Kidney
4
Lack of Aldosterone: -less Na+ absorption -> volume contraction -less K+ secretion -> hyperkalemia -less H+ secretion -> metabolic acidosis driving force is the high [ions] moving into the blood, loss of water volume, concentrating the ions K+ is zero urine [K+]determined by principal cells -10mV Na+ reabsorption by ENac Not water permeable Carbonic Anhydrase inhibitors: Increase HCO3- secretion Thiazide diuretics Inhibition of Na+Cl- cotransport Increase NaCl secretion K+ secretion Decrease Ca2+ secretion diluted urine WNK mutations -> overactive NCC: -NaCl reabsorption -Increased ECF volume -Hypertension stimulated by angiotensin II Bulk of Ca2+ absorbed Water Permeable -2mV Na+ taken in by SGLT2 H+ ATPase, H+ leaving cell Cl- exchanges with formic acid Most of the K+ is recycled Not water permeable -20-30% HCO3- is taken up, same mechanism as Proximal Tubule -the rest of the NaCl Na+, glucose/ amino acids/ phosphate low permeability of Cl- -> trapping it in the lumen Bulk reabsorption of Na+, HCO3-, H20, leaky epithelia K+ sparing diuretics Inhibition of Na+ absorption K+ secretion H+ secretion Increase Na+ secretion Decrease K+ secretion H+ secretion Bulk of Mg2+ absorbed Loop diuretics: Inhibition of Na+K+Cl- cotransport Increase NaCl secretion K+ secretion Ca2+ secretion Decrease concentrated urine +16mV K+ recycling by NKCC2 Ca2+ Sensing Receptor: Inhibits NKCC2 and ROMK lowering the potential in the lumen, reducing the electrical driving for Ca2+
description
physio
Transcript of Kidney

!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
Lack of Aldosterone:!-less Na+ absorption ->
volume contraction!-less K+ secretion ->
hyperkalemia!-less H+ secretion ->
metabolic acidosis
driving force is the high [ions] moving
into the blood, loss of water
volume, concentrating the
ions
K+ is zero !urine [K+]determined by
principal cells!
-10mV!Na+
reabsorption by ENac
Not water permeable
Carbonic Anhydrase
inhibitors:!Increase HCO3-
secretion
Thiazide diuretics!Inhibition of Na+Cl- cotransport!
Increase!NaCl secretion!
K+ secretion!Decrease!
Ca2+ secretion!diluted urine
WNK mutations -> overactive NCC:!
-NaCl reabsorption!-Increased ECF
volume!-Hypertension
stimulated by angiotensin II
Bulk of Ca2+ absorbed
Water Permeable
-2mV!Na+ taken in
by SGLT2
H+ ATPase, H+ leaving cell
Cl- exchanges with formic acid
Most of the K+ is recycled
Not water permeable
-20-30% HCO3- is taken up, same mechanism as
Proximal Tubule!-the rest of the NaCl
Na+, glucose/amino acids/
phosphate
low permeability
of Cl- -> trapping it in
the lumen
Bulk reabsorption of Na+, HCO3-, H20, leaky epithelia
K+ sparing diuretics!Inhibition of !
Na+ absorption!K+ secretion!
H+ secretion!Increase!
Na+ secretion!Decrease !
K+ secretion!
H+ secretion
Bulk of Mg2+ absorbed
Loop diuretics: Inhibition of Na+K+Cl- cotransport!
Increase !NaCl secretion!
K+ secretion!Ca2+ secretion!
Decrease!concentrated urine!
+16mV!K+ recycling by
NKCC2
Ca2+ Sensing Receptor: Inhibits NKCC2 and ROMK
lowering the potential in the lumen, reducing the
electrical driving for Ca2+

!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
Vasoconstriction:!
Sympathetic !of A"erent arteriole!Decrease GFR and RBF (renal blood flow)!
Increase Na+ reabsorption!Angiotensin II!
Acts on both a"erent and e"erent arteriole!
Decreasing GFR and RBF!Vasodilation!
Prostaglandins!
Prevents large changes in GFR by AngII -> Increasing GFR!
Atrial Natriuretic Peptide (ANP)!
Increase GFR
Glomerular Filtration Rate (GFR): volume of fluid filtered into Bowman's Capsule per
unit time!Renal Blood Flow (RBF):
Sympathetic E"ects:!
-Vasoconstriction!-Enhance Na+ reabsorption by Proximal Tubule!
-Renin (produced by granular cells in the a"erent arteriole) secretion
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
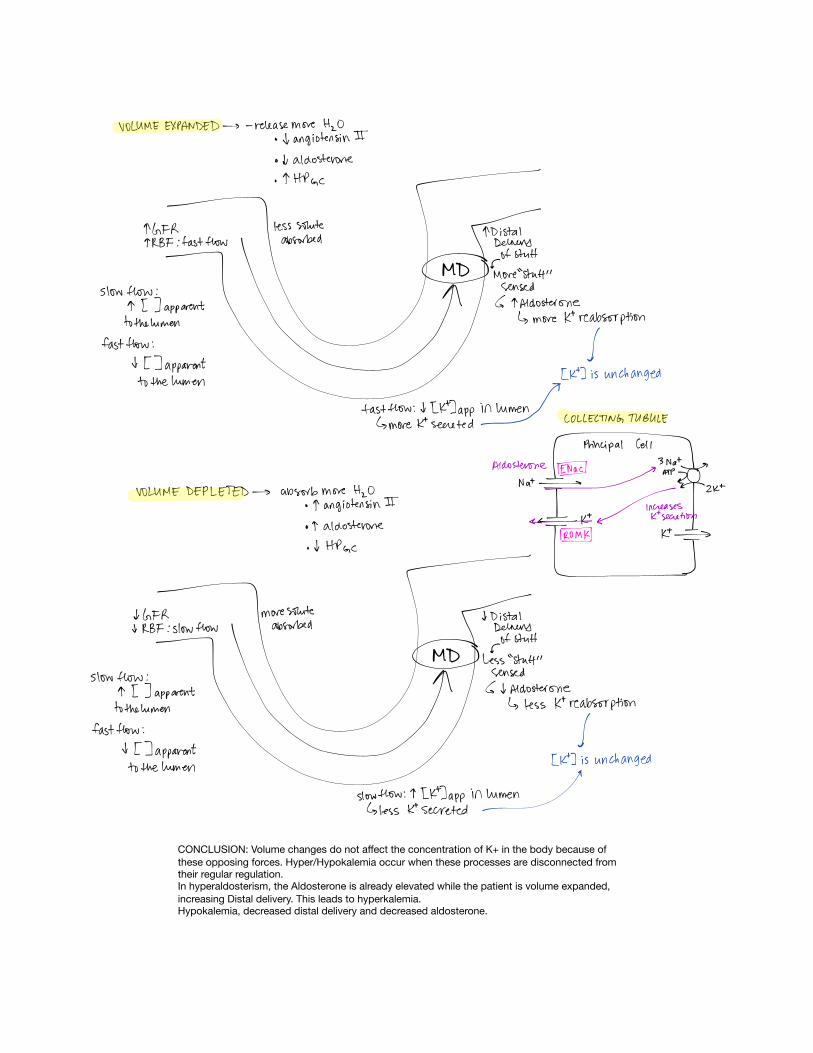
CONCLUSION: Volume changes do not a"ect the concentration of K+ in the body because of
these opposing forces. Hyper/Hypokalemia occur when these processes are disconnected from their regular regulation.!In hyperaldosterism, the Aldosterone is already elevated while the patient is volume expanded,
increasing Distal delivery. This leads to hyperkalemia.!Hypokalemia, decreased distal delivery and decreased aldosterone.
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
+16mV!K+ recycling by
NKCC2
Loop diuretics: Inhibition of Na+K+Cl- cotransport!
Increase !NaCl secretion!
K+ secretion!Ca2+ secretion!
Decrease!concentrated urine!
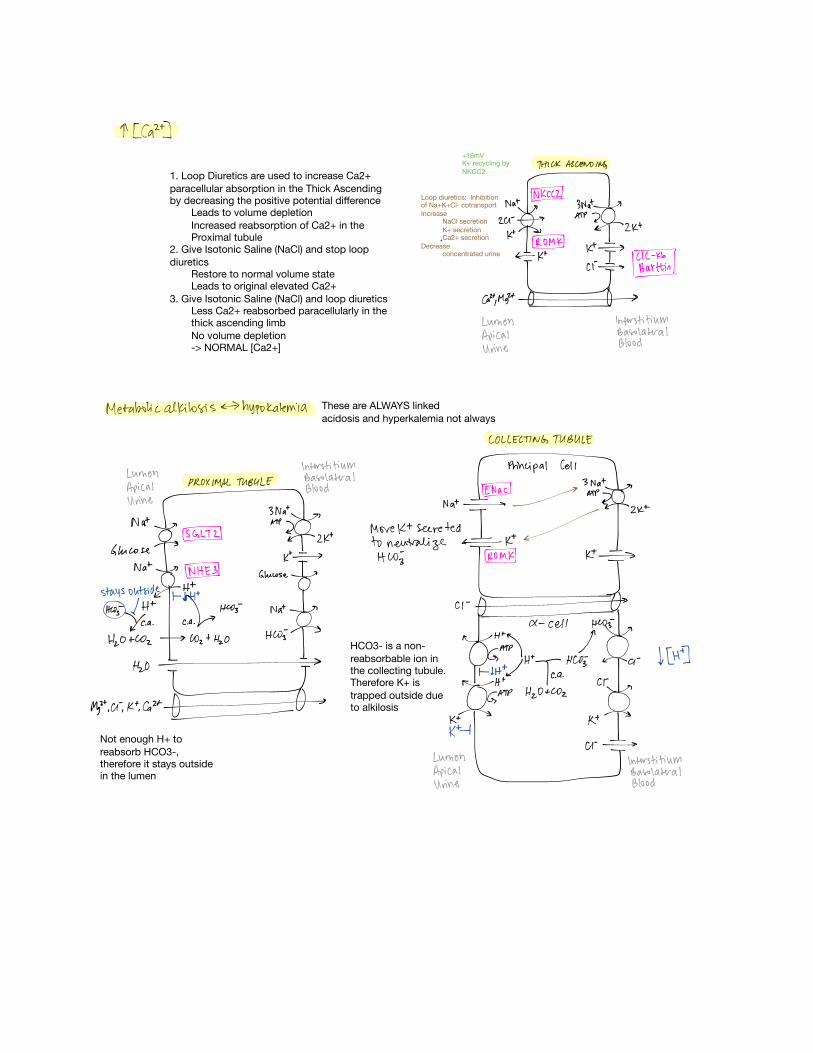
HCO3- is a non-
reabsorbable ion in the collecting tubule. Therefore K+ is
trapped outside due to alkilosis
Not enough H+ to
reabsorb HCO3-, therefore it stays outside in the lumen
1. Loop Diuretics are used to increase Ca2+
paracellular absorption in the Thick Ascending by decreasing the positive potential di"erence!
Leads to volume depletion!
Increased reabsorption of Ca2+ in the Proximal tubule!
2. Give Isotonic Saline (NaCl) and stop loop
diuretics!Restore to normal volume state!Leads to original elevated Ca2+ !
3. Give Isotonic Saline (NaCl) and loop diuretics!Less Ca2+ reabsorbed paracellularly in the thick ascending limb!
No volume depletion!-> NORMAL [Ca2+]
These are ALWAYS linked!
acidosis and hyperkalemia not always