Kitty Chan School of Nursing,The Hong Kong Polytechnic University
102
1 Kitty Chan School of Nursing,The Hong Kong Polytechnic University Email: [email protected] Date: 2005
description
Basic Clinical. Electrocardiography. Kitty Chan School of Nursing,The Hong Kong Polytechnic University Email: [email protected] Date: 2005. Objectives. Upon completion of the session, the students should: - PowerPoint PPT Presentation
Transcript of Kitty Chan School of Nursing,The Hong Kong Polytechnic University

1
Kitty Chan
School of Nursing,The Hong Kong Polytechnic University
Email: [email protected]
Date: 2005

2
Upon completion of the session, the students
should:
have developed a basic understanding of anatomy and
of the physiology of cardiac conduction in relation
to ECG interpretation;
have developed a systematic and pragmatic approach
to ECG interpretation;
appreciate the clinical significance of ECG
interpretation.
Objectives

3
■ Wiegand, L-M D. J. & Carlson, K. K. (Eds.) (2005). American Association of Critical-Care Nurses AACN Procedure Manual for Critical Care. (5th ed.). Philadelphia: W B Saunders.Section 8
■ Huszar, R. J. (2002). Basic Dysrhythmias: Interpretation & Management. (3rd Ed.). St Louis: Mosby.
Indicative Readings

4
The electrocardiogram [ECG] is a helpful in diagnosing cardiac & non-cardiac illnesses. It is also used to monitor the effects of therapeutic treatment. Cardiac monitoring, or telemetry provides a continuous and real-time observation of the client’s cardiac rhythm. A single-strip ECG gives a prompt identification of life-threatening rhythms. In addition, abnormalities that are detected can serve as a basis for 12-Lead ECG or other investigations.12-Lead ECG imparts more information, such as ischaemia and myocardial infarction. The above two aspects will be the main focus of this module.Of course, interpreting axis deviation & hypertrophies or other abnormalities is highly recommended.
Introduction

5
Electrical activities produce current that transmit through the heart conduction system. This is sensed and transformed into ECG waveforms. Depolarization and repolarization occurs in a precise sequence. Normally, mechanical heart contraction follow to generate the cardiac output.However, when disturbances arise, cardiac contraction may not be effective, and there may even be no contractions.Therefore, always match the ECG rhythm with the patients’ clinical manifestation and complains.Before we start interpreting ECG, the anatomy, cardiac cycle and electrophysiology are reviewed
Introduction

6
Five Phases of the Depolarization-Repolarization CyclePHASE Response and Action Potential
0 Rapid Depolarization
A current is conducted from adjacent cells.In response to a stimulus from connecting cells, a sodium channel opens There is a rapid influx of Sodium into the cells Calcium moves slowly into the cells The cell membrane charge moves from -90mv to +20-+30mv
1 Early Repolarization
Sodium channels closeThe cells begin to return to a negative state
2 Plateau The Calcium channels open Slow influx of Calcium Outflow of Potassium Cell membrane potential is around 0mv
3 Rapid Repolarization
The Calcium channels close Rapid outflow of Potassium Cell membrane potential drops rapidly back to it resting membrane potential [RMP]
4 Resting The Sodium pump is reactivated (* It depends on an adequate amount of Magnesium & Phosphate). Normal electrolytes distribution restored: The Cell membrane is impermeable to Sodium Potassium inside the cell & sodium outside the cell The Resting Membrane Potential -90mv

7
Myocardial Transmembrane PotentialsPotential milivolts
0
Resting State
Rapid Depolarization
Early Repolarization
Rapid Repolarization
Absolute Refractory
Period
Absolute Refractory
Period
Restoration of
Balance
+ + + + + + + + + + + + + + + +
Sodium Pump
KK++
Na+
+ + + + + + + + + + + + + + + +
Relative Refractory
Period
Relative Refractory
Period
Cardiaccell
Cellmembrane
Cellmembrane
Outside cell
Outside cell
+ + + + +
- - - - - + + + + + + + + + + + + + +
KK++
Na+Ca++
Na+ K+
- - - - - - - - - - - - - -
- - - - - - - - - - - - - - - -
- - - - - - - - - - -
Mechanical Contractio
n
Action Potentials
Threshold Potentials
- - - - - - - - - - - - - -
+ + + + + + + + + + + + + +Fast
Sodium Influx
Slow Calcium channel open Plateau
Plateau

8
Properties of Cardiac CellsTerm Electrophysiological Properties
Automaticity
Spontaneous Depolarization (Pacemaker Potential):Cardiac cells initiate their own action potential WITHOUT a stimulus from another cellA cell membrane allows Na+ & Ca++ ions to move in & prevents K+ from diffusing out. A NET build-up of positive ions inside the cell enables it to reach a threshold (TP) & depolarizeThe slope of the pacemaker potential (i.e., the time it takes to reach TP) determines the automaticity of the cells
Excitability Ability of a cell to depolarize in response to a stimulus:The more negative the Resting Membrane Potential
The LESS excitable is the cell; The FASTER the conduction velocity
Conductivity
Ability of a cardiac cell to transmit an impulse
Refractoriness
The state of a cardiac cell: Regardless of the intensity of the stimulus (much stronger than normally required) to initiate repolarization

9
Automaticity of Cardiac CellsCardiac
CellsElectrophysiological Properties
SA Node Main Pacemaker:Intrinsic firing at a rate of 60-100 times/minuteImpulse generation is fastest & dominantImpulse transmission follow specific path
AV Node Slow Node:Depolarizes at a rate of 40-60 times/minuteDelays impulses from the SA node by 0.04 secondsGenerates impulses when the impulse generation function of the SA node pulse impairs
His-Purkinje Fibres
The Left & Right Bundle Branch conduct impulses at different speeds to synchronize the depolarization of the Left & Right VentriclesPurkinje fibres are usually not activated unless the pulse transmission is blocked or not generated from higher pacemakersGenerates impulses & serves as a pacemaker at a rate of 20-40 bpm or slowerThe impulse transmission is chaotic

10
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Pacemaker Action Potentials & Automaticity
Automaticity in cardiac muscles:
a gradual in K+ permeability resting potential Transmembranous Potential [TMP] reaches a threshold Spontaneous depolarization occurs
SA node - shortest phase 4 dominates impulse generation
Pacemaker Potential: Pacemaker Potential: Spontaneous Depolarization

11
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Pacemaker Action Potentials & Automaticity
Steeper Slope: Automaticity
Increase
Pacemaker Potential: Pacemaker Potential: Spontaneous Depolarization

12
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Pacemaker Action Potentials & Automaticity
Slope Decreases : Automaticity Decreases
Pacemaker Potential: Pacemaker Potential: Spontaneous Depolarization

13
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Effect of Change in RMP
RMPRMP
TPTPBigger Difference
RMP Decreases (More Negative):
Cells are less excitable Stronger stimulus required for depolarization contractility weakens
This occurs in HYPOKalaemia

14
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Effect of Change in RMP
RMPRMPTPTP
RMP Increases (Less Negative):
Cells are easily excitable Depolarization occurs with a very weak stimulus contractility slow & ineffective
This occurs in HYPERKalaemia
Closer to TP

15
Time (Second) 0 1.
60.8
2.4
+ + 10mV10mV
--90mV90mV
Membrane Potential
Threshold Threshold PotentialPotential
Action Action PotentialPotential
Resting Resting Membrane Membrane PotentialPotential
-60mV-60mV
Effect of Change in TP
TP Decreases:
Closer to RMP, the cells are more excitable Depolarization occurs with a very weak stimulus contractility slow & ineffective
This occurs in HYPOCalaemia
HYPERCALCAEMIA is a Positive Inotrope since it sustains & strengthens cardiac contractions
TPTP
Closer to RMP
RMPRMP

16
Electrical Conduction System
Sinoatrial (SA) Node
Atrioventricular (AV) Node
Bundle of His
Left Bundle Branch
Left posterior fascicle
Left anterior fascicle
AV Junction
Purkinje fibresRight Bundle Branch
Interatrial conduction tract(Bachmann Bundle)
Internodal atrial conduction tract

17
Wave Deflection & Current Direction
Current Direction-ve
+ve
Electrical Waveform
Deflection
Toward the Lead
UPRIGHTUPRIGHT
Away from the Lead
DOWNWADOWNWARDRD
Perpendicular to the Lead
BIPHASICBIPHASIC

18
11
4433
22 RR
Cardiac Depolarization & Electrical Current
11. Atrial Depolarization
2. Septal vector
3. Apical vector & both ventricles
4. Remainder of the left ventricle
RR. Resultant Cardiac Vector. Resultant Cardiac Vector
A positive deflection (upstroke) Λ is recorded as depolarization proceeds towards the particular electrode & vice versa.

19
Limb Leads: Frontal Plane of the HeartStandard Bipolar Leads
Inferior
Lead ILead I+
+
Lead IILead II
Lead IIILead III
+
Einthoven’s Equilateral Triangle

20
Limb Leads: Frontal Plane of the HeartThe Augmented Unipolar Leads
Lead Lead aVLaVL
Lead Lead aVFaVF
Lead Lead aVRaVRLead Lead aVRaVR
xNull Null ReferencReference Pointe Point
Null Reference Point: the negative reference for leads aVR, aVL, aVF & the precordial leads V1 - V6
(calculated from the right & left arm and right & left leg electrodes)

21
Hexaxial Reference Circle
aVR -1500
+300
aVL-300
+1500
I 00
+1800
II +600
-1200
aVF +900
-900
III +1200
-600
LADLAD
RADRAD
NORMALNORMAL
IndeterminatIndeterminatee
For determining frontal plane axis deviation

22
12-Lead Electrode Placement
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implications for patient care. Philadelphia: Saunders.
i.e., Electrode Placement at V6 equivalent of MCL6
✼Precordial Leads are useful in detecting ST
Changes & Aberrant Ventricular Conductions
Septal Septal LeadsLeads
Anterior Anterior LeadsLeads
Lateral Lateral LeadsLeads
V1 to V6: Corresponding sites for monitoring of MCL1 to MCL6
V2V2V1V1V6V6
V4V4V5V5V3V3
Mid-Clavicular Mid-Clavicular LineLine
Anterior Axillary LineAnterior Axillary Line
Mid-Axillary LineMid-Axillary Line

23
Right-sided Chest Electrode Placement
V2V2RR
V3V3RR
V5V5RRV6V6RR
V4V4RR
Mid-Clavicular LineMid-Clavicular Line
Anterior Axillary LineAnterior Axillary Line
Mid-Axillary LineMid-Axillary Line

24
Posterior Chest Electrode Placement
Mid-Axillary Mid-Axillary LineLine
Posterior Axillary LinePosterior Axillary LineLeft Paraspinal LineLeft Paraspinal Line
V9V9V7V7V6V6 V8V8
Wiegand & Calrson, 2004, p. 426

25
Cardiac Monitoring & Lead Placement
3-Lead-Wire system:
limited to leads I, II, III &
modified chest leads (MCL1-6)
For single-lead ECG monitoring, unless a specific part of the heart is under scrutiny, Lead II is usually chosen since both the positive & negative vectors are travelling in the same direction of cardiac impulse conduction, producing upright P & QRS complexes.

26
Cardiac Monitoring & Lead Placement
5-Lead-Wire system:
4 standardized electrodes corresponding to limbs leads I, II, III, aVR, aVL & aVF
placement of 5th chest leads provides 7 precordial lead options
V1-V6 (1 at a time)

27*Sweep speed of ECG & paper dispense @ 25mm per second
1 1 Large Large
SquareSquare
5mm across = 0.2
second
1mm across
= 0.04 second
1mm tall = 0.1mV of amplitude
1 1 Small Small
SquarSquar
ee
55 Large Large Squares Squares
= = 11 SecondSecond

28
Normal ECG/EKG Waveform
PPTT
UU
RR
QQSS
ST ST SegmentSegment
PR PR IntervalInterval
QT QT IntervalInterval
Lead II
P
PR Interval
Q
R
S
TU
ST Segment
QT Interval

29
Normal ECG Waveforms & ConfigurationsWavefor
mConfiguration & Duration (second) Leads
Amplitude Duration
P Rounded & SymmetricalAmplitude 0.5-2.5cm
0.06-0.10
I, II, aVF, V4-V6
PR Interval
0.12-0.20
QRS Q: Small & Non-significant 0.06-0.12
I, II, III, aVL, V4-V6
R: progressively higher in amplitude –
limb leads > 5mmchest leads > 10mm
V2-V5, gradually diminish in V5-V6
ST Curves gently into the proximal limb of the T waveIsoelectric in ALL Leads
Elevation < 1mm & Depression < 0.5mm
J Point Junction of QRS complex & the ST segment
T wave Rounded & Symmetrical, amplitude:limb leads< 5mm & chest leads < 10mm
Positive in I, II, V3-V6
Inverted in aVR
QT (<½ preceding RR)
U wave Delayed depolarization of the purkinje system

30
P
PR INTERVAL
P wave: Atrial Depolarization
P:P:
•rounded & symmetrical
• 0.06- 0.10 sec
•amplitude: 0.5-2.5mm
•positive in Lead I, II, aVF & V4-V6
PR Interval:PR Interval:
•0.12-0.20 sec
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implications for patient care. Philadelphia: Saunders.

31
QRS: Ventricle Depolarization
P
QRS
QRS: QRS:
•Q waves is small &
nonsignificant in leads I, II, III,
aVL, V4-V6
•R wave progressively higher
in amplitude from V2-V4/V5
gradually diminish to V6
•0.06- 0.12 sec
•amplitude: >5mm in limb
leads; >10mm in Chest leadsPaul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implication for patient care. Philadelphia: Saunders

32
P
QRS
ST:ST:
•Curves gently into the proximal limb of the T wave
•Isoelectric in ALL Leads
•elevation <1mm
•depression <0.5mm
J Point:J Point:
•The junction of QRS complex & the J point of the ST segment
•deviates from the isoelectric line if an ST elevation/
depression exist
ST SEGMENT
ST Segment: Isoelectric Line
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implications for patient care. Philadelphia: Saunders.
J Point

33
T: T: •slightly rounded & symmetrical
•positive in leads I, II, V3-V6
•inverted in aVR
•amplitude <5mm in limb leads & <10mm in chest leads
QT: QT: ventricular refractory period
•0.30-0.44sec
•*0.12-0.20 sec (<½ preceding RR)
U wave:U wave: delayed repolarization of the purkinje
system
T
QRS
P
QT
T wave: Ventricular Repolarization
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implications for patient care. Philadelphia: Saunders.

34
Sinus Rhythm
Rhythm Atrial Rate
Ventricular Rate
P wave PR Interval
QRS P:QRS Ratio
Normal Sinus Rhythm
regular 60-100 Before every QRS (Normal Configuraton)
Normal 1:1
Sinus Tachycardia
regular >100 usu. < 160
Before every QRS (Normal Configuraton)
Normal 1:1
Sinus Bradycardia
regular < 60
Before every QRS (Normal Configuraton)
Normal 1:1
Sinus Dysrhythmia
irregular 60-100 ✼ inspiration expiration
Before every QRS (Normal Configuraton)
Normal 1:1
Sinus Rhythm

35
Normal Sinus Rhythm [NSR]
P P P PPP P P
66 SecondsSeconds
Total in 6 seconds
Characteristics
P Waves: 7 Upright & amplitude 1mm
PR Interval 0.12 second
Each P is followed by a QRS
QRS Complex 7 (HR=70bp
m)
Normal (0.12 second)
RR Interval Regular

36
Sinus Bradycardia
P PPP P6 6 SecondsSeconds
QRS QRS ComplexComplex
Total in 6 seconds
Characteristics
P Waves: 5 Upright & amplitude 1mm
PR Interval 0.12 second
Each P is followed by a QRS
QRS Complex 5 (HR=50bp
m)
Normal (0.12 second)
RR Interval Regular

37
Sinus DysrhythmiasSinus
DysrhythmiasCharacteristics
Sinus Pause dropped P wave & SR resumed subsequently
Sinus Arrest /Sinoatrial Exit Block
SA node fails to initiate an impulse for 3 seconds
Sick Sinus Syndrome (SSS):
Paroxysmal or alternating sinus bradycardia & atrial tachycardia (brady-tachy syndrome)Failure to HR to meet body demand

38
Atrial Dysrhythmias
Rhythm Atrial Rate
Ventricular Rate
P wave PR Interval QRS P:QRS Ratio
Premature Atrial Complexes (PACs)
Irregular Depends on underlying rhythm
Early Morphology varies
Varies Normal 1:1
Wandering Atrial Pacemaker
Irregular 60-100 Before every QRS
Some variations
Normal 1:1
Atrial Flutter Regular/ irregular
240-340 Depends on AV conduction
Saw-toothed flutter wave
Not measurable
Normal P QRS
Atrial Fibrillation
Irregular 350 varies Coarse or fine fibrillatory waves
Not measurable
Normal P QRS

39
Atrial Flutter
66 SecondsSeconds
Total in 6 seconds
Characteristics
P Waves: Varies Saw-Tooth
QRS Complex 9 (HR=90bp
m)
Normal
RR Interval IRREGULAR
Identical undulating SAW-TOOTH FLUTTER WAVES
F F F F F F F F F F QRS QRS ComplexComplex
QRS QRS ComplexComplex

40
Atrial Fibrillation [Fine AF]
Total in 6 seconds
Characteristics
P Waves: Varies FIINE Fibrillatory Waves
QRS Complex HR 50-60 bpm
Normal
RR Interval IRREGULAR6 6 SecondsSeconds

41
Atrial Fibrillation [Coarse AF]
Total in 6 seconds
Characteristics
P Waves: Varies Coarse Fibrillatory Waves
QRS Complex
HR 80bpm
Normal
RR Interval IRREGULAR6 6 SecondsSeconds

42
Atrial Dysrhythmias
P’ P’ P’ P’ P’
MAT (multifocal atrial tachycardia)•Various P morphologies originate from multiple atrial ectopic foci
*(3 or more pacemaker sites)
•Rate = 160-240bpm

43
Juntional Rhythm
6 6 SecondsSeconds
Total in 6 seconds
Characteristics
P Waves: 0
QRS Complex 6(HR=60bp
m)
Normal
RR Interval 0.98 second
REGULAR
QRS QRS ComplexComplex

44
Junctional Dysrhythmias1o pacing from the AV node
Rhythm Atrial Rate Ventricular Rate
P waves QRS PR Interval P:QRS Ratio
AV Junctional Rhythm
Regular Indeterminate 40-60 Inverted Before /After/Being Buried in QRS
Normal 0.2 sec if P precedes QRS
P QRS
Junctional Tachycardia
Regular Indeterminate 100-250 Inverted Before /After/ Being Buried in QRS
Normal Indeterminate P QRS
Paroxysmal Supraventricular Tachycardia (PSVT)
Regular Present or absent
160-240 *begins abruptly & last from a few seconds to many hours
Inverted Before /After/ Being Buried in QRS
Usually normal
0.2 sec if P precedes QRS
P QRS

45
Non-uniform recovery from refractory period leading to re-entry circuit:
1. Slow conduction of impulses at a refractory zone
→ Unidirectional Block→ Detouring of Impulse
2. Activation & transmission of impulse via accessory pathway
3. Subsequent activation of impulse through the previously refractory zone (now recovered)
4. The reentry & activation of new impulses occur in a circuitry manner
Re-Entry Phenomenon [1]

46
Unidirectional Block & Delayed Conduction within the circuit
→Original impulse emerges & reenters the adjacent tissue (just recovered)
→ Recycles within the circuit
Unidirectional Block & Delayed Conduction within the circuit
→Original impulse emerges & reenters the adjacent tissue (just recovered)
→ Recycles within the circuit
Normal Impulse NOT yet fired from SAN ∴ AV Node NOT Reactivated
Normal Impulse NOT yet fired from SAN ∴ AV Node NOT Reactivated
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implications for patient care. Philadelphia: Saunders.
Re-Entry Phenomenon [2]

47
AVNRT (AV Node Re-entry Tachycardia)Micro-Circuits: At cellular level within the AV node with unidirectional block & the Purkinje fibers
Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implication for patient care. Philadelphia: Saunders
Ventricular Pre-excitation

48Paul S & Hebra J D 1998 The Nurse’s Guide to Cardiac Rhythm Interpretation: Implication for patient care. Philadelphia: Saunders
AVRT (AV Re-entry Tachycardia)-
Macro-Circuits: Antegrade travel through the AV node & retrograde across an accessory pathway
Classic Ventricular Pre-excitation
Wolf-Parkinson-White Syndrome:pre-excitation via a Bundle of Kent without delay at the AV node
Depolarization occurs with AV impulse after normal delay
delta wave(slurred upstroke)

49
PSVT (Paroxysmal Supraventricular Tachycardia)
*It is useful to capture the beginning of the PSVT to
identify the re-entry loop, especially when aberrant
conduction occurs & a wide bizarre QRS exists

50
Atrioventricular Blocks(Heart Block)
Rhythm Atrial Rate Ventricular Rate
P Wave PR Interval QRS P:QRS Ratio
1o Heart Block regular 60-100 Precedes each QRS
Prolonged ( 0.2s)
Normal 1:1
2o Heart Block (Wenkebach, Mobitz Type I)
irregular ventricular rate
sinus rate Precedes each QRS EXCEPT a non-conducted P (regular)
Cycles of Progressive lengthening until non-conduction
Normal 1:1
2o Heart Block (Mobitz Type II)
irregular ventricular rate
Depends on degree of block
Periodic non-conducted P wave (dropped beat)
Normal or constantly prolonged
Normal P QRS
3o Complete Heart Block
regular ventricular rate
60 Regular No relationship
٪ P & QRS
Normal or 0.12 sec
P QRS

51
PR Interval: Constant
RR Interval: Constant
P:QRS Relationship -1:1
Heart Block
1o HB11oo
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
P P P P

52
Heart Block
Type I 2o HB (Wenkebach)
22oo
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
PR Interval: Progressive lengthening
P P P P P
Non-conduction
Absence of QRS complex after P

53
Heart Block
22oo
Advanced AV Block
3:1 Block
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
PR Interval: Constant
Type II 2o HB sudden drop beat
PR Interval: Constant RR Interval: Constant Regular drop beat(s)

54
NO Relationship between P & QRS complex
Heart Block
33oo
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
3 o HB
P-P Interval Constant
P-P Interval Constant
R-R Interval Constant
R-R Interval Constant

55
Third Degree Heart Block & A-V Dissociation
Sinus Dysrhythmias, AV Conduction distrubances or Junctional/Ventricular Tachycardai may result in complete Atrioventricular (AV) Dissociation
Differentiate 3o HB & AV Dissociation:
3o HB Atrial Rate > Ventricular Rate
AV Dissociation Atrial Rate ≈ Ventricular Rate (slightly faster)
RARELY the Primary Problem

56
Right Bundle Branch Block
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
rSR’ pattern Wide S wave
✼ RBBB: QRS 0.12 secT wave Inversion in V1 is common
rR’
Late abnormal electrical vector leading to depolarization of right ventricle > (R’)
RBBB

57
Left Bundle Branch Block
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
LBBB
Impulse activates across the septum from Right to LeftDelayed & prolonged electrical vector toward the eft ventricle → notched R wave
✼LBBB: QRS 0.12 secElevated ST is common in V1-V4
V1
QS WAVE: Wide negative QRS
V6
Large notched R wave
T wave inversion

58
Hemi-/ Fascicular Blocks
Left Anterior Fasicular Block (LAFB)
Left Anterior Fasicular Block (LAFB)
Left Posterior Fasicular Block (LPFB)Left Posterior Fasicular Block (LPFB)
Block Characteristics LAFB Left axis deviation
Prolonged QRS
Q1S3 syndrome
(Q in Lead I; Deep S in Lead III) LPFB Right axis deviation
Prolonged QRS
S1Q3 syndrome
(S in Lead I; Q in Lead III)

59
Ventricular Dysrhythmias
Rhythm Atrial Rate Ventricular Rate
P wave
PR Interval
QRS P:QRS Ratio
Premature Ventricular Complexes (PACs)
irregular indeterminate Depends on the underlying rhythm
unidentifiable Bizzare ( 0.12s) 1:1
Ventricular Tachycardia
Slightly irregular
indeterminate 150-250 unidentifiable Bizzare ( 0.12s) QRS
Ventricular Fibrillation
Irregular indeterminate rapid unidentifiable Fibrillatory waves
none
Idioventricular Rhythm
Regular or irregular
none 40 None or retrograde
Bizzare ( 0.12s) none
Accelerated Idioventricular Rhythm
Usually regular
none 40 - 100 None or retrograde
Bizzare ( 0.12s) none
Ectopic foci

60
Premature Ventricular Contractions
(PVCs)
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby
Group Beats Couplet Ventricular Tachycardia
R-on-T
Bigeminy
Trigeminy

61
Ventricular Dysrhythmias
Ventricular tachycardia (monomorphic)
Torsades de pointes
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby

62
Ventricular Dysrhythmias
Coarse V F
Fine V F
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby

63
Ventricular Dysrhythmias
1. EMD (electromechanical dissociation):*apparently normal ECG but no cardiac output/pulse generated
2. PEA (pulseless electrical activity)
3. Asystole
PEA
Asystole

64
Atrial & Ventricular Hypertrophies
P wave characteristics Associated Conditions Right Atrial Enlargement
Leads II, III aVF: P pumonale Tall Peaked P 2.5mm Lead V1: Biphasic P
COPD Tricuspid valve disease Pulmonary valve disease Pulmonary hypertension
Left Atrial Enlargement
Leads I, II & V4-V6: P Mitrale Leads V1 & V2: Diphasic P 1mm
Left ventricular failure Mitral valve disease Aortic valve disease Systemic hypertension
Right Ventricular Hypertrophy
Lead V1: Tall R wave ( S wave) Inverted T
Lead V6: Deep S wave Right axis deviation
COPD Mitral valve disease Pulmonary stenosis Ventricular septal defect Pulmonary hypertension
Left Ventricular Hypertrophy
Lead I – R wave + Lead III- S wave 25mm Precordial Leads:
V1 – S wave + V5 or V6 - R wave 35mm ST depression
Left axis deviation
SVR Aortic stenosis or insufficiency Mitral insufficiency

65
P Pulmonale in Leads II, III & aVF :Direction: Upright Amplitude: ≥ 2.5mm
4mm
Right Atrial Hypertrophies

66
Left Atrial Hypertrophies
P-Mitrale in Lead I, II, V4-6
Biphasic P: duration > 0.10 second

67
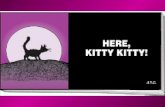
Left Ventricular Hypertrophies
S wave in Lead V1 : 12mmR wave in Leads V5 & 6: 45 & 39mm, respectivelyS [V1] + R [V5] = 41mm (Fit criteria ≥ 35mm)
R wave in Lead I : 20mmS wave in Lead III: 20mm R [I] OR S [III] = 20mm (Fit criteria ≥ 20mm) R [I] + S [III] = 40mm (Fit criteria ≥ 25mm)

68
Normal 12-Lead Electrocardiogram
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby

69Totora G J & Grabowski S R 2003 Principles of Anatomy and Physiology. 10th ed. New York: John Wiley & Sons.
Acute Coronary Syndrome & Coronary Circulation
Coronary atherosclerosis poses the
potential risk of plague rupture,
mircroemboli & occlusive thrombus
A spectrum of clinical syndromes will develop due to coronary artery occlusion:
1. Unstable angina
2. Non-Q MI
3. Q wave MI
4. Sudden cardiac arrest

70
Anterior View of Coronary
Arteries
Right
Atrium
Left
Atrium
Arch of Aorta
Ascending Aorta
Pulmonary
Trunk
Right Coronary Artery [RCA]
Left Coronary Artery [LCA]
Circumflex Coronary
Artery [Cx]
Right Ventricle
Left
VentricleAcute Marginal
Artery
Left Anterior Descending
Coronary Artery[LAD]
Posterior Descending Artery [RD]

71
Myocardial Injury: Ischaemia and
Infarction
V5
Acute Transmural Ischaemia
V5
Acute Subendocardial Ischaemia

72
Ischaemic Zone
Injury Zone
Infarction Zone
Infarction significant Q/QS wave*absence of depolarization current from dead myocardial tissue facing lead recorded opposing electrical vector “through” infarcted area
Injury elevated ST
Ischaemia T wave inversion
* Reciprocal Effect on Opposite Leads
Recovery ST & T wave return to normal
Myocardial Injury:Ischaemia and Infarction
Lead I

73Anterior View of Coronary Arteries
InferiorInferior
II, III, aVFII, III, aVF
LateralLateral
I, aVLI, aVL
LateralLateral
V5 & V6V5 & V6
AnteriorAnterior
V3 & V4V3 & V4
SeptalSeptal
V1 & V2V1 & V2
Coronary Circulation & Ischemic Changes

74
Myocardial Infarction & 12-Lead ECGType of Infarction
Coronary Arteries Involved Leads Involved
Possible ECG Changes
Extensive: LCA LAD
I, V1-V4 Anterior
Localized: LAD diagonal branches
V3 & V4
ST elevation T wave inversion Significant Q waves Progressive loss of R wave
Lateral Left Circumflex Marginal branch of left circumflex Diagonal branch of LAD
I, aVL or V5 & V6
ST elevation T wave inversion Significant Q waves Right axis deviation
Inferior RCA II, III & aVF ST elevation T wave inversion Significant Q waves Left axis deviation
Septal LAD (septal perforator branch)
V1 & V2 ST elevation T wave inversion Significant Q waves loss of R wave in V1 Left axis deviation
Posterior Posterior RCA Distal Circumflex
V1 & V2 reciprocal changes in V1-2: R S ST depression Elevated T

75
Anteroseptal Myocardiac Infarction
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
QS waves: V1 & V4*(r waves absent)
ST segment elevation: V1-V4
EARLY ECG CHANGES: 0 - 2 hours

76
Anteroseptal Myocardiac Infarction
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby.
2- 24 hours:•Maximal ST elevation•minimal Q wave formation
24- 72 hours:•QS wave in V1-V4•ST returned to Baseline•T waves inversion
LATE ECG CHANGES

77
ST Changes
Huszar R J 2002 Pocket Guide to Basic Dysrhythmias: Interpretation & Management. 3rd ed. St Louis: Mosby
ST Elevation
Normal ST
Associated conditions:•Myocardial injury or infarction•pericarditis•ventricular fibrosis, aneurysm•ventricular hypertrophy•digitalis effect
ST Depression
Flat Downsloping Upsloping

78
ECG Changes in Hypokalemia
Gradual ST depression
Flattened T wave
Tall U wave
Serum <K+ 3mEq/L
Serum <K+ 2.7mEq/L
Prolonged PR
U wave size increases
Serum <K+ 2.0mEq/L
Widened & Bizarre QRS complex
Marked ST depression
Inverted T

79
ECG Changes in Hyperkalemia
Serum K+ > 5.5 mEq/L
Peaked, narrow, 60-100bpm
Serum K+ progressive 6.5 8.0mEq/L
Loss of P wave & Bizarre QRS
Atrioventricular block, sinus arrest, VF , asystole
Serum K+ progressive 6.5 8.0mEq/L
Loss of P wave & Bizarre QRS
Atrioventricular block, sinus arrest, VF , asystole

80
ECG Changes: Hypocalcemia/Hypercalcemia
Serum Ca++ > 10.5mg/dL
Shortened ST
Shortened QT
Serum Ca++ < 8.5mg/dL
Lengthened ST
Lengthened QT
May cause Torsades de pointes

81
ECG Changes: Hypomagnesemia/ Hypermagnesemia
Serum Mg++ > 2.5mEq/L
Prolonged PR
Lengthened QT
QRS > 0.12sec
Serum Mg++ < 1.5mEq/L
Lengthened QT
Broad & flattened T
often co-exist with hypokalemia

82
Systematic ECG Interpretation
1: Determine Dysrhythmia Calculate HR
Determine the ventricular rhythm
Measure the RR regularity - variance < 0.12 second (use a caliper or the paper-&-pencil method)
Identify & examine the P waves morphology
Measure the PR interval
Measure & Examine QRS complex morphology
Examine P:QRS correlation
Look for escape or dropped beats
Look for miscellaneous abnormalities
2: Identify Atrioventricular Block & Aberrant Conduction
3: Identify Axis Deviation & Hypertrophies
4: Determine MI - 12-Lead ECG overview

83
Heart Rate Calculation
1. Six Second Count Method: Number of R-R intervals in a 6sec strip x 10 = HR bpm
2. R-R Interval Method: HR bpm = 300 Number of Large Squares
between the peaks of 2 consecutive R waves
6 second Interval
RR Interval

84
Heart Rate Calculation
3. Conversion table: Number of Small Squares between the peaks of 2 consecutive R waves
4. Heart Rate Calculator Ruler Method:
HEART RATE CALCULATORHEART RATE CALCULATOR
* 3rd Complex from Arrow = bpm

85
P wave•Indeterminat
e
VENTRICULAR DYSRHYTHMIAS
ALGORITHM•P-R normal
SINUS RHYTHM
ALGORITHM
•P-R > 0.2 s
HEART BLOCK
ALGORITHM
•Identifiable
•Normal•P’ present or absent
•QRS normal
•Polymorphic
•Irregular R-R
•Irregular P-R
•160-240 bpm
MULTIFOCAL ATRIAL
TACHYCARDIA
•Fibrillatory baseline
•Irregular R-R
•Flutter waves
•Regular or irregular R-R
ATRIAL FIBRILLATION
ATRIAL FLUTTER
SUPRAVENTRICULAR TACHYCARDIA
•P:QRS = 1:1
•Regular R-R
•Regular P-R
HR40-60
HR>100
HR60-100
HR160-240
ACCELERATED JUNCTINAL
RHYTHM
JUNCTIONAL
RHYTHM
JUNCTINAL THCHYCARDIA
Basic Dysrhythmias Interpretation Algorithms

86
Sinus Dysrhythmias & Heart Blocks Algorithms
P-R interval normal 0.12-0.20sec.
•P:QRS = 1:1
•Regular atrial rhythm
•Regular R-R
HR<60
Sinus Bradycardia
HR100-160
Sinus Tachycardia
HR60-100
Regular Sinus Rhythm
Irregular atrial rhythm
Irregular R-R
Sinus Arrhythmia
•Regular R-R
•P:QRS = 1:1
Progressive PRRegular non-conducted QRS
2o Heart Block
Wenkebach
Morbitz Type I
Constant prolonged PRHR 60-100
1o Heart Block
•Irregular R-R
P > QRS
Constant PRSudden dropped QRS
2o Heart Block
Morbitz Type II
No relationship ./. P & QRS
3o Complete
Heart Block
P-R interval > 0.20sec.
P WAVE NORMAL

87
Ventricular Dysrhythmias Algorithms
•Unidentifiable QRS
•Coarse & or fine fibrillatory waves
Ventricular
Fibrillation
•Narrow-complex QRS ( 0.12 sec)
•HR 160-240 bpm
PSVT
•Wide-complex QRS (>0.12 sec)
•HR = 40-100
Accelerated
Idioventricular
Rhythm
•HR< 40
Idioventricular
Rhythm
•HR: 150-250
Monomorphic
SVT &
Aberrant
Conduction
Polymorphic
Torsade de
Pointes
Ventricular
Tachycardia
P WAVE Indeterminate

88
QRS Axis Determination: Frontal Plane
There are a few methods for determining the
Frontal Plane Axis and identifying any Axis
Deviation. Each has its advantages.
The Quadrant method for locates deviation
quickly & easily, while the Degree Method
gives exact measurements.
Choose the one that is most suitable for you &
practice reading 12-Lead ECG using the same
method.
Once you are familiar with a method, you
might try another one.

89
QRS Axis Determination: Frontal Plane
Quadrant Method:Use Leads I & aVFLocate the Main Deflection of the QRS complex
Axis QRS complex
Lead I Lead aVF
Normal Upright in Both Leads
Left Axis Deviation
UprightPoints
Downward
Right Axis Deviation
Points Downward
Upright
Indeterminate
Points Downward

90
QRS Axis Determination: Frontal Plane
Quadrant Method:
+0o
+90o
-90o
±180o

91
QRS Axis Determination: Frontal Plane
Degree Method:
Use Leads I & aVF
A negative wave (usually an S wave)
is subtracted from the height of the R
wave.
Plot the resultant vector on the
hexaxial reference circle to locate the
axis

92
QRS Axis Determination: Frontal Plane
Degree Method: Step 1

93
QRS Axis Determination: Frontal Plane
Degree Method: Step 2

94
QRS Axis Determination: Frontal Plane
Degree Method: Step 3

95
QRS Axis Determination: Frontal Plane
Null Plane Method:
Identify the equiphasic QRS
Locate the corresponding perpendicular
lead
Map the axis that is parallel to this lead
The axis points to the predominant
direction of either the positive or
negative pole

96
Horizontal Axis Rotation
◈ Dominance of Electrical Vector (Normal):
◈ V3 : R > S
◈ V4 : S > R
(V3 & V4 is the transition zone)◈ Identify the relationship of S-deflection &
R-deflection in V1 to V6
◈ Determine Axis Rotation:
◈ Clockwise Rotation – Shift to V5 & V6
◈ Counter-clockwise Rotation – Shift to V1
& V2
◈ Dominance of Electrical Vector (Normal):
◈ V3 : R > S
◈ V4 : S > R
(V3 & V4 is the transition zone)◈ Identify the relationship of S-deflection &
R-deflection in V1 to V6
◈ Determine Axis Rotation:
◈ Clockwise Rotation – Shift to V5 & V6
◈ Counter-clockwise Rotation – Shift to V1
& V2

97
Clinical Significance of ECG Interpretation
Recognizing Life-threatening dysrhythmias
is extremely important:
prompt interventions for cardiac arrest & cardiac
compromise
restoration of haemodynamic stability
Familiarizing with anti-arrhythmic
medications & life-saving measures are
essential
Further readings:
Advanced Cardiac Life Support (ACLS)
algorithms

98
Medication Indications Adult Dosage Amiodarone Extremely potent & effective:
Ventricular fibrillation and pulseless VT (FIRST CHOICE in newest ACLS guidelines)
SVT Recurrent life-threatening ventricular
arrhythmias
300mg IV push x refractory ventricular arrhythmias
150mg IV bolus over 10 mins for hemodynamically stable ventricular arrhythmias
infusion: 1mg/min for 6 hrs then 0.5mg/min for 18 hrs
maintenance dose 200-600mg/day p.o.
Lidocaine Acute ventricular arrhythmias (second-tier choice)
Stable VT
Loading bolus 1mg/Kg Additional boluses 0.5-1.5mg/kg Q5-
10mins to total 3mg/Kg IV infusion 0.5-4mg/min
Digoxin Narrow toxic-to-therapeutic dose especially with hypokalemia, hypomagnesemia & acid-base abnormalities
Rapid ventricular response in atrial flutter or atrial fibrillation
Beta-blockers: e.g.,
Propanolol Metoprolol Labetolol
Refractory SVT Ventricular arrhythmias associated
with digitalis toxicity Hypertensive crisis
Calcium channel blockers: e.g.
Verapamil Diltiazem
PSVT Narrow complex tachyarrhythmias
Adenosine (ATP) Drug of choice for symptomatic PSVT Arrhythmias due to reentry pathways
involving AV or sinus nodes
6.0mg initially IV PUSH (1-3sec.) repeat at 12mg after 1-2mins & repeat12mg IV push to a total of 30mg
consider alternative therapy for persistent tachyarrhythmias
Antiarrhythmic Therapy

99
References Davis, D. (2001). Quick and Accurate: 12-Lead ECG
Interpretation. (3rd Ed.). Philadelphia: Lippincott.
Huszar, R. J. (2002). Basic Dysrhythmias: Interpretation & Management. (3rd Ed.). St Louis: Mosby.
Huszar, R. J. (2002). Pocket Guide to Basic Dysrhythmias: Interpretation & Management. (3rd Ed.). St Louis: Mosby.
Jackson, K. (Ed.). (2002). ECG Interpretation made Incredibly Easy. (2nd Ed.). Springhouse: Springhouse.
Linda, D., Urden, K. & Stacy, M. E. L. (2002). Thelan’s critical care nursing: diagnosis and management. (4th ed.). St Louis: Mosby.
Lewis, K. M. (2000). Sensible ECG Analysis. Albany: International Thomson Publishng Company.

100
References Paul, S. & Hebra, J. D. (1998). The Nurse’s
Guide to Cardiac Rhythm Interpretation: Implication for patient care. Philadelphia: Saunders.
Swearingen, P. L. & Keen, J. H. (2001). Manual of Critical Care Nursing: Nursing Interventions & Collaborative Management. (4th Ed.). St Louise: Lippincott.
1998 12-Lead ECG Interpretation. Baltimore: Williams & Wilkins *CD-ROM

101
Journals Adams-Hamoda, M. G., Caldwell, M. A., Stotts, N. A. &
Drew, B. J. (2003). Factors to Consider When Analyzing 12-Lead Electrocardiograms for Evidence of Acute Myocardial Ischemia. American Journal of Critical Care, 12(1) 9-18.
Hutchisson, B., Cossy, S. & Wheeler, R., (1999). Basic Electrocardiogram Interpretation for the OR Nurse. AORN Journal, 69(1) 221-239.
Henderson, N. (1997). Electrocardiography. Nursing Standard, 11(44) 45-56.
Drew, B. J. (2002). Celebrating the 100th birthday of the electrocardiogram: Lessons learned from research in cardiac monitoring. American Journal of Critical Care, 11(4) 378.

102
Web Resources■ Jenkins, D. & Gerrid, S. (2002). ECG Library. Retrieved July 20, 2005, from
http://www.ecglibrary.com/ecghome.html
■ Mysioki, F. (2003). McGill Medical Informatics. Electrocardiology and Cardiac Arrhythmias. Retrieved July 20, 2005, from McGill Univeristy, Physiology Department Web site: http://sprojects.mmi.mcgill.ca/cardiophysio/
■ SkillStat Learning Inc. (2005). SkillStat Learning Tools. Retrieved July 20, 2005, from http://www.skillstat.com/learn.htm
■ Scheinman, M. M. (n.d.). Supraventricular Tachycardias Tutorial. Retrieved July 20, 2005, from the Electrophysiology Service at UCSF in San Francisco, California Website: http://www.blaufuss.org/SVT/index.html
■ Texas Arrhythmias Institute. (n.d.). Educational Material: Arrhythmias & Heart Failure. Retrieved July 20, 2005, from http://www.txai.org/edu/education.htm
■ Wong, R. (n.d.). Heart Sound Tutorial. Retrieved July 20, 2005, from The Harbor-UCLA Medical Center, Research lab of John Michael Criley, M.D. Website: http://www.blaufuss.org/tutorial/indexTut.html#
■ Yaniwitz, F. G. (2002). ECG Learning Center in Cyberspace. Retrieved July 20, 2005, from University of Utah School of Medicine, ECG Department Web site: http://medlib.med.utah.edu/kw/ecg/index.html