
Knee Pain/OA Physical Therapy Approaches · Knee Pain/OA Physical Therapy Approaches G. Kelley...
42
Department of Physical Therapy Knee Pain/OA Physical Therapy Approaches G. Kelley Fitzgerald, PT, PhD, FAPTA Professor, Department of Physical Therapy, School of Health and Rehabilitation Sciences Director, Physical Therapy Clinical and Translational Research Center
Transcript of Knee Pain/OA Physical Therapy Approaches · Knee Pain/OA Physical Therapy Approaches G. Kelley...

Department of Physical Therapy
Knee Pain/OA Physical Therapy ApproachesG. Kelley Fitzgerald, PT, PhD, FAPTA
Professor, Department of Physical Therapy, School of Health and Rehabilitation SciencesDirector, Physical Therapy Clinical and Translational Research Center

Department of Physical Therapy
• Dosage
• Manual Therapy
• Motor Learning

Department of Physical Therapy
Strength Training Dosage
• % of a repetition maximum
• Perceived Exertion Scales
• For our patients with arthritis, these should be “pain-free” entities

Department of Physical Therapy
Strength Training Dosage• American College of Sports Medicine
Recommendations for Older Adults– 60-80% 1 RM, 8-12 reps, 1-3 sets, with 1-3
min rest between sets.
– Can also incorporate power programs of 30-60% 1 RM, 6-10 reps, 1-3 sets at higher repetition velocity.
– For endurance training, use lighter loads (50-60%) with higher reps (10-15 or more)

Department of Physical Therapy
Progression of Strength Training Intensity
• When patient can perform 1-2 reps over the target reps for 2 consecutive sessions, training load should be increased by 2 to 10%.
• Recommend re-establishing the 1 RM every 2 to 4 weeks to re-adjust training loads appropriately.

Department of Physical Therapy
Alternative to Repetition Maximum for Dosing
• Modified Borg Perceived Exertion Scale
Borg Perceived Exertion Scale0 Nothing at all
1 Very light
2 Fairly light
3 Moderate
4 Somewhat Hard
5 Hard
6
7 Very Hard
8
9
10 Very very hard
Borg, G. (1982) Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise, 14 (5), p. 377-81

Department of Physical Therapy
Alternative to Repetition Maximum for Dosing
• Emphasize gains in muscle force output
• Increase resistance as patient progresses and RPE falls below desired level.
Borg Perceived Exertion Scale0 Nothing at all
1 Very light
2 Fairly light
3 Moderate
4 Somewhat Hard
5 Hard
6
7 Very Hard
8
9
10 Very very hard

Department of Physical Therapy
Alternative to Repetition Maximum for Dosing
• Emphasize gains in endurance
• Increase resistance as patient progresses and RPE falls below desired level.
Borg Perceived Exertion Scale0 Nothing at all
1 Very light
2 Fairly light
3 Moderate
4 Somewhat Hard
5 Hard
6
7 Very Hard
8
9
10 Very very hard

Department of Physical Therapy
• Potential Advantages of RPE– Can dose without need
for major testing equipment
– Easy to teach patient for independent exercise and activity programs
• Potential Disadvantages of RPE– Not yet known if it will
produce the same strength outcomes as %RM approach
Alternative to Repetition Maximum for Dosing

Department of Physical Therapy
Aerobic Training Dose• 30 to 60 minutes per week
• 50-70% of heart rate reserve (HRR)
• Target HR = 220- Age –(Resting HR x %HRR) + Resting HR
• Example: 60 y/o with resting HR of 80, exercise at 60% of HRR:
220 – 60 – (80 X .60) + 80 =128 beats/min

Department of Physical Therapy
Manual Therapy
• Techniques include accessory and physiologic motion techniques, manual stretching techniques, and soft tissue manipulation techniques

Department of Physical Therapy
Examples of Manual Therapy Techniques
P-A glide of tibia on femur with medial tibial rotation: Target
anterior-lateral capsule
Manually applied stretch to the hamstrings and posterior
capsule

Department of Physical Therapy
Examples of Manual Therapy Techniques
Accessory Motion: Patellofemoral inferior glides
Soft tissue manipulation with manual stretching

Department of Physical Therapy
Manual Therapy: Joint Mobilization • Can be used to induce relaxation and reduce
pain (grades 1 and 2)
• Can be used to improve joint mobility (grades 3-5)
• Objective of treatment is to manually reproduce joint accessory motions such as distractions and joint surface translations.
• Can also be used to apply more targeted stretching of joint capsule
Moss P, et al, Manual Therapy. 2007;12:109-118Deyle G, et al, Phys Ther. 2005;85:1301-1317

Department of Physical Therapy
Joint Mobilization: Indications
• Hypomobility on accessory motion testing (reproduction of joint translatory movements)
• Measureable reduction in joint motion even after de-emphasizing contribution from tight muscles
• Pain/stiffness in specific portions of the peri-articular soft tissue on joint motion

Department of Physical Therapy
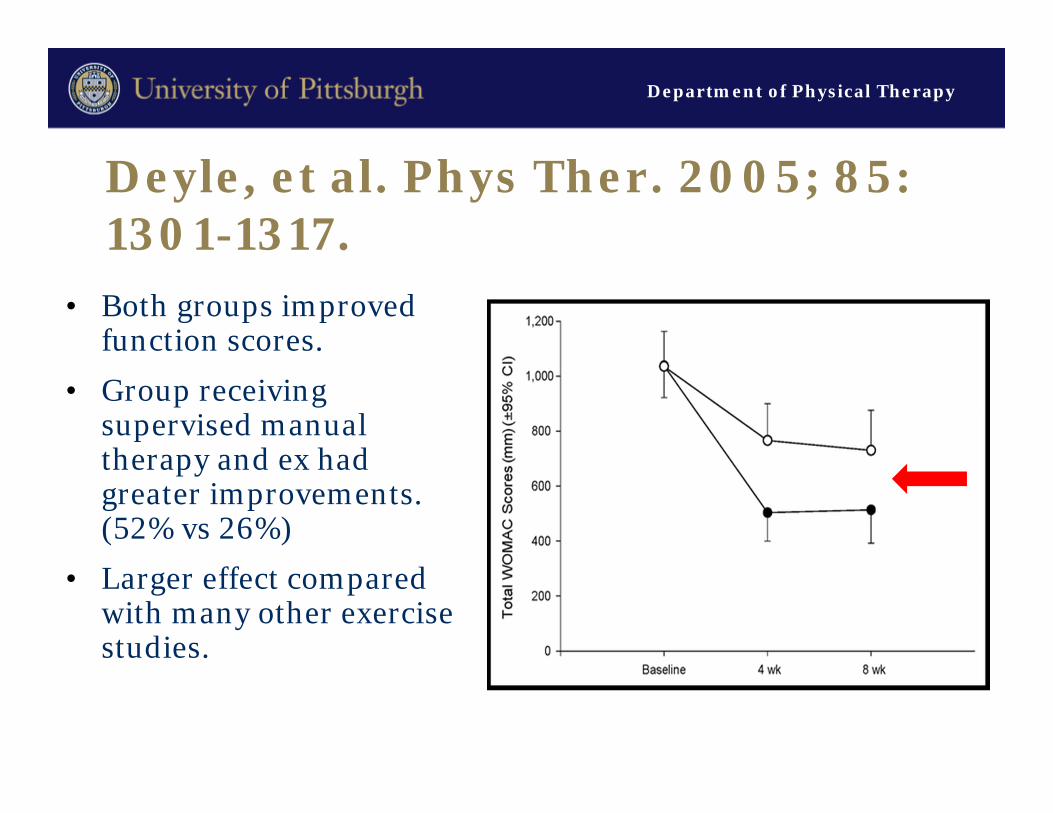
Deyle, et al. Phys Ther. 2005; 85: 1301-1317.
• Compared group with knee OA receiving supervised manual therapy and exercise to group receiving home exercise.
• Manual therapy and exercise delivered to lumbo-pelvic, hip, knee, foot and ankle regions based on reduced motion or pain in these regions.
Department of Physical Therapy
Deyle, et al. Phys Ther. 2005; 85: 1301-1317.
• Both groups improved function scores.
• Group receiving supervised manual therapy and ex had greater improvements. (52% vs 26%)
• Larger effect compared with many other exercise studies.
Department of Physical Therapy
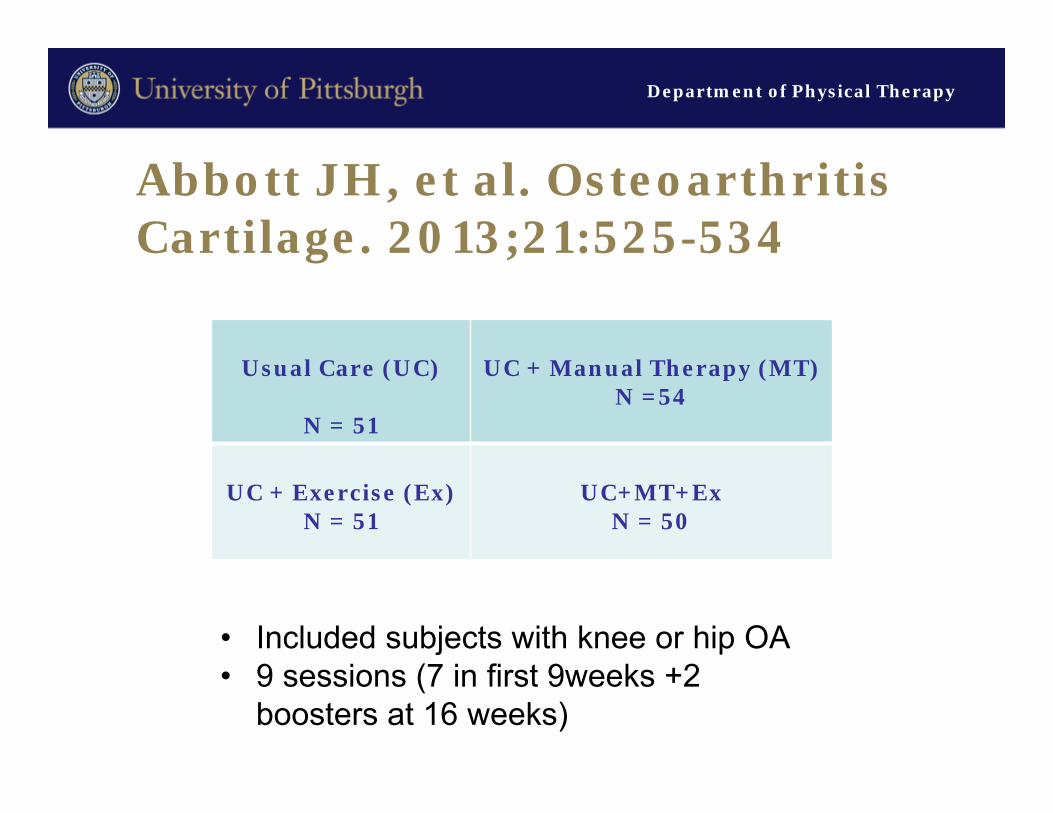
Abbott JH, et al. Osteoarthritis Cartilage. 2013;21:525-534
Usual Care (UC)
N = 51
UC + Manual Therapy (MT)N =54
UC + Exercise (Ex)N = 51
UC+MT+ExN = 50
• Included subjects with knee or hip OA• 9 sessions (7 in first 9weeks +2
boosters at 16 weeks)

Department of Physical Therapy
Abbott JH, et al. Osteoarthritis Cartilage. 2013;21:525-534
ONE YEAR FOLLOW-UP CHANGES
UC MT Ex MT + Ex
WOMAC -12.9 (51.8)
-41.4 (55.5)
-29.3 (50.4)
-27.4 (41.1)
30s sit to stand (# stands)
.02 (-.79;.84)
.67(-.12;1.45)
1.6(.80;2.40)
1.59(.60;2.59)
40m walk (sec) .78(-1.40;2.95)
-.50(-3.70;2.70)
-3.18(-4.41; -1.99)
-.61(-2.22; 1.00)
NNT* 5 6 8* Number needed to treat for achieving responder to treatment status based on OMERACT-OARSI responder criteria

Department of Physical Therapy
Enhancing the Effectiveness of Physical Therapy in People with Knee Osteoarthritis1 RO1 HS019624-01
University of Pittsburgh, Pittsburgh PA- Data Coordinating Center (PI: G. Kelley Fitzgerald)
Other Study Sites:
University of Utah/Intermountain Healthcare, Salt Lake City, UT (PI: Julie M. Fritz)
Army-Baylor University, San Antonio, TX (PI: John Childs)
University of Otago, Dunedin NZ (PI: Haxby Abbott)

Baseline TestingSummary of Experimental Design
R
Exercise MT +Exercise Exercise +Booster
MT+ Exercise +Booster
12 Rx Sessions 12 Rx Sessions 8 Rx Sessions 8 Rx Sessions
9 Wk F/U
9 Wk F/U
9 Wk F/U
9 Wk F/U
Home Program Home Program Home Program Home Program
5 mo Booster – 2Rx 5 mo Booster – 2Rx
8 mo Booster – 1Rx 8 mo Booster – 1Rx
11 mo Booster – 1Rx 11 mo Booster – 1Rx
1 YR F/U 1 YR F/U1 YR F/U 1 YR F/U
2 YR F/U 2 YR F/U2 YR F/U 2 YR F/U

Department of Physical Therapy
Motor Learning Approaches
• Biomechanical unloading
• Task Specific Training

Department of Physical Therapy
Contralateral Cane Use
• ↓ KAM by 7-10%• ↓ cumulative loading by:
– ↑ stride length
– ↓ cadence
• ↓ GRF by 25%-35% during gait
• Most effective if placed as far laterally as possible without inducing sx.

Department of Physical Therapy
Gait Retraining Approaches
• Goal to reduce knee adduction moment
• Foot progression angle (toe out)
• Trunk sway (lateral)

Department of Physical Therapy
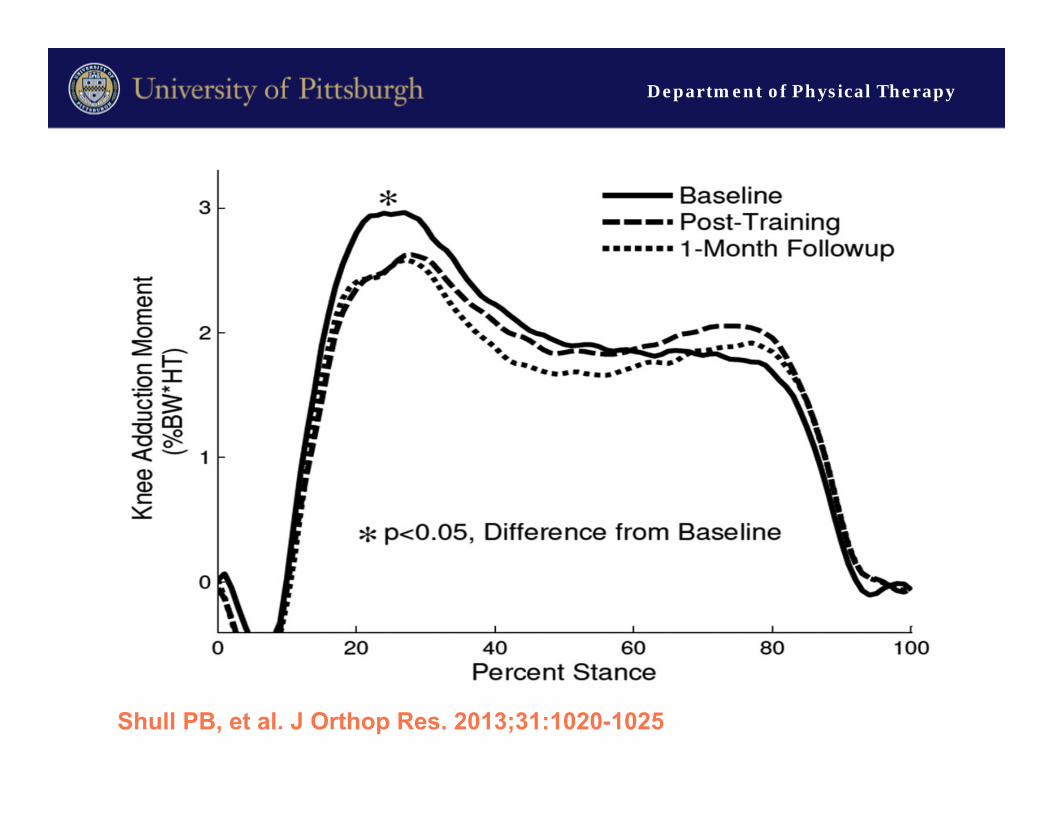
• Motion capture and instrumented treadmill
• Patient tailored altered foot progression angle or lateral trunk to get 10% ↓ in KAM
• Vibration motors on tibia (foot angle) and scapula (trunk sway) for feedback during training
Shull PB, et al. J Orthop Res. 2013;31:1020-1025

Department of Physical Therapy
• 1x/week, 6 weeks
• 10 min practice daily
• Subject selected method of alteration– Foot progression angle
– Trunk sway
– Both
• Fading feedback training design
Shull PB, et al. J Orthop Res. 2013;31:1020-1025
Department of Physical Therapy
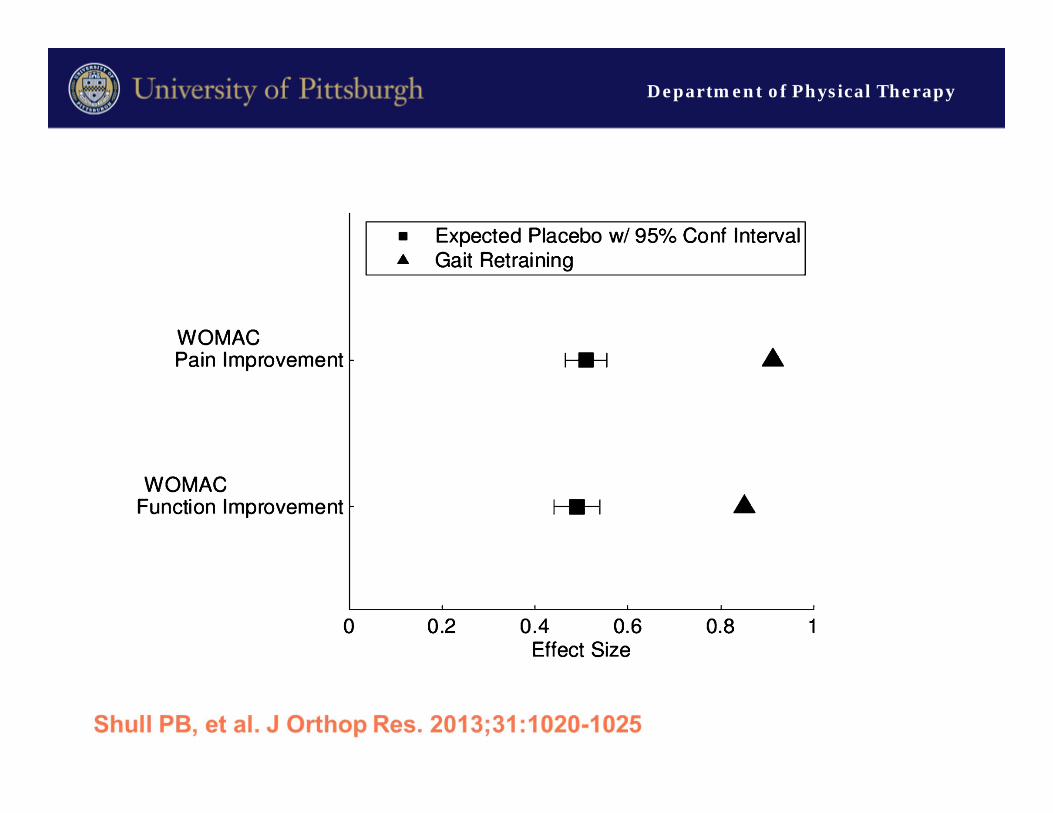
Shull PB, et al. J Orthop Res. 2013;31:1020-1025

Department of Physical Therapy

Department of Physical Therapy
Department of Physical Therapy
Department of Physical Therapy
Task-Specific Training
Department of Physical Therapy
Traditional Premise
↓Physical Function +
Performance

Department of Physical Therapy
Traditional Premise
↑Physical Function +
Performance
Department of Physical Therapy
Fitzgerald GK, White DK, Piva SR. Associations for change in physical and psychological factors and treatment response following exercise in knee osteoarthritis: An exploratory study. Arthritis Care Res. 2012;64:1673-1680
• Changes in impairments (muscle strength, flexibility, joint mobility) not associated with clinical outcome of pain and function in subjects with knee OA.

Department of Physical Therapy
Teixeira PEP, Piva SR, Fitzgerald GK. Effect of impairment-based exercise on performance of specific self-reported functional tasks in individuals with knee osteoarthritis. Phys Ther. 2011;91:1752-1765
• Impairment-based rehabilitation approach yielded only modest self-reported improvements in functional task performance ability

Department of Physical Therapy
Task-Specific Training
• Use the specific task that is problematic as the training tool
• Can work on strength and joint mobility in context of the task
• Provide opportunity to improve motor patterns in context of task
• May consider task modifications

Department of Physical Therapy
Chair Rise Task Step 1: Moving to Edge of Seat

Department of Physical Therapy
Chair Rise Task Step 2: Lift Off

Department of Physical Therapy
Chair Rise TaskStep 3: Terminal Stand

Department of Physical Therapy
Chair Rise TaskFull Task Practice
Department of Physical Therapy
Floor Transfers

Department of Physical Therapy
THANK YOU!!!


















