Kidney disease and African ancestry
2
NEWS AND VIEWS Kidney disease and African ancestry Martin R Pollak Mapping by admixture linkage disequilibrium (MALD) leverages differences in disease frequencies among ancestry groups to map disease-susceptibility loci on the basis of genetic admixture. Two new studies use MALD to identify variation at the MYH9 locus as a major factor for the increased risk of nondiabetic kidney disease in African Americans. Individuals of African descent carry a signifi- cantly increased risk of kidney failure 1,2 . The nature of this increased risk has not been well understood. This disparity represents a serious public health problem given the high cost of keeping individuals with end-stage renal disease (ESRD) alive by kidney transplantation or dialy- sis, as well as the high morbidity and mortality even among people with moderate kidney dis- ease who do not yet require these heroic forms of treatment. Often, individuals with kidney disease do not receive a histological evaluation: physicians frequently make the clinical diagno- sis of hypertension-induced kidney damage, particularly in African Americans with long- standing hypertension and progressive kidney dysfunction. Notably, the pattern of kidney injury known as focal and segmental glom- erulosclerosis (FSGS), diagnosed on the basis of kidney biopsy examination, is three to four times more common in individuals of African ancestry. Two new studies, on pages 1175 and 1185 of this issue 3,4 , now report a genetic locus, MYH9, that explains much of the increased risk of both of these diagnoses in this popula- tion, and thereby suggest a shared genetic (and pathophysiologic) etiology. Admixture mapping The admixture mapping scans described in both studies take advantage of the admixed genetic makeup of most African Americans, whose genomes contain a mixture of recent European and African ancestry 5 . The theory behind this approach is that regions of the genome carrying disease-susceptibility alleles should show a greater percentage of African ancestry when a sufficiently large population is studied. Such studies have been used in analy- ses of a number of clinical phenotypes with large differences in frequencies among these populations 6 . In one study, Kopp et al. 3 performed a genome-wide admixture scan in African Americans with FSGS and identified a region on chromosome 22 associated with a sig- nificant excess of African ancestry in affected individuals. Subsequent fine mapping iden- tified noncoding SNPs in or near the MYH9 gene (encoding nonmuscle myosin IIA) that conferred dose-dependent increases in FSGS risk. Similarly, Kao et al. 4 carried out a genome- wide admixture scan and found excess African ancestry in nondiabetic end-stage kidney dis- ease cases at this same locus. Further genotyp- ing again identified multiple linked noncoding SNPs in MYH9 conferring two to four times increased risk of ESRD. Both studies show a marked effect of MYH9 genotypes on the susceptibility of HIV-infected individuals to kidney disease. HIV nephropathy, like FSGS, is typically characterized by podocyte abnor- malities, as well as podocyte proliferation and collapse of glomerular capillaries (collapsing glomerulopathy). Of note, the MYH9 risk vari- ants are much more common among African Americans (60% of alleles) compared to European Americans (4% of alleles). In the study by Kopp et al., the presence of the FSGS-associated haplotype conferred an approximately fivefold increased risk under a recessive model. The absolute risk of devel- oping FSGS in an individual with the disease- associated haplotype is still quite low, but the population-attributable risk is significant. Thus, although highly penetrant mutations in the FSGS-associated genes ACTN4, TRPC6 or NPHS2 can be said to cause FSGS 7–9 , the same cannot be said of these MYH9 variants. The question of what other genetic or environmen- tal factors trigger disease in the population with the high-risk MYH9 genotype is still open. As interesting as what these studies did find is what they did not find: no association was observed between these MYH9 variants and Martin R. Pollak is in the Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts 02115, USA. e-mail: [email protected] NATURE GENETICS | VOLUME 40 | NUMBER 10 | OCTOBER 2008 1145 Figure 1 Sequential electron micrographs (EM) of a glomerulus showing glomerular capillary loops covered by podocytes and their interdigitating contractile extensions known as foot processes. (a) Scanning EM of a single glomerulus. (b) Scanning EM of a capillary segment. (c) Transmission EM showing transverse section of a glomerular capillary. GCW, glomerular capillary wall; PODO, podocyte cell body; FP, podocyte foot processes. Images courtesy of J. Henderson (Department of Pathology, Brigham and Women’s Hospital).
Transcript of Kidney disease and African ancestry

news and v iews
Kidney disease and african ancestryMartin R Pollak
Mapping by admixture linkage disequilibrium (MaLd) leverages differences in disease frequencies among ancestry groups to map disease-susceptibility loci on the basis of genetic admixture. Two new studies use MaLd to identify variation at the MYH9 locus as a major factor for the increased risk of nondiabetic kidney disease in african americans.
Individuals of African descent carry a signifi-cantly increased risk of kidney failure1,2. The nature of this increased risk has not been well understood. This disparity represents a serious public health problem given the high cost of keeping individuals with end-stage renal disease (ESRD) alive by kidney transplantation or dialy-sis, as well as the high morbidity and mortality even among people with moderate kidney dis-ease who do not yet require these heroic forms of treatment. Often, individuals with kidney disease do not receive a histological evaluation: physicians frequently make the clinical diagno-sis of hypertension-induced kidney damage, particularly in African Americans with long-standing hypertension and progressive kidney dysfunction. Notably, the pattern of kidney injury known as focal and segmental glom-erulosclerosis (FSGS), diagnosed on the basis of kidney biopsy examination, is three to four times more common in individuals of African ancestry. Two new studies, on pages 1175 and 1185 of this issue3,4, now report a genetic locus, MYH9, that explains much of the increased risk of both of these diagnoses in this popula-tion, and thereby suggest a shared genetic (and pathophysiologic) etiology.
Admixture mappingThe admixture mapping scans described in both studies take advantage of the admixed genetic makeup of most African Americans, whose genomes contain a mixture of recent European and African ancestry5. The theory behind this approach is that regions of the
genome carrying disease-susceptibility alleles should show a greater percentage of African ancestry when a sufficiently large population is studied. Such studies have been used in analy-ses of a number of clinical phenotypes with large differences in frequencies among these populations6.
In one study, Kopp et al.3 performed a genome-wide admixture scan in African Americans with FSGS and identified a region on chromosome 22 associated with a sig-nificant excess of African ancestry in affected individuals. Subsequent fine mapping iden-tified noncoding SNPs in or near the MYH9 gene (encoding nonmuscle myosin IIA) that conferred dose-dependent increases in FSGS risk. Similarly, Kao et al.4 carried out a genome-wide admixture scan and found excess African ancestry in nondiabetic end-stage kidney dis-ease cases at this same locus. Further genotyp-ing again identified multiple linked noncoding SNPs in MYH9 conferring two to four times increased risk of ESRD. Both studies show a marked effect of MYH9 genotypes on the susceptibility of HIV-infected individuals to
kidney disease. HIV nephropathy, like FSGS, is typically characterized by podocyte abnor-malities, as well as podocyte proliferation and collapse of glomerular capillaries (collapsing glomerulopathy). Of note, the MYH9 risk vari-ants are much more common among African Americans (60% of alleles) compared to European Americans (4% of alleles).
In the study by Kopp et al., the presence of the FSGS-associated haplotype conferred an approximately fivefold increased risk under a recessive model. The absolute risk of devel-oping FSGS in an individual with the disease-associated haplotype is still quite low, but the population-attributable risk is significant. Thus, although highly penetrant mutations in the FSGS-associated genes ACTN4, TRPC6 or NPHS2 can be said to cause FSGS7–9, the same cannot be said of these MYH9 variants. The question of what other genetic or environmen-tal factors trigger disease in the population with the high-risk MYH9 genotype is still open.
As interesting as what these studies did find is what they did not find: no association was observed between these MYH9 variants and
Martin R. Pollak is in the Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts 02115, USA. e-mail: [email protected]
nature genetics | volume 40 | number 10 | october 2008 1145
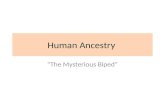
Figure 1 Sequential electron micrographs (EM) of a glomerulus showing glomerular capillary loops covered by podocytes and their interdigitating contractile extensions known as foot processes. (a) Scanning EM of a single glomerulus. (b) Scanning EM of a capillary segment. (c) Transmission EM showing transverse section of a glomerular capillary. GCW, glomerular capillary wall; PODO, podocyte cell body; FP, podocyte foot processes. Images courtesy of J. Henderson (Department of Pathology, Brigham and Women’s Hospital).

news and v iews
the risk of nephropathy from diabetes. It is cer-tainly plausible that risk factors for one form of chronic renal injury (for example, that resulting from hypertension) would also be risk factors for others (diabetic kidney disease). However, this was not observed in either study. This is particularly interesting because hypertension and diabetes so often occur together in affected individuals. The fact that, despite this potential confounder, no association was observed in dia-betic kidney disease is strong support that dif-ferent genetic factors (and therefore different cellular mechanisms) underlie the susceptibil-ity to kidney damage from these two common disorders.
Clinical implicationsThere are a number of notable clinical and pathophysiological questions that arise from these findings. High on the list is defining the precise variant(s) that alter disease susceptibil-ity. Highly penetrant mutations in the MYH9 coding region cause forms of inherited disease leading to both kidney and hematologic abnor-malities10. Other cytoskeletal proteins have been shown to be critical for normal podo-cyte function9,11. Nonmuscle myosins have been known for some time to be components of the podocyte cytoskeleton, contributing to its contractile functions (Fig. 1)12. Although podocytes have been the focus of much recent
research in inherited and secondary renal dis-ease, it is premature to assume that altered myosin function in podocytes is responsible for modulating human disease. For example, nonmuscle myosin IIA is the only isoform of nonmuscle myosin II expressed in platelets, and one could imagine how genetic variants altering the regulated expression of MYH9 could alter platelet function in some subtle way that predisposes the glomerular endothelium to damage. Other mechanistic hypotheses are possible as well.
Although it may be difficult to unravel the biology underlying these associations, there are some important and relatively straightfor-ward clinical questions that arise and should be answerable. Immune-modulating therapies have widely variable success in treating FSGS. Does an individual’s MYH9 genotype predict the response to these forms of treatment? Are drugs that act on the renin-angiotensin system—the mainstay of treatment for proteinuric kidney diseases—more (or perhaps less) effective in individuals with a given haplotype? How does the MYH9 genotype in a kidney harvested for transplantation (or its recipient) alter the clini-cal outcome?
In the meantime, clinicians should realize that the kidney damage seen in the context of two common disorders, hypertension and diabetes, may be distinct entities. On the other
hand, these results also suggest a shared etiology to many forms of nondiabetic kidney disease. The genetic relationship between hypertensive nephropathy and FSGS suggests that FSGS may be underdiagnosed. It also highlights the fact that use of the term FSGS, given the etiologi-cal complexity of this injury pattern, should be limited to histological description, rather than used as a clinical diagnosis. The success of these two studies further highlights the power of the admixture mapping approach. If we are to translate the genetic basis of human disease into improved patient care, understanding the broad implications of these important new studies will be critical.
1. Freedman, B.I. J. Am. Soc. Nephrol. 14, S192–S194 (2003).
2. Price, D.A. & Crook, E.D. J. Natl. Med. Assoc. 94, 16S–27S (2002).
3. Kopp, J.B. et al. Nat. Genet. 40, 1175–1184 (2008).
4. Kao, W.H.L. et al. Nat. Genet. 40, 1185–1192 (2008).
5. Patterson, N. et al. Am. J. Hum. Genet. 74, 979–1000 (2004).
6. Zhu, X., Tang, H. & Risch, N. Adv. Genet. 60, 547–569 (2008).
7. Winn, M.P. et al. Science 308, 1801–1804 (2005).8. Boute, N. et al. Nat. Genet. 24, 349–354 (2000).9. Kaplan, J.M. et al. Nat. Genet. 24, 251–256 (2000).10. Heath, K.E. et al. Am. J. Hum. Genet. 69, 1033–1045
(2001).11. Asanuma, K. et al. J. Clin. Invest. 115, 1188–1198
(2005).12. Drenckhahn, D. & Franke, R.P. Lab. Invest. 59, 673–
682 (1988).
1146 volume 40 | number 10 | october 2008 | nature genetics
Pristionchus pacificus: an appropriate fondness for beetlesJagan Srinivasan and Paul W Sternberg
The nematode Pristionchus pacificus associates with one particular beetle and eats its rotting corpse. The report of the genome sequence of P. pacificus, the fifth nematode to be sequenced and a useful secondary nematode genetic model system, highlights genes that may have influenced the route to parasitism.
J.B.S. Haldane saw the divine in the diver-sity of beetle species. Nematodes (round-worms), however, greatly outnumber beetles, comprising about a million species, includ-ing many parasites of humans, livestock and plants. One nematode, Caenorhabditis elegans, is a laboratory model for a wide
range of biological processes including sig-nal transduction and longevity, and it was one of the first animals to have its complete genome sequenced1. Although C. elegans has proven invaluable for studies of human genes and pathways, it has had far less of an impact on research of parasitic nematodes. Now, Ralf J. Sommer and colleagues2 report a draft genome sequence of the nematode Pristionchus pacificus, which might help bridge the gap between the model C. elegans and the diversity of nematode species.
P. pacificus (Fig. 1a), with its 3-day gen-eration time3, is highly amenable to genetic analysis, as it has similar genetics as C.
elegans: both have self-fertilizing hermaph-rodites, allowing rapid homozygosis of reces-sive alleles, and males, allowing crosses for genetic analysis. A SNP and physical map exists and allows positional cloning of genes4. The other three nematodes whose genomes are sequenced and published are C. briggsae5, a close relative of C. elegans, Meloidogyne incognita, a plant parasite6, and Brugia malayi, the causative agent of filariasis and elephantiasis7. P. pacificus is of interest not only because of its ease of manipulation in the laboratory but also because of its genetic distance from C. elegans and its different lifestyle.
Jagan Srinivasan and Paul W. Sternberg are in the Howard Hughes Medical Institute and Biology Division, California Institute of Technology, 156-29 1200 E. California Blvd, Pasadena, California 91125, USA. e-mail: [email protected] or [email protected]