Kidney Stones. EpidemiologyEpidemiology Bladder and kidney stones detected in Egyptian mummies...
25
Kidney Stones Kidney Stones
-
Upload
eustacia-mosley -
Category
Documents
-
view
231 -
download
11
Transcript of Kidney Stones. EpidemiologyEpidemiology Bladder and kidney stones detected in Egyptian mummies...
Kidney StonesKidney StonesKidney StonesKidney Stones
EpidemiologyEpidemiologyEpidemiologyEpidemiology
• Bladder and kidney stones Bladder and kidney stones detected in Egyptian mummies detected in Egyptian mummies dating back to 4800 BCdating back to 4800 BC
• Frere Jacques Beaulieu – Frere Jacques Beaulieu – renowned 17renowned 17thth century open century open stone surgeon who performed stone surgeon who performed 5000 open lithotomies over 30 5000 open lithotomies over 30 yearsyears
• Bladder and kidney stones Bladder and kidney stones detected in Egyptian mummies detected in Egyptian mummies dating back to 4800 BCdating back to 4800 BC
• Frere Jacques Beaulieu – Frere Jacques Beaulieu – renowned 17renowned 17thth century open century open stone surgeon who performed stone surgeon who performed 5000 open lithotomies over 30 5000 open lithotomies over 30 yearsyears
EpidemiologyEpidemiologyEpidemiologyEpidemiology
• Genetic FactorsGenetic Factors– Rare in Native Americans, Blacks, native Rare in Native Americans, Blacks, native
born Israelisborn Israelis– More common among Whites and AsiansMore common among Whites and Asians– 25% have family history25% have family history– May be result of polygenic defect with May be result of polygenic defect with
partial penetrance (Resnick, 1968)partial penetrance (Resnick, 1968)– RTA, cystinuria, several X-linked disordersRTA, cystinuria, several X-linked disorders
• Genetic FactorsGenetic Factors– Rare in Native Americans, Blacks, native Rare in Native Americans, Blacks, native
born Israelisborn Israelis– More common among Whites and AsiansMore common among Whites and Asians– 25% have family history25% have family history– May be result of polygenic defect with May be result of polygenic defect with
partial penetrance (Resnick, 1968)partial penetrance (Resnick, 1968)– RTA, cystinuria, several X-linked disordersRTA, cystinuria, several X-linked disorders
EpidemiologyEpidemiologyEpidemiologyEpidemiology
• Age and SexAge and Sex– Peak incidence in 20’s to 40’sPeak incidence in 20’s to 40’s– 3:1 male to female 3:1 male to female
• Higher incidence of struvite stones in femalesHigher incidence of struvite stones in females
– Equal tendency during childhoodEqual tendency during childhood– May have hormonal influenceMay have hormonal influence
• Age and SexAge and Sex– Peak incidence in 20’s to 40’sPeak incidence in 20’s to 40’s– 3:1 male to female 3:1 male to female
• Higher incidence of struvite stones in femalesHigher incidence of struvite stones in females
– Equal tendency during childhoodEqual tendency during childhood– May have hormonal influenceMay have hormonal influence
EpidemiologyEpidemiologyEpidemiologyEpidemiology
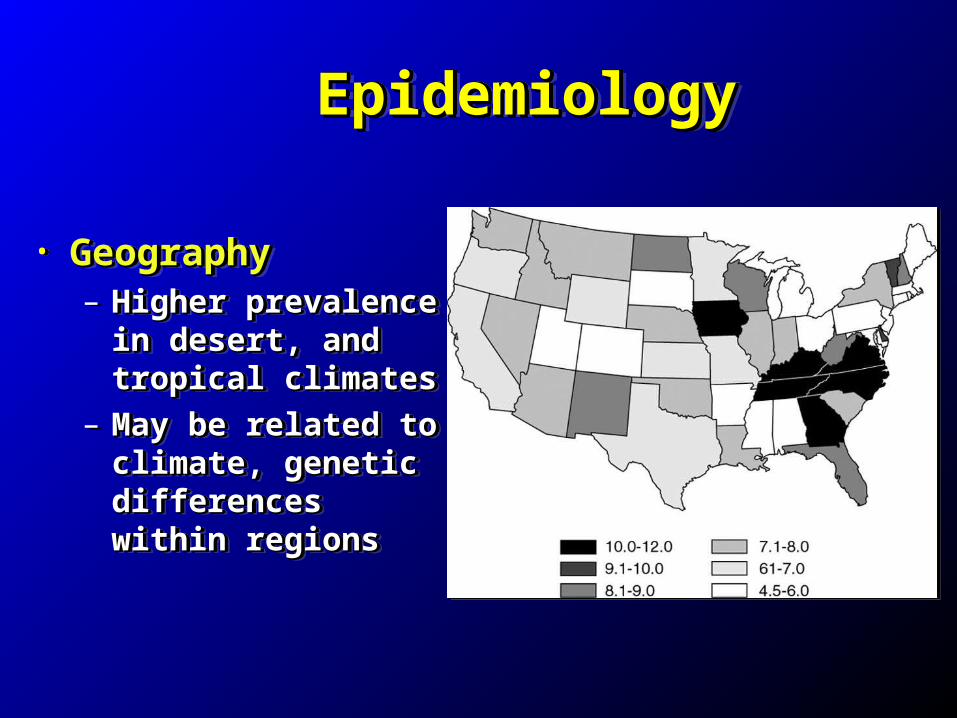
• GeographyGeography– Higher prevalence in Higher prevalence in
desert, and tropical desert, and tropical climatesclimates
– May be related to May be related to climate, genetic climate, genetic differences within differences within regionsregions
• GeographyGeography– Higher prevalence in Higher prevalence in
desert, and tropical desert, and tropical climatesclimates
– May be related to May be related to climate, genetic climate, genetic differences within differences within regionsregions
EpidemiologyEpidemiologyEpidemiologyEpidemiology
• Climatic and Seasonal FactorsClimatic and Seasonal Factors– Higher incidence in summer monthsHigher incidence in summer months– Peak 1-2 months after the max mean Peak 1-2 months after the max mean
temperature (Prince and Scardino, 1960)temperature (Prince and Scardino, 1960)– Increased perspiration leads to increased urine Increased perspiration leads to increased urine
concentrationconcentration– Increased sunlight exposure leads to vitamin D, Increased sunlight exposure leads to vitamin D,
and increased urinary calcium excretion (Parry and increased urinary calcium excretion (Parry and Lister, 1975)and Lister, 1975)
• Climatic and Seasonal FactorsClimatic and Seasonal Factors– Higher incidence in summer monthsHigher incidence in summer months– Peak 1-2 months after the max mean Peak 1-2 months after the max mean
temperature (Prince and Scardino, 1960)temperature (Prince and Scardino, 1960)– Increased perspiration leads to increased urine Increased perspiration leads to increased urine
concentrationconcentration– Increased sunlight exposure leads to vitamin D, Increased sunlight exposure leads to vitamin D,
and increased urinary calcium excretion (Parry and increased urinary calcium excretion (Parry and Lister, 1975)and Lister, 1975)
EpidemiologyEpidemiologyEpidemiologyEpidemiology
• Water IntakeWater Intake– Water intake versus water lost through Water intake versus water lost through
perspiration and respirationperspiration and respiration– Mineral content of water consumedMineral content of water consumed– Dilutes and decreases transit time of solutesDilutes and decreases transit time of solutes
• OccupationOccupation– Stone disease more likely in sedentary Stone disease more likely in sedentary
individuals, increased bone resorptionindividuals, increased bone resorption– Risk increased in more affluent individualsRisk increased in more affluent individuals
• Water IntakeWater Intake– Water intake versus water lost through Water intake versus water lost through
perspiration and respirationperspiration and respiration– Mineral content of water consumedMineral content of water consumed– Dilutes and decreases transit time of solutesDilutes and decreases transit time of solutes
• OccupationOccupation– Stone disease more likely in sedentary Stone disease more likely in sedentary
individuals, increased bone resorptionindividuals, increased bone resorption– Risk increased in more affluent individualsRisk increased in more affluent individuals
Types of StonesTypes of StonesTypes of StonesTypes of Stones• CalciumCalcium• Uric AcidUric Acid• Struvite – Magnesium Ammonium PhosphateStruvite – Magnesium Ammonium Phosphate• CystineCystine• OthersOthers– DihydroxyadenineDihydroxyadenine– XanthineXanthine– Silicate – antacid abusersSilicate – antacid abusers– Matrix – urease-splitting organismsMatrix – urease-splitting organisms– Ammonium Acid UrateAmmonium Acid Urate– TriamtereneTriamterene– IndinavirIndinavir
• CalciumCalcium• Uric AcidUric Acid• Struvite – Magnesium Ammonium PhosphateStruvite – Magnesium Ammonium Phosphate• CystineCystine• OthersOthers– DihydroxyadenineDihydroxyadenine– XanthineXanthine– Silicate – antacid abusersSilicate – antacid abusers– Matrix – urease-splitting organismsMatrix – urease-splitting organisms– Ammonium Acid UrateAmmonium Acid Urate– TriamtereneTriamterene– IndinavirIndinavir
Clinical PresentationClinical PresentationClinical PresentationClinical Presentation
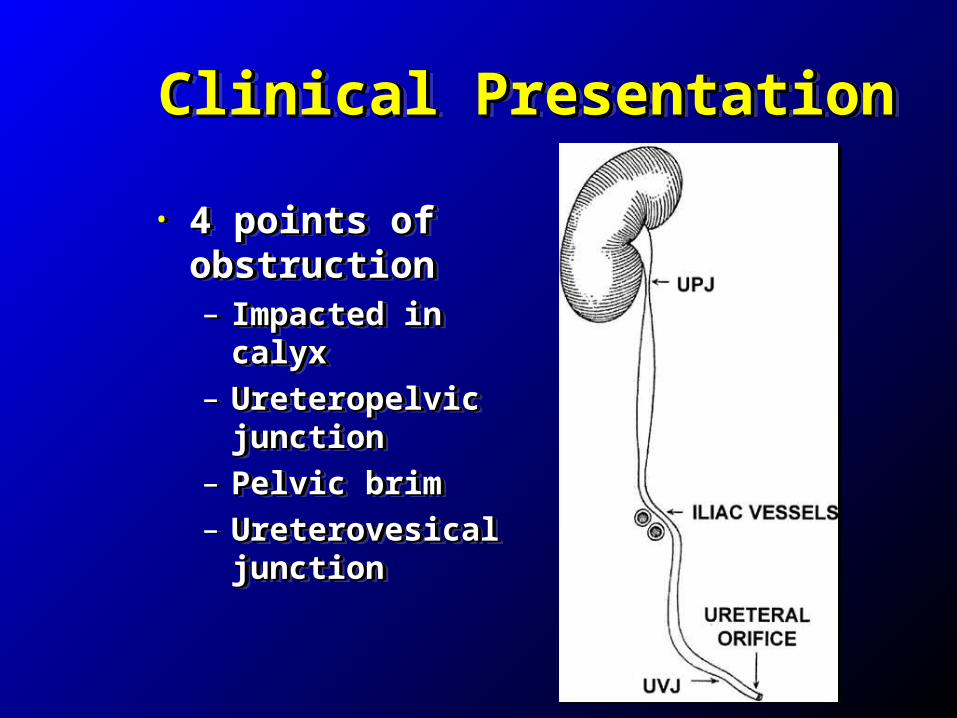
• 4 points of 4 points of obstructionobstruction– Impacted in calyxImpacted in calyx
– Ureteropelvic Ureteropelvic junctionjunction
– Pelvic brimPelvic brim
– Ureterovesical Ureterovesical junctionjunction
• 4 points of 4 points of obstructionobstruction– Impacted in calyxImpacted in calyx
– Ureteropelvic Ureteropelvic junctionjunction
– Pelvic brimPelvic brim
– Ureterovesical Ureterovesical junctionjunction
Clinical PresentationClinical PresentationClinical PresentationClinical Presentation
• Renal or ureteral colicRenal or ureteral colic– Acute onsetAcute onset– Usually begins in flank, courses laterally Usually begins in flank, courses laterally
around abdomen and radiates to the groin or around abdomen and radiates to the groin or genital regiongenital region
– Patients find it impossible to find comfortable Patients find it impossible to find comfortable positionposition
– Often nausea, emesis, ileus, diarrheaOften nausea, emesis, ileus, diarrhea
• Renal or ureteral colicRenal or ureteral colic– Acute onsetAcute onset– Usually begins in flank, courses laterally Usually begins in flank, courses laterally
around abdomen and radiates to the groin or around abdomen and radiates to the groin or genital regiongenital region
– Patients find it impossible to find comfortable Patients find it impossible to find comfortable positionposition
– Often nausea, emesis, ileus, diarrheaOften nausea, emesis, ileus, diarrhea
Clinical PresentationClinical PresentationClinical PresentationClinical Presentation
• UrinalysisUrinalysis– Microscopic or gross hematuriaMicroscopic or gross hematuria
• 15% without hematuria (Press and Smith, 1995)15% without hematuria (Press and Smith, 1995)
– Moderate LE / pyuriaModerate LE / pyuria– May have urinary crystalsMay have urinary crystals
• Calcium oxalate crystals may be found if urine Calcium oxalate crystals may be found if urine allowed to sitallowed to sit
• UrinalysisUrinalysis– Microscopic or gross hematuriaMicroscopic or gross hematuria
• 15% without hematuria (Press and Smith, 1995)15% without hematuria (Press and Smith, 1995)
– Moderate LE / pyuriaModerate LE / pyuria– May have urinary crystalsMay have urinary crystals
• Calcium oxalate crystals may be found if urine Calcium oxalate crystals may be found if urine allowed to sitallowed to sit
Radiographic EvaluationRadiographic EvaluationRadiographic EvaluationRadiographic Evaluation
• Plain abdominal radiograph (KUB)Plain abdominal radiograph (KUB)– 90% radio-opaque90% radio-opaque
• Uric acid, indinavir, triamterene and matrix Uric acid, indinavir, triamterene and matrix radiolucentradiolucent
• Cystine, struvite less radiodenseCystine, struvite less radiodense• Sensitivity 45-59%Sensitivity 45-59%• Specificity 71-77%Specificity 71-77%• Can be useful to guide treatment (i.e. offer ESWL)Can be useful to guide treatment (i.e. offer ESWL)
• Plain abdominal radiograph (KUB)Plain abdominal radiograph (KUB)– 90% radio-opaque90% radio-opaque
• Uric acid, indinavir, triamterene and matrix Uric acid, indinavir, triamterene and matrix radiolucentradiolucent
• Cystine, struvite less radiodenseCystine, struvite less radiodense• Sensitivity 45-59%Sensitivity 45-59%• Specificity 71-77%Specificity 71-77%• Can be useful to guide treatment (i.e. offer ESWL)Can be useful to guide treatment (i.e. offer ESWL)
Radiographic EvaluationRadiographic EvaluationRadiographic EvaluationRadiographic Evaluation
• Intravenous Pyelogram (IVP)Intravenous Pyelogram (IVP)– Previously the study of choicePreviously the study of choice– Allows determination of obstruction, relative Allows determination of obstruction, relative
functionfunction– More time consumingMore time consuming– More invasiveMore invasive– Sensitivity 64-87%Sensitivity 64-87%– Specificity 92-94%Specificity 92-94%
• Intravenous Pyelogram (IVP)Intravenous Pyelogram (IVP)– Previously the study of choicePreviously the study of choice– Allows determination of obstruction, relative Allows determination of obstruction, relative
functionfunction– More time consumingMore time consuming– More invasiveMore invasive– Sensitivity 64-87%Sensitivity 64-87%– Specificity 92-94%Specificity 92-94%
Radiographic EvaluationRadiographic EvaluationRadiographic EvaluationRadiographic Evaluation
• CT scan (non-contrast)CT scan (non-contrast)– Decreased time / Cost effectiveDecreased time / Cost effective– No need for IV access or IV contrastNo need for IV access or IV contrast– Sensitivity 95-100%Sensitivity 95-100%– Specificity 92-94%Specificity 92-94%– Does not give definitive information regarding Does not give definitive information regarding
function, obstructionfunction, obstruction– Secondary signs of obstructionSecondary signs of obstruction
• Hydroureter, perinephric stranding, hydronephrosisHydroureter, perinephric stranding, hydronephrosis
• CT scan (non-contrast)CT scan (non-contrast)– Decreased time / Cost effectiveDecreased time / Cost effective– No need for IV access or IV contrastNo need for IV access or IV contrast– Sensitivity 95-100%Sensitivity 95-100%– Specificity 92-94%Specificity 92-94%– Does not give definitive information regarding Does not give definitive information regarding
function, obstructionfunction, obstruction– Secondary signs of obstructionSecondary signs of obstruction
• Hydroureter, perinephric stranding, hydronephrosisHydroureter, perinephric stranding, hydronephrosis
Radiographic EvaluationRadiographic EvaluationRadiographic EvaluationRadiographic Evaluation
• Ultrasound – Ultrasound – • can demonstrate hyperechoic focus with can demonstrate hyperechoic focus with
posterior shadowing c/w a stoneposterior shadowing c/w a stone
• Overall, not a very good imaging modality Overall, not a very good imaging modality for stones.for stones.
• MRIMRI• Also a poor imaging modality for stones.Also a poor imaging modality for stones.
• Ultrasound – Ultrasound – • can demonstrate hyperechoic focus with can demonstrate hyperechoic focus with
posterior shadowing c/w a stoneposterior shadowing c/w a stone
• Overall, not a very good imaging modality Overall, not a very good imaging modality for stones.for stones.
• MRIMRI• Also a poor imaging modality for stones.Also a poor imaging modality for stones.
ManagementManagementManagementManagement• Hospital admission required if…Hospital admission required if…– Severe Pain, N/V not controlled by medicationsSevere Pain, N/V not controlled by medications– Bilateral obstruction, anuria, or ureteral stone Bilateral obstruction, anuria, or ureteral stone
with a solitary kidneywith a solitary kidney– Signs of obstruction & UTI/sepsis from stoneSigns of obstruction & UTI/sepsis from stone
Elevated WBC, fevers, clinical pyelonephritisElevated WBC, fevers, clinical pyelonephritis
• Obstructing ureteral stones > 6 mm are less Obstructing ureteral stones > 6 mm are less likely to pass, may require interventionlikely to pass, may require intervention• stent placement vs. surgical removalstent placement vs. surgical removal
• Hospital admission required if…Hospital admission required if…– Severe Pain, N/V not controlled by medicationsSevere Pain, N/V not controlled by medications– Bilateral obstruction, anuria, or ureteral stone Bilateral obstruction, anuria, or ureteral stone
with a solitary kidneywith a solitary kidney– Signs of obstruction & UTI/sepsis from stoneSigns of obstruction & UTI/sepsis from stone
Elevated WBC, fevers, clinical pyelonephritisElevated WBC, fevers, clinical pyelonephritis
• Obstructing ureteral stones > 6 mm are less Obstructing ureteral stones > 6 mm are less likely to pass, may require interventionlikely to pass, may require intervention• stent placement vs. surgical removalstent placement vs. surgical removal
ManagementManagementManagementManagement
• Adequate Fluids / HydrationAdequate Fluids / Hydration– Increased diuresis may reduce rate of ureteral Increased diuresis may reduce rate of ureteral
peristalsis and inhibit stone passage?peristalsis and inhibit stone passage?• Anti-inflammatory agentsAnti-inflammatory agents– OK if creatinine is normalOK if creatinine is normal– Patients who received Toradol versus Demerol left Patients who received Toradol versus Demerol left
hospital earlier, better pain control (Larkin, 1999)hospital earlier, better pain control (Larkin, 1999)• Narcotics: Morphine / DilaudidNarcotics: Morphine / Dilaudid• Flomax / Uroxatral to help pass the stoneFlomax / Uroxatral to help pass the stone• Only about 10% of patients require admissionOnly about 10% of patients require admission
• Adequate Fluids / HydrationAdequate Fluids / Hydration– Increased diuresis may reduce rate of ureteral Increased diuresis may reduce rate of ureteral
peristalsis and inhibit stone passage?peristalsis and inhibit stone passage?• Anti-inflammatory agentsAnti-inflammatory agents– OK if creatinine is normalOK if creatinine is normal– Patients who received Toradol versus Demerol left Patients who received Toradol versus Demerol left
hospital earlier, better pain control (Larkin, 1999)hospital earlier, better pain control (Larkin, 1999)• Narcotics: Morphine / DilaudidNarcotics: Morphine / Dilaudid• Flomax / Uroxatral to help pass the stoneFlomax / Uroxatral to help pass the stone• Only about 10% of patients require admissionOnly about 10% of patients require admission
Stone Prevention: DietaryStone Prevention: Dietary Stone Prevention: DietaryStone Prevention: Dietary Calcium Oxylate: Calcium Oxylate: – Most common type of stone ( About 80%)Most common type of stone ( About 80%)– Benefit from avoiding foods that are high in Benefit from avoiding foods that are high in
oxylate (low oxylate diet) oxylate (low oxylate diet) draft beer, certain juices and berries, certain green leafy draft beer, certain juices and berries, certain green leafy
vegetables, coffee, tea, peanut butter, chocolate, certain nuts vegetables, coffee, tea, peanut butter, chocolate, certain nuts
Avoid high doses of Vit. C ( > 500 mg) Avoid high doses of Vit. C ( > 500 mg) or Dor DVit C converted to oxylate and can increase Vit C converted to oxylate and can increase
urinary oxylateurinary oxylate
Calcium Oxylate: Calcium Oxylate: – Most common type of stone ( About 80%)Most common type of stone ( About 80%)– Benefit from avoiding foods that are high in Benefit from avoiding foods that are high in
oxylate (low oxylate diet) oxylate (low oxylate diet) draft beer, certain juices and berries, certain green leafy draft beer, certain juices and berries, certain green leafy
vegetables, coffee, tea, peanut butter, chocolate, certain nuts vegetables, coffee, tea, peanut butter, chocolate, certain nuts
Avoid high doses of Vit. C ( > 500 mg) Avoid high doses of Vit. C ( > 500 mg) or Dor DVit C converted to oxylate and can increase Vit C converted to oxylate and can increase
urinary oxylateurinary oxylate
Dietary Counseling: CalciumDietary Counseling: CalciumDietary Counseling: CalciumDietary Counseling: Calcium
Diet should contain adequate calciumDiet should contain adequate calcium– Moderate Ca intake, normal Ca diet (800-Moderate Ca intake, normal Ca diet (800-
1000 mg/day)1000 mg/day)– Prevents calcium oxylate stones with lower GI Prevents calcium oxylate stones with lower GI
oxylate absorption. oxylate absorption.
Don’t avoid calciumDon’t avoid calcium Although certain kinds of stones can be caused by Although certain kinds of stones can be caused by
excessive calcium, overall lower incidence of stones in excessive calcium, overall lower incidence of stones in people who have adequate, but not excessive amounts of people who have adequate, but not excessive amounts of calcium compared to too little calcium in the dietcalcium compared to too little calcium in the diet
Diet should contain adequate calciumDiet should contain adequate calcium– Moderate Ca intake, normal Ca diet (800-Moderate Ca intake, normal Ca diet (800-
1000 mg/day)1000 mg/day)– Prevents calcium oxylate stones with lower GI Prevents calcium oxylate stones with lower GI
oxylate absorption. oxylate absorption.
Don’t avoid calciumDon’t avoid calcium Although certain kinds of stones can be caused by Although certain kinds of stones can be caused by
excessive calcium, overall lower incidence of stones in excessive calcium, overall lower incidence of stones in people who have adequate, but not excessive amounts of people who have adequate, but not excessive amounts of calcium compared to too little calcium in the dietcalcium compared to too little calcium in the diet
Dietary CounselingDietary CounselingDietary CounselingDietary Counseling
Fluid consumption: Fluid consumption: – adequate to produce > 2L daily urine output adequate to produce > 2L daily urine output – To accomplish this, one must drink >2L To accomplish this, one must drink >2L
some fluid is lost with breathing, sweating and some fluid is lost with breathing, sweating and other normal body functionsother normal body functions
– Supplementing the diet with lemonade Supplementing the diet with lemonade helpful since it contains citrate which can helpful since it contains citrate which can
dissolve some crystals that form stones.dissolve some crystals that form stones.
Fluid consumption: Fluid consumption: – adequate to produce > 2L daily urine output adequate to produce > 2L daily urine output – To accomplish this, one must drink >2L To accomplish this, one must drink >2L
some fluid is lost with breathing, sweating and some fluid is lost with breathing, sweating and other normal body functionsother normal body functions
– Supplementing the diet with lemonade Supplementing the diet with lemonade helpful since it contains citrate which can helpful since it contains citrate which can
dissolve some crystals that form stones.dissolve some crystals that form stones.
Dietary CounselingDietary CounselingDietary CounselingDietary Counseling Excessive protein (high purine diet)Excessive protein (high purine diet)– should be avoided, especially red meatsshould be avoided, especially red meats– High protein (Atkins diet) leads to a High protein (Atkins diet) leads to a
chronic acidosis increasing stone ratechronic acidosis increasing stone rate Low Sodium DietLow Sodium Diet– Also recommended, generally <2g daily, Also recommended, generally <2g daily,
with avoidance table salt, canned foods, with avoidance table salt, canned foods, processed foods, or things such as Chinese processed foods, or things such as Chinese food that may be high is sodium. food that may be high is sodium.
Excessive protein (high purine diet)Excessive protein (high purine diet)– should be avoided, especially red meatsshould be avoided, especially red meats– High protein (Atkins diet) leads to a High protein (Atkins diet) leads to a
chronic acidosis increasing stone ratechronic acidosis increasing stone rate Low Sodium DietLow Sodium Diet– Also recommended, generally <2g daily, Also recommended, generally <2g daily,
with avoidance table salt, canned foods, with avoidance table salt, canned foods, processed foods, or things such as Chinese processed foods, or things such as Chinese food that may be high is sodium. food that may be high is sodium.
ObesityObesityObesityObesity
• Higher rates of kidney stones in obese or Higher rates of kidney stones in obese or overweight (Multifactorial)overweight (Multifactorial)
• Sedentary lifestyleSedentary lifestyle• Dietary: Purine Gluttony, excessive NaDietary: Purine Gluttony, excessive Na• More difficult to intervene surgicallyMore difficult to intervene surgically• ESWL or PCNLESWL or PCNL
• Recommend a balanced approach with Recommend a balanced approach with diet, weight loss and exercisediet, weight loss and exercise
• Higher rates of kidney stones in obese or Higher rates of kidney stones in obese or overweight (Multifactorial)overweight (Multifactorial)
• Sedentary lifestyleSedentary lifestyle• Dietary: Purine Gluttony, excessive NaDietary: Purine Gluttony, excessive Na• More difficult to intervene surgicallyMore difficult to intervene surgically• ESWL or PCNLESWL or PCNL
• Recommend a balanced approach with Recommend a balanced approach with diet, weight loss and exercisediet, weight loss and exercise
Counseling ContinuedCounseling ContinuedCounseling ContinuedCounseling Continued
Initial stone episode:Initial stone episode:– Overall, with no treatment or dietary Overall, with no treatment or dietary
changes, there is about a 50% chance of changes, there is about a 50% chance of forming another stone within 5 years. forming another stone within 5 years.
– If another stone episode does occur despite If another stone episode does occur despite dietary measures, I recommend a full dietary measures, I recommend a full metabolic work-up to include blood tests and metabolic work-up to include blood tests and a urorisk panel.a urorisk panel.
CA, Mg, Phos, Uric Acid, Urorisk.CA, Mg, Phos, Uric Acid, Urorisk.
Initial stone episode:Initial stone episode:– Overall, with no treatment or dietary Overall, with no treatment or dietary
changes, there is about a 50% chance of changes, there is about a 50% chance of forming another stone within 5 years. forming another stone within 5 years.
– If another stone episode does occur despite If another stone episode does occur despite dietary measures, I recommend a full dietary measures, I recommend a full metabolic work-up to include blood tests and metabolic work-up to include blood tests and a urorisk panel.a urorisk panel.
CA, Mg, Phos, Uric Acid, Urorisk.CA, Mg, Phos, Uric Acid, Urorisk.
Surgical InterventionSurgical InterventionSurgical InterventionSurgical Intervention
ESWLESWL– Radiodense stones <2 cm in good locationRadiodense stones <2 cm in good location
Ureteroscopy/Stone removalUreteroscopy/Stone removal– Renal/Ureteral stones <2 cmRenal/Ureteral stones <2 cm
PCNLPCNL– Large Renal or proximal ureteral stones, Large Renal or proximal ureteral stones,
staghorn calculistaghorn calculi Open/Laparoscopic stone removal (rare)Open/Laparoscopic stone removal (rare)
ESWLESWL– Radiodense stones <2 cm in good locationRadiodense stones <2 cm in good location
Ureteroscopy/Stone removalUreteroscopy/Stone removal– Renal/Ureteral stones <2 cmRenal/Ureteral stones <2 cm
PCNLPCNL– Large Renal or proximal ureteral stones, Large Renal or proximal ureteral stones,
staghorn calculistaghorn calculi Open/Laparoscopic stone removal (rare)Open/Laparoscopic stone removal (rare)
Questions?Questions?