
Knee Joint - Doctor 2017 - JU Medicine
43
Knee Joint Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
Transcript of Knee Joint - Doctor 2017 - JU Medicine

Knee Joint
Dr. Heba Kalbouneh
Associate Professor of Anatomy and Histology

Articulation between
the femur and tibia
(weight- bearing)
Articulation between
the patella and patellar
surface of femur
Allows the pull of
quadriceps femoris to
be directed anteriorly
over the knee to the
tibia without tendon
wear
Knee joint is the largest synovial joint
in the body. Consists of two joints:
Knee joint Articulating surfaces:
Quadriceps
tendon
Patellar
ligament

Tibiofemoral joint
Modified synovial hinge
(bicondylar)
Allows flexion and
extension with some
degree of medial and
lateral rotation
Patellofemoral joint
Plane gliding joint
Type:

Capsule:
The capsule is attached to the margins of
the articular surfaces and surrounds the
sides and posterior aspect of the joint.
On the front of the joint, the capsule is
absent. The capsule is completed
anteriorly by patella, ligamentum patellae,
medial and lateral patellar retinacula
Posterior view of the knee

On each side of the patella, the
capsule is completed anteriorly by
expansions from the tendons of
vastus lateralis and medialis
forming Medial and Lateral patellar
retinacula
Patellar ligament
Medial patellar
retinaculum Lateral patellar
retinaculum
The ligamentum patellae is
attached above to the lower
border of the patella and below
to the tuberosity of the tibia.

Ligaments:
Extracapsular ligaments:
Ligamentum patellae
Lateral collateral ligament
Medial collateral ligament
Oblique popliteal ligament
Intracapsular Ligaments
(within the joint cavity):
Anterior Cruciate Ligament
Posterior Cruciate Ligament
The ligaments may be
divided into those that lie
outside the capsule
(extracapsular) and those that
lie within the capsule
(intracapsular)

The lateral collateral ligament is
cordlike and is attached above to the
lateral femoral epicondyle and below
to the head of the fibula.
The medial collateral ligament is
a flat band and is attached above to
the medial femoral epicondyle and
below to the upper medial surface
of tibia.
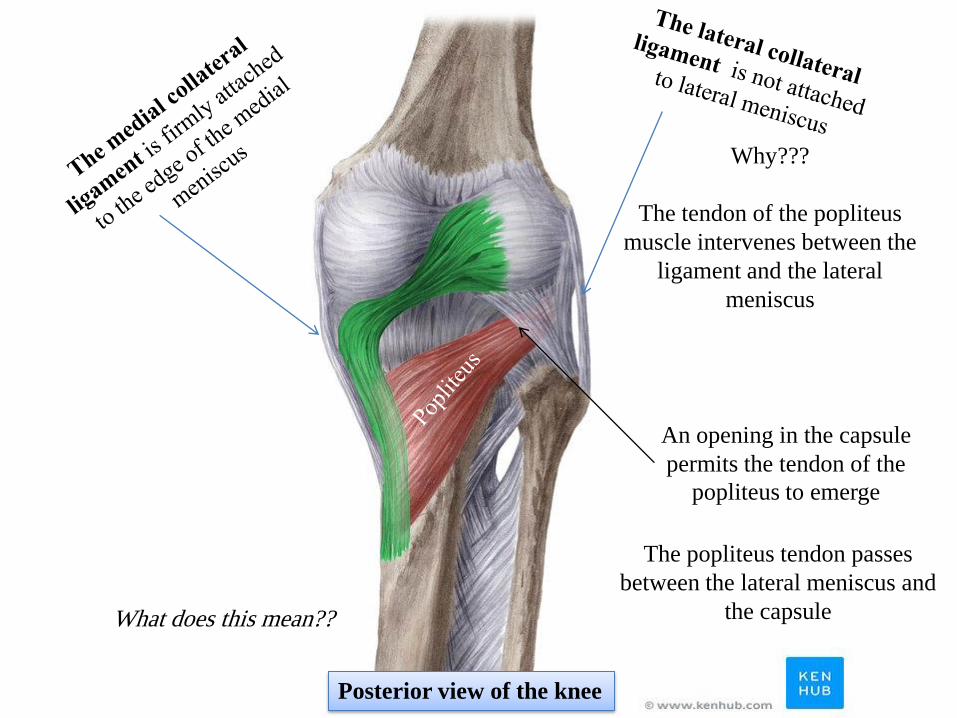
Why???
The tendon of the popliteus
muscle intervenes between the
ligament and the lateral
meniscus
What does this mean??
Posterior view of the knee
An opening in the capsule
permits the tendon of the
popliteus to emerge
The popliteus tendon passes
between the lateral meniscus and
the capsule
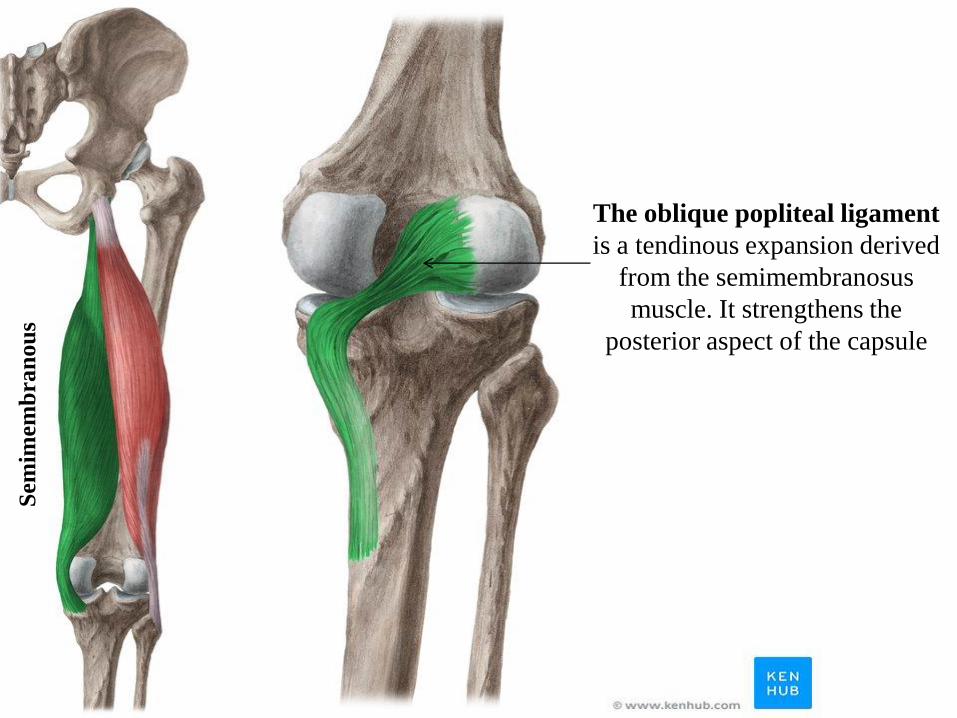
The oblique popliteal ligament
is a tendinous expansion derived
from the semimembranosus
muscle. It strengthens the
posterior aspect of the capsule
Sem
imem
bra
nou
s
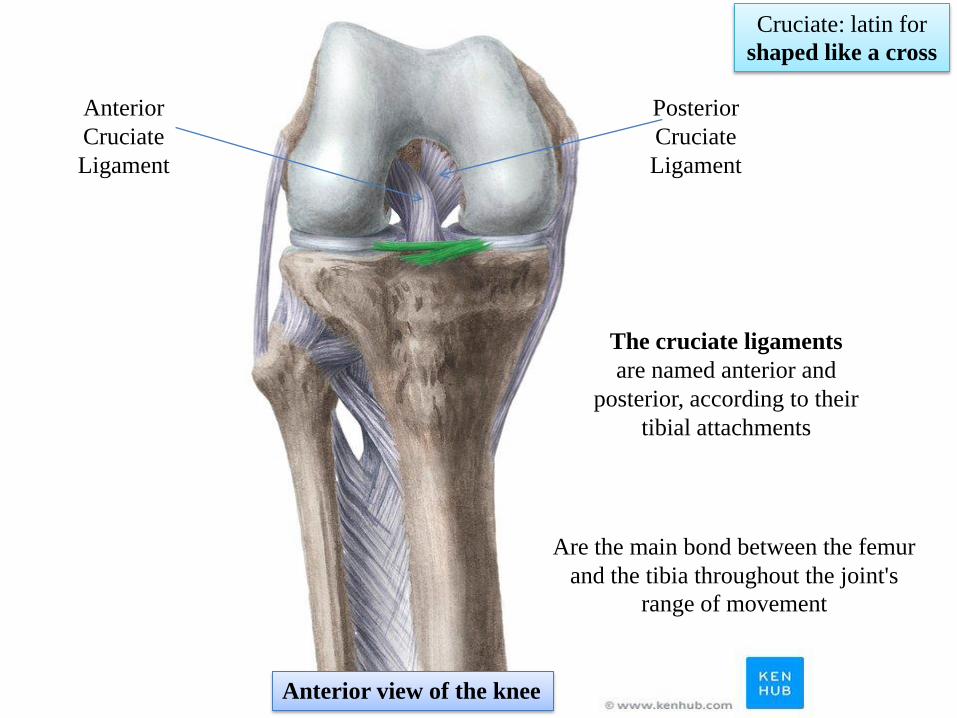
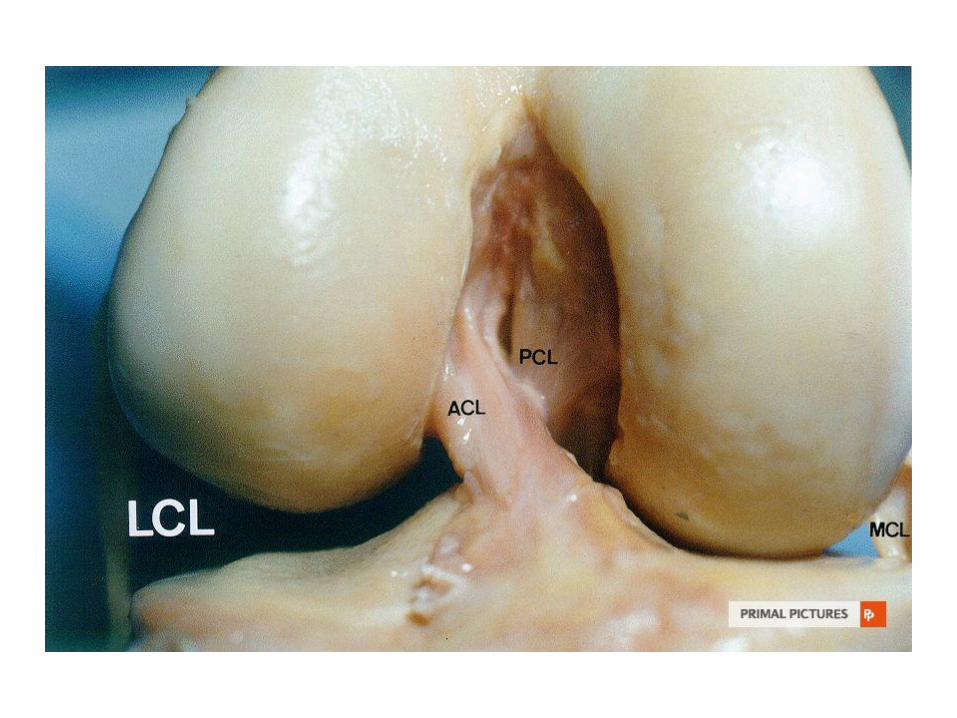
The cruciate ligaments
are named anterior and
posterior, according to their
tibial attachments
Anterior
Cruciate
Ligament
Posterior
Cruciate
Ligament
Cruciate: latin for
shaped like a cross
Are the main bond between the femur
and the tibia throughout the joint's
range of movement
Anterior view of the knee

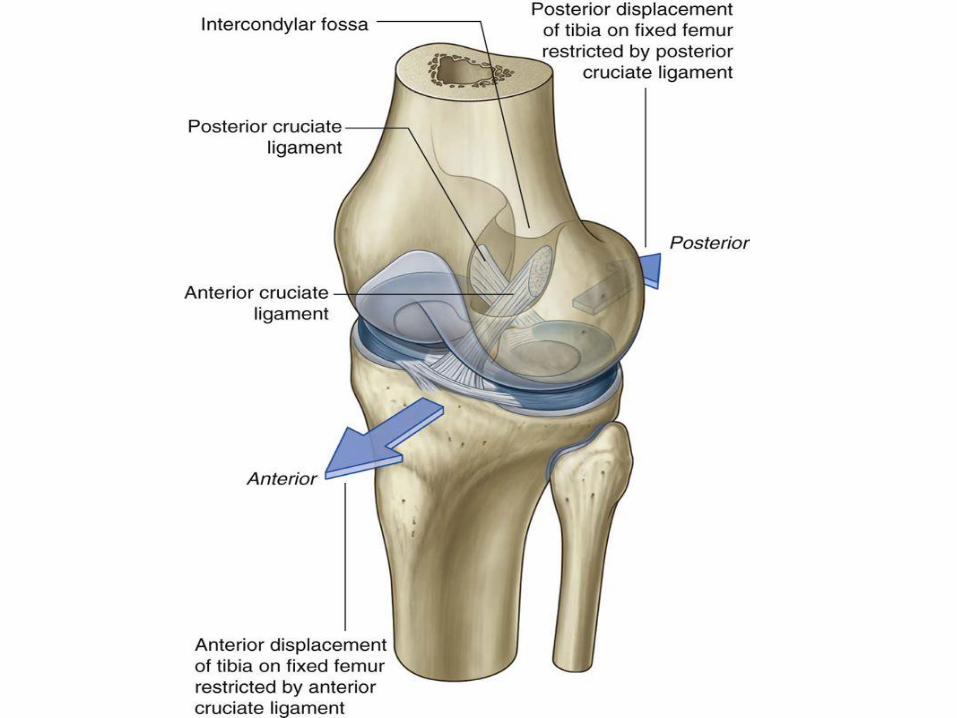
The anterior cruciate ligament is
attached to the anterior intercondylar area
of the tibia and passes upward, backward,
and laterally, to be attached to the posterior
part of the lateral wall of intercondylar
fossa
The anterior cruciate ligament restricts
anterior displacement of the tibia relative
to the femur

The posterior cruciate ligament is
attached to the posterior intercondylar area
of the tibia and passes upward, forward,
and medially to be attached to the anterior
part of the medial wall of intercondylar
fossa
The anterior cruciate ligament restricts
posterior displacement of the tibia relative
to the femur

The tests for the integrity of the cruciate ligaments are
the anterior and posterior drawer signs
Tearing of the posterior cruciate ligament
allows the tibia to be easily pulled
posteriorly
(posterior drawer sign)
Tearing of the anterior cruciate ligament
allows the tibia to be easily pulled
forward
(anterior drawer sign)
Test anterior cruciate ligament
Test posterior cruciate ligament
Ruptured ACL Ruptured PCL

Menisci
Are medial and lateral C-
shaped fibrocartilages
The upper surfaces are in
contact with femoral condyles
The lower surfaces are in
contact with tibial condyles.
Their function is to deepen
the articular surfaces of the
tibial condyles to receive the
convex femoral condyles; they
also serve as cushions between
the two bones
Each meniscus is attached to
the upper surface of the tibia
by anterior and posterior horns

Superior view of the proximal end of Tibia

The medial meniscus is
attached to the capsule of the
knee joint and the medial
collateral ligament, it is
relatively immobile
Medial collateral ligament
Medial meniscus

Note
The lateral condyle of femur
is a bit longer than the medial
Helps in preventing the
lateral dislocation of patella

Synovial Membrane The synovial membrane lines the capsule
For example
On the front and above the joint, it forms a
pouch, which extends up beneath the
quadriceps femoris for three fingerbreadths
above the patella, forming the suprapatellar
bursa. This is held in position by the
attachment of the articularis genu muscle
Note: Suprapatellar bursa communicates with
the joint cavity
The synovial membrane of the knee joint forms
pouches (bursae)
To provide low-friction surfaces for the
movement of tendons associated with the joint
Some bursae communicate with the joint cavity
and some do not normally communicate
Articularis
genu
Note:

Suprapatellar
bursa Consequently, abrasions or
penetrating wounds (e.g stab
wounds) superior to the patella
may result in suprapatellar
bursitis caused by bacteria
entering the bursa from the torn
skin. The infection may spread
to the knee joint

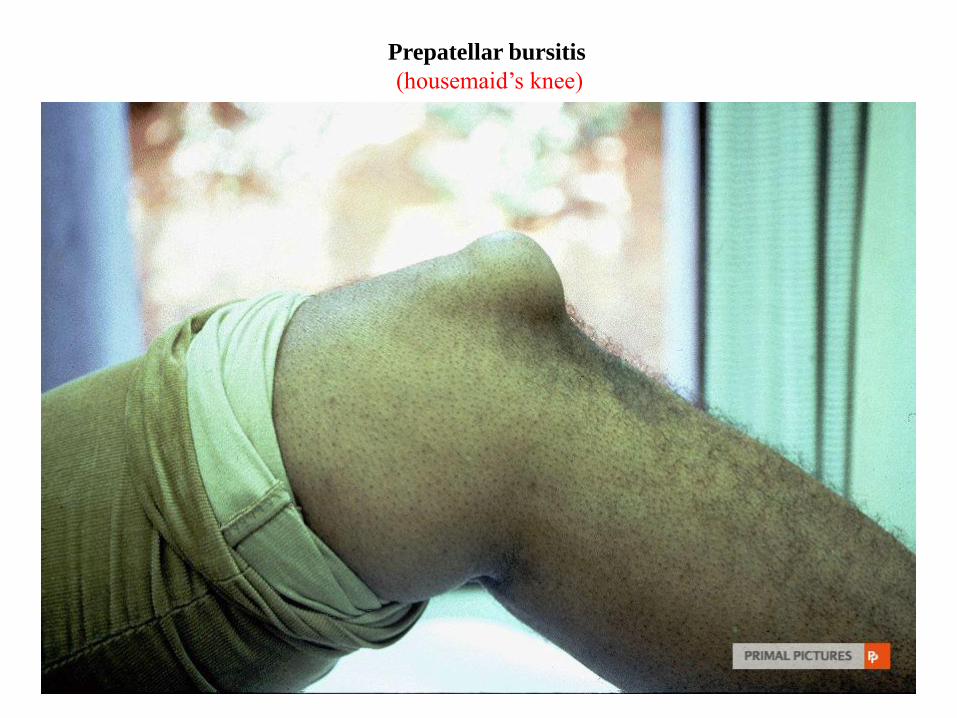
The prepatellar bursa lies in the
subcutaneous tissue between the
skin and the patella
Prepatellar bursitis
(housemaid’s knee)
Is usually a friction bursitis caused
by friction between the skin and
patella
Prepatellar
bursa

Subcutaneous infrapatellar
bursitis results from
excessive friction between the
skin and tibial tuberosity
Subcutaneous
infrapatellar
bursa
The superficial infrapatellar
bursa lies in the subcutaneous
tissue between the skin and the
ligamentum patellae
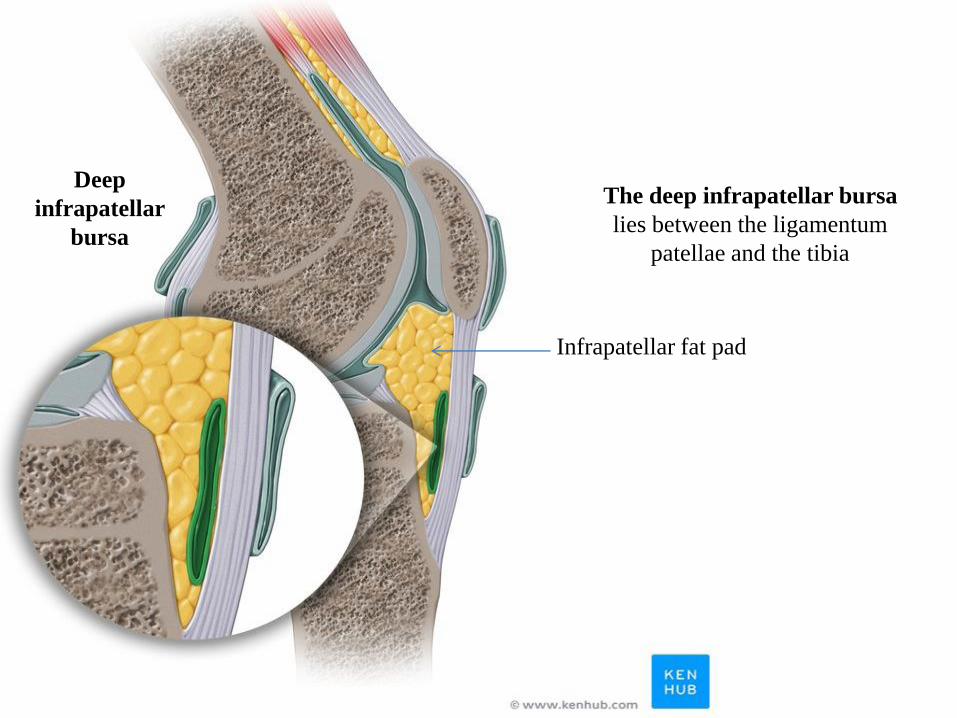
Deep
infrapatellar
bursa
The deep infrapatellar bursa
lies between the ligamentum
patellae and the tibia
Infrapatellar fat pad

Bursae are found wherever skin,
muscle, or tendon rubs against
bone. Four are situated in front of
the joint and the rest are found
behind the joint
The other bursae are found related to the
tendon of insertion of the biceps femoris;
related to the tendons of the sartorius,
gracilis, and semitendinosus muscles as
they pass to their insertion on the tibia;
beneath the lateral head of origin of the
gastrocnemius muscle; and beneath the
medial head of origin of the
gastrocnemius muscle, beneath thhe
iliotibial tract
Subtendinous
bursa of biceps
femoris
Anserinus
bursa
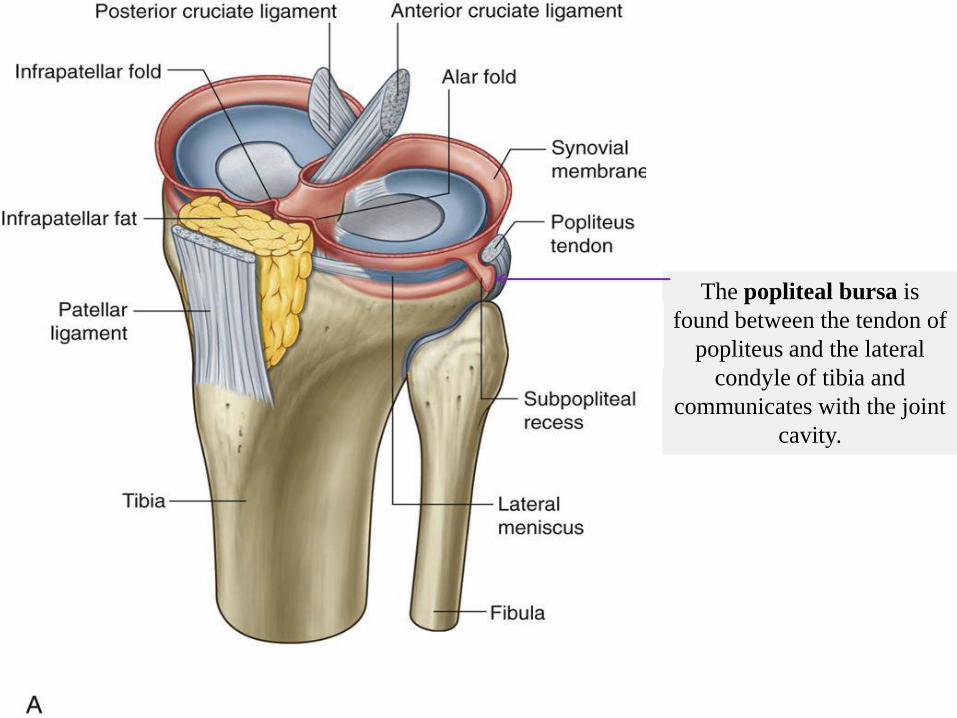
The popliteal bursa is
found between the tendon of
popliteus and the lateral
condyle of tibia and
communicates with the joint
cavity.
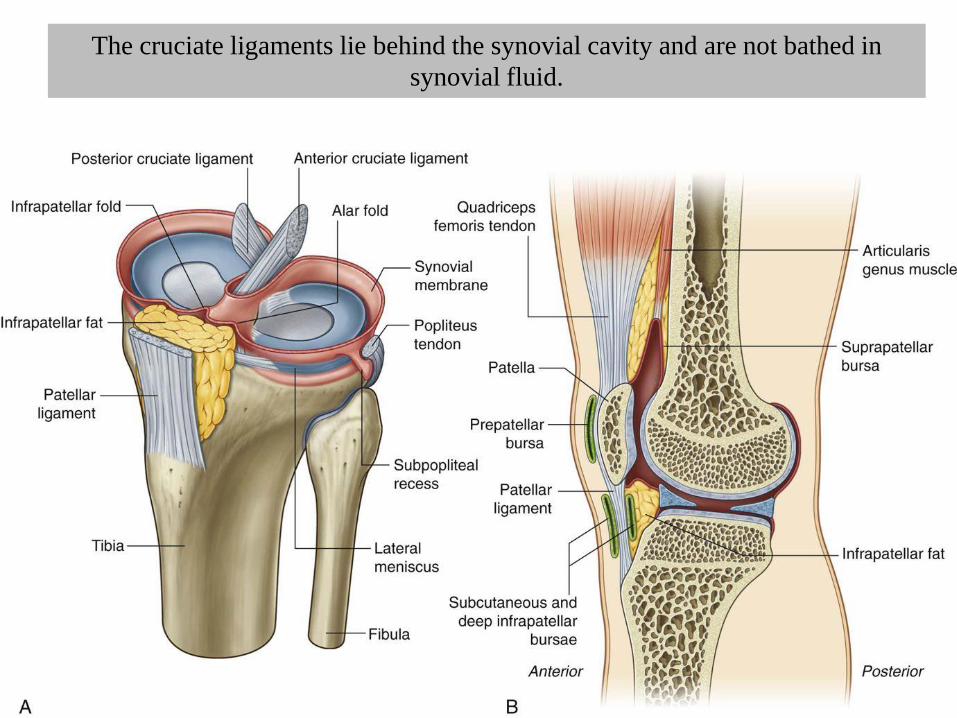
The cruciate ligaments lie behind the synovial cavity and are not bathed in
synovial fluid.

Locking mechanism
When standing the knee joint is locked into
position, thereby reducing the amount of muscle
work needed to maintain the standing position
Locking mechanism has 3 components:
1- The change in the shape and size of the
femoral articular surfaces
2- The medial rotation of the femur on the
tibia during extension
Medial rotation and full extension tightens all
the associated ligaments
3- The body’s center of gravity is positioned
along vertical line that passes anterior to the
knee joint
Keeps the knee extended when standing
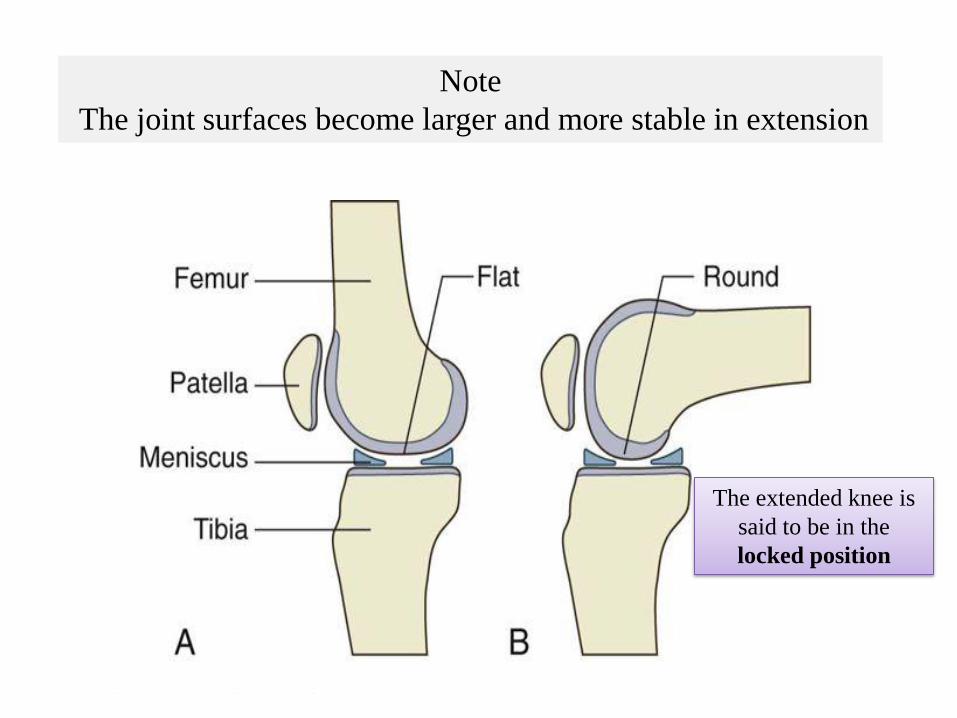
Note
The joint surfaces become larger and more stable in extension
The extended knee is
said to be in the
locked position

The knee joint can not be flexed
unless it is unlocked by the
popletius
Before flexion of the knee can occur, it is
essential that the major ligaments
Be untwisted/ slackened to permit movements
between the joint surfaces
This unlocking or untwisting process is
accomplished by the popliteus muscle
Which laterally rotates the femur on tibia

Popliteus
Origin: lateral surface of
lateral condyle of femur by
a rounded tendon
Insertion: posterior surface
of tibia above soleal line
Nerve supply: Tibial nerve
Action: flexes leg at knee
joint, unlocks the extended
knee at the initiation of
flexion by lateral rotation
of femur on tibia (when
the foot is on the ground)
and slackens ligaments of
knee joint
Medial rotates the tibia on
the femur
Unlocking means Lateral
rotation of the femur
Or Medial rotation of the
tibia
Locking means…………..
rotation of the femur Or
…………rotation of the
tibia

Note
The popliteus arises within
the knee joint
Its tendon separates the lateral meniscus
from the lateral collateral ligament and
the capsule
It emerges through the lower part of the
posterior surface of the capsule to pass to
its insertion

Flexion
Biceps femoris, Semitendinosus, and Semimembranosus muscles,
assisted by Gracilis and Sartorius muscles
Flexion is limited by the contact of the back of the leg with the thigh
Extension
Quadriceps femoris
Extension is limited by the tension of all the major ligaments of the
joint.
Medial Rotation
Sartorius, Gracilis, and Semitendinosus
Lateral Rotation
Biceps femoris
Movements of the knee joint
The stability of the knee joint depends on the tone of the strong
muscles acting on the joint and the strength of the ligaments.
Of these factors, the tone of the muscles is the most important,
and it is the job of the physiotherapist to build up the strength
of these muscles, especially the quadriceps femoris, after injury
to the knee joint.
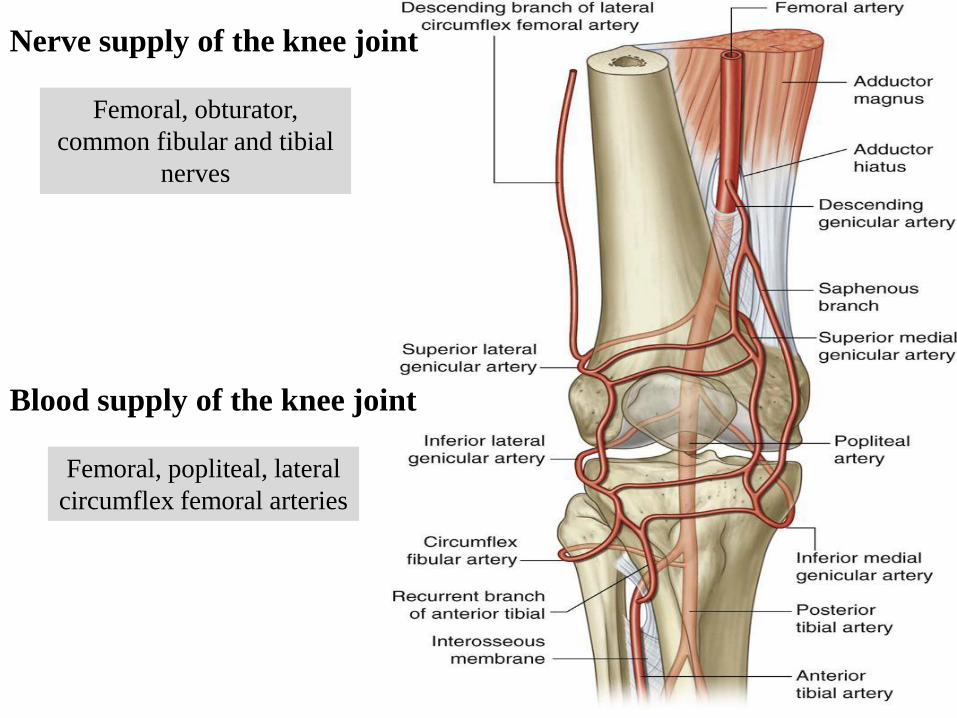
Femoral, obturator,
common fibular and tibial
nerves
Femoral, popliteal, lateral
circumflex femoral arteries
Nerve supply of the knee joint
Blood supply of the knee joint

Tibial collateral
ligament extends from
medial epicondyle of
femur to medial aspect
of tibia
The tibial collateral
ligament prevents lateral
displacement
(abduction) of tibia
under femur
The medial collateral ligament
is firmly attached to the capsule
and medial meniscus
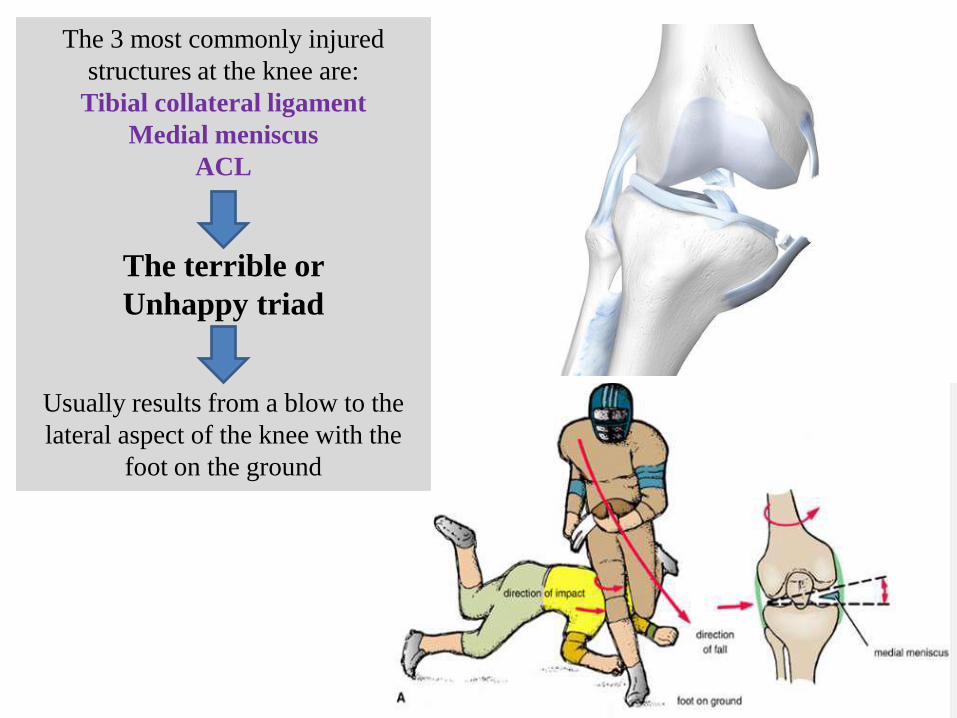
The 3 most commonly injured
structures at the knee are:
Tibial collateral ligament
Medial meniscus
ACL
The terrible or
Unhappy triad
Usually results from a blow to the
lateral aspect of the knee with the
foot on the ground

Knee joint and menisci from above
ACL and PCL attachment points
Prepatellar bursitis
(housemaid’s knee)
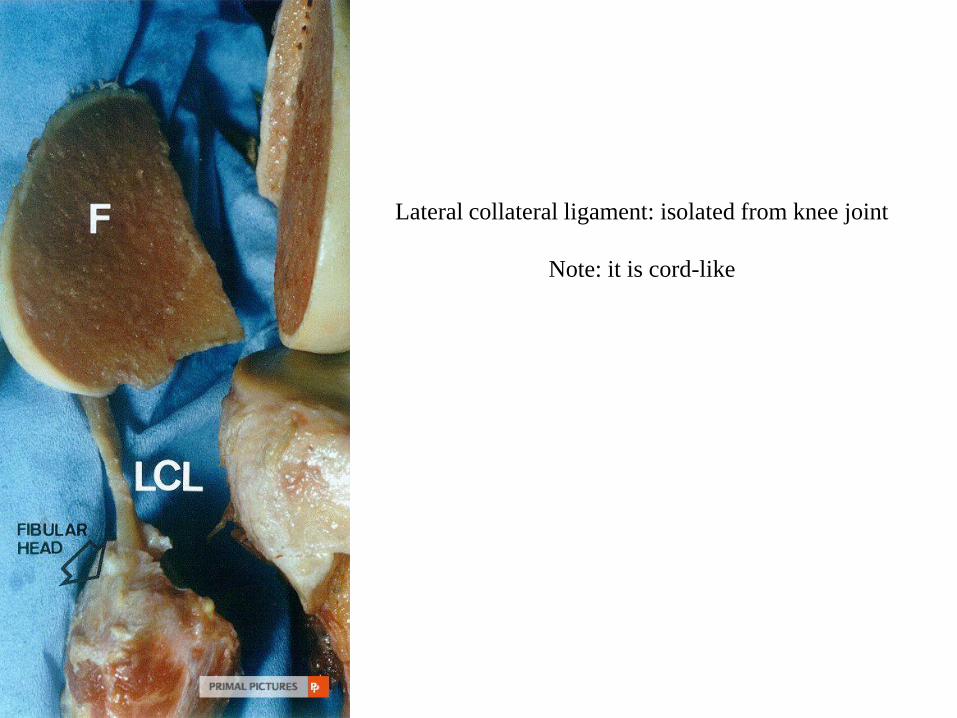
Lateral collateral ligament: isolated from knee joint
Note: it is cord-like

Medial collateral ligament: isolated from knee joint
Note: it is flat

Patellar tendon
rupture:
Sagittal
radiograph

Suprapatellar bursa
Quadriceps tendon
Patellar ligament
Femur
Tibia
Patella
Fibula
Lateral meniscus
MRI of the Knee (Sagittal View)

MRI of the Knee
(Coronal View)
Femur
Tibia
Lateral
meniscus Medial meniscus
ACL
PCL


















