Kelistrikan_Pembentukan Dan Pengaturan Irama
35
Pembentukan dan Pembentukan dan pengaturan pengaturan Irama Jantung Irama Jantung
-
Upload
wedha-jati-tyas -
Category
Documents
-
view
223 -
download
0
Transcript of Kelistrikan_Pembentukan Dan Pengaturan Irama
Pembentukan dan Pembentukan dan pengaturan Irama pengaturan Irama
JantungJantung
Propagation of Electrical Activity Propagation of Electrical Activity Through the HeartThrough the Heart
The Cardiac Action PotentialThe Cardiac Action Potential
Generation of the Cardiac PacemakerGeneration of the Cardiac Pacemaker
The ElectrocardiogramThe Electrocardiogram
Cardiac VectorsCardiac Vectors
Electrical Conductivity in the HeartElectrical Conductivity in the Heart
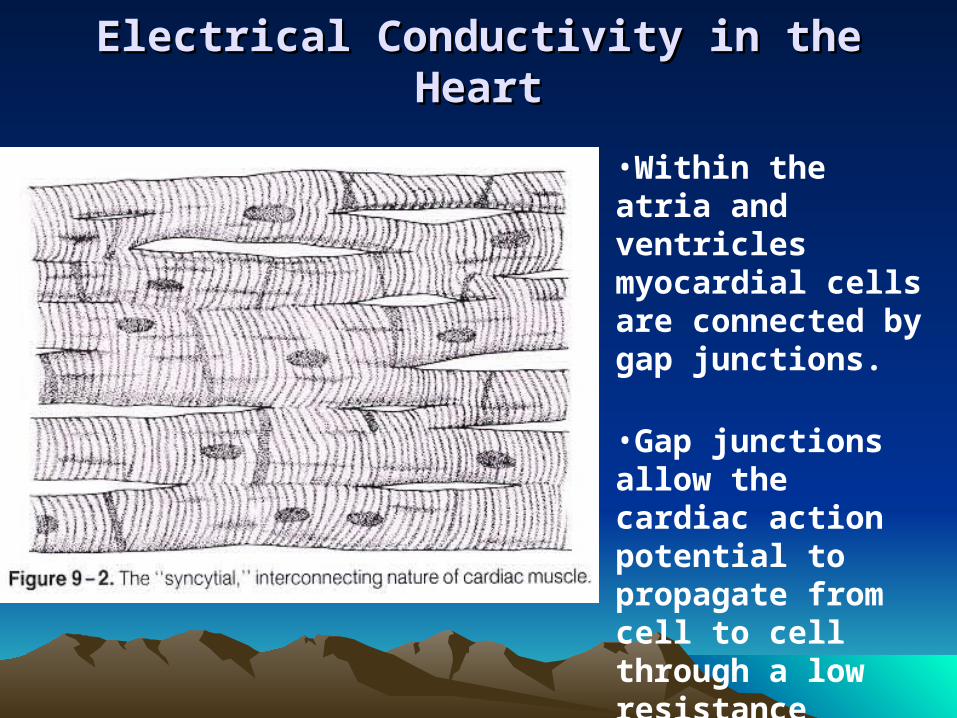
•Within the atria and ventricles myocardial cells are connected by gap junctions.
•Gap junctions allow the cardiac action potential to propagate from cell to cell through a low resistance pathway.
Electrical Conductivity in the HeartElectrical Conductivity in the Heart Electrical activity can pass from cell to cell in the atria
and ventricles.
The atria and ventricles are electrically isolated by the hearts fibrous skeleton the Annulus fibrosus.
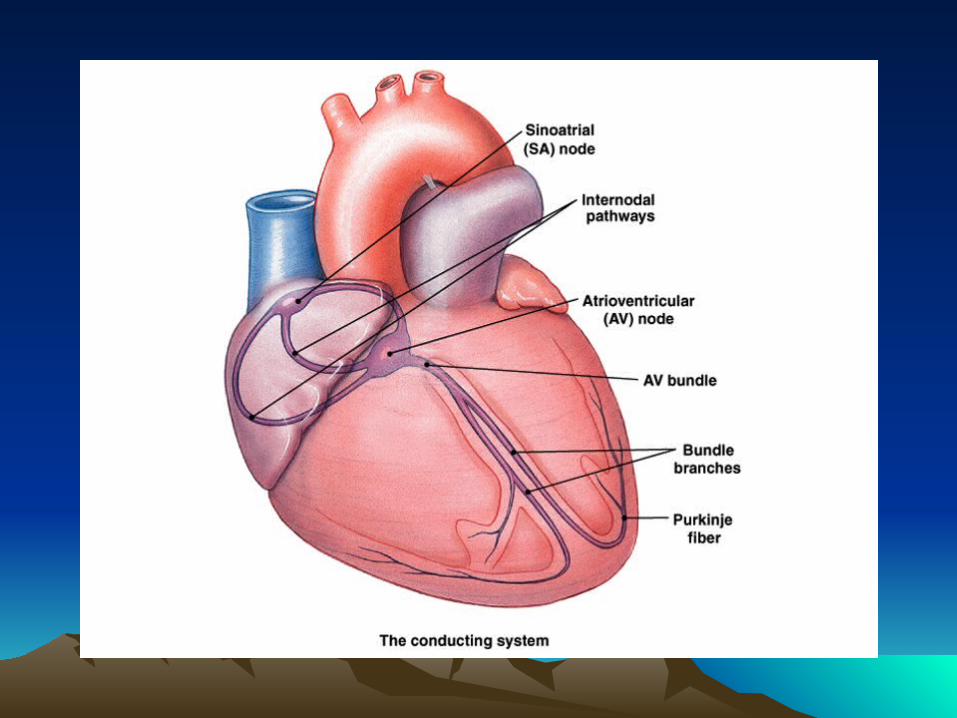
The heart has specialised electrically active cells in addition to contractile myocardium.
These cells form the Sinatorial (SA) node, Atrioventricular (AV) node, Bundle of His and Purkinje Fibres
Electrical activity normally originates in the SA node.
The AV node forms the only site of electrical connection between the atria and ventricles.
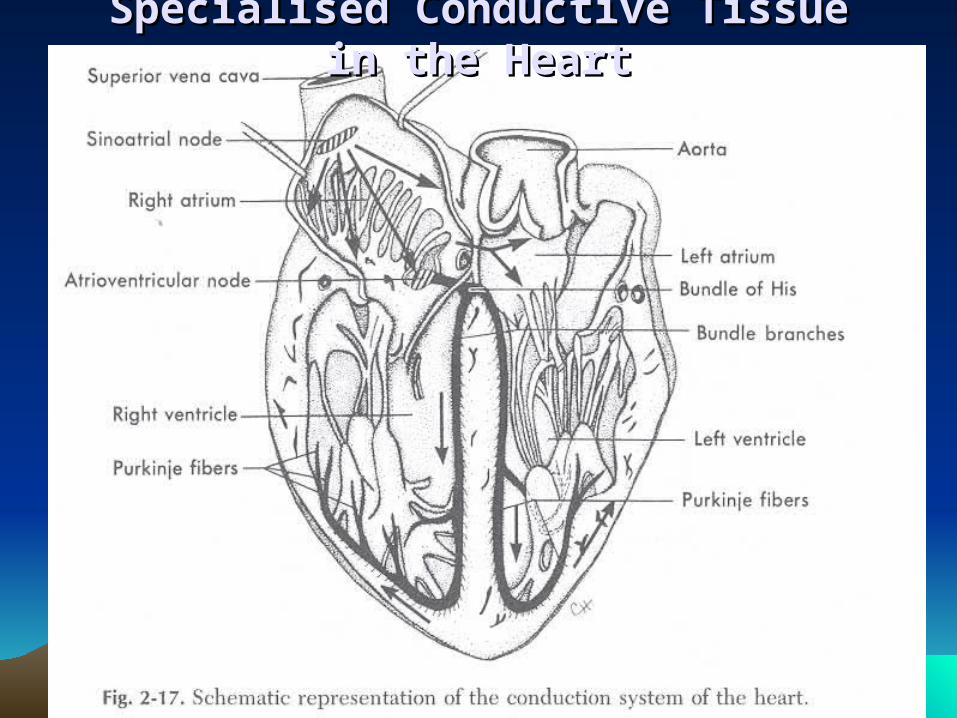
Specialised Conductive Tissue in the Specialised Conductive Tissue in the HeartHeart
AutorhythmicityAutorhythmicity
Some heart cells (SA, AV node and Purkinje) show automaticity, the ability to generate a heart beat.
These cells have an intrinsic rhythmicity which generates a pacemaker potential.
The heart does not require nerve or hormonal input to beat.
The heart transplant patents the nerves are severed but the heart beats on.
Propagation of the Cardiac Action Propagation of the Cardiac Action PotentialPotential
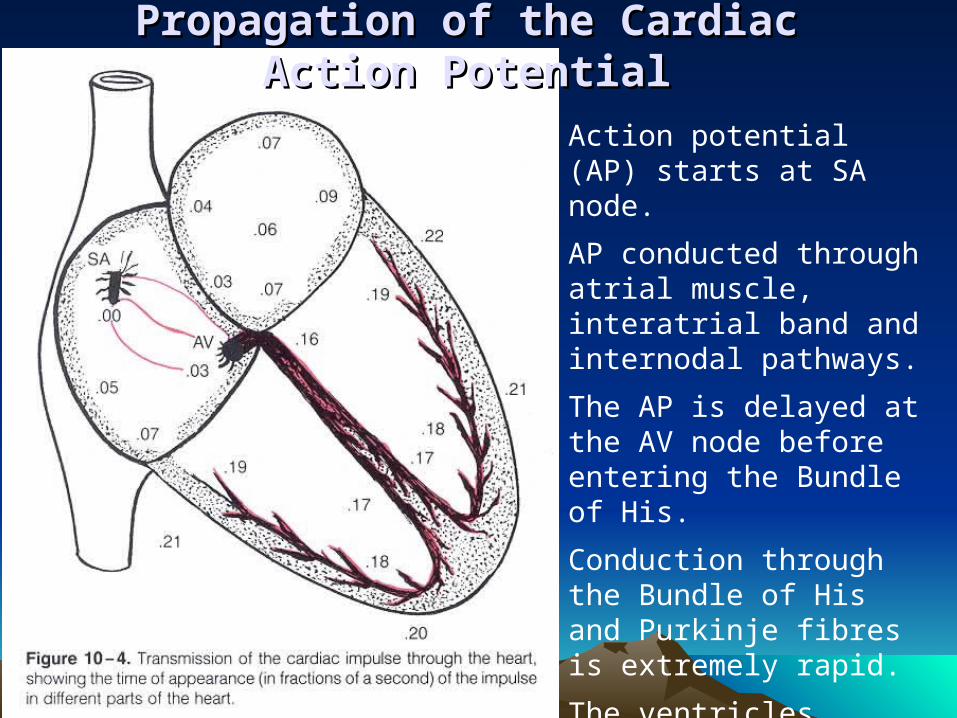
Action potential (AP) starts at SA node.
AP conducted through atrial muscle, interatrial band and internodal pathways.
The AP is delayed at the AV node before entering the Bundle of His.
Conduction through the Bundle of His and Purkinje fibres is extremely rapid.
The ventricles depolarise from endo to epicardium and from apex to base.
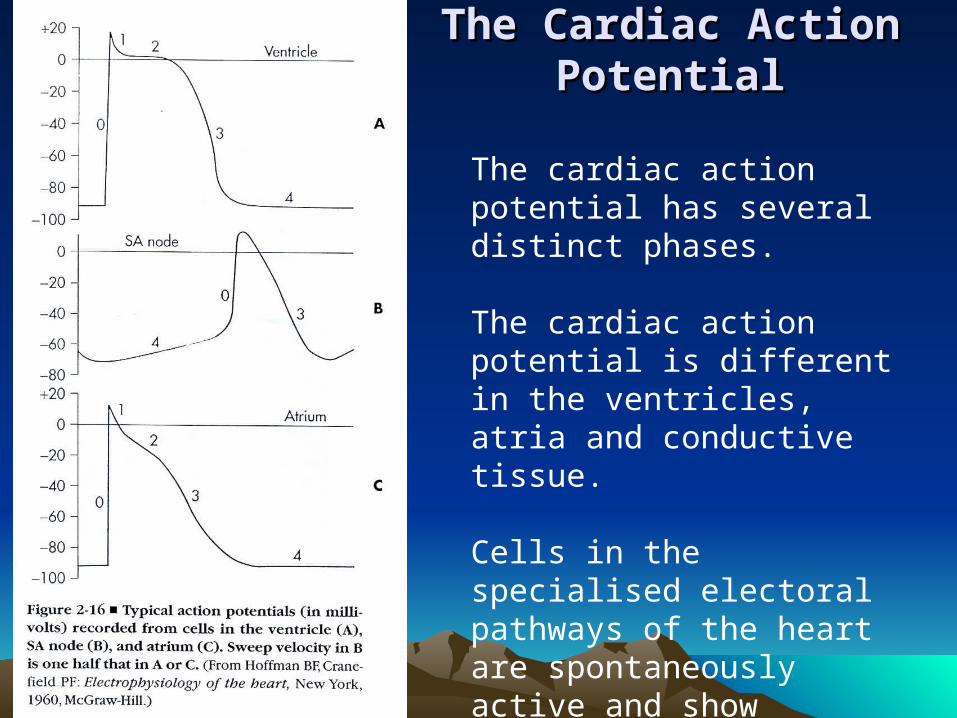
The Cardiac Action The Cardiac Action PotentialPotential
The cardiac action potential has several distinct phases.
The cardiac action potential is different in the ventricles, atria and conductive tissue.
Cells in the specialised electoral pathways of the heart are spontaneously active and show automaticity.
These cells do not have a true resting membrane potential.
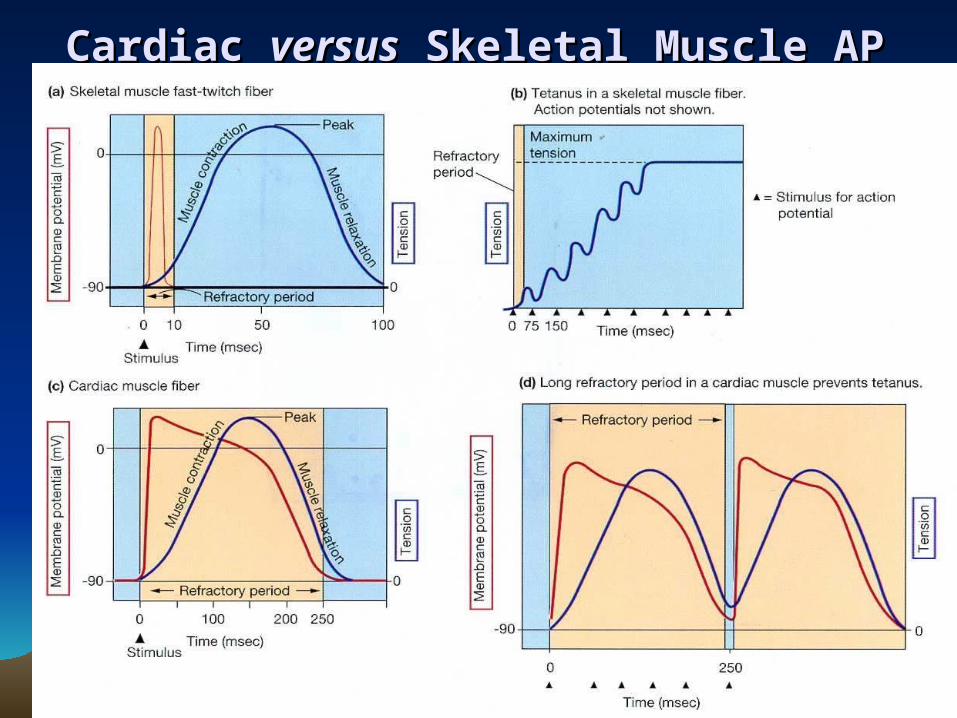
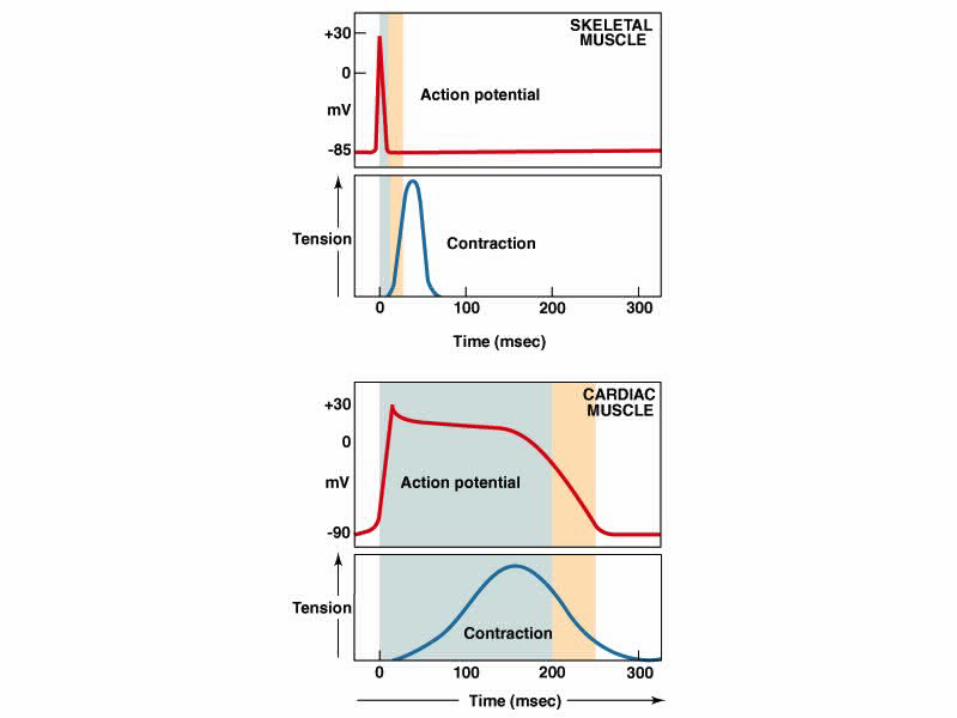
Cardiac Cardiac versusversus Skeletal Muscle AP Skeletal Muscle AP
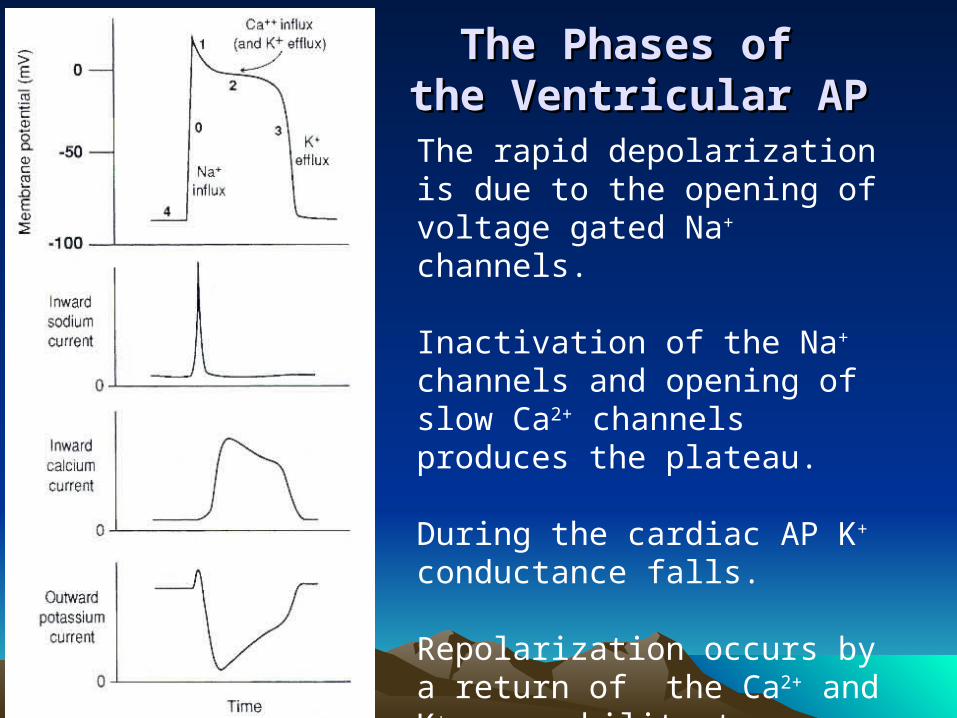
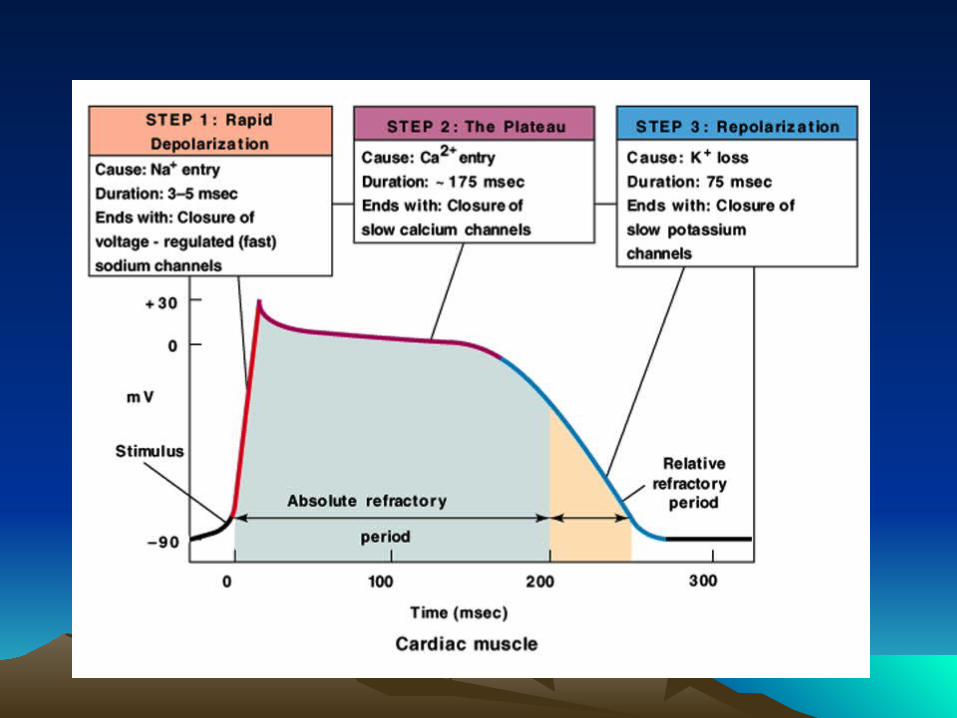
The rapid depolarization is due to the opening of voltage gated Na+ channels.
Inactivation of the Na+ channels and opening of slow Ca2+ channels produces the plateau.
During the cardiac AP K+ conductance falls.
Repolarization occurs by a return of the Ca2+ and K+ permeability to resting values.
The Phases of The Phases of the Ventricular APthe Ventricular AP
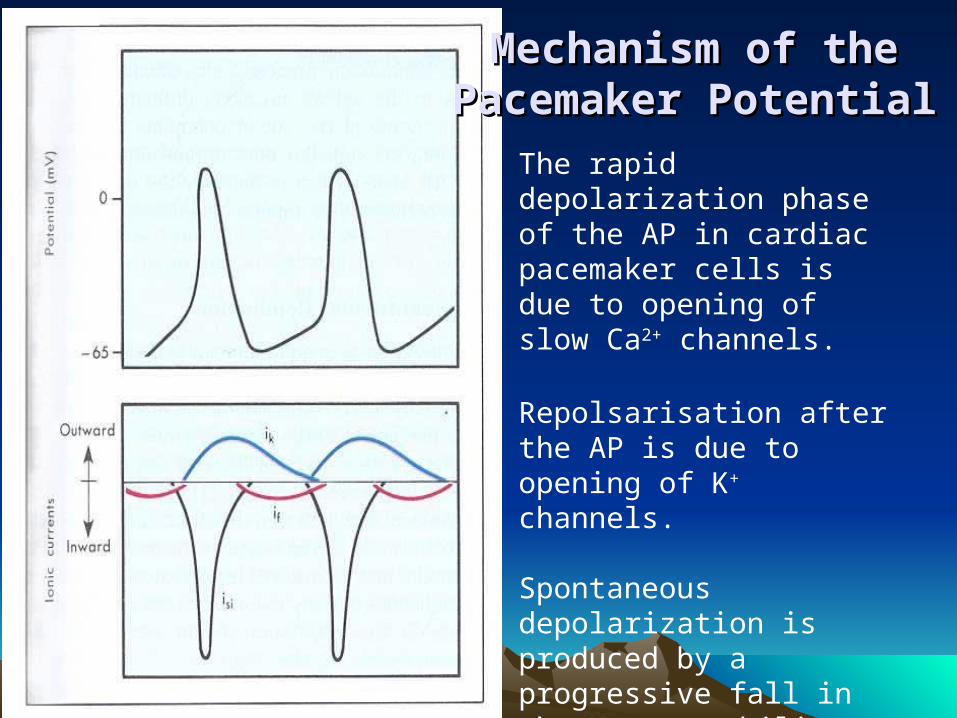
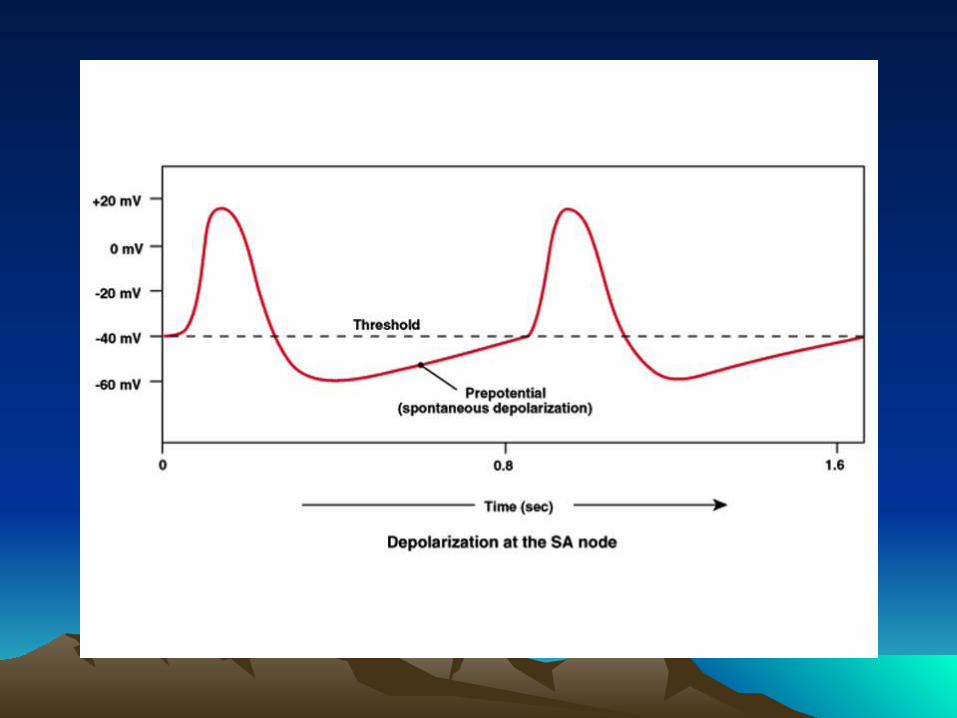
Mechanism of the Mechanism of the Pacemaker PotentialPacemaker Potential
The rapid depolarization phase of the AP in cardiac pacemaker cells is due to opening of slow Ca2+ channels.
Repolsarisation after the AP is due to opening of K+ channels.
Spontaneous depolarization is produced by a progressive fall in the K+ permeability combined with an inward current if (the nature of if is still under investigation).
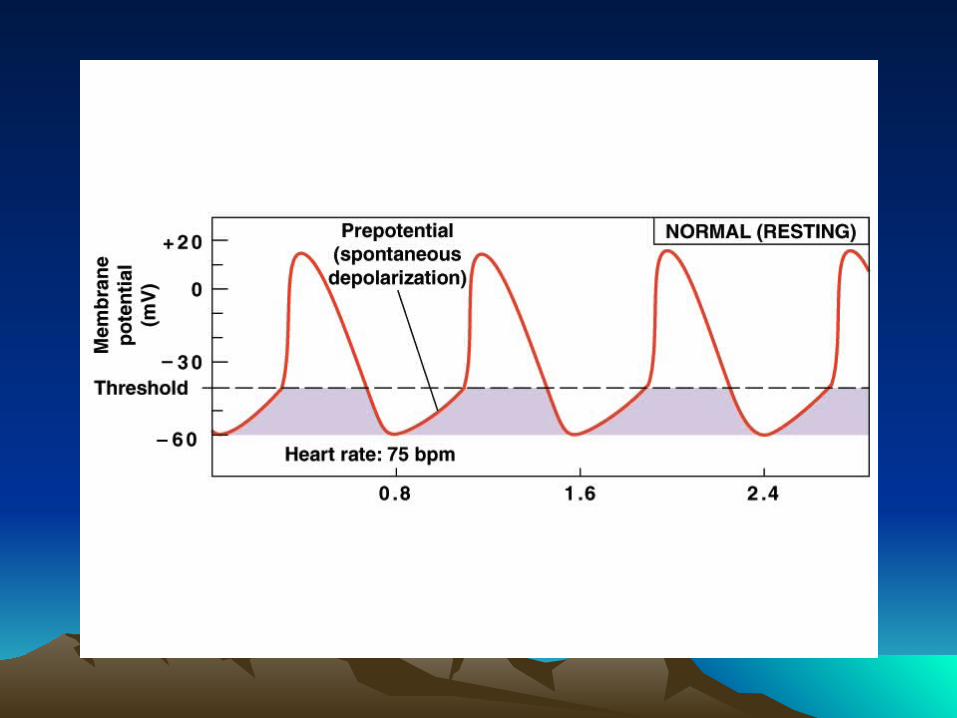
Cardiac PacemakersCardiac Pacemakers The sinoatrial has the fastest pacemaker potential (~90-
100 beats/min) and is the normal pacemaker
The atrioventricular node is the next fastest (~40-60 beats/min) followed by cells in the bundle of His (15-30).
The fastest pacemaker normally drives the heart and suppresses other pasemakers (overdrive suppression).
A beat generated outside the normal pacemaker is an ectopic beat.
The site that generates an ectopic beat is known as an ectopic focus (foci pl.) or ectopic pacemaker.
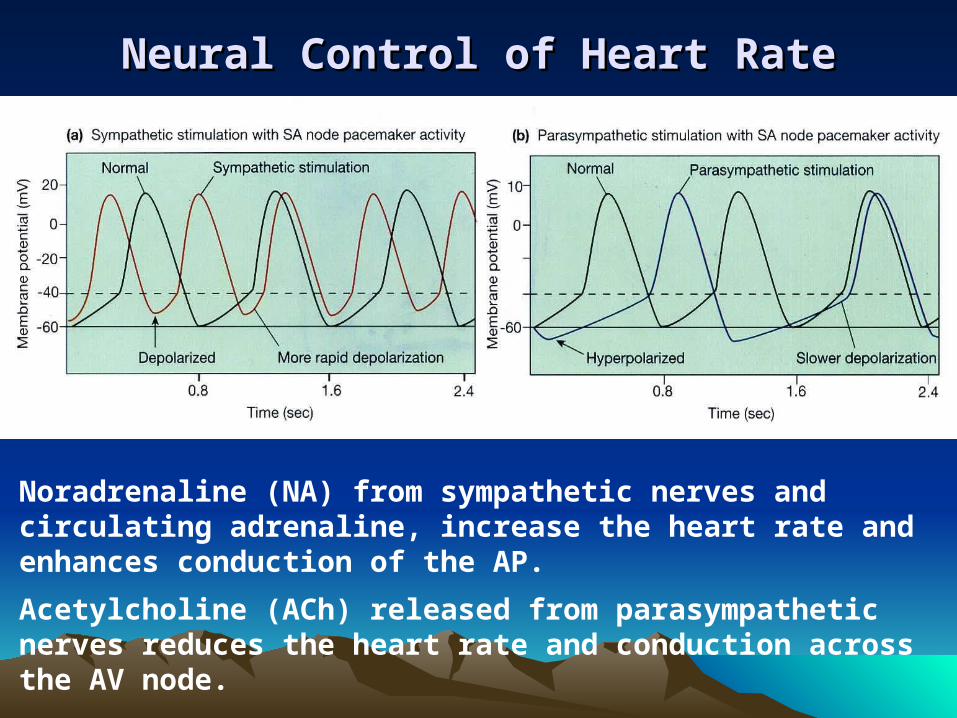
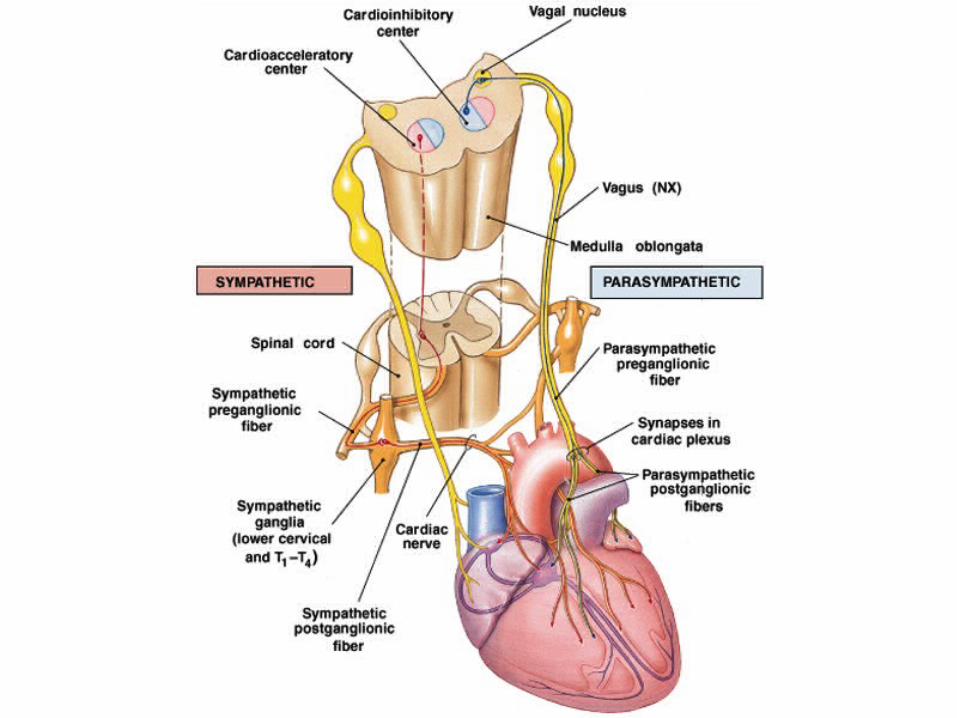
Neural Control of Heart RateNeural Control of Heart Rate
Noradrenaline (NA) from sympathetic nerves and circulating adrenaline, increase the heart rate and enhances conduction of the AP. Acetylcholine (ACh) released from parasympathetic nerves reduces the heart rate and conduction across the AV node.
Neural Control of Heart RateNeural Control of Heart Rate Agents that alter heart rate are chronotropic. Positive chronotropic argents increase heart rate.
Adrenaline and NA act on-adrenergic receptors on the heart.
Isoprenaline (isoproterenol) is -adrenergic agonist which increases heart rate.
Propranolol is a -adrenergic antagonist that blocks the actions of adrenaline, NA and isoprenaline.
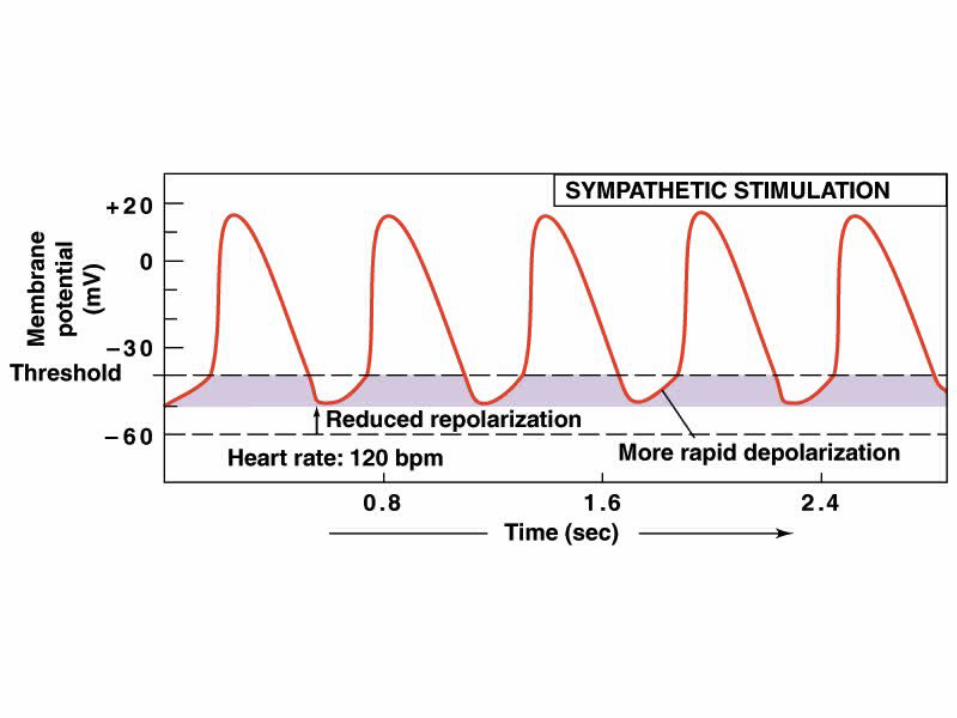
Adrenergic stimulation increases the Na+ and Ca2+ permeability of cardiac cells, hypopolarising them and increasing the pacemaker potential rise.
At rest the heart is under week sympathetic tone.
Neural Control of Heart RateNeural Control of Heart Rate Agents with negative chronotropic actions slow the heart.
Acetylcholine acts on M-cholinergic (muscarinic) receptors on the heart.
Methacholine, carbachol (carbamylcholine) and muscarin are pharmacological stimulants of muscarinic receptors.
Atropine is a muscarinic antagonist that blocks the actions of ACh and other muscarinic receptor agonists
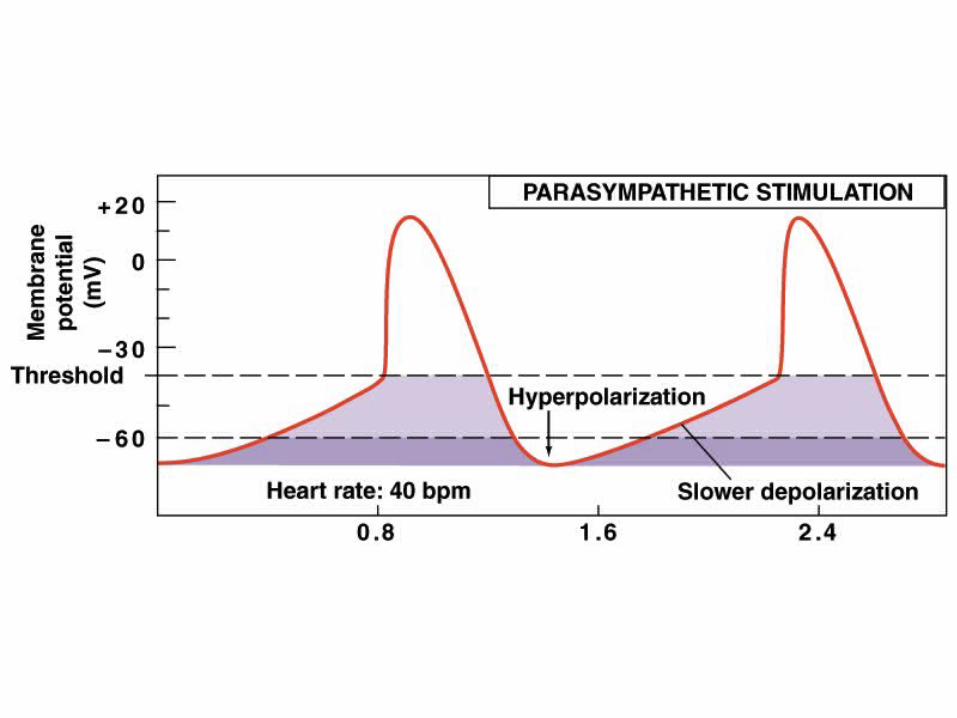
ACh increases K+ permeability of cardiac cell hyperpolarising them and reducing the rise in the pacemaker potential
At rest the heart is under parasympathetic tone which slows the natural rhythm of the heart.
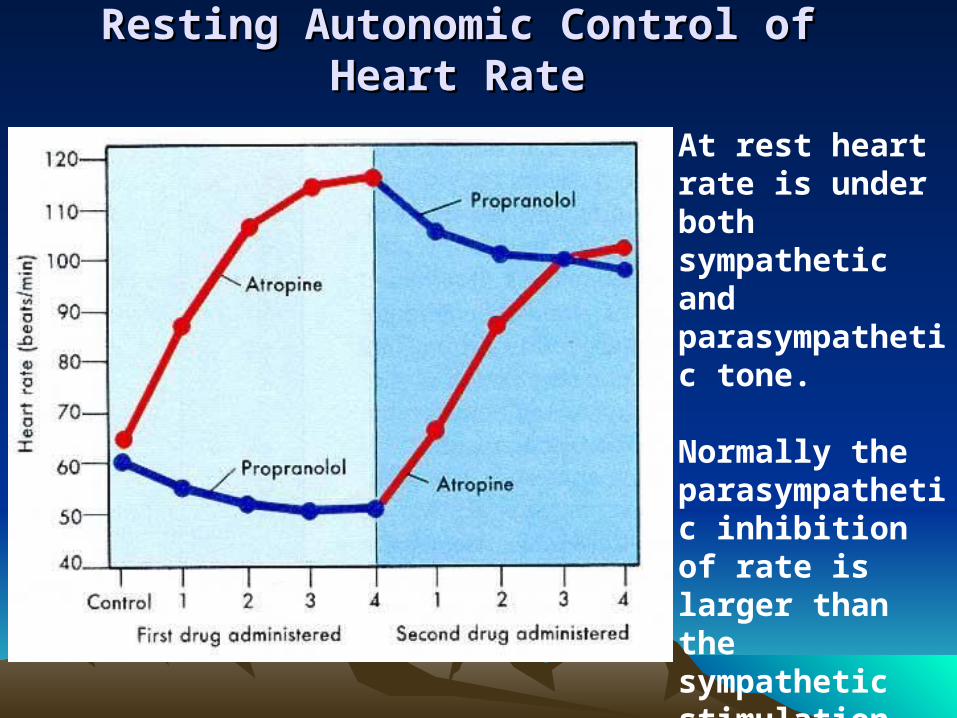
Resting Autonomic Control of Heart RateResting Autonomic Control of Heart Rate
At rest heart rate is under both sympathetic and parasympathetic tone.
Normally the parasympathetic inhibition of rate is larger than the sympathetic stimulation.
Some Other Agents.Some Other Agents. Nifedipine and Verapamil are calcium channel blocking
agents that reduce heart rate.
Increased extracellular K+ (hyperkalaemia): hypopolarises cardiac myocytes, shortens the AP and slows the heart. Arrhythmia or heart block is often produced with fibrillation at higher levels. Only a 5-10mM rise in extracellular K+ can cause death.
Excessive extracellular Ca2+ (hypercalcaemia) can produce spastic contractions of the heart.
Reduced Ca2+ (hypocalcaemia) concentrations inhibit heart contraction and can trigger ectopic foci.
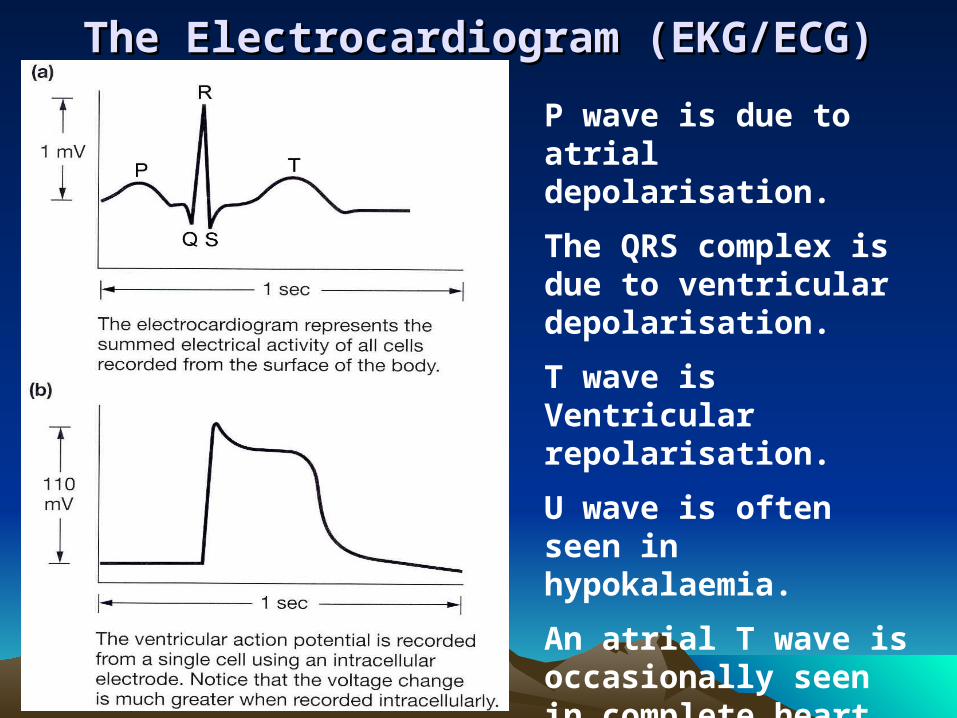
The Electrocardiogram (EKG/ECG)The Electrocardiogram (EKG/ECG)P wave is due to atrial depolarisation.
The QRS complex is due to ventricular depolarisation.
T wave is Ventricular repolarisation.
U wave is often seen in hypokalaemia.
An atrial T wave is occasionally seen in complete heart block
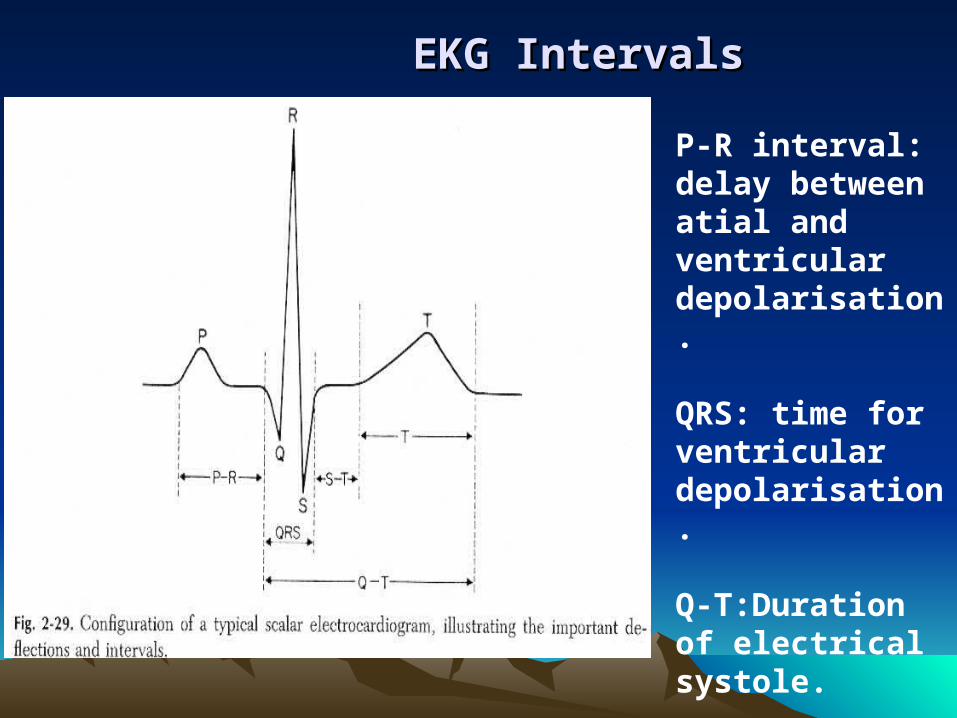
EKG IntervalsEKG Intervals
P-R interval: delay between atial and ventricular depolarisation.
QRS: time for ventricular depolarisation.
Q-T:Duration of electrical systole.
Normal EKG IntervalsNormal EKG Intervals
P-R interval is normally 0.12-0.20 sec, most of this time is delay at the AV node. An increased P-R interval (>0.28 sec) is characteristic of 1st degree heart block.
QRS complex normally lasts less than 0.10 sec. Increased width of the complex is a characteristic of defects in the branch bundles or Purkinje fibres i.e. branch bundle block.
Q-T interval varies inversely with heart rate.
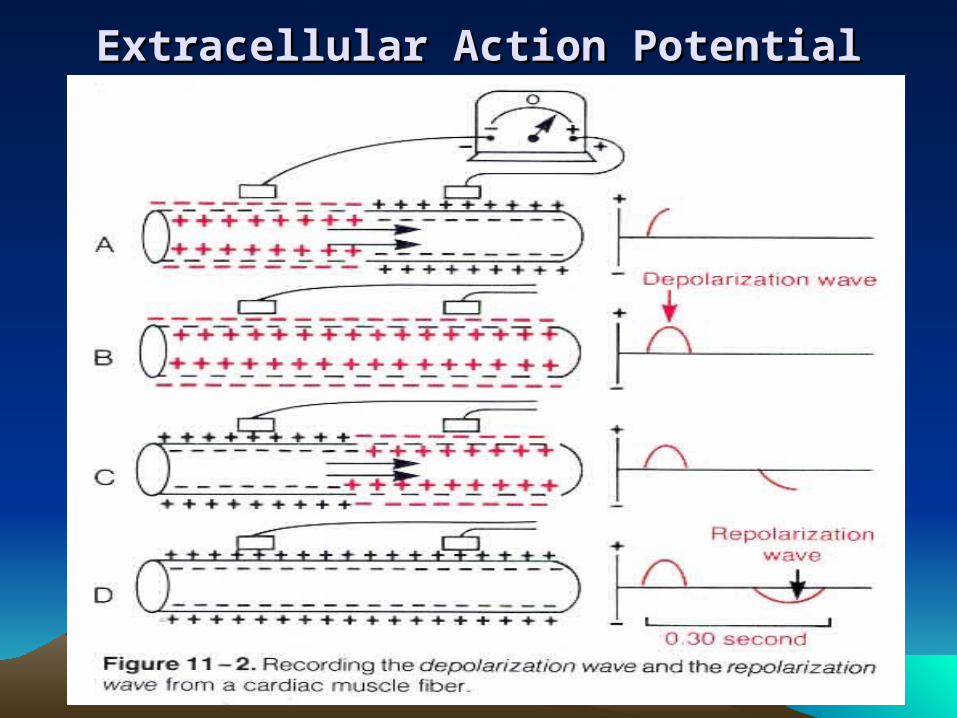
Extracellular Action PotentialExtracellular Action Potential
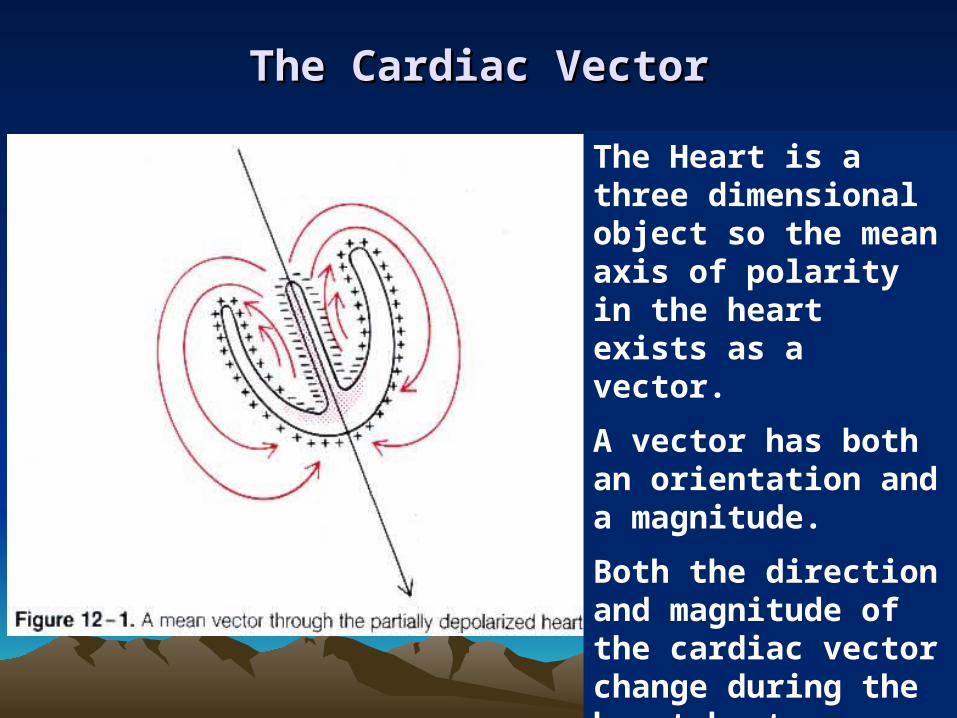
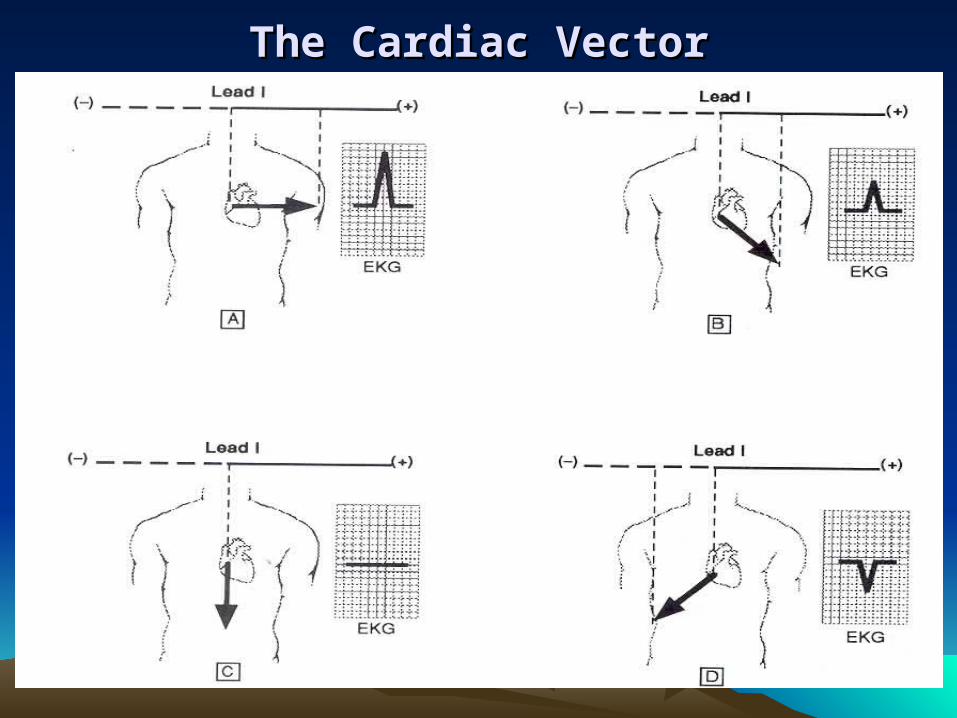
The Cardiac VectorThe Cardiac Vector
The Heart is a three dimensional object so the mean axis of polarity in the heart exists as a vector.
A vector has both an orientation and a magnitude.
Both the direction and magnitude of the cardiac vector change during the heart beat.
The Cardiac VectorThe Cardiac Vector
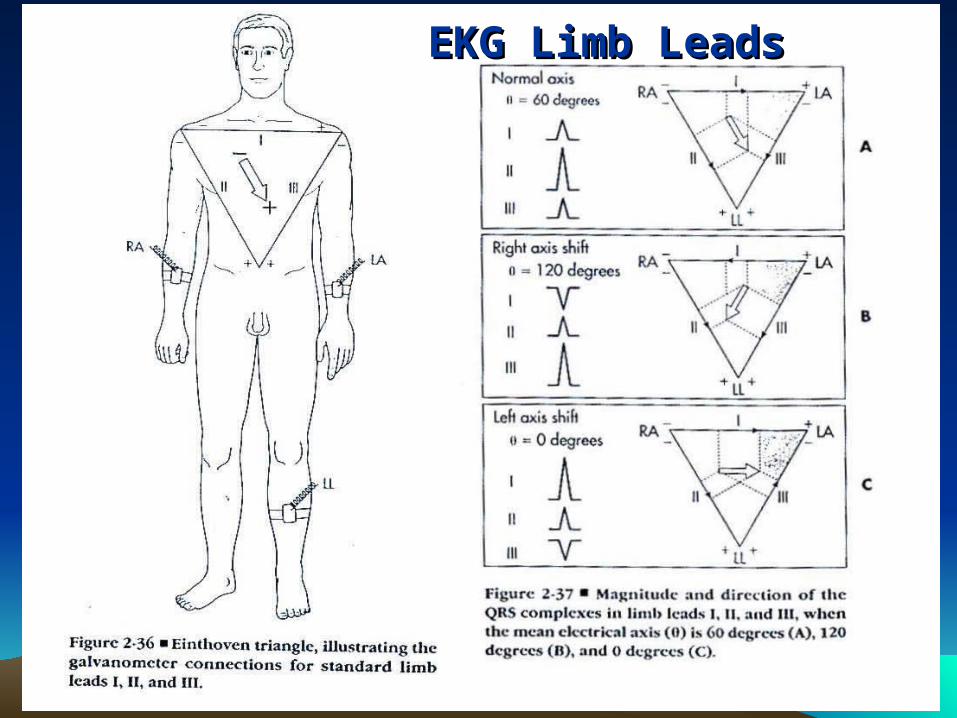
EKG Limb LeadsEKG Limb Leads
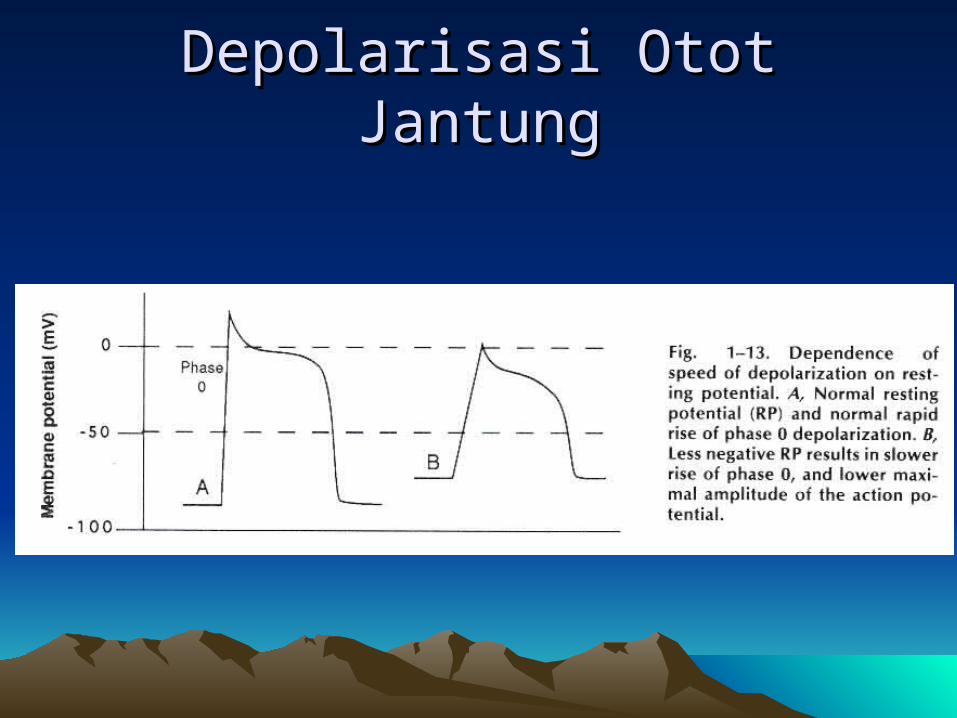
Depolarisasi Otot JantungDepolarisasi Otot Jantung
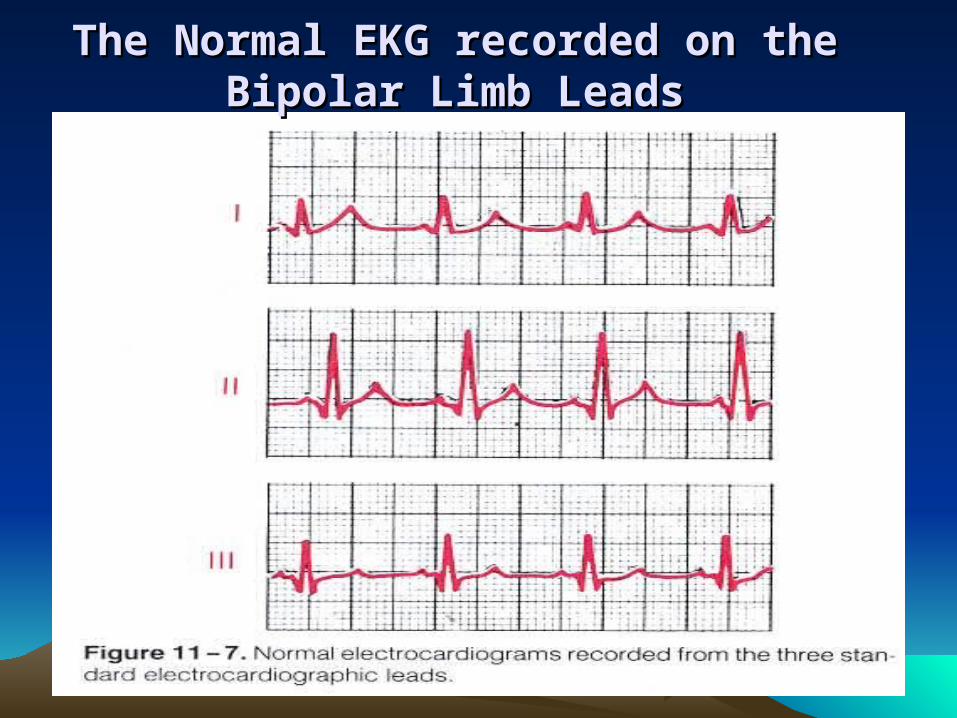
The Normal EKG recorded on the Bipolar The Normal EKG recorded on the Bipolar Limb LeadsLimb Leads
Uses of the EKGUses of the EKG
Heart RateConduction in the heartArrythmias Direction of the cardiac vectorDamage to the heart muscle
Provides NO information about pumping or mechanical events in the heart.