIX I: QUESTIONNAIRE.........................................................................................71
APPENDIX II: IN-DEPTH INTERVIEW GUIDE.................................................................73
9

LIST OF FIGURES
Figure 2.1, Conceptual framework..........................................................................................32
Figure 4.2: Source of tradition medication..............................................................................43
Figure 4.3: Source of information on tradition medication.....................................................44
10

LIST OF TABLES
Table4.1Socio-Demographic Characteristic of Respondents..................................................41
Table 4.2: Prevalence of Traditional medicine usage..............................................................42
Table 4.3: Knowledge of Traditional medicine among pregnant women................................43
Table 4.4: Level of Knowledge regarding Traditional medicine.............................................44
Table 4.5: Distribution of responses on Practice.....................................................................45
Table 4.9: Reasons for traditional medicine usage during pregnancy.....................................53
Table 4.10: Stage of pregnancy at which women mostly use TM..........................................54
Table 4.11: Risk of using TM among pregnant women...........................................................55
Table4.12: Responses on common herbal medicine used by pregnant women.......................56
11
LIST OF ACRONYMS AND ABBREVIATIONS
CAM : Complementary and Alternative Medicine
CHW : Community Health Workers
DHHS : Department of Health and Human Services
FDA : Food and Drug Administration
GMP : Good Manufacturing Procedure
OTC : Over the Counter
PHC : Primary Health Care
TAM : Traditional African Medicine
TBA : Traditional Birth Attendants
TH : Tradition Healer
TM : Traditional Medicine
TMP : Traditional Medical Practitioner
WHO : World Health Organization
12

DEFINITION OF KEY TERMS
Knowledge: Specific information about traditional medicine that is perceived discovered of
learned through study.
Practice: The habitual or customary act of using or utilization Tradition medicine substances
use.
Traditional Medicine: These are fresh juices, gums, fixed oils, essential oils, and dry
powders of herbs processed locally for treatment of various illness.
13
CHAPTER ONE: INTRODUCTION
1.0 Introduction
This chapter deals with a background of the study such as general overview of traditional
medicine, problems and challenges face in Rwanda significance scope, limitation and
organization of the study.
1.1 Background of the study
The sick, just like the poor, will always be present in the world. In sub-Saharan Africa where
you may find some of the world´s poorest population, there exist also a high burden of
disease with huge rate of morbidity and mortality. In resource poor settings traditional
medicine (TM) has proved to be a useful resource which could be exploited to tackle some of
the health problems in the community (Ernst, 2000).
Traditional medicine comprises knowledge systems that developed over generations within
various societies before the era of modern medicine. This is particularly important in African
countries; where up to 80% of the population relies on traditional medicine for their primary
health care needs. When adopted outside of its traditional culture, traditional medicine is
often called complementary or alternative medicine (WHO, 2000), especially at a time when
Africa faces serious problems in the health systems including skilled worker migration and
brain drain (Parker, 2009). Traditional medicine has been used by Africans for the
prevention, diagnosis and treatment of social, mental and physical ailments of different
origins before and even after the advent of conventional medicine (WHO, 2004).
Complementary medicine is alternative medicine used together with conventional medical
treatment in a belief, not proven by using scientific methods, that it "complements" the
treatment (Ernst, 2000).
1
Knowledge on indigenous medicine is generally transmitted orally through a community,
family and individuals until "collected". Within a given culture, elements of indigenous
medicine knowledge may be diffusely known by many, or may be gathered and applied by
those in a specific role of healer such as (traditional birth attendant) midwife. Three factors
legitimize the role of the healer their own beliefs, the success of their actions and the beliefs
of the community. When the claims of indigenous medicine become rejected by a culture,
generally three types of adherents still use it those born and socialized in it who becomes
permanent believers, temporary believers who turn to it in crisis times, and those who only
believe in specific aspects, not in all of it (Ernst, 2000).
Pregnancy is a condition associated with immense physiological alterations resulting in many
pregnancy- related problems, including nausea, vomiting, constipation, and heartburn
(Lindzon et al., 2011). Despite the fact that evidence on the safety profile of herbal products
is inadequate to substantiate their use in pregnancy, it is increasingly used by expectant
mothers. The prevalence of herbal medicine utilization in pregnancy ranges between 7% and
55% in different geographical, social and cultural settings, and ethnic groups (Dugoua,
2010).
1.2 Problem statement
In as much as it is generally accepted that traditional medicine and traditional health products
have many benefits in primary healthcare. A hospital based study in South Africa compared
women reporting use of traditional medicine with those not reporting such use, and found
that traditional medicine use in pregnancy was relatively common (55% of delivering
women). Furthermore, a higher cesarean section rate was observed in women who used
traditional medicine compared to women who did not use traditional medicine (39% vs.
2

22%) (Mabina, 1997), a higher frequency of meconium-stained fluid in women who used
traditional medicine during pregnancy compared to those who did not (56% vs. 15%) was
also noted. This is similar to the perceptions of the Rwandan medical providers, who have
reported that there is a high rate of abnormally bright green meconium staining amongst
women who had used phytomedicine during their pregnancy; (Republic of Rwanda, 2012).
Rwanda as one African countries with a history of using traditional medicine for a variety of
medical and non-medical reasons and there is little understanding about its practice in
pregnancy in existing literature. Questions regarding the efficacy, safety and quality of
traditional medicine and traditional health products are important issues that are gaining
attention in research. For policies regarding traditional medicine ultimately geared towards
integration of traditional medicine into the National Health Service to be formed and
implemented, users opinions and perception s need to be sampled so that policies taken will
be able to protect the interest of those making use of this health care option. It is based on
this that the study was aimed to determine the knowledge and practice of traditional medicine
among pregnant mothers in Kibagabaga hospital, a referral of urban rural community in
Gasabo District of Kigali city Province, Rwanda.
1.3 Objectives of the Study
The study has both general and specific objectives.
1.3.1 General Objectives
To determine knowledge and practice of traditional medicine among pregnant women
attending Kibagabaga District hospital.
3
1.3.2 Specific Objectives
This study was guided by the following objectives;
i. To determine the prevalence of pregnant mothers using traditional medicine at
Kibagabaga hospital.ii. To determine the level of knowledge of traditional medicine by pregnant women at
Kibagabaga hospital.iii. To identify the purpose of traditional medicines used by pregnant women at
Kibagabaga hospital.
1.4 Research Questions
The study sought to answer the following research questions;
i. What is the prevalence of pregnant mothers using traditional medicine at
Kibagabaga hospital?ii. What is the level of knowledge of traditional medicine by pregnant women at
Kibagabaga hospital?iii. What are the purposes of traditional medicines used by pregnant women at
Kibagabaga hospital?
1.5 Significance of the Study
In order to aid the process of modernization of traditional medicine the researcher
recommends that the government of Rwanda should put in place educational, professional
and legal frameworks to govern the practice. Traditional medicine in Rwanda should adopt
modern scientific approaches in their practices. This entails that they use traditional medicine
products and therapeutic techniques which are effective and safe and that are applicable for
specific indications. Research in traditional medicine using biomedical techniques should be
fostered so that practice of traditional medicine will be backed by evidence from research.
Practitioner of traditional medicine, policy makers and policy planers within and outside the
4

ministry of public health should take steps to ensure quality and safety of traditional
medicine in Rwanda in order to protect both the practitioners and users of traditional
medicine. This could be achieved by setting the appropriate frameworks for registering and
regulating traditional medicine in the country as well as making sure that traditional medicine
practice meets minimum levels of adequate knowledge, skills and awareness of indications
and contraindications.
This study is also beneficial among healthcare workers and instructors to be aware of this
possibility and routinely inquire about use of traditional for self-medication, on the effective
dissemination of information on the proper use of herbal medicines that include its proper
indication and use and possible toxicities. The study’s findings improved knowledge and
practice traditional medicine as well provided preliminary information for further researchers
who would wish to investigate on traditional medicine.
At the end of the study, the study finding will help the international organizations to fund
more of the research to investigate more on traditional medicine practice and knowledge and
any related studies. On the other international health partners such as WHO, UNICEF, The
World Bank and USAID need to tailor programs and policies to increase accessibility and
usage of biomedicine among the populace in this part of the world especially the poor and
vulnerable like the elderly, women and children.
To promoting rational use of herbal medicines among mothers, Community mobilization
should include the husbands, community and religious leaders in order to change the
orientation of the community and create awareness on the risks involved in indiscriminate
use of herbal medicines during pregnancy and the need to get herbal drug use information
from health practitioners.
5

1.6. Limitations of the Study
This study was subject to several limitations. Like all self reported exposure assessments,
under reporting was very likely, especially in our environment where patients, for fear of
rebuke by their physicians may down play their use of medicines not prescribed by their
doctors, to avoid all these limitations the researcher and his team explained, reassured the
respondent and informed the doctors and nurses and research team as a whole on how to
handle them.
1.7. Scope of the Study
The scope of the study covered the geographical location of the hospital, the content scope
which deals with the discipline covered and duration to carry out this research.
1.7.1 Geographical scope
This study was done in Rwanda, a country located in the East Africa where traditional
medicine forms a major part of health care system. Rwanda is known to be a land of a
thousand hills; a country of wildlife gorillas, Rwanda borders Congo to the west Tanzania to
the east, Burundi to the south and Uganda partly to the north. The health system model
operating in Rwanda is the dual health system with a predominant allopathic health facility
and an overwhelming presence of traditional medicine (Ministry of Health, Republic of
Rwanda). HMIS Health Facilities database (2013).The national health system comprises both
the private and public sector with the public sector as the principal provider of health
services. Kibagabaga hospital is one of the public sector facility in the country located in
Gasabo District, Kigali Province, Rwanda as shown in the geographical map in appendix
VIII.
6

1.7.2 Time scope
The period of study was three month from September to November 2016.
1.7.3 Content scope
The subject was focusing on maternal and child health, Newborn health and survival are
closely linked to care the mother receives before and during pregnancy, childbirth, and the
postnatal period. Throughout the continuum of care, the period with the highest risk of death
and disability for both mothers and newborns is labor, birth, and the first few hours after
birth. Complications and lack of care at this crucial time has consequences for mothers and
babies Herbal use among pregnant women is on an increasing trend which raises concerns of
safety that are attributed to the herbal ingredients itself. Most of them procured in their crude
forms although some pharmaceutical prepackaged forms also exist and are available over the
counter .i.e. determining knowledge & practice of traditional medicine amongst pregnant
mothers.
1.8 Organization of the Study
This research report consists of five chapters. Chapter one, is the introduction were
background of the study, problem statement, purpose of the study, research objectives,
research questions, significance of the study, limitations of the study, and the scope of the
study are discussed. It is then followed by chapter two, which presents a literature review
which includes theoretical review, empirical review, conceptual framework, critical review of
the existing literature related to this study, and the summary of the literature reviewed
In chapter three, the research methodology is presented: It comprises the introduction,
research design, target population, sample design, sample size data collection methods, data
collection instruments, administration of data collection instrument, reliability and validity,
7

data analysis procedure and ethical considerations. Chapter four presents research findings
and discussions of the findings of the study. This is followed by chapter five, which presents
the summary of findings, conclusions and recommendations of the study.
8

CHAPTER TWO: LITERATURE REVIEW
2.0 Introduction
This chapter highlights the theoretical aspect of the study in that reviewing what other people
are saying about traditional medicine in pregnancy, studies already done on TM and finally
formulation of conceptual framework.
2.1 Theoretical Literature Review
2.1.1 Complementary and Alternative Medicine (CAM)
Complementary and Alternative Medicine (CAM) is a group of diverse medical and
healthcare systems, therapies and products that are not presently considered to be an integral
part of conventional medicine (WHO, 2002). A therapy is generally considered to be
“complementary” when it is used in addition to conventional treatments. It is considered
“alternative” when it is used instead of conventional treatment. Conventional treatments are
defined as those that are widely accepted and practiced by the mainstream medical
community. CAM is the term for medical products and practices that are not part of standard
care. Standard care is what medical doctors, doctors of osteopathy, and allied health
professionals, such as nurses and physical therapists, practice, Alternative medicine is used in
place of standard medical care. Traditional medicine covers a wide variety of therapies and
practices which vary from country to country and region to region. In some countries, it is
referred as "alternative" or complementary" medicine (CAM)
Forms of Traditional medication involve herbal medicines, animal parts and minerals,
Finished, medicinal products that contain as active ingredients aerial or underground parts of
plants, or other plant material, or combinations thereof, whether in the crude state or as plant
preparations. Plant material includes juices, gums, and fatty oils, essential oils, and any other
9

substances of this nature. Herbal medicines may contain excipients in addition to the active
ingredients (Barnes et al, 2007) Medicines containing plant material combined with
chemically defined active substances, including chemically defined, isolated constituents of
plants, are not considered to be herbal medicines.
Exceptionally, in some countries herbal medicines may also contain, by tradition, natural
organic or inorganic active ingredients which are not of plant origin. On the other hand,
complementary health approaches: including acupuncture, Ayurveda, biofeedback, chelation
therapy, chiropractic or osteopathic manipulation, cranio-sacral therapy, energy healing
therapy, guided imagery, herbs and other non-vitamin supplements, hypnosis, homeopathy,
massage, meditation (mantra, mindfulness, and spiritual), Alexander technique, Feldenkreis,
Pilates, Trager psychophysical integration, naturopathy, progressive relaxation, special diets,
traditional healers, and yoga (with meditation or deep breathing), tai chi, and qi gong
exercises. (Barnes et al, 2007).
2.1.2 Traditional Medical Practitioner
Majority of the traditional herbal medicines used in Africa are provided by practitioners who
live within the communities, trusted over time and are often willing to assist the patients with
their knowledge and skills, sometimes at minimal costs. Most of these herbal medicines are
procured in their crude forms although some pharmaceutical prepackaged forms also exist
and are available over the counter (OTC).
The traditional medical practitioner (TMP) or Traditional Healer (TH) is described as a
person who is recognized by the community in which he lives as competent to provide health
care by using vegetable, animal and mineral substances and certain other methods (WHO,
2002); serving as the nurse, pharmacist, physician, dentist, mid-wife, dispenser etc. The
10

specialists include herbalists, bone setters, traditional psychiatrists, traditional pediatricians,
traditional birth attendants (TBA), occult practitioners, herb sellers, general practitioners, etc;
they are certainly more readily available, accessible and approachable than the orthodox
physicians while their services are much more affordable than modern medical facilities.
No doubt, the traditional healers, diagnosing and managing various common diseases at
primary health center level, with various herbal dosage forms namely, concoctions,
decoctions, infusions, dried powders, ointments, tinctures and macerates, are much closer to
the community than the orthodox doctors who are mainly found in urban healthcare
locations. Although most governments in Africa are yet to pass into law, the official
recognition of their practices (like in China, Japan, India, Thailand and Korea), the
practitioners have been generally acknowledged excellent at PHC level in the areas of bone
setting, psychotherapy in psychiatry, hydrotherapy as well as obstetrics and gynecology (by
the TBA). However, there has been more interest expressed recently in the effects of some of
the medicinal plants of Africa. "The pharmaceutical industry has come to consider traditional
medicine as a source for identification of bio-active agents that can be used in the preparation
of synthetic medicine" Parker and Roope, 2009). Pharmaceutical industries are looking into
the medicinal effects of the most commonly and widely used plants to use in drugs. It's
apparent that there are some things that can be learned from traditional African practice.
2.1.3 Advantages of TM
Herbs cost much less than prescription medications. Research, testing, and marketing add
considerably to the cost of prescription medicines. Most herbal medicines are well tolerated
by the patient, with fewer unintended consequences than pharmaceutical drugs. Herbs
typically have fewer side effects than traditional medicine, and may be safer to use over time.
11

On the other hand patients turn to TM/CAM for complementary care is the increasing cases
of chronic and debilitating diseases for which there is no cure (NIH, 2004). Herbs tend to be
inexpensive compared to drugs. Yet another advantage of herbal medicines is their
availability. Herbs are available without a prescription. You can grow some simple herbs,
such as peppermint and chamomile, at home. In some remote parts of the world, herbs may
be the only treatment available to the majority of people (Parker and Roope, 2009).
2.1.4 Disadvantages of TM
Herbs are not without disadvantages, and herbal medicine is not appropriate in all situations.
Inappropriate for many conditions: - Modern medicine treats sudden and serious illnesses and
accidents much more effectively than herbal or alternative treatments. An herbalist would not
be able to treat serious trauma, such as a broken leg, nor would he be able to heal
appendicitis or a heart attack as effectively as a conventional doctor using modern diagnostic
tests, surgery, and drugs.
Herbal medicine is the very real risks of doing yourself harm through self-dosing with herbs.
While you can argue that the same thing can happen with medications, such as accidentally
overdosing on cold remedies, many herbs do not come with instructions or package inserts.
Harvesting herbs in the wild is risky, if not foolhardy, yet some people try to identify and
pick wild herbs. They run a very real risk of poisoning themselves if they don't correctly
identify the herb, or if they use the wrong part of the plant. Herbal treatments can interact
with medications. Nearly all herbs come with some warning, and many, like the herbs used
for anxiety example (De Smet, 2002) Valerian, kava (Ang-Lee et al., 2001) and (Singh 2005)
and St.John’swort is the most notoriously interactive herbal product and has been shown to
interfere with numerous drugs metabolized by the cytochrome P-450 liver enzyme system,
12

including protease inhibitors, chemotherapeutic agents, and oral contraceptives (Hammerness
et al., 2003). It's important to discuss your medications and herbal supplements with your
doctor to avoid dangerous interactions. Because herbal products are not tightly regulated,
consumers also run the risk of buying inferior quality herbs. The quality of herbal products
may vary among batches, brands or manufacturers. This can make it much more difficult to
prescribe the proper dose of an herb (Feierman, 1986).
A particularly morbid case series describes 105 patients in Belgium who had been taking a
Chinese herbal product for weight loss and developed nephropathy caused by the herb
Aristolochiafangchi. Forty-three patients developed end-stage renal failure, and 39 had
prophylactic kidney removal. Eighteen of these patients were found to have Urothelial
carcinoma, which was shown to be related to the formation of DNA, adducts from the
aristolochic acid in this herb (Nortier et al., 2000). Another common toxicity from herbal
medicines involves pyrrolizidine alkaloids, which are complex molecules found in certain
plants that may be used or inadvertently added to herbal medicines (including comfrey,
which is still available in the United States). These alkaloids produce hepatotoxicity through
a characteristic veno-occlusive disease that may be rapidly progressive and fatal (Stickel et
al., 2005). Contaminants in herbal products may be particularly problematic in medicines
imported from Asia.
A study examining the contents of 260 Asian patent medicines found that 25% of products
contained high levels of heavy metals and another 7% contained undeclared drugs,
purposefully and illegally added to produce a desired effect (KoR, 1998), the safety of using
most herbs with drugs is not well established. Some herbs are known to interact with
pharmaceutical drugs, although most of this information comes from case reports rather than
13

systematic investigations. For example, ephedra, contains ephedrine, was widely used in
traditional Chinese medicine for thousands of years, and then became popular in this country
in the 1990s as a component of weight-loss and energy-enhancing products. An analysis of
contacts to poison control centers found that, compared with other commonly used herbal
products, ephedra was 40 times more likely to lead to a report of a side effect (Bent et.al,
2003). A systematic review found that ephedra led to a 2 to 3 fold increased risk of nausea,
vomiting, psychiatric symptoms, and palpitations compared with placebo (Shekelle et al.,
2003). Because of this and other evidence, ephedra was banned by the FDA on April 12,
2004. (DHHS, FDA, 2004). Shortly after the ephedra ban, the 7 largest manufacturers of
ephedra-containing products started marketing “ephedra-free” products, all of which
contained the herb citrus aurantium. This herb, also known as bitter orange, contains
synephrine, which has many of the same pharmacological properties as ephedrine, Hoffman,
and Taylor, (2001).and therefore potential to cause many of the same side effects. Use of a
combination of an herbal product containing citrus aurantium and caffeine has been shown to
cause statistically significant increases in systolic and diastolic blood pressure
(approximately 9mmHg) and pulse (16.7 beats per minute) in healthy adults. (Haller et al.,
2005).Patients taking such products may have an elevated pulse and blood pressure or report
insomnia or feeling “jittery” all of which may be caused by the caffeine and citrus auranitum-
containing supplement.
2.1.4 Traditional Medicine Usage
The use of herbal medicine has been on increase in many developing and industrialized
countries. It is known that between 65 and 80% of the world's population use herbal
medicines as their primary form of health care. Reports from WHO show traditional
14

medicine use in Uganda and Tanzania at 60 per cent, in Benin and Rwanda at 70 per cent,
and in Ethiopia at 90 per cent (WHO,2013) Also within the African continent the proportion
of individual using the five most popularly used systems of traditional medicine varies as
follows; 80 per cent of the population use herbal therapies, 13 percent make use of spiritual
therapies, 5 per cent use manual therapy and less than 1 percent use both homeopathy and
chiropractic. Studies show that demand for traditional medicine is increasing in many other
countries (Bannermann, et al., 1983) CAM has been described as a broad domain of healing
resources that encompasses all health systems, modalities, and practices and their
accompanying theories and beliefs, other than those intrinsic to the politically dominant
health system of a particular society or culture in a given historical period. CAM includes all
such practices and ideas self-defined by their users as preventing or treating illness or
promoting health and well-being. Boundaries within CAM and between the CAM domain
and that of the dominant system are not always sharp or fixed. In several parts of the world,
particularly in developing countries access to herbal medicines is largely unrestricted.
In developed countries, communities and midwives are showing a renewed interest in the
use of herbal and alternative medicine (Bayles, 2007). In the African context, traditional
medicine (TM) in pregnancy and labor continues to play, as it did in the past, an important
role in health systems.
The significant increase in the use of herbal medicines has resulted WHO’s promotion of
traditional medicine, countries have been seeking the assistance of the Organization in
identifying safe and effective herbal medicines for use in national health care system for
achieving the goals of Primary Health Care, most especially in the rural areas which cover
almost 80% of the entire population. On the hand at the international level the discussion of
15

co-operation focused first on incorporation of traditional healers (THs) in Primary Health
Care. However, it has been increasingly questioned whether western biomedicine and TM
can operate in a complementary way without one changing or oppressing the other
(Feierman, 1986).
2.1.5 Herbal Remedies Efficacy, Safety, and Regulation.
Herbal products have gained increasing popularity in the last decade, and are now used by
approximately 20% of the population. Herbal products are complex mixtures of organic
chemicals that may come from any raw or processed part of a plant, including leaves, stems,
flowers, roots, and seeds (Rotblatt and Ziment, 2002). Substance based practices use
substances found in nature such as herbs, foods, non-vitamin supplements and mega-
vitamins, and minerals, and includes traditional herbal remedies with herbs specific to
regions in which the cultural practices arose.
Although the practice of herbalism is not strictly based on evidence gathered using the
scientific method, modern medicine, does, however, make use of many plant-derived
compounds as the basis for evidence-tested pharmaceutical drugs, and phytotherapy works to
apply modern standards of effectiveness testing to herbs and medicines that are derived from
natural sources (Rotblatt and Ziment, 2002). Although herbs are often perceived as “natural”
and therefore safe, many different side effects have been reported owing to active
ingredients, contaminants, or interactions with drugs (Bent et al., 2004).
Safety: In general, traditional procedure-based therapies are relatively safe, if they are
performed properly by well-trained practitioners. However, accidents do occasionally occur,
most probably when practitioners are not fully trained or can result from misidentification or
misuse of healing plants. Therapies should be performed within accepted parameters, and the
16

indications for a therapy should be evidence based when possible. Serious adverse effects of
therapies are rare, but supportive data on adverse effects are not readily available.
Accordingly, the evaluation of adverse effects should be considered a priority area for
systematic evaluation of safety of these therapies, (Rotblatt and Ziment, 2002).
One problem in ensuring safety of a therapy is variable quality control in the manufacture of
therapy equipment. The most effective safety measures, therefore, are to ensure that the
equipment used is of good quality, as well as ensuring that the practitioners who use it have
had sound and well supervised theoretical and practical training. These are the appropriate
ways to minimize incompetent examination of patients, incorrect diagnoses and errors of
technique, and to ensure that patients are properly selected for traditional procedure-based
therapy (Bent et al., 2004).It should also ensure that the practitioner knows how to deal with
accidents when they occur, and knows how to refer the patient to an appropriate physician if
the patient does not respond to therapy or if there is a medical emergency (Bent et al., 2004).
Efficacy: Alternative therapies lack the requisite scientific validation, and their effectiveness
is either unproved or disproved. Many of the claims regarding the efficacy of alternative
medicines are controversial, since research on them is frequently of low quality and
methodologically flawed. Selective publication of results (misleading results from only
publishing positive results, and not all results), marked differences in product quality and
standardization, and some companies making unsubstantiated claims, call into question the
claims of efficacy of isolated examples where herbs may have some evidence of containing
chemicals that may affect health. The Scientific Review of Alternative Medicine points to
confusions in the general population a person may attribute symptomatic relief to an
otherwise-ineffective therapy just because they are taking something (the placebo effect); the
17

natural recovery from or the cyclical nature of an illness (the regression fallacy) gets
misattributed to an alternative medicine being taken; a person not diagnosed with science
based medicine may never originally have had a true illness diagnosed as an alternative
disease category. The efficacy of most forms of traditional procedure-based therapies
depends heavily upon the proficiency of the practitioners, including their skills and
experience (Bent, 2004).
In the same way as for conventional therapies, medicine, and interventions, it can be difficult
to test the efficacy of alternative medicine in clinical trials. In instances where an established,
effective, treatment for a condition is already available, the Helsinki Declaration states that
withholding such treatment is unethical in most circumstances. Use of standard-of-care
treatment in addition to an alternative technique being tested may produce confounded or
difficult-to-interpret results (Bent et al., 2003).
Regulation: In developing nations most especially, regulation of sales, importation and
manufacturing of herbal medicines are not subject to rigorous scrutiny in terms of safety and
efficacy as is the case for conventional western/allopathic medicines. The past decade has
seen a significant increase in the use of herbal medicines. Nowadays the discussion
concentrates more on integration through regulation (associations, licenses and training),
research and investments in effective services, products and consumer information
(Bodecker, 2001; WHO, 2002).
Pregnancy: is timed from the first day of last menstrual period and normally lasts 37-42
weeks (average 40 weeks). It is split in three trimesters: 1st trimester is week 1 – 13, 2nd
week 14 – 27 and 3rd week 28 – 40. Organogenesis takes place in the first trimester making
the fetus most sensitive to any compounds ingested by the mother in this period (Chuang,
18

2006), When referring to the condition of a newborn baby, “Apgar score” is commonly used.
This is a scoring system for heart rate, respiratory effort, muscle tone, reflex irritability and
color. Each characteristic is assigned a value of 0 to 2 points so the total score is 0 to 10. The
newborn is evaluated at1 and 5 minutes after birth. A score of 7 or more is considered
normal, 4-6 compromised and 3 or below medical emergency (Apgar, 1953). Pregnancy is a
special physiological state where medication intake presents a challenge and a concern due to
altered drug pharmacokinetics and drug crossing the placenta possibly causing harm to the
fetus (Banhidy et al., 2005).
Medication treatment in pregnancy cannot be totally avoided since some pregnant women
may have chronic pathological conditions that require continuous or interrupted treatment
(e.g. asthma, epilepsy, and hypertension). Also during pregnancy new medical conditions can
develop and old ones can worsen (e.g. migraine, headache, hyperacidity, nausea and
vomiting) requiring drug therapy (Deborah et al., 2005). So it becomes a major concern for
pregnant women to take medication whether prescription, over-the counter, or herbal
medication. Since the thalidomide era, there has been great awareness about harmful effects
of medications on the unborn child (Kacew, 1994; Melton, 1995). It has been documented
that congenital abnormalities caused by human teratogenic drugs account for less than 1% of
total congenital abnormalities (Sachdeva et al., 2009). Hence in 1979, Food and Drug
Administration developed a system that determines the teratogenic risk of drugs by
considering the quality of data from animal and human studies (Sachdeva et al., 2009). FDA
classifies various drugs used in pregnancy into five categories, categories A, B, C, D and X.
Category A is considered the safest category and category X is absolutely contraindicated in
pregnancy (FDA, 2005). This provides therapeutic guidance for the clinician.
19

Although some pregnant women may have the sufficient knowledge about high-risk
medication in pregnancy, there is a “general fear” from medications (Nordeng et al., 2010b).
The hesitation in medication use by pregnant women might result in serious consequences
which include but are not limited to: termination of a wanted pregnancy (Einarson, 2013),
reluctance to drug-use for nausea and vomiting (Baggley et al., 2004), preference of herbal
medications (Glover et al., 2003), non-compliance to prescriber’s medication (Ito et al., 1993;
Williams et al., 2002) and inclination toward OTC drugs (Erebaraet al., 2008) and other self-
medication methods (Holst et al., 2009). Medication use in pregnancy has been studied in
different communities. The high prevalence of herbal medicine use in this environment
among pregnant women can be adduced to its longstanding integration into the culture of the
people, and its perception as their own indigenous medicine.
In pregnancy herbs are normally used orally on a regular basis as a tonic to clean the womb
(Varga and Veale, 1997), to attain an easy and quick delivery (Gumede, 1990), and in order to
protect the child from evil and to have a healthy child (Gonçalves, 2001). Other factors
underlying the use of traditional medicine have been identified as social pressure,
dissatisfaction with the behavior of clinic staff, reluctance of clinic staff to give drugs and
lack of privacy within the clinic environment (Jewkes et al., 1998b; Abrahams, et al., 2002).
Taking herbal medicines during different trimesters of pregnancy may cause different effects.
Exposure of fetus to herbal medicines during the first trimester may lead to congenital
malformation, while taking herbal medicines during the second or third trimester may lead to
fetotoxicity such as intrauterine growth retardation, fetal distress, fetal hypoxia and
intrauterine death. The majority of mothers in the study took herbal medicines during the
third trimester only (79.6%), mainly to facilitate labor. About 4.6% of mothers were exposed
20

to herbal medicines during the first trimester only and 9.3% were exposed to herbal
medicines during the first and third trimester. Mothers who were exposed to herbal medicines
during the first trimester were those who usually consumed herbal medicines before
pregnancy but because of the unplanned pregnancy, they continued taking herbal medicines
during pregnancy without realizing that they were pregnant. By the time they stopped taking
herbal medicines, they have already been pregnant for several weeks, (Jewkes et al., 1998b;
Abrahams et al., 2002)
2.2 Empirical Literature Review
Referring to WHO (2013) estimates, 65 and 80% of the world's population, use traditional
medicine. Indeed, few studies are available on the use of herbs for pregnant women. Also, a
study conducted in 2002 in the United States revealed that 62% of adults used alternative
medicine in the previous year before the year of the research (Barnes et al., 2007).
According to the European Information Centre for Complementary and Alternative
Medicine (EICCAM, 2008) report analysis of surveys done over the past ten years preceding
2008 indicate that 20% of European citizens have clear preference for complementary and
alternative medicine (CAM), and another 20% are regular users of CAM. The report further
states that more than 100 million citizens in the EU make use of CAM and the most
commonly used CAM therapies are homeopathy, phytotherapy (herbal medicine),
anthroposophic medicine, naturopathy, traditional Chinese herbal medicine, osteopathy and
chiropractic. In the developing world, the co-existence of various traditional medical systems
such as Ayurvedic, classical Chinese, Yoruba, Unani Tibbi and Akan with biomedicine is
well-documented phenomenon (Good, 1987). Together, these various modes of interpreting
21
and responding to sickness from what Charles Leslie (in Janzen 1978 pg14) termed “more or
less pluralistic, more or less integrated, and more or less syncretistic regional systems”.
Cross-sectional surveys in one Australian state in 1993, 2000 and 2004 demonstrated high
levels of use of CAMs and CAM therapists, (MacLennan et al., 2004, Kristoffersen et al.,
1996, MacLennan et al., 2002). While overall use of CAMs was stable, with approximately
50% of respondents using at least one non-medically prescribed alternative medicine in the
previous year, there were an increased number of women using herbal medicines
(MacLennan et al., 2004). Users of CAM are more likely to be female, better educated,
employed. (MacLennan et al., 2004, Kristoffersen et al., 1996, MacLennan et al., 2002 and
have a higher income (MacLennan et al., 2004,MacLennan et al., (2002).
A descriptive cross-sectional study design was used to determine the use of home remedies
during pregnancy among Jordanian women. A convenient sample of 332 Jordanian pregnant
women attending the MCH centers (antenatal clinic for follow-up) in Amman city; capital of
Jordan, were interviewed by a semi-structured questionnaire in the period from October 2009
to January 2010. About three quarter of the participants (73.8%) have used home remedies
because they considered it better than medications. The majority of users (90.2%) perceived
that the effect of home remedies on their pregnancy complaints was total improvement. Fluid
herbal remedies are the most common used, more than sixty one percentage of the
participants reported the source of information was the mother and mother-in-low. The use of
home remedies had no significant relationship with mother’s age, educational level, and job
status of participants as well as family size. The majority of the participants in the study used
home remedies during pregnancy as part of their traditional practices. As there is very limited
22
information about the safe use of home remedies; the mothers need education to avoid the
use of home remedies during pregnancy.
In West Africa, a Nigerian city, re-searchers reported that pregnant women used both
traditional herbal medicine and pharmaceutical drugs, with the highest prevalence of
concomitant use among nulliparous mothers (Gharoro and Igbafe 2000). Social demographic
factors, such as geopolitical zones and educational attainment, had an effect on the views of
women on the safety of herbal medicine for the fetus, and side effects of herbal medicines
(Fakeye et al., 2009).
In South African hospital-based study compared women reporting use of traditional medicine
with those not reporting such use, and found that traditional medicine use in pregnancy was
relatively common (55% of delivering women). Furthermore, a higher cesarean section rate
was observed in women who used traditional medicine compared to women who did not use
traditional medicine (39% vs. 22%) (Mabina et. al., 1997). A higher frequency of me
conium-stained fluid in women who used traditional medicine during pregnancy compared to
those who did not 56% vs. 15%) was also noted a higher frequency of meconium-stained
fluid in women who used traditional medicine during pregnancy compared to those who did
not (56% vs. 15%) was also noted.
In East Africa a study in largely rural districts of Kenya found wide spread use of herbal
medicine among women cared for by traditional birth attendant s during pregnancy, labor and
the postpartum period Family Care International. The use of herbal medicine was often
complementary to medical care, depending on barriers to health care access, complications,
and socio-cultural beliefs. According to the literature, use of herbal medicine during
pregnancy, labor or the postpartum period occurs at rates ranging from 30% to 70 % in a
23

health care setting in urban area s of sub-Saharan Africa (Addo, 2007, Gharoro and Igbafe
2000, Fakeye et al., 2009, Tamuno et al., 2011).
In the Bushenyi district of rural Uganda, a health survey study found that nearly all of the
285 women interviewed reported using herbal medicines during pregnancy and/or to induce
labor (Kamatenesi and Oryem-Origa, 2007). Health surveys reported seventy-five plants that
were used to induce labor, some of which were believed to be oxytocin by the authors of the
study. In central Africa, a study carried in 2005 at Nyamasheke District western Rwanda
where five physicians, eighteen nurses, five community health workers, and four traditional
medicine providers interviewed, estimated the average utilization rates of phytomedicine
during pregnancy to be 50-80%. CHWs, nurses, and physicians perceived the following to be
the most common indications for phytomedicine use by pregnant women: prevention of
malformations, induction of labor and augmentation of contractions, prevention of a
husband’s infidelity while a woman is pregnant, prevention of abdominal pain during
pregnancy, and protection against witchcraft. Physicians and nurses more commonly
perceived there to be non-medical reasons that women use traditional medicines, such as
protection from witchcraft, compared to the more commonly reported medical indications by
the CHWs and traditional medicine providers. Aside from protection from infidelity,
traditional medicine providers only reported clinical indications for use (Beste, 2015).
2.3 Critical Literature and Gap Identification
Research and development: Research in chemistry and bio-active components of medicinal
plants of Africa has been ongoing for quite some time, funded by multi or bi-lateral aid or
non-governmental donor organizations (Walter et al., 1993). A systematic and concerted
approach to this activity has not been maintained, for want of sophisticated equipment and
24

high-cost chemicals. Much of the research has been mainly academic. The concept of applied
research in the industrial use of plants has not received much attention. Furthermore, research
and training activities for traditional medicine has not received due support and attention.
The main problem facing the use of traditional medicines is the proof requirement that the
active components contained in medicinal plants are useful, safe and effective. This is
required to assure the medical field and the public regarding the use of medicinal plants as
drug alternatives. The proofs of pharmacology activity that are available at present are mostly
based on empirical experience. The scientific proof then becomes the most important thing,
in order to eliminate the concern of using medicinal plants as drugs for alternative treatment.
Unfortunately, most African countries are not able to conduct research or provide scientific
proof of pharmacology. Reasons for the lack of research data involve not only policy
problems, but also the research methodology for evaluating traditional medicine. There is
literature and data on the research of traditional medicine in various countries, but not all
scientists may accept them. As the characteristics and practice of traditional medicine is quite
different from western medicine, how to evaluate traditional medicine and what kinds of
academic research approaches and methods may be used to evaluate the safety and efficacy
of traditional medicine are new challenges which have emerged in recent years (Safowora,
1982).
Legislation: despite its existence over many centuries and its expansive use during the last
decade, in most African countries, traditional medicine, including herbal medicines, has not
yet been officially recognized, and the regulation and registration of herbal medicines has not
been well established (Bodecker, 1994).
25
Although, in most African countries more than 80% of the populations rely on traditional
medicine for their primary health care needs, the governments have not yet promulgated
edicts or decrees visa regulation and recognition of the practice of traditional medicine. Even
in countries where there is an apparent recognition, appropriate budgeting to facilitate the
functioning of the Traditional Medicine Board is usually inadequate or totally lacking
(Cunningham, 1993).
In many countries in Africa, the entire traditional medicine community seems to be operating
outside the framework of national legislation on the collection and trade in wild species.
There is also a large inter-African trade in medicinal plants, again almost entirely outside the
usual international trade controls. There is thus a need for the formulation and development
of national as well as regional policies and legislation in terms of the trade and access to
these resources if maximum benefits are to be reaped in order for such policies to be
successful. Many African countries do not have procedures to register medicinal plant
preparations although they are widely used for the health care needs of a majority of the
people. The regulations, if any, are very stringent, requiring the same standards expected of
modern medicines (Myles, 1998).
2.4 Theoretical Framework
2.4.1 Monopolistic Health Care Model
This health care model allows only modern biomedical (allopathic) doctors and health
practitioners to practice health care. In this type of health care model, traditional medicine
and complementary and alternative medicine are not legal practices. This form of health care
system may encourage the illegal practice of traditional medicine.
26

In such cases traditional healthcare users may have no protection. This model was
predominant in most African countries during the colonial era. The monopolistic healthcare
model is almost rare to find the world over with the increased popularity gained by
traditional medical practice.
2.4.2 Tolerant (Co-existence) Health Care Model
In the tolerant health care model, the traditional health practitioners are allowed to practice
but are not officially recognized. The practice is usually done under an unofficial capacity.
The main national health care delivery system is based entirely on allopathic medicine or
biomedicine. This is found in many countries with no regulatory or legal mechanism for the
practice of traditional medicine (Snow, 2008).
2.4.3 Parallel (inclusive) or Dual Health Care Model
The inclusive health care model comprises of two health care systems each operating
independently but acknowledging and respecting the contributions of each system.
The traditional and modern allopathic are separate components of the national health care
system. In some cases, the national authorities are developing the appropriate frameworks for
traditional medicine related policy, regulation, practice, health insurance coverage, research
and education. Examples of countries practicing the inclusive system of integrating
traditional medicine into their national health care systems are Benin, Burkina Faso,
Cameroon, Equatorial Guinea, Guinea, and Cote d'Ivoire, the Democratic Republic of
Congo, Equatorial Guinea, Niger, Nigeria, Madagascar, Mali, Mozambique, Swaziland,
Tanzania and Zimbabwe (WHO, 2009).
27

2.4.4 Integrative Health Care Model
In this situation, traditional medicine is fully recognized and incorporated into all areas of
health care delivery including national medicines policy, registration of traditional medicine
products, regulation of traditional medicine practice, establishment of traditional medicine
hospitals, inclusion of traditional medicine in national insurance schemes as reimbursable
items, establishment of relevant research institutions on traditional medicine, and training of
traditional medicine practitioners at all levels of education, including universities. Integration
also subsumes visibility of traditional medicine international health programmes, and its
reflection in national planning and budgeting schemes. Globally only four countries the
People's Republic of China, the Democratic Republic of Korea, the Republic of Korea and
Vietnam have integrated traditional medicine into their national health care systems. No
country in the WHO African Region has yet established this integrative system regarding the
incorporation of traditional medicine into national health care systems.
Traditional medicine practitioners need support, education and cooperation. (Olson and
Nkiwane, 2006) observed that traditional health systems are often misunderstood, sometimes
to the extent of causing fear. This system of healthcare should be examined with an open
mind, further developed and finally integrated with the national healthcare system for it to
provide the best healthcare benefits possible.
2.4.5 Traditional Model of Health
Health is a complex term and different people have different ways to interpret it. (Laverack,
2007) Observed that health is subjective and its interpretation is based largely on personal
experienced and influenced by the culture and environment in which people live and
function. Individuals may define their health based on ability to carry out certain roles and
28
responsibilities for self or community rather the absence of disease or illness (Nelms and
Gorsk, 2006), stated that the African woman´s conceptualization of good health is
characterized by a disease free state and the ability to work and perform tasks, take care of
children, and keep the house and clothes clean and the attribute poor health to the influence
of supernatural forces.
The WHO definition of health states that health is a state of complete physical, mental and
social wellbeing and not merely the absence of disease or infirmity (WHO, 2006). Laverack
pointed out that physical wellbeing deals with a healthy functioning of the body, biological
normality, physical fitness and capacity to perform tasks (Laverack, 2007). Social wellbeing
on the other hand includes interpersonal relationships as well as wider social issues such as
marital satisfaction, the ability to engage in paid work and community involvement. Mental
wellbeing involves self-efficacy, subjective wellbeing and social inclusion and the ability to
adapt to the environment and society in which an individual lives and functions. However
critics hold that the WHO definition of health lacks the emotional and spiritual aspect of
health (Ewles and Simnett 2003). In the traditional model of health the emotional and
spiritual aspect of health is greatly emphasized. (Snow, 2008) in a study carried out among
poor Afro-Americans, reported that lower class Afro-American classified illness into two
groups; Natural and Unnatural illnesses based on their perceptions of the causes of the
illness. This influences their interpretation of health. Causality beliefs can well be used to
differentiate the different medical systems, i.e. traditional medical systems from biomedical
system or conventional medical systems. Foster reported two basic principles of Causality
that characterize the traditional (non-western) medical system; the Personalistic and the
Naturalistic Etiologies of illness. This is because in the traditional model of health the
29

perception of health is extricable bound up with religion, morality and the supernatural, so
that natural versus unnatural are closely allied with good versus evil or godly versus ungodly.
Naturalistic Causality explains illness in terms of the natural forces or conditions such as
cold, heat, dampness etc. Natural events take place in the world as God made it and as He
intended it to be. Natural illness could come about as a failure to take care of self (body) or
by sinful behavior (failure to take care of soul) in which case illness is seen as divine
punishment (Foster, 1976).
Personalistic Causality allows little room for chance. It accounts for the etiology of the so
called unnatural illness which cannot be explained using the ordinary laws of nature. It
explains the cause of a disease to be due to an active and purposive intervention of an agent
who may be a human (a witch or wizard); a non-human (ancestral spirit) or a supernatural
being such as a deity: - (Lisa et al., 2009).This is usually termed the work of the devil. This is
based on the belief that a being with extraordinary power can influence the natural course of
events and cause illness in people. Even emotional disturbance such as fear, envy and shame
or grief are attributed to evil spiritual forces. The sick person is usually seen as a victim. Such
illnesses are believed that they cannot be cured by orthodox biomedicine but traditional
medicine or through divine intervention. Such belief is common in society where life is seen
as a challenge and the world as hostile, where God or an ancestral spirit may strike you down
for sinning or an envious neighbor may bewitch you through dark magic, (Snow, 2008). Such
health beliefs leave all members in the community suspicious of each other, friendship is
fragile and relationships are brittle and even family members are not to be trusted. The
traditional model of health is largely based on the Personalistic etiology of disease or illness.
30

2.5 Conceptual Framework
Figure 2.1 Conceptual Framework
INDEPENDENT VARIABLES DEPENDENT VARIABLES
Intervening variables
Source: Researcher 2017
31
Socio-cultural factors Religion /culture Believes Influence from family
Health policies Acceptability Accessibility Availability
Socio-economic Income Health insurance Employment
Socio-demographic factors
Age Marital status Parity Level of education
Knowledge&Practice of TM

2.6 Summary
The use of herbal supplements in pregnancy is relatively high and it is important to ascertain
what herbs (if any) women are taking. Pregnancy care providers should be aware of the
common herbal supplements used by women, and of the evidence regarding potential
benefits or harm. It is important that care providers do not prescribe any treatments,
medications or herbal supplements where they are unaware of the evidence supporting their
use. Pregnant women should also be aware about the risks which may occur not only to
themselves but also to their babies.
32

CHAPTER THREE: RESEARCH METHODOLOGY
3.0 Introduction
This chapter deals with methodology, it descriptions the design, data collection procedures
and instruments used during this research. Moreover, it provides information about materials,
study area description, and methods used to carry out this study.
3.1 Research design
The study adopted descriptive research design with both qualitative and quantitative
approaches. Descriptive research design is most appropriate when the purpose of study is to
create a detailed description of an issue (Mugenda and Mugenda, 2003). The quantitative
research methodology that was used in the study employed statistics expressed in frequencies
and percentages and they were used to explain demographic social and economic
characteristics of the respondents. Qualitative approach involved interviewing sampled
pregnant women. This technique was used to get information from respondents regarding
knowledge and practice of tradition medicine.
3.2Target Population
Population refers to the total group of people from whom the information is needed. A
research design is the plan and structure of investigating so conceived as to obtain answers to
research questions (Kothari, 2004).The study population for the study comprised of all
pregnant mothers attending Kibagabaga district hospital totaling 179 during the time of
research.
33
3.3 Sample Design
3.3.1 Sample size
A sample is a portion of the population selected to achieve the objectives of the study. A
sample size is a smaller group obtained from accessible population. This group is carefully
selected so as to be representative of the whole population with the relevant characteristics
(Mugenda & Mugenda, 1999). The researcher will randomly select the respondents the use of
Slovin’s formula as follows:
n = N/1+ N (e)2
Where;
n is the sample size,
N is the population size (179)
e is the desired level of precision (0.05)
……………………………… ..0.05¿¿¿¿2
1+179 ¿n=¿¿
¿
= 123
Therefore the sample size for this study was 123.
3.3.2 Sampling Technique
According to Dencombe (2007), sampling procedure defines the rules that specify how the
system calculates the sample size and it contains information about the valuation of an
inspection characteristic during results recording. Random sampling technique was used in
selecting samples. Purposive sampling was used in selecting the interviewees. This was
34
based on their TM usage. Only mothers that were using TM at the time of study were in a
position to provide reliable information pertaining to reasons for TM usage.
3.4 Data Collection Methods
3.4.1 Data Collection Instruments
3.4.1.1Questionnaire
The study used questionnaire as the tool for collecting primary data. The questionnaire was
translated to local language (Kinyarwanda) to ensure that all the respondents understand the
questions. This method of data collection was preferred for this study due to its ease in
collecting data from large population, friendly cost of administration in-terms of time and
money. A questionnaire was also emailed to respondents who are not easily accessed for hard
delivery. The questionnaires were organized in two parts. The first part divided into the
demographic and socio-economic characteristics. The second part covered respondent’s
knowledge and practice of the traditional medicine.
3.4.1.2 In-Depth Interviews
Interviews of pregnant mothers were used to gain increased knowledge on TM practice
among pregnant women. Interviewing is a qualitative research technique that involves
conducting intensive individual interviews, to explore their perspectives on a particular idea.
All the participants who used traditional medicine were selected purposively to get more
details on the use of TM. The researcher contacted the interviewees through phone calls to
confirm their availability for the interview as well as their preferred venue. The interview
was aimed at collecting information related to the opinion of the interviewees on pregnant
women use TM, perceived reasons for the use of TM among pregnant women, stage of
35

pregnancy in which women use and perceived effect of TM use during pregnancy. A tape
recorder was used to capture all the information and this helped us to cross check with
previous answers from respective questionnaires.
3.4.2 Administration of Data Collection Instruments
The scientific method in quantitative research attempts to mirror people’s social and
geographic worlds, however, qualitative research interviews employ interactive approach to
gain access to the meanings people attach to their everyday experience in these worlds
(Cloke et al. 2004). A structured questionnaire was developed in English and translated to
commonly spoken local language (Kinyarwanda).The tool was self-administered, where
necessary with the aid of well-trained research assistants, it was administered to gather
quantitative information regarding their knowledge and practice about traditional medicine.
Closed questionnaires were used. The questionnaire was pre piloted using a sample of
women from the same antenatal clinic who will not chose to be part of the study. Necessary
modifications were made before the study.
The use of In-Depth interview technique made the interviewing process content focused and
dealt with the issues and questions raised in the interview guide; as well as giving room for
the informants to freely express themselves. Informants were used in the interview for this
study. The researcher conducted the interview as per the participant’s preference of language
and in a quite comfortable environment.
Interview guide questions were designed specifically to elicit information on practice of
herbal in pregnancy.
36

3.4.3 Reliability and validity
Content reliability was tested by group of experts including obstetrician, midwife and
community health worker. The questionnaire and interview questions were then piloted
among 10 pregnant women at the antenatal clinic to test the validity and feasibility of the
questionnaire. According to the results that were obtained, a few wordings were changed and
some questions were rephrased again to improve the clarity of instrument. Cranach’s alpha
for the questionnaire to determine reliability and internal consistency.
Trustworthiness in qualitative research will be used in the evaluation of a study based on
different criteria depending on specific aspects of the research (Strauss and Corbin 1998).
Dahlgren et al (2007) suggested that judgment should be made regarding the credibility,
transferability, dependability and conformability criteria. These strategies are important to
researchers in designing ways of increasing the rigor of their qualitative studies and also for
readers to use as a means of assessing the value of the findings of qualitative research. For
example, according to Krefting (1991), “truth value is usually obtained from the discovery of
human experiences as they are lived and perceived by informants.” The lived experiences
that participants will share are going serve to support this. Furthermore, the findings can be
generalized to pregnant mothers in other parts of Rwanda as well. This ensures applicability
and consistency. Finally, the researcher strove towards neutrality by allowing the data to
speak rather than elaborately explain the data through the researchers’ lens.
3.5 Data analysis Procedure
Quantitative data collected through the use of questionnaires, were categorized, coded and
then entered into the computer. Basic descriptive analysis was done using the SPSS version
21 Descriptive statistics was generated through descriptive analysis and it included frequency
37

distribution and percentages. Qualitative data collected was organized into themes and then
analyzed. Themes included reason for TM usage; stage of pregnancy when TM are used,
effect of TM use during pregnancy and suggestions for reducing TM usage among pregnant
women.
For each knowledge and practice question, a score of one was given for a correct answer,
whereas a zero score was given for incorrect and do not know responses. Questions on the
knowledge and practice part were rated and a total score was obtained. The median score was
then computed. Therefore, those with a total score equal to or below the median were
classified as having poor knowledge and practice, whereas those above the median were
considered having good knowledge.
3.6 Ethical Consideration
Authorization for data collection was sought from Mount Kenya University. The researcher
ensured that participants completely understood the purpose and methods that were used in
the study. The participants were also made to understand that they had the right to withdraw
from the study at any time. A consent form was availed to the participants to sign as to
whether they would participate in the study or not. Aassurance that all the information
provided by the respondents would be treated with utmost confidentially was also granted.
38

CHAPTER FOUR: RESEARCH FINDINGS AND DISCUSSION
4.0 Introduction
This chapter presents the findings and discussion with regard to the study objective. The
purpose of the study was to determine knowledge and practice of traditional medicine among
pregnant mothers. The findings are presented in percentages and frequency distributions
tables. A total of 123 questionnaires were issued out. The completed questionnaires were
edited for completeness and consistency. All 123 questionnaires issued were returned. This
represented a response rate of 100%.
4.1 Demographic Characteristics of Respondents
The study sought to investigate the demographic information of the respondents. These data
were important in ascertaining the background of the respondents in relation to the study.
Analyses of the demographic findings are presented in this section and they include; age
marital status, religion, level of educational, gestation age.
39
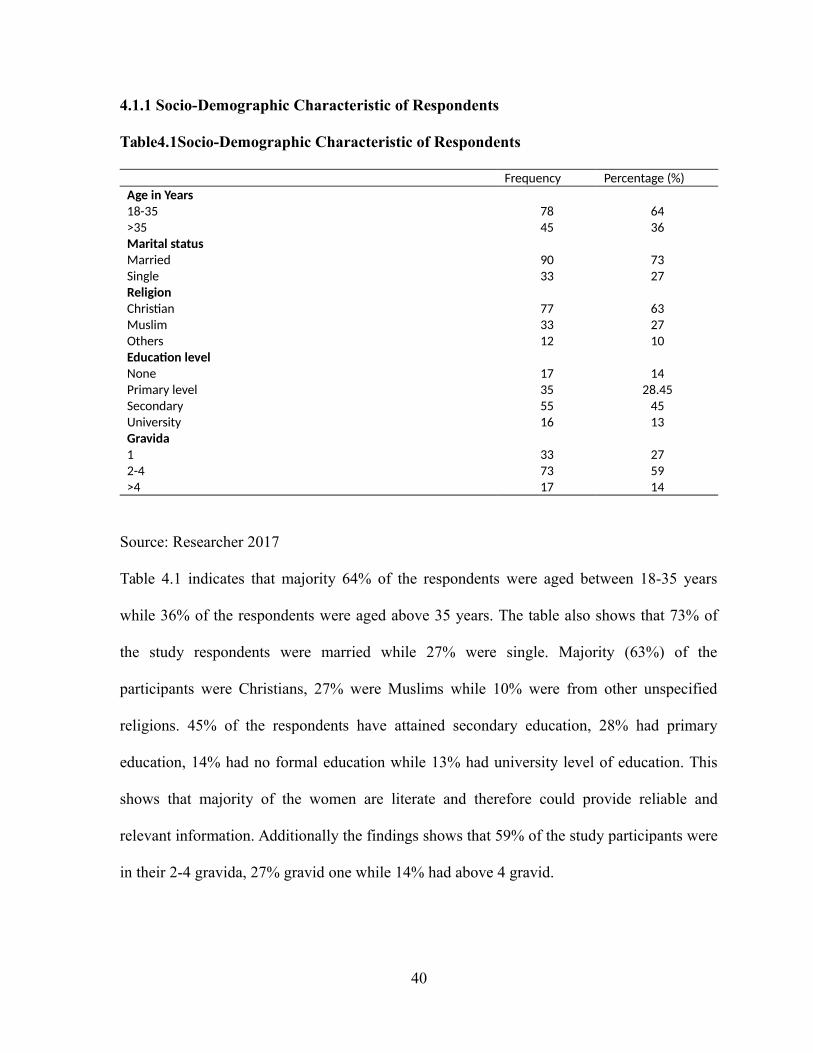
4.1.1 Socio-Demographic Characteristic of Respondents
Table4.1Socio-Demographic Characteristic of Respondents
Frequency Percentage (%)Age in Years18-35 78 64>35 45 36Marital statusMarried 90 73Single 33 27ReligionChristian 77 63Muslim 33 27Others 12 10Education levelNone 17 14Primary level 35 28.45Secondary 55 45University 16 13Gravida1 33 272-4 73 59>4 17 14
Source: Researcher 2017
Table 4.1 indicates that majority 64% of the respondents were aged between 18-35 years
while 36% of the respondents were aged above 35 years. The table also shows that 73% of
the study respondents were married while 27% were single. Majority (63%) of the
participants were Christians, 27% were Muslims while 10% were from other unspecified
religions. 45% of the respondents have attained secondary education, 28% had primary
education, 14% had no formal education while 13% had university level of education. This
shows that majority of the women are literate and therefore could provide reliable and
relevant information. Additionally the findings shows that 59% of the study participants were
in their 2-4 gravida, 27% gravid one while 14% had above 4 gravid.
40

4.2 Presentation of Findings
4.2.1 Prevalence of TM usage among pregnant women
The study sought to determine the prevalence of traditional medicine usage among the
pregnant women who participated in the study.
Table 4.2: Prevalence of Traditional medicine usage
Detail Frequency Percentage
Use at least one type of TM 38 31
Never used any form of TM 85 69
Total 123 100
Source: Researcher 2017
Table 4.2 indicates that the prevalence of those that never used TM during pregnancy was
69% while 31% of the pregnant women used traditional medicine. The study by Tamuno et
al., (2010) in a tertiary hospital in Nigeria revealed a 31.4% prevalence of traditional
medicine use among pregnant women. This prevalence is the same as that of the current
study. The studies conducted by Sattari et al., (2012) and Al-Riyami et al., (2011) reported
23.8% and 22.3% prevalence of traditional medicine use among pregnant women
respectively. This is lower than that of the current study. Dabaghian et al, (2012); Tabatabaee
et al., (2011) and Hashim et al, (2005) revealed 82%, 67% and 65% prevalences of traditional
medicine use among pregnant women respectively. These prevalences are too high compared
to that of the current study. Lower prevalence revealed by the current study could be
attributed to the strong health care system, strict in the regulatory framework for traditional
herbal practitioners in Rwanda.
41

4.2.2 Knowledge of TM among pregnant women
The study sought to determine the knowledge of pregnant women regarding traditional
medicine. Analysis of the data collected is displayed in table 4.3.
Table 4.3: Knowledge of Traditional medicine among pregnant women
Statement Yes No
Do you thing that TM could be harmful to your health 115 (94%) 8 (6%)
Do you think that the TM is dangerous to the health of thefetus
90 (73%) 33 (27%)
Do you have information regarding the tradition medicineyou use
42 (34%) 82 (66%)
Do you know how the TM you use is prepared 33 (27%) 90 (73%)
Source: Researcher 2017
Table 4.3 shows that majority (94%) of the women were aware that traditional medicine
could be harmful to their health while 6% thought it couldn’t be harmful. Majority (66%) of
the respondents thought that the traditional medicine is dangerous to the health of the fetus
unlike 34%. Most of the respondents (73%) did not know how the medication they were
receiving was prepared while 27% were aware.
42

4.2.2.1 Level of Knowledge regarding Traditional medicine
Table 4.4: Level of Knowledge regarding Traditional medicine
Knowledge level Frequency PercentageGood 79 64%Poor 44 36%Total 123 100
Source: Researcher 2017
Table 4.4 indicates that 64% of the study respondents had scored above the median score
(>3). This implies that 64% of the respondents had good knowledge regarding TM. Also the
table shows that 36% of the respondents had poor level of knowledge regarding traditional
medicine (≤ 3)
43
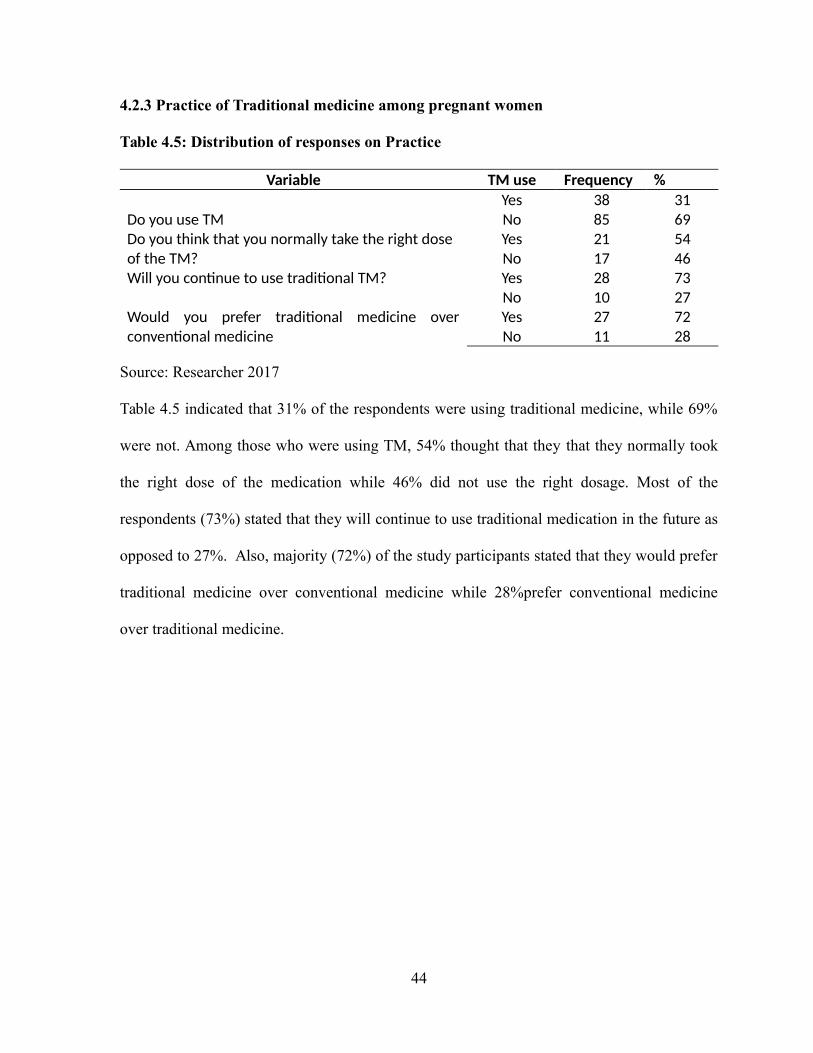
4.2.3 Practice of Traditional medicine among pregnant women
Table 4.5: Distribution of responses on Practice
Variable TM use Frequency %
Do you use TMYes 38 31No 85 69
Do you think that you normally take the right dose of the TM?
Yes 21 54No 17 46
Will you continue to use traditional TM? Yes 28 73No 10 27
Would you prefer traditional medicine overconventional medicine
Yes 27 72No 11 28
Source: Researcher 2017
Table 4.5 indicated that 31% of the respondents were using traditional medicine, while 69%
were not. Among those who were using TM, 54% thought that they that they normally took
the right dose of the medication while 46% did not use the right dosage. Most of the
respondents (73%) stated that they will continue to use traditional medication in the future as
opposed to 27%. Also, majority (72%) of the study participants stated that they would prefer
traditional medicine over conventional medicine while 28%prefer conventional medicine
over traditional medicine.
44

4.2.4 Sources of herbal medicines
Figure 4.1 Sources of herbal medicines
Source: Researcher 2017
Figure 4.2 indicated that 33% of the respondents buy the medication and prepare themselves,
28% obtain the medication from the tradition midwives, 31% from peers while 8% buy from
traditional healers. In a study conducted by Kim and Keng (2013) pregnant women were
reported to buy herbal medicines directly from traditional midwives as well as preparing the
medication themselves. This is consistent with findings of the current study.
45

4.2.5 Source of information regarding traditional medicine
Figure 4.2 Source of information on tradition medication
The study sought to determine the sources of information regarding traditional medicine
among the study participants.
Figure 4.3 shows that (45%) of the study participants obtained information regarding to
traditional medication from parents (mother and/or mother-in-low), Similar findings, with
different percentages, have been reported in a previous study in Tumpat District, Kelantan.
The previous result shows that the older generations like parents and parents’ in-law were the
most common persons (63.9%) who suggested the women to use herbal medicines during
their pregnancy which is higher than the current study. 31% from tradition midwives, 17%
from friends while 6% had relatives as their source of information regarding to traditional
medication. Kim and Keng (2013) reported that most women get information on herbal
medication from their parents, friends and from traditional midwives (This is in agreement
46

with the current findings. Mothers, peers, radio and television and traditional healers were
important sources of information on herbal medicine (Tamuno et al., 2010).
4.2.6 Factors influencing pregnant women knowledge and practice regarding TM
Table 4.6: Factors influencing pregnant women knowledge and practice regarding TM
Statement
Str
ongl
y A
gree
%
Agr
ee %
Dis
agre
e %
Education level of pregnant women influences their
knowledge and practice regarding traditional medicine
111(90%)
12(10%)
Religion of pregnant women influences their knowledge
and practice regarding traditional medicine
18(15%) 74(60%) 31 (25%)
Family and friends can influence knowledge and
practice of pregnant women regarding traditional
medicine
49(40%) 68(55%) 6 (5%)
Socio-economic factors can influence knowledge and
practice of pregnant women regarding traditional
medicine
55(45%) 59(48%) 9(7%)
Source: Researcher 2017
Table 4.7 indicates that 90% of the study respondents strongly agreed with the statement that
education level of pregnant women influences their knowledge and practices regarding
traditional medicine while 10% just agreed with the statement. Also the table shows that 15%
of the study respondents strongly agreed with the statement religion of pregnant women
influences their knowledge and practices regarding traditional medicine, 60% just agreed
while 25% disagreed with the statement. Majority (55%) of the respondents agreed with the
statement that family and friends can influence knowledge and practices of pregnant women
regarding traditional medicine, 40% strongly agreed while 5% disagreed. The table also
47

shows that 45% of the study respondents strongly agreed with the statement that socio-
economic factors can influence knowledge and practices of pregnant women regarding
traditional medicine, 48% agreed while 7% disagreed.
48
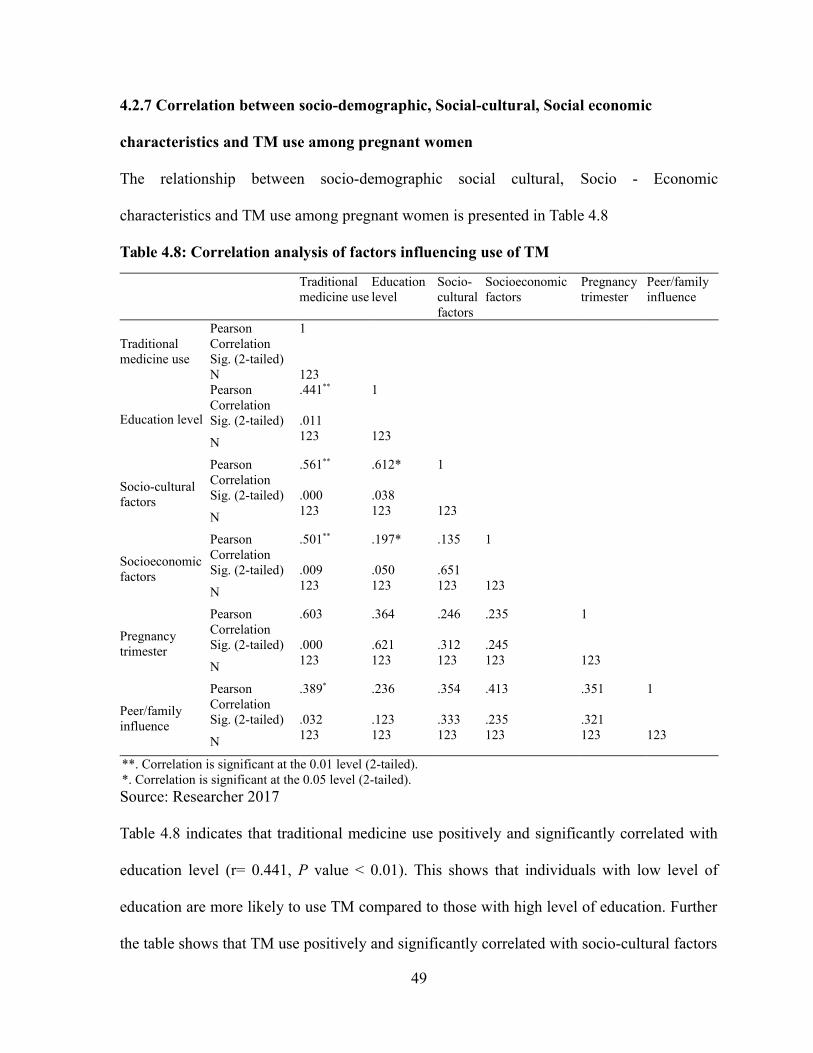
4.2.7 Correlation between socio-demographic, Social-cultural, Social economic
characteristics and TM use among pregnant women
The relationship between socio-demographic social cultural, Socio - Economic
characteristics and TM use among pregnant women is presented in Table 4.8
Table 4.8: Correlation analysis of factors influencing use of TM
Traditionalmedicine use
Educationlevel
Socio-culturalfactors
Socioeconomicfactors
Pregnancytrimester
Peer/familyinfluence
Traditionalmedicine use
PearsonCorrelation
1
Sig. (2-tailed)N 123
Education level
PearsonCorrelation
.441** 1
Sig. (2-tailed) .011
N 123 123
Socio-culturalfactors
PearsonCorrelation
.561** .612* 1
Sig. (2-tailed) .000 .038
N 123 123 123
Socioeconomicfactors
PearsonCorrelation
.501** .197* .135 1
Sig. (2-tailed) .009 .050 .651
N 123 123 123 123
Pregnancytrimester
PearsonCorrelation
.603 .364 .246 .235 1
Sig. (2-tailed) .000 .621 .312 .245
N 123 123 123 123 123
Peer/familyinfluence
PearsonCorrelation
.389* .236 .354 .413 .351 1
Sig. (2-tailed) .032 .123 .333 .235 .321
N 123 123 123 123 123 123
**. Correlation is significant at the 0.01 level (2-tailed).*. Correlation is significant at the 0.05 level (2-tailed).Source: Researcher 2017
Table 4.8 indicates that traditional medicine use positively and significantly correlated with
education level (r= 0.441, P value < 0.01). This shows that individuals with low level of
education are more likely to use TM compared to those with high level of education. Further
the table shows that TM use positively and significantly correlated with socio-cultural factors
49

(r= 0.561, P value < 0.01). This means that women from various social and cultural
backgrounds will have varying levels of TM consumption. Also the findings shows that TM
use positively and significantly correlated with socioeconomic factors (r= 0.501, P value <
0.01). This implies that pregnant women from various social and economic backgrounds will
have varying levels of TM consumption. The trimester of pregnancy also showed a
significant relationship with Tradition medicine usage (r= 0.603, P value < 0.01). This means
that at different trimesters of pregnancy, women will show varying behaviors in regards to
TM use. Peer or family backgrounds of the pregnant women has a significant influence on
TM usage (r= 0.389, P value < 0.05) implying that women from different family
backgrounds will exhibit varying levels of TM usage.
Qualitative Analysis Results
4.2.8 Level of practice among pregnant women who used Traditional medicine
The study sought to determine level of practice among study participants who used
Traditional medicine.
Table 4.8: Level of practice regarding Traditional medicine
Level of practice Frequency PercentageGood 26 68%Poor 12 32%Total 38 100
Table 4.8 indicates that 68% of the study respondents who used Traditional medicine had
good level of practice regarding traditional medicine while 32%of the respondents had poor
level of practice regarding traditional medicine (≤ 3).
4.2.9 Reasons for traditional medicine usage during pregnancy
The interviewees were asked to give reasons for TM usage by pregnant women. Thirty eight
percent of the interviewees stated that “most of the pregnant women when growing up found
50

their mothers and relatives using traditional medicine during pregnancy and therefore they
too result in using the same”. Additionally 75% of the interviewees stated that “using TM use
during pregnancy help women to have a short time of pain when about to deliver”. Further,
majority 86% of the study interviewees stated that “when pregnant women take Traditional
medicine they do not vomit, avoid nausea and others bad feelings during pregnancy”. Finally,
25% of the interviewees stated that “after delivery women who use traditional medication in
order to have sufficient breast milk for the new born”.
The table 4.9 shows the themes that were constructed from the stated quotes and their
frequencies.
Table 4.6: Reasons for traditional medicine usage during pregnancy
Reasons Frequency (%)N=38 Percentage (%)Culture 14 38%Facilitate labor 29 75%Ease common discomforts during pregnancy 32 86%Enhance milk production after birth 10 25%
Table 4.9 indicate that 38% of the study interviewees stated that traditional medicine was
being used by pregnant women due to culture, 75% to facilitate labor, 86% to ease common
discomforts during pregnancy and 25% to enhance milk production after birth. In agreement
with the findings of the current study, a study conducted by Kim and Keng (2013) reported
that pregnant women used herbal medicines to shorten and ease labor and to relieve common
discomfort during pregnancy. A study conducted by Tamuno et al., (2010) found that
respondent’s reason for using herbal medicines was their culture to use the medication as a
traditional medicine. This is consistent with findings of the current study.
51

4.2.10 Stage of pregnancy at which women mostly use TM
The study sought to determine the stage in pregnancy when pregnant women most use
traditional medicine. The interviewees were asked to mention the stages of pregnancy at
which pregnant women mostly use TM. Eighty eight percent of the interviewees stated that
“most of women use TM during the first three months of their pregnancy”. Also, 62% of
them stated that “pregnant women use TM mainly during the fourth to sixth month of the
pregnancy”. Most (75%) of interviewees said that “traditional medicine is used by pregnant
women who are at their last months of their pregnancy”. Additionally a fair percentage of the
interviewees (38%) said that “pregnant women use traditional medicine all times during
pregnancy”. Table 4.10 display the analysis of their responses
Table 4.7: Stage of pregnancy at which women mostly use TM
Frequency (n=38) Percent (%)
1st Trimester 33 88
2nd Trimester 24 62
3rd Trimester 29 75
Throughout pregnancy 14 38
Table 4.10 indicates that 88% of the interviewees indicated that pregnant women use
traditional medicine during the first trimester, 62% stated that the use of TM is during second
trimester, 75% third trimester while 38% indicated that pregnant women use the TM
throughout the pregnancy.
4.2.11 Risk of using Traditional medicine
Table 4.11 indicates interviewees’ responses on the perceived risk of using traditional
medicine during pregnancy.
52
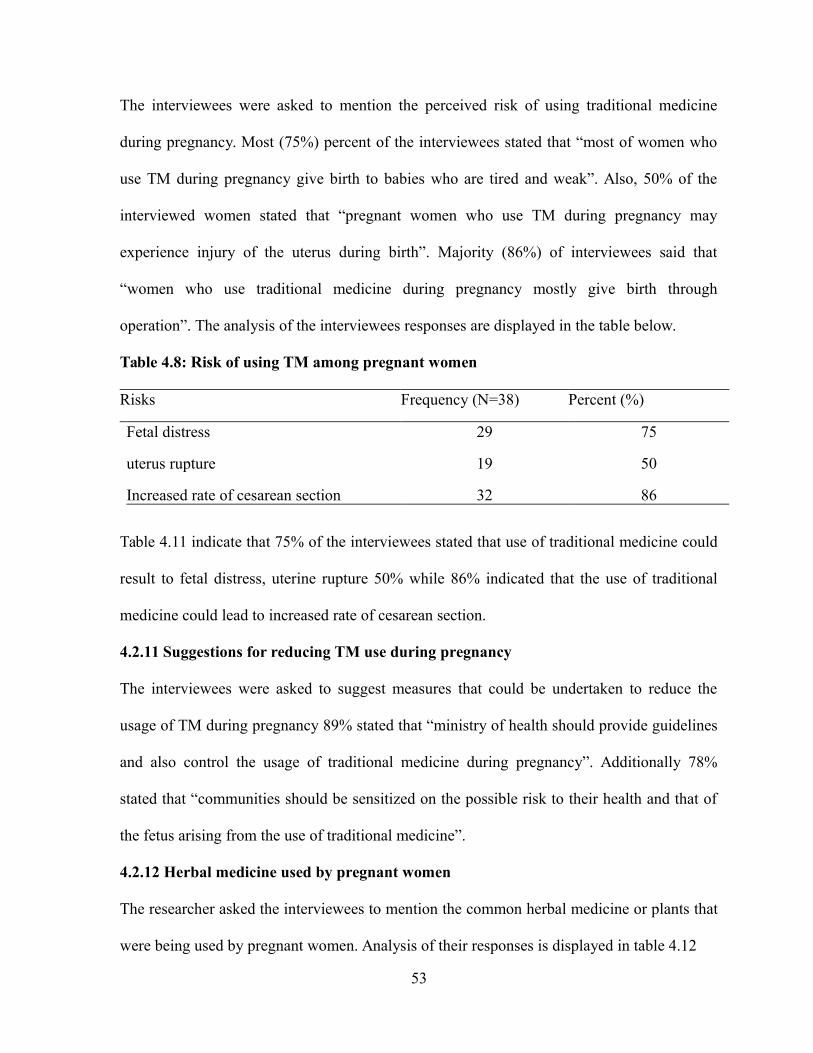
The interviewees were asked to mention the perceived risk of using traditional medicine
during pregnancy. Most (75%) percent of the interviewees stated that “most of women who
use TM during pregnancy give birth to babies who are tired and weak”. Also, 50% of the
interviewed women stated that “pregnant women who use TM during pregnancy may
experience injury of the uterus during birth”. Majority (86%) of interviewees said that
“women who use traditional medicine during pregnancy mostly give birth through
operation”. The analysis of the interviewees responses are displayed in the table below.
Table 4.8: Risk of using TM among pregnant women
Risks Frequency (N=38) Percent (%)
Fetal distress 29 75
uterus rupture 19 50
Increased rate of cesarean section 32 86
Table 4.11 indicate that 75% of the interviewees stated that use of traditional medicine could
result to fetal distress, uterine rupture 50% while 86% indicated that the use of traditional
medicine could lead to increased rate of cesarean section.
4.2.11 Suggestions for reducing TM use during pregnancy
The interviewees were asked to suggest measures that could be undertaken to reduce the
usage of TM during pregnancy 89% stated that “ministry of health should provide guidelines
and also control the usage of traditional medicine during pregnancy”. Additionally 78%
stated that “communities should be sensitized on the possible risk to their health and that of
the fetus arising from the use of traditional medicine”.
4.2.12 Herbal medicine used by pregnant women
The researcher asked the interviewees to mention the common herbal medicine or plants that
were being used by pregnant women. Analysis of their responses is displayed in table 4.12
53

Table4.9: Responses on common herbal medicine used by pregnant women
Herbal type Purpose Frequency Percentage (%)Igisura Umusura Relieve backache 29 76Umushishiro Ingando Relieve backache /lower
abdominal pain24 63
Ikinyamata Vomiting 32 83
Table 4.12 indicates that Igisura Umusura, Umushishiro Ingando, Ikinyamata and Inkuri are
among the herbal medications used by pregnant women.
54

CHAPTER FIVE: SUMMARY, CONCLUSION AND
RECOMMENDATIONS
5.0 Introduction
This chapter provides the summary of the findings conclusions drawn from the findings and
suggestions for further studies
5.1 Summary of Findings
5.1.1 Objective i: Prevalence of Traditional medicine usage among pregnant women
The study findings indicated that the prevalence of traditional medicine usage among the
pregnant women was 31%.The study findings indicated that 64% of the study participants
used traditional medicine due to culture, 85% to facilitate labor, 70% to ease common
discomforts during pregnancy and 57% to enhance milk production after birth. Also the
findings showed that 33% of the respondents buy the medication and prepare themselves,
28% obtain the medication from the tradition midwives, 31% from peers while 8% buy from
traditional healers.
5.1.2 Objective ii: Level of Knowledge regarding TM by pregnant women
The study findings indicated that 64% of the study respondents had good knowledge
regarding TM while 36% had poor level of knowledge regarding traditional medicine. The
study findings also indicated that majority (54%) of the study participants were sure of the
dosage of the medication they took while 46% were not sure of the dosage. Majority (66%)
thought that there were risks associated with the use of traditional medicine unlike 34% who
did not see any risk. Most of the respondents (73%) stated that they will continue to use
traditional medication in the future as opposed to 27%. Also, majority (72%) of the study
participants stated that they would prefer traditional medicine over conventional medicine.
55

Additionally, the findings showed that majority (45%) of the study participants obtained
information regarding to traditional medication from parents, 31% from tradition midwives,
17% from friends while 6% had relatives as their source of information regarding to
traditional medication.
5.1.3 Objective iii: Level of practice regarding TM by pregnant women
The study findings indicated that 68% of the study respondents had good level of practice
regarding traditional medicine while 32% had poor practice. Further, the findings showed
that 31% of the respondents were using traditional medicine, while 69% were not. Among
those who were using TM, 54% thought that they that they normally took the right dose of
the medication while 46% did not use the right dosage. Most of the respondents (73%) stated
that they will continue to use traditional medication in the future as opposed to 27%. Also,
majority (72%) of the study participants stated that they would prefer traditional medicine
over conventional medicine while 28%prefer conventional medicine over traditional
medicine
5.2 Conclusion
Traditional medication usage is still being held as an important practice among the pregnant
women in Kibagabaga. This is evidenced by the fairly high prevalence of TM usage by
pregnant women studied. The level of knowledge and practice regarding TM use during
pregnancy is good. Also the study concluded that most of the women using traditional
medication are not aware of the risks associated with TM use. The consumers are also not
well conversant with the dosage of the medication. Sources of information regarding
traditional medication utilized by pregnant women include; parents, traditional midwives,
friends and relatives. Reason that may influence pregnant women attending Kibagabaga
56

hospital to use traditional medicines includes, culture, to facilitate labor, to ease common
discomforts during pregnancy and to enhance milk production after birth. Also traditional
medicines used by pregnant women attending Kibagabaga hospital are bought and prepared
by pregnant women themselves, obtained from tradition midwives or from peers.
5.3 Recommendations
Pregnancy care providers should be aware of the common traditional medicines used and the
need to know with evidence-based research regarding potential benefits or harmful side
effects of the medications. Obstetricians should advise women not to expose their unborn
babies to the risks of herbal medicines. Further, documentation of knowledge regarding the
use of various common traditional medication are needed, as information gathered could help
in educational intervention essential to the Rwandan healthcare system. Community
mobilization is needed to ensure that information on the risks and safety of traditional
medicines to the fetus and mother in pregnancy are well known by the women. There is also
a need for health care providers to counsel pregnant women on possible dangers of traditional
medicines use.
5.4 Suggestions for further study
This study recommended the following areas for further study;
1. The study suggests that a detailed study to establish the efficacy and safety of the
common tradition medicines especially herbal medicine to ensure the well-being of
the mother and fetus.2. Further the study suggests that a study that would evaluate the risk associated with
traditional medication use during pregnancy should be conducted. This will instill
confidence in women who may fear to use TM due to unknown risks, Also such study
57

would ensure that pregnant women make choice to use of not to use traditional
medication basing on known facts
58
REFERENCES
Abrahams, N., Jewkes R & Mvo Z, (2002) Indigenous healing practices and self medication
amongst pregnant women in Cape Town South Africa. African journal of
reproductive health 6 (2):79-86.
Adams, J., (2011) Growing popularity of complementary and alternative medicine during
pregnancy and implications for healthcare providers; Review obstetric gynecology,
(4):365-366.
Al-Riyami IM, Al-Busaidy IQ, Al-Zakwani IS, (2011) Medication use during pregnancy in
Omani women, International Journal Clinical Pharmacology, 33(4): 634-41.
Ang-Lee MK, Moss J, Yuan, CS., (2001) Herbal medicines and perioperative care.
Journal of American medical Association; 286: 208–16.
Alrawi, N. & Fetters, M., (2012), Traditional Arabic & Islamic medicine: a conceptual
model for clinicians and researchers. Global Journal of Health Science 4 (3):164-169.
Apgar V., (1953) proposal for a new method of evaluation of the newborn infant. Current
Research on Anesthesia Analgesics; 32:260-267.
Baggley, A., Navioz, Y., Maltepe, C., Koren, G., Einarson, A., (2004) Determinants of
women’s decision making on whether to treat nausea and vomiting of pregnancy
pharmacologically. Journal of midwifery Womens Health: (49) 350–354.
Banhidy, F, Lowry, R.B., Czeizel, A.E., (2005) Risk and benefit of drug use during
pregnancy; International Journal of Medical Science:( 2), 100–106.
Bannerman H., Burton J., & Wen-Chieh C., (1983) Traditional medicine in health
care: coverage a reader for health administrators and practitioners: WHO, Geneva,
The Journal of Modern African Studies: 342.
59
Barbee, E., (1986) Biomedical resistance to ethnomedicine in Botswana; Social Science
& medicine 22 (1): 75-80.
Barnes J., (2003) Quality, efficacy and safety of complementary medicines: fashion
facts and the future. part1, regulation and quality, British journal of clinical
Pharmacology; 226-233.
Barnes J., (2013) New approaches and perspectives in pharmacovigilance for herbal
Medicines. European Journal Clinical pharmacology 36(1):1-12.
Barnes, PM., Bloom b Nahin R L., (2007) Complementary and alternative medicine use
among adults: United States, The American journal of medicine;( (343):1–19, Vol. 2,
No. 254-71.
Bayles B., (2007) Herbal and other complementary medicine use by Texas midwives
Journal of Midwifery & Women's Health 52(5):473-8.
Bamidele, O., Wasiu, A., Edward, O. (2009) Knowledge, attitude and use of
alternative medical therapy amongst urban residents of Osun state, south western
Nigeria; African Journal of Traditional, Complementary and Alternative Medicine;
(6):281–288.
Bent, S., (2004) Commonly used herbal medicines in the United States: The American
journal of medicine ;( 116):478–85.
Bent S., Padula A., Neuhaus, J., (2004) Safety and efficacy of citrus aurantium for
weight Loss; American journal of cardiology; (94): 1359–61.
Bercaw, J., Maheshwari B., Sangi Haghpeykar H., (2010) The use during pregnancy of
60

Prescription over the counter, and alternative medications among Hispanic women;
Birth 37 (3):211-218.
Cunningham, A.B. ( 1993) African medicinal plants: setting priorities at the interface
Between conservation and primary health care, working paper 1, UNESCO,
Paris.
De Smet., (2002) Herbal remedies; Northern England journal of Medicine; (347):2046–
56.
Deborah, E., McCarter M., Spaulding M S., (2005) Medications in pregnancy and
lactation, American journal of maternal child nursing (30), 10–17.
Dugoua, J., (2010) Herbal medicines and pregnancy; Journal of Medicine, 1686-1692
Drew A K., (1997) Safety Issues in Herbal Medicine: Implication for the Health
Progression; Medical journal of Australia; 166: 538.
Edzard Ernst, Igbo Onakpoya, Lucy Davies., (2011) Efficacy of herbal supplements
containing Citrus aurantium and synephrine alkaloids for the management of
overweight and obesity: a systematic review; Focus on Alternative and
Complementary Therapies. Volume 16(4); 254–260.
E I C C A M., (2008) European information centre for complementary and alternative
medicine: Retrieved on 25th June, 2016 from
www.eiccam.eu/pdfs/eiccambrochurecomplete.pdf.
Ewles L & Simnett I (2003) Promotion in practice: Promoting Health, A practical guide
to health education; Health Education Journal; (5e); London: Bailliere Tindall.
Ernst E., (2002) Prevalence of the use of complementary/alternative medicine:
61

a systematic review. Bulletin of the World Health Organization (78):252-257.
Ernst E., (2002) Herbal medicinal products during pregnancy: are they safe? British
Journal of obstetrics and gynecology; (109): 227–35.
Ernst E., (1998) Harmless herbs? A review of the recent literature: American Journal of
Medicine: (104):170–8.
Ernst E., (2006) Herb Drug Interactions, Potentially Important but Woefully Under
Researched; European Journal Clinical pharmacology; (56): 523 – 4.
Feierman S. (1986) Popular control over the institutions of health, a historical
study; The professionalization of African medicine. Manchester: Manchester
University Press. pp. 205-220.
Fakeye T & Adisa R., (2009) Attitude and use of herbal medicines among pregnant
women in Nigeria. Biomedical central, complementary alternative medicine; (9): 53.
Foster, G., (1976) Disease etiologies in non-western medical systems, American
anthropology; 773-782.
Freeman, M. & Motsei M., (1992) Planning health care in South Africa is there a role for
traditional healers? Social Science and Medicine 34: 1183-1190.
Gharoro E & Igbafe A., (2000) Pattern of drug use among antenatal patients in Benin
City; Nigeria Medical Science Monitor, 6: 84 – 87.
Glover, D., Amonkar, M. Rybeck, B.F. Tracy, T.S. (2003) Prescription, over the
counter, and herbal medicine use in a rural, obstetric population; American journal of
obstetrics &gynecology; 188, 1039–1045.
Good C., (1987) Ethnomedical systems in Africa: patterns of traditional medicine in
62

rural and urban Kenya; New York: Guilford Press. 354.
Gonçalves, R., (2001) Assessment of Maternal and Fetal outcomes following ingestion of
herbal remedies; A M F I H R Study Protocol; Pretoria.
Government of Rwanda (Ministry of Health, 2013) HMIS Health Facilities database
Guba, G., (1981) Criteria for assessing the trustworthiness of naturalistic inquiries;
Educational technology research & development; 29 (2), 75-91.
Gumede M., (1990) Traditional healers: a medical doctor’s perspective.
Johannesburg: Skotaville.
Hammerness P., Basch E., Ulbricht C et al., (2003) St.John’swort systematic review of
Adverse effects and drug interactions for the consultation psychiatrist;
Psychosomatics; (44):271–82.
Haram L. (1991) Tswana medicine in interaction with biomedicine; Social Science
Medicine 33 (2): 167-175.
Hoffman B., Taylor P., (2001) Neurotransmission in Hardman JG, Limbird LE, Goodman
and Gilman’s; The pharmacological basis of therapeutics. New York, NY: McGraw-
Hill: 115–53.
Holst L., Nordeng H., Haavik S., (2008) Use of herbal drugs during early pregnancy in
relation to maternal characteristics and pregnancy outcome. Pharmacoepidemiology
Drug Safety; 17(2):151-159.
Jewkes, R., Abrahams, N. and Mvo, Z. (1998b) Why do nurses abuse patients?
Reflections from the South African obstetric services; Social Science Medicine 47
(11): 1781-1795.
63

Janzen M., (1978) The comparative study of medical systems as changing social
Systems; social science and medicine; Part b: medical anthropology, 12, 121–129.
Kacew S., (1994) Fetal consequences and risks attributed to the use of prescribed
and over-the-counter (OTC) preparations during pregnancy. International Journal of
Clinical Pharmacology and Therapeutics; (32): 335–343.
Kamatenesi Mugisha M., Oryem Origa H., (2007). Medicinal plants used to induce
labour during childbirth in western Uganda. Journal of Ethnopharmacology; (109):1–
9.
Kamuhabwa & Rashid Jalal., (2011) Drug use in pregnancy: Knowledge of drug
dispensers and pregnant women in Dar es Salaam, Tanzania; Indian Journal of
Pharmacology Vol: 43 Issue: 3, Pg: 345-349.
Kooi, R, & Theobald S., (2006) Traditional medicine in late pregnancy and labor:
Perceptions of kgaba remedies amongst the Tswana in South Africa. African journal
of traditional, complementary and alternative medicines Volume 3, no 1.
KOR J., (1998) Adulterant in Asian patent medicines; New England Journal of Medicine,
Kristoffersen S et al, (1996) Uptake of alternative medicine; Lancet,(347): 972 339; 847:12.
Ito S., Koren, G., Einarson T., (1993) Maternal non-compliance with antibiotics
during breastfeeding; Annals of Pharmacotherapy 27: 40–42.
Laverack G., (2007) Health Promotion Practice, Building Empowered Communities.
Open University Press.
Landy D., (1977) Culture disease and healing: Macmillan; New York. Chapters 2, 5,
14, 16, 17, 20, 21, 25.
64

Lindzon G, Sadry S, Sharp J. (2011) Obstetric in Toronto notes for medical students.
27th Edition; Type & graphics inc. Canada
Lisa M. Vaughn, Farrah Jacquez and Raymond C. Baker; (2009) The Open Medical
education Journal. , 2, 64-74.
Mabina M., (1997) The effect of traditional botanical medicines on pregnancy outcome:
Melton, M., (1995) Take two aspirin or not? Risk of medication use during pregnancy;
Mother Baby Journal 4:25-32.
Morris, J., Burke, V., Mori, T.A., Vandongen, R., Beilin, L.J., (2003) Effects of garlic
extract on platelet aggregation: a randomized placebo controlled double-blind study.
Clinical and Experimental Pharmacology and Physiology, (22): 414-417.
Mugenda, M. & Mugenda, G. (2003) Research Methods: Quantitative and Qualitative
Approaches; Nairobi University Press.
Nelms L W & Gorsk J. (2006) The role of the African traditional healer in women’s
health; Journal of Trans-cultural Nursing; (17): 184-189,
Nordeng, H., Koren, G., Einarson, A., (2010a) Pregnant women’s beliefs about
medications a study among 866 Norwegian women. Ann. Pharmacotherapy. 44,
1478–1484.
Nortier J., (2000) Urothelial Carcinoma Associated with the Use of a Chinese Herb.
New Obstetrics and Gynecology, 443-443.e6.CE Test: Herb Use in Pregnancy.
Odalovic M., Vezmar, Kovacevic S., Ilic, K., Sabo, A., Tasic, L. (2012) Drug use before
and during pregnancy in Serbia. International journal of clinical pharmacology: (34),
719–727.
Olson, J & Nkiwane S., (2006) Integrate for Efficiency; Traditional Yoruba medicine
in Nigeria, GS 218 introduction to Africa; Colorado College.
65

Parke G & Roope R., Turner S.,(2009)General practitioners' use of sickness; General
practitioners and occupational health services 10: 254–269. 21.
Pinkoane M & Greeff M., (2012) A model for the incorporation of traditional healers into the
national healthcare delivery system of South Africa; Focus on Alternative and
Complementary therapies. African Journal of traditional Complement Alternative
Medicine; 9(3S):12-18.
Posey, D. & Dutfield G., (1996) Beyond intellectual property: towards traditional resource
rights for indigenous peoples and local communities, Ottawa, Canada; international
Development Research Centre, Republic of Rwanda., (2012): Nyamasheke.
Rotblatt M & Ziment I., (2002) Evidence-based herbal medicine; Philadelphia, PA:
Hanley & Belfus Sachdeva, P., Patel, B.G., Patel, B.K., (2009 Drug use in
pregnancy; a point to ponder! Indian Journal of Pharmacology Science (71), 1–7.
Shekelle P, Mary L, Sally C., Margaret M., Walter A,, Marika J. Shannon L., Lara J James
G., (2003) Efficacy and safety of ephedra and ephedrine for weight loss and athletic
performance: a meta-analysis: Journal of the American medical asociation1537–45.
Safowora, A., (1982) Medicinal Plants and Traditional Medicine in Africa, John Wiley
and Sons Limited, Chichester.
Sattari M, Dilmaghanizadeh M, Hamishehkar H, Mashayekhi SO (2012) Self-reported Use
and Attitudes Regarding Herbal Medicine Safety during Pregnancy in Iran.
Jundishapur Journal of Natural Pharmacological products; 7(2): 45-9.
Singh Y., (2005) Potential for interaction of kava and St. John's wort with drugs; Journal
of Ethnopharmacology; (100) (1-2):108-13.
66

Snow L F., (2008) Traditional health beliefs and practices among lower class black
Americans, In Cross-cultural medicine, Western Journal of Medicine; (198); 139:820-
828. Therapeutics, 239-244.
Stickel F, Patsenker E & Schuppan D., (2005) Herbal hepatotoxicity; Journal of
Hepatology; 43:901–10.
Tabatabaee M, (2011) Use of herbal medicine among pregnant women referring to Valiasr
hospital in Kazeroon, Fars, South of Iran. Journal of Medicinal Plants 1(37): 96-108.
Tamuno I et al., (2011) Use of herbal medicine among pregnant women attending a
tertiary hospital in Northern Nigeria. International journal of Gynecology and
obstetrics 15(2), 10.5580/2932.
Varga C. & Veale H., (1997) Isihlambezo: Utilization patterns and potential
health effects of pregnancy related traditional herbal medicine. Social Science
Medical (44): 911-24.
Vickers, A. and C. Zollman., (1999) ABC of complementary medicine: Herbal medicine.
Biomedical journal ;( 319): 1050 – 3.
Walter V. Reid et al., (1993) Biodiversity Prospecting: using genetic resources for
sustainable development, World Resources Institute (WRI).
Williams J., Myson, V., Steward, S., Jones, G., Wilson, J., Kerr, P., Smith, E.,
(2002) Self-discontinuation of antiepileptic medication in pregnancy: detection by
hair analysis. Epilepsia (43); 824–831.
W H O, (2002) Traditional medicine strategy, World Health Organization, Geneva
Switzerland, 2002.
67

W H O, (2006) The World Health Report, working together for Health, World Health
Organization.
W H O, (2009) Traditional medicine in the WHO African region, WHO African region,
Brazzaville.
W H O., (2005) WHO traditional medicine strategy; Geneva, WHO, 2002
(Document reference WHO/EDM/TRM/2002.1).
W H O, (2008) Traditional medicine; Geneva, Retrieved on
http://www.who.int/medicines/areas/traditional/en/. Accessed June 30th 2016.
WH O, (2013) Traditional medicine Fact sheet Number 134: Retrieved on 4th February
from http:/www.who.int/mediacentre/factsheets/fs134/en.
W H O, (1978) Alma Ata declaration; primary health care: health for all series; no.1.
W H O., (2005) National policy on traditional medicine and regulation of herbal
medicines: report of a world health organization global survey: 1–168.
W H O., (2008) Traditional medicine; fact sheet number 134: retrieved from
www.who. int/media centre/factsheets/fs134/en/ on 15 July 2016.
68

APPENDIX I: QUESTIONNAIRE
Please fill in the required information and only the most you think is the right answer
Section 1
Socio-demographic
information
What is your age (years)? 18-35 years ( )>35 years ( )
What is your marital status?Married ( ) Unmarried ( )
Which is your religion?Christian ( )Muslim ( ) Others ( )
Which is your educational level?None ( )Primary school( )Secondary school( )university( )
Gravidity1 ( )2-4 ( )>4 ( )
Tick only the MOST appropriate answer
Section 2
Knowledge
on TM
Statement Yes NoDo you thing that TM could be harmful to your health
Do you think that the TM is dangerous to the health of the fetusDo you have information regarding the tradition medicine you useDo you know how the TM you use is prepared
Section 3
Information
on Practice of
Statement Yes NoDo you use TM?
If you are using TM will you continue to use traditional medication
Would you prefer traditional medicine over conventional medicine
69

TM Section 4
Sources of
herbal
medicines
Buy and self preparedTradition midwivesPeersBuy from tradition healers
Source of
information
regarding TM
ParentsTraditional midwives Friends Relatives
Statement
Stro
ngly
Agre
e %
Agre
e %
Dis
agr
ee%Education level of pregnant women influences their knowledge and practices
regarding traditional medicineReligion of pregnant women influences their knowledge and practices
regarding traditional medicineFamily and friends can influence knowledge and practices of pregnant women
regarding traditional medicineSocio-economic factors can influence knowledge and practices of pregnant
women regarding traditional medicine
70
APPENDIX II: IN-DEPTH INTERVIEW GUIDE
1. In your opinion do you think pregnant women use TM
2. What do you think are the reasons for the use of TM among pregnant women
3. In which stage of pregnancy do you think most women use TM?
4. What do you think could be the effect of TM use during pregnancy
5. What do you think should be done to reduce use of TM among women?
6. Indicate the type and purpose of TM you used
71