
Kathy D. Miller, MD Associate Professor and Sheila D. Ward Scholar Indiana University Melvin and...
68
Kathy D. Miller, MD Associate Professor and Sheila D. Ward Scholar Indiana University Melvin and Bren Simon Cancer Center Indianapolis, IN Advances in Targeted Therapies for Breast Cancer A Report From SABCS 2009 Clinical Updates
-
Upload
stewart-fields -
Category
Documents
-
view
216 -
download
1
Transcript of Kathy D. Miller, MD Associate Professor and Sheila D. Ward Scholar Indiana University Melvin and...
Kathy D. Miller, MDAssociate Professor and Sheila D. Ward Scholar
Indiana University Melvin and Bren Simon Cancer CenterIndianapolis, IN
Advances in Targeted Therapies for Breast Cancer
A Report From SABCS 2009
Clinical Updates

Discussion Topics
• HER2 positive disease
– Growing number of options
• Angiogenesis
– Bevacizumab questions answered and rephrased
– Small molecule success and disappointment

HER2: What We Knew Before SABCS
• Trastuzumab
– Active as single agent and adds to chemo/HRT
– Effective with chemo beyond PD
– Adds to lapatinib monotherapy (ORR, PFS)
• Lapatinib
– Active as single agent and adds to chemo/HRT
– Effective with chemo after PD on trastuzumab
• MULTIPLE new agents in development

Case 1
• 54 year old woman with newly diagnosed stage II breast cancer s/p lumpectomy and axillary dissection
– Primary tumor 1.9 cm
– Involves 1 of 14 LN (1/2 SN, 0/12 additional LN)
– Grade III
– ER+ 15%, PR-
– HER2 2+ by IHC (intense staining in 20% of cells)
– FISH equivocal with ratio 2.15
• Do you recommend adjuvant trastuzumab?

Background
• In 2007, ASCO/CAP recommended new guidelines to define HER2 positivity by both IHC 3+* and FISH+**
– 3+ IHC: Uniform intense membrane staining of > 30% of invasive tumor cells
– FISH+: HER2/CEP17 ratio > 2.2
• Original HER2 eligibility criteria in the pivotal N9831 Phase III Adjuvant HER2 Trial
– 3+ IHC: Uniform intense membrane staining of > 10% of invasive tumor cells
– FISH+: HER2/CEP 17 ratio ≥ 2.0
HerceptTest DAKO, Carpenteria, CA; FISH: PathVysion, Abbott Molecular; Masood S et al. Ann Clin Lab Sci 1998;28(4):215-223;
Perez EA et al. SABCS 2009 #701
HerceptTest DAKO, Carpenteria, CA; FISH: PathVysion, Abbott Molecular; Masood S et al. Ann Clin Lab Sci 1998;28(4):215-223;
Perez EA et al. SABCS 2009 #701

N9831 DFS Based on Original Criteria: HER2 Non-positive* vs. HER2+**
* HER2 Non-positive (IHC ≤ 10 and FISH Ratio < 2.0) ** HER2+ (IHC > 10 or FISH Ratio ≥ 2.0)* HER2 Non-positive (IHC ≤ 10 and FISH Ratio < 2.0) ** HER2+ (IHC > 10 or FISH Ratio ≥ 2.0) Perez EA et al. SABCS 2009 #701 Perez EA et al. SABCS 2009 #701

N9831 DFS Based on 2007 ASCO/CAP: HER2 Non-positive* vs. HER2+**
* HER2 Non-positive (IHC ≤ 30 and FISH Ratio ≤ 2.2)** HER2+ (IHC >30 or FISH Ratio > 2.2)
* HER2 Non-positive (IHC ≤ 30 and FISH Ratio ≤ 2.2)** HER2+ (IHC >30 or FISH Ratio > 2.2)
Perez EA et al. SABCS 2009 #701 Perez EA et al. SABCS 2009 #701

Conclusions
• A small percentage (by IHC:3.7%, FISH 1.4%, both:1.7%) of N9831 pts did not meet ASCO/CAP 2007 HER2 positivity guidelines when applied retrospectively
• Trastuzumab effect appeared similar for HER2+ pts regardless of ASCO/CAP or originally used FDA-approved guidelines
• Data support determining eligibility for trastuzumab based on the original definition of HER2 positivity (IHC 3+, >10% staining; FISH ratio>2.0).
Perez EA et al. SABCS 2009 #701 Perez EA et al. SABCS 2009 #701

Case 1
• 54 year old woman with newly diagnosed stage II breast cancer s/p lumpectomy and axillary dissection
– Primary tumor 1.9 cm
– Involves 1 of 14 LN (1/2 SN, 0/12 additional LN)
– Grade III
– ER+ 15%, PR-
– HER2 2+ by IHC (intense staining in 20% of cells)
– FISH equivocal with ratio 2.15
• Do you recommend adjuvant trastuzumab?
– YES

Adjuvant Trastuzumab
1 v 2 years
IHC, immunohistochemistry;FISH, fluorescence in situ hybridisation
AC P D DCarbo Standard
HERA
IHC orFISH
Observation
Trastuzumab 1 year
NCCTG N9831 BCIRG 006
FISH
NSABP B-31
IHC orFISH
IHC orFISH

BCIRG 006 DFS Events
First / Second / Third Planned Efficacy Analyses (cutoff dates: 30June2005 / 01Nov2006 / 16Oct2009)
• Median follow-up time = 23/36/65 months
• 322/462/656 DFS events (42% additional events)
– Breast cancer relapse
– Second primary malignancy
– Death
• 84/185/348 deaths (88% additional deaths)
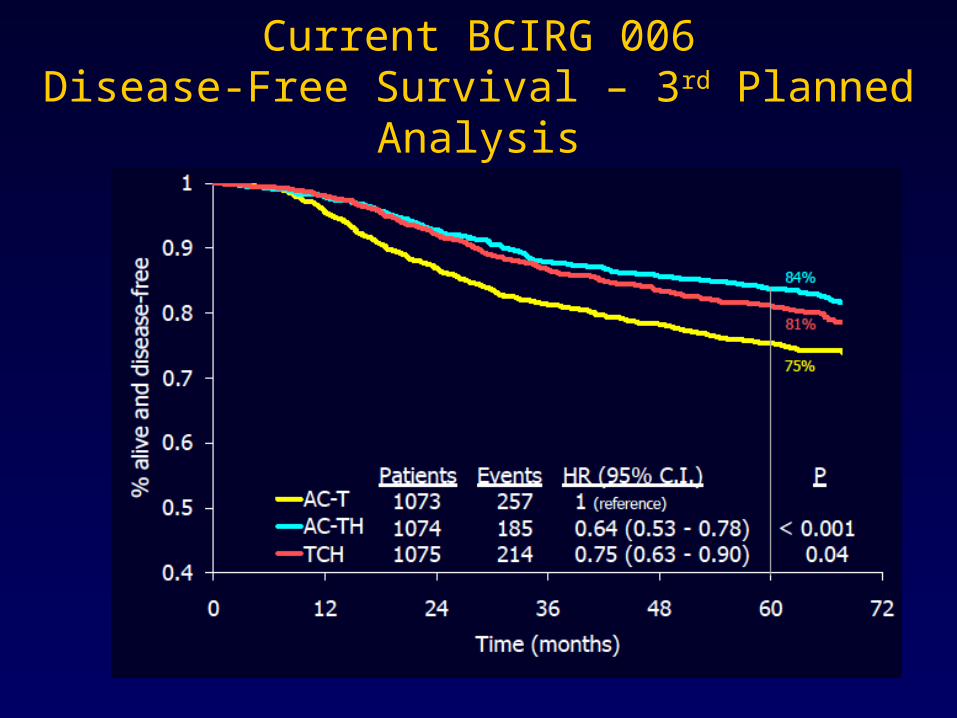
Current BCIRG 006Disease-Free Survival – 3rd Planned Analysis

Current BCIRG 006Overall Survival – 3rd Planned Analysis

Cardiac Deaths and CHF as per Independent Review Panel

Therapeutic Index – Most Recent Data

Efficacy Analysis
*Patients eligible for crossover censored
Data frozen on 11/3/2009
AC → TAC → T AC → T → HAC → T → H
vsControl (A)* Sequential (B)*
Perez EA et al, SABCS 2009

Perez EA et al, SABCS 2009
Alive anddisease free (%)
Years from randomization
No. at riskNo. at risk735735
728728675675
643643624624
581581586586
529529513513
447447
85.2%85.2%
79.7%79.7%
80.1%80.1%
71.9%71.9%
40
50
60
70
80
90
100
0 1 2 3 4 5
AC → T(222 events)
AC → T → H(164 events)
Log rank P=0.0005Log rank P=0.0005
10971097
10871087
Control vs Sequential

Efficacy Analysis
*Censoring based on temp closure of C,and eligibility for crossover
Data frozen on 11/3/2009
AC → T+H → HAC → T+H → HAC → T → HAC → T → H
vs Concurrent (C)Sequential (B)*
N9831
Perez EA et al, SABCS 2009

Sequential vs Concurrent 1st Interim Analysis
• At 50% of planned number of events (312 events)
– 1,903 pts, median follow-up: 5.3 yr
– 75% of pts followed for 5 yr
• DFS may differ with respect to the timing of trastuzumab’s addition to AC → T
– Log rank P=0.019 (HR 0.77; 95% CI 0.61-0.96)
• Not crossing the boundary for statistical significance, pre-set at 0.00116
Perez EA et al, SABCS 2009

Alive anddisease free (%)
837837830830
788788766766
740740705705
676676641641
456456418418
No. at riskNo. at risk
89.1%89.1%
85.7%85.7%
84.2%84.2%
79.8%79.8%
40
50
60
70
80
90
100
0 1 2 3 4 5Years from randomization
AC → T → H(174 events)
AC →T+ H → H(138 events)
Logrank p=0.0190Logrank p=0.0190
949949954954
Perez EA et al, SABCS 2009
Sequential vs Concurrent

Perez EA et al, SABCS 2009
Conclusions
• DFS is significantly improved with the additionof 52 wks of trastuzumab to AC T
• There is a statistically significant 33% reduction in the risk of an event with the sequential addition of trastuzumab following AC T
– 5 yr DFS: 72% vs. 80%
• There is a strong trend for a 25% reductionin the risk of an event with starting trastuzumab concurrently with taxane relative to sequentially
– 5 yr DFS: 80% vs. 84%

Piccart-Gebhart et al 2005; Romond et al 2005;Slamon et al 2005;Joensuu et al 2005
0 1 2
HERA 1 year
Combined analysis 2 years
Median follow-up
FavorsTrastuzumab
Favors noTrastuzumab
HR
BCIRG 006 DCarboH 2 years
2 yearsBCIRG 006 AC DH
FinHER VH / DH CEF 3 years
Trastuzumab DFS

Adjuvant Trastuzumab
• Test everyone for HER2, inquire about testing quality and look carefully at ‘equivocal’ results
– Most important message -> Give Trastuzumab!
– Either TCH or AC>TH supported by data
– Differences between regimens modest
• Slightly more recurrence with TCH balanced by increased cardiac and long-term marrow toxicity with AC>TH
• Give concurrently with chemo unless there is a compelling reason not to

Case 2
• 74 year old presents with 5 cm primary breast mass with associated axillary adenopathy.
– ER-, PR-, HER2 3+ by IHC (FISH ratio 8.9)
– Staging finds several liver lesions, largest 2.2 cm
• Biopsy of liver lesion confirms MBC, HER2+
• LFTs normal
• LVEF 62%
• She refuses chemotherapy but will consider other options, family supports her wishes
• What would you recommend?

TrastuzumabLapatinib
Pathway ActivationHER Ligands

Heavily pretreated patients with HER2-positive
MBC and progression on trastuzumab
(N = 296)
Stratified by visceral disease and hormone receptor status
Lapatinib 1500 mg PO QD(n = 148)
Lapatinib 1000 mg PO QD + Trastuzumab 4 mg/kg loading
dose, then 2 mg/kg IV wkly(n = 148)
Optional crossover to trastuzumab arm
if PD after 4 wks (n = 77)
PO, orally; QD, once daily.
Primary endpoint:PFS
Secondary endpoints:OSORRCBR
EGF104900
Blackwell K, et al. SABCS 2009 # 61.
Lapatinib + Trastuzumab

52% of patients crossed over from single-agent lapatinib to combination therapy on progression.
Lapatinib + Trastuzumab
Blackwell K, et al. SABCS 2009 # 61.
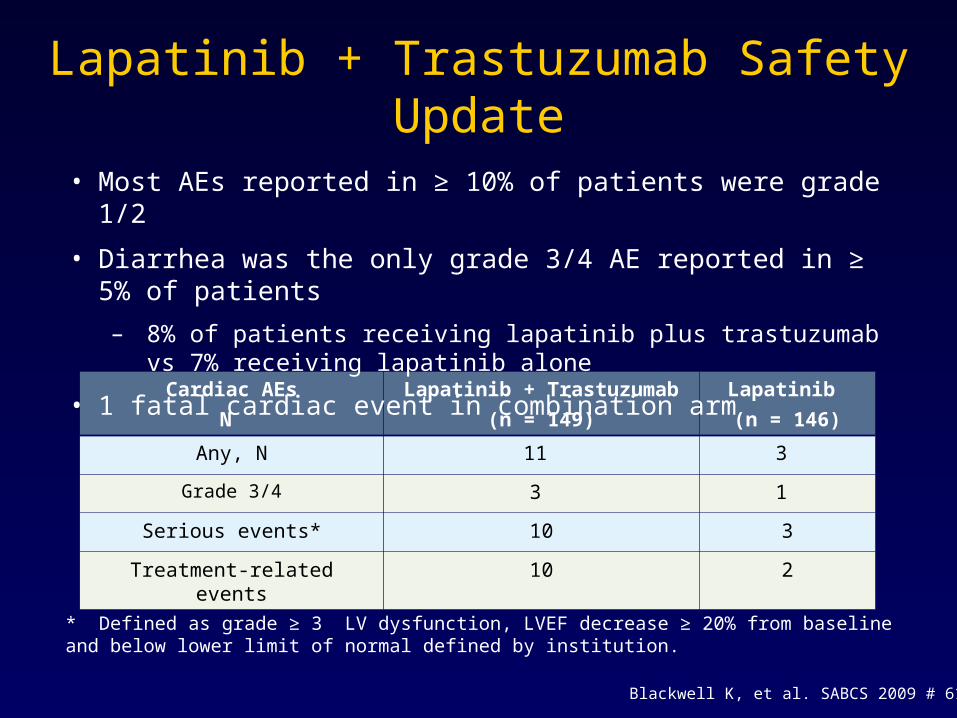
Cardiac AEs
N
Lapatinib + Trastuzumab
(n = 149)
Lapatinib
(n = 146)
Any, N 11 3
Grade 3/4 3 1
Serious events* 10 3
Treatment-related events 10 2
* Defined as grade ≥ 3 LV dysfunction, LVEF decrease ≥ 20% from baseline and below lower limit of normal defined by institution.
Lapatinib + Trastuzumab Safety Update
• Most AEs reported in ≥ 10% of patients were grade 1/2
• Diarrhea was the only grade 3/4 AE reported in ≥ 5% of patients
– 8% of patients receiving lapatinib plus trastuzumab vs 7% receiving lapatinib alone
• 1 fatal cardiac event in combination arm
Blackwell K, et al. SABCS 2009 # 61.

Blackwell K, et al. SABCS 2009 # 61.
• Lapatinib + trastuzumab associated with 26% improvement in OS vs lapatinib alone
– Significant survival benefit despite 52% crossover
– Supports combination arm of ALTTO
• Lapatinib plus trastuzumab well tolerated
– AEs comparable to lapatinib alone
• Offers possible options for heavily pretreated patients who progress on trastuzumab
Lapatinib + Trastuzumab

Austin CD et al. Mol Biol Cell. 2004;15:5268-5282.
T-DM1
• T-DM1, an antibody-drug conjugate, combines biologic effect of trastuzumab against HER2-expressing cells with highly potent antimicrotubule agent DM1
– MOA likely involves receptor-mediated internalization of T-DM1 after binding to HER2, resulting in intracellular release of DM1

T-DM1 Monotherapy
• Multicenter, single arm (N=110)
• Primary endpoint – ORR by IRF at 24 weeks
• Eligibility
– Prior anthracycline, taxane, capecitabine, trastuzumab, lapatinib
– Active disease progression on last therapy
– LVEF 50% or better
Krop I, et al. SABCS 2009.#5090.

Krop I, et al. SABCS 2009 #5090.
• ORR (by independent review) 32.7%
• Clinical benefit rate (by independent review) 44.5%
• Median PFS 7.3 months
• T-DM1 well tolerated
– Thrombocytopenia
• Offers a very real option for additional therapy for HER2+ patients
T-DM1 Monotherapy

Response Rates for Novel HER2-Targeting Agents After Progression on Trastuzumab
Modi et al, ASCO 2008; Gelmon et al, ASCO 2008; Swaby et al, ASCO 2009; Burris et al, ESMO 2009.
P<0.0001

Topics
• HER2 positive disease
– Growing number of options
• Angiogenesis
– Bevacizumab questions answered and rephrased
– Small molecule success and disappointment
Angiogenesis
• Angiogenesis is important for tumor growth
• Highly regulated, multiple redundant pathways
– VEGF among the most potent and frequently overexpressed
• Bevacizumab
– Modest activity as monotherapy
– Disappointing results in initial randomized trial
– E2100, then AVADO and RIBBON-1
• Now RIBBON-2

Stratify:• DFI < 24 mos. vs. > 24 mos.
• < 3 vs. > 3 metastatic sites
• Adjuvant chemotherapy: yes vs. no
• ER+ vs. ER- vs. ER unknown
RANDOMIZE
Paclitaxel +
Bevacizumab28-day cycle:• Paclitaxel 90 mg/m2 D1, 8 and 15• Bevacizumab 10 mg/kg D1 and 15
Paclitaxel
Miller K, et al. N Engl J Med. 2007;357:2666-2676
E2100

AVADO
• Primary endpoint: progression-free survival
• Secondary endpoints: overall response rate, duration of response, time to treatment failure, overall survival, safety, quality of life
*Docetaxel was administered for a maximum of nine cycles, but earlier discontinuation was permitted
Docetaxel* 100mg/m2 + placebo q3w
Docetaxel* + bevacizumab 7.5mg/kg
q3w
Docetaxel* + bevacizumab 15mg/kg
q3w
All patientsgiven optionto receive
bevacizumabwith 2nd-line
chemotherapy
1st-line locally recurrentor mBC (n=705)
Stratification factors:• region• prior taxane/time to
relapse since adjuvant chemo
• measurable disease• hormone receptor
status
Treat withplacebo/
bevacizumabto disease
progression
Miles D, et al. J Clin Oncol. 2008;26(18S). LBA 1011.

• Capecitabine (1000 mg/m2 BID x 14d)
• Taxane (docetaxel or protein-bound paclitaxel)
• Anthracycline-based chemotherapy (AC, EC, FAC, FEC)
• Placebo or bevacizumab (15 mg/kg)
CHOICE OF CHEMOBY INVESTIGATOR
Capecitabineor
Taxaneor
Anthracycline
Previously untreated MBC
(n=1,237)
Stratification Factors:
• Disease-free interval
• Previous adjuvant chemotherapy
• Number of metastatic sites
• Cape, T or Anthra
Chemo +bevacizumab
q3w
Chemo +placebo
q3w
Treat untilPD
RA
ND
OM
IZE
2:
1
Optional2nd-line Chemo
+bevacizumab
Robert et al, ASCO 2009 #1005
RIBBON-1

1Miller K, et al. N Engl J Med. 2007;357:2666-2676;
2Miles D, et al. J Clin Oncol. 2008;26(18S). LBA 1011.
E21001 AVADO2 RIBBON-1: Cape
RIBBON-1: A/T
Placebo Controlled
No Yes Yes Yes
ChemotherapyWeekly
paclitaxelq3w docetaxel Capecitabine
q3w doce/nabP
AC/FAC/EC/FEC
Dose of Bevacizumab
10 mg/kg q2wk7.5 or 15 mg/kg
q3wk15 mg/kg q3wk 15 mg/kg q3wk
Primary Endpoint
PFS PFS (IRF) PFS (Inv) PFS (Inv)
IRF review Retrospective Yes Yes Yes
39
Study Design

E21001 AVADO2 RIBBON-1: Cape
RIBBON-1: A/T
N 673 736 615 622
ER-/PR - 35% 22% 23% 24%
> 3 sites 45% 46% 44% 45%
Measureable disease
73% 83% 80% 84%
Adjuvant Chemo/Taxane
65%/16% 66%/15% 72%/40% 45%/15%
Patient Population
1Miller K, et al. N Engl J Med. 2007;357:2666-2676;
2Miles D, et al. J Clin Oncol. 2008;26(18S). LBA 1011.

E2100 AVADO RIBBON-1: Cape
RIBBON-1: A/T
P P+B D+Pl D+B C+Pl C+B A/T + Pl A/T+B
ORR 25% 49% 49% 55%/63% 24% 35% 38% 51%
PFS (months) 5.9 11.8 8.0 8.7/8.8 5.7 8.6 8.0 9.2
HR 0.60
P <0.0001
0.79 (7.5 mg)
P = 0.0318 0.72 (15 mg)
P = 0.0099
0.69
P = 0.0002
0.64
P <0.0001
OS (months)
25.2 26.7 NR NR 21.2 29 23.8 25.2
HR 0.88
P = 0.16
0.92 (7.5 mg)
0.86 (15 mg)
0.85
P = 0.27
1.03
P = 0.83
Relative increase in RR 20-50%
Efficacy

Case 3
• 63 year old with metastatic breast cancer consults you for advice on additional therapy
– Initial diagnosis 6 years ago, adjuvant AC x 4 cycles followed by AI for stage I disease (T2.1 cm, LN-, G2, ER+, PR-, HER2-)
– Metastatic disease identified with bone invovlement and mediastinal and SC adneopathy ~28 months ago
• Initially treated with fulvestrant > PR lasting 12 months
• Tamoxifen > SD lasting 6 months
• Exemestane > PD after 2 months
• Capecitabine > PR lasting 8 months, now with PD

Case 3
• Currently has minimally symptomatic bone involvement (does not require narcotics) with asymptomatic mediastinal nodes and new pulmonary nodules (largest 1.6 cm)
• PS = 1
• Local oncologist has recommended taxane based therapy
• Would you add bevacizumab?

National Cancer Institute. Clinical Trials (PDQ). Available at: http://www.cancer.gov/search/clinical_trials/.
Second-line
HER (-)Chemotherapy of choice†
Bevacizumab 10 mg/kg q2w(Bevacizumab 15 mg/kg q3w)
Chemotherapy of choice†
Placebo
†Docetaxel, paclitaxel (qw or q3w), nab-paclitaxel, gemcitabine, vinorelbine, or capecitabine.
Randomize2:1
Ribbon 2

Key Eligibility Criteria
• One prior cytotoxic treatment for MBC
• ECOG performance status (PS) 0 or 1
• HER2-negative or HER2 status unknown
• No prior therapy with bevacizumab or other VEGF pathway- target therapy

Brufsky et al, SABCS 2009 #42
Primary Endpoint of PFS(ITT Population)

Brufsky et al, SABCS 2009 #42
Cohort-Specific Analyses of PFS(ITT Population)

What We’ve Learned
• Bevacizumab is an important component of initial chemotherapy for metastatic HER2- breast cancer
– Increases RR
– Prolongs PFS
• Adds to second-line chemo in patients who didn’t get bevacizumab with initial chemo
• Toxicity differs among reported regimens
– Bevacizumab associated toxicity consistent

Remaining Questions
• Combine with anti-HER2 and hormonal therapies
• Optimal duration of therapy
• Why have we failed to demonstrate a difference in OS?

In Search of OS
• There is no difference
• Subsequent therapy obscures benefit of 1st line therapy
• Reported trials individually underpowered
– Amenable to meta-analysis (see ASCO 2010)
• Resistance to bevacizumab = more aggressive disease
• Rapid regrowth of vasculature after stopping bevacizumab

Remaining Questions
• Combine with anti-HER2 and hormonal therapies
• Optimal duration of therapy
• Why have we failed to demonstrate a difference in OS?
• Does the choice of chemotherapy matter?

Does the Choice of Chemo Matter?
• HR broadly similar but absolute improvements in PFS gain differ widely
– Ability to continue combined therapy
– Interval censoring
• May depend on mechanism(s) of action?
– Inherent anti-angiogenic effect of chemotherapy
– Chemotherapy induced release of bone marrow progenitors
– Role of VEGF on tumor cells

TKI Alternatives: SorafenibTargets Both Tumor-Cell Proliferation and Angiogenesis
Wilhelm et al, SABCS 2009 #42

TIES ProgramTrials to Investigate the Efficacy of Sorafenib in Breast Cancer

Baselga et al, SABCS 2009 #45
A Multinational Double-Blind, Randomized Phase 2b Study Evaluating the Efficacy and Safety of Sorafenib Compared to
Placebo when Administered in Combination with Capecitabine in Patients with Locally Advanced Metastatic Breast Cancer

Gradishar et al, SABCS 2009 #44
A Double-Blind, Randomized Phase 2b Study Evaluating the Efficacy and Safety of Sorafenib Compared to Placebo when Administered in Combination with Paclitaxel in Patients with
Locally Advanced Metastatic Breast Cancer
http://www.clinicaltrials.gov/ct/show/NCT00499525

Top Line Efficacy and Safety(SOLTI-0701 & NU 07B1)
Baselga et al.
(Capecitabine+/- Sorafenib)
Gradishar et al.
Paclitaxel +/- Sorafenib
Median PFS, * mos4.1 vs. 6.4
HR=0.576; P=0.0006**
5.6 vs. 6.9
HR=0.788; P=0.09**
TTP, * mos4.2 vs. 6.8 (P=0.0005**)
HR=0.562 (0.394, 0.799)
5.6 vs. 8.1 (P=0.0171**)
0.674 (0.465, 0.975)
Overall response rate, * %31 vs 38
P=0.1229**
54 vs 67
P=0.0234**
On-study deaths, * n (%) 5 (4.5) vs 5 (4.5) 4 (3) vs 16 (14)
Subjects with AE leading to discontinuation of study
treatment, * n (%)9 (8) vs 14 (13.4) 12 (10) vs 35 (30)
* Chemotherapy + placebo vs chemotherapy + sorafenib** One-sided

Adverse Event Rates (Safety Population)
Overall incidence ≥ 10% and Grade 3/4 ≥ 3% in either teratment arm
Baselga et al. Gradishar et al.
S+C
N=112
Pl+C
N=112
S+P
N=115
Pl+P
N=118
All (%)
Grade 3 (%)
All (%)
Grade 3 (%)
All (%)
Grade 3 (%)
All (%)
Grade 3 (%)
HFSR 89 45 63 13 55 30 7 3
Diarrhea 53 5 30 5 37 3 25 3
Asthenia 24 0 27 2 29 7 21 3
Fatigue 14 2 13 1 14 3 20 2
Dyspnea 12 5 12 3 13 1 14 3
Neutropenia 11 4 4 2 24 10 19 4
P=Paclitaxel, S=Sorafenib, C=Capecitabine, Pl=Placebo

SABCS 2009 #45
PFS: ITT Population

SOLTI-0701: Capecitabine +/- Sorafenib
• 42% reduction in risk of disease progression or death
– PFS benefit observed in subgroup analyses
– PFS benefit noted in both first-line and second-line therapy
• Increased incidence of hand-foot syndrome
– Attention to dose modification critical
• Phase III registration trial planned for sorafenib/capecitabine in advanced breast cancer

Motesanib Blocks More Than One Mechanism Involved in Tumorigenesis

Mackey et al, SABCS 2009 #47
Study Design
Mackey et al, SABCS 2009 #47

Mackey et al, SABCS 2009 #47
Objective Response Rate(ITT Population)
Mackey et al, SABCS 2009 #47

Mackey et al, SABCS 2009 #47
Progression-Free Survival(ITT Population)
Mackey et al, SABCS 2009 #47

Mackey et al, SABCS 2009 #47
Progression-Free Survival(ITT Population)

Favors Capecitabine
Phase III Sunitinib vs. Capecitabine
• HER2 negative, prior anthracycline and taxane required
• N=483
• ORR 11.3 % vs. 16.4%
• PFS 2.8 months vs. 4.2 months
Barrios et al, SABCS 2009 #46
Conclusions
• Bevacizumab is an important component of initial chemotherapy for patients with HER2- disease
– Some benefit in second line if not given prior
• All bevacizumab containing regimens are not equal
– Toxicity differences clear
– Efficacy?
– Differences in chemotherapy affects may be important
• Small molecule VEGF TKIs have some activity as well but toxicity troublesome

I don’t know if heavier than air flight is possible, but I’m committed to living my life dedicated to its possibility. - Wilbur Wright
The Future Is Possible


















