Methods of suicide: international suicide patterns derived ...
Upload
rodger-jacksonCategory
view
226download
3
Kate Comtois, PhD, MPHUniversity of Washington
Treatment Interventions for Suicide Prevention
Suicide prevention has many forms
Public health or injury prevention
Gatekeeper Training
Treating Depression
Suicide prevention has many forms
This talk is about preventing suicide with mental health interventions to treat suicide attempts or other suicidal behavior
Overview
• What does the clinical trial research tell us about treatment with suicidal patients?– What doesn’t work?– What does work?
• What can we learn clinically from the research data?
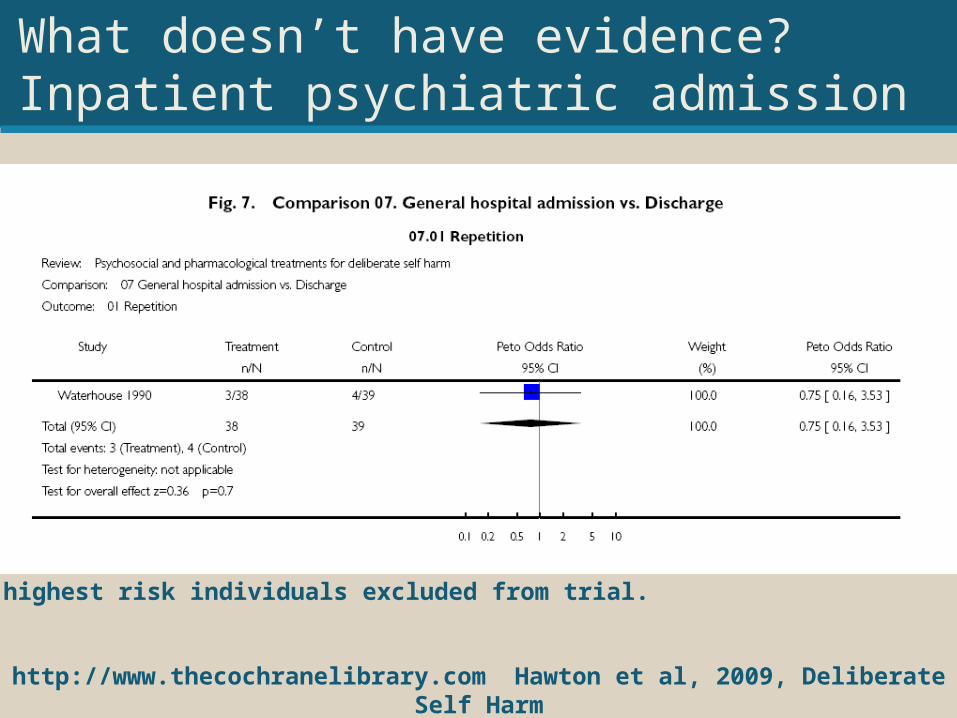
What doesn’t have evidence?Inpatient psychiatric admission
http://www.thecochranelibrary.com Hawton et al, 2009, Deliberate Self Harm
Note, highest risk individuals excluded from trial.
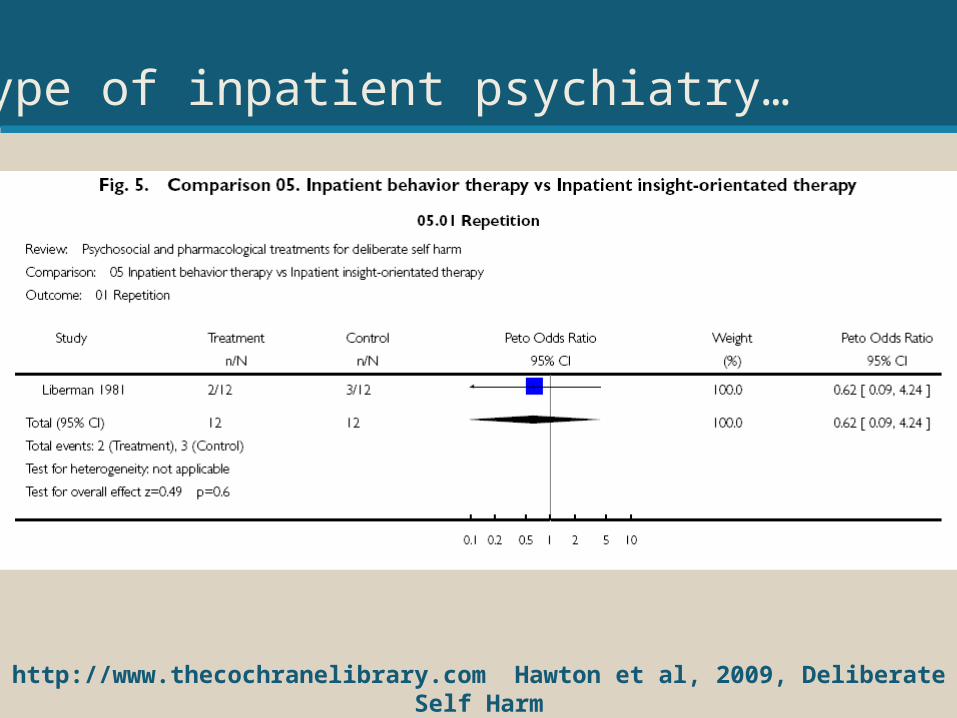
Or type of inpatient psychiatry…
http://www.thecochranelibrary.com Hawton et al, 2009, Deliberate Self Harm
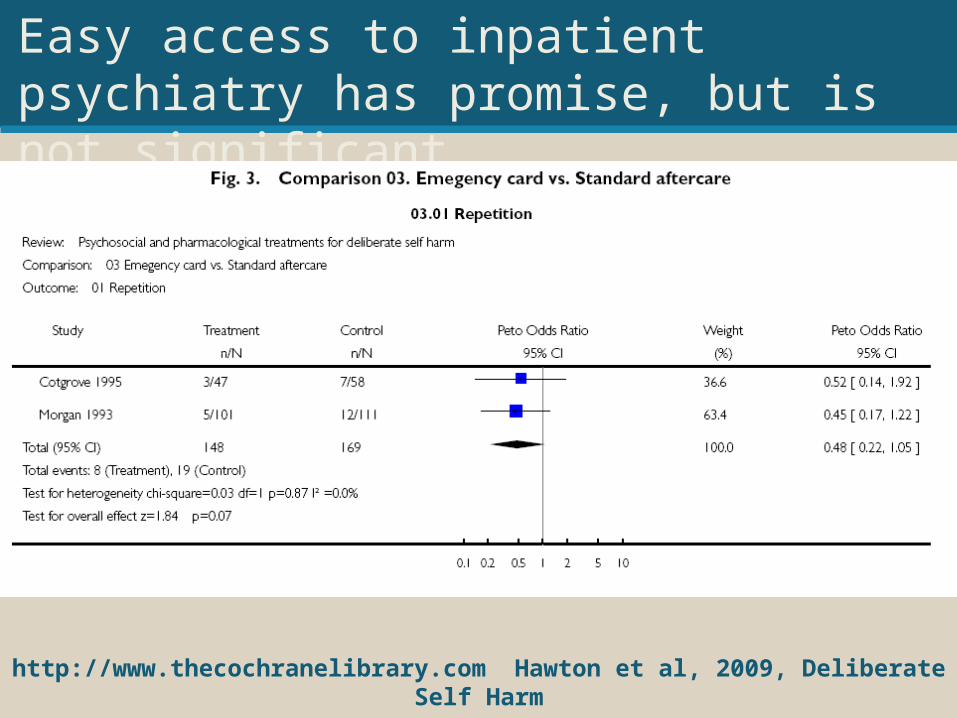
Easy access to inpatient psychiatry has promise, but is not significant.
http://www.thecochranelibrary.com Hawton et al, 2009, Deliberate Self Harm
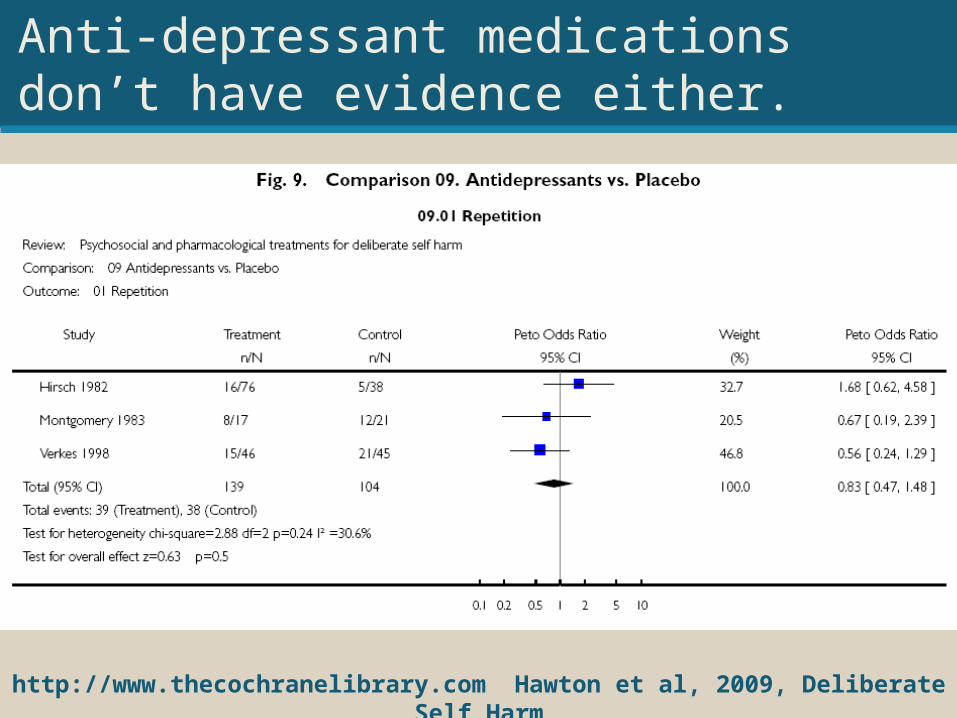
Anti-depressant medications don’t have evidence either.
http://www.thecochranelibrary.com Hawton et al, 2009, Deliberate Self Harm
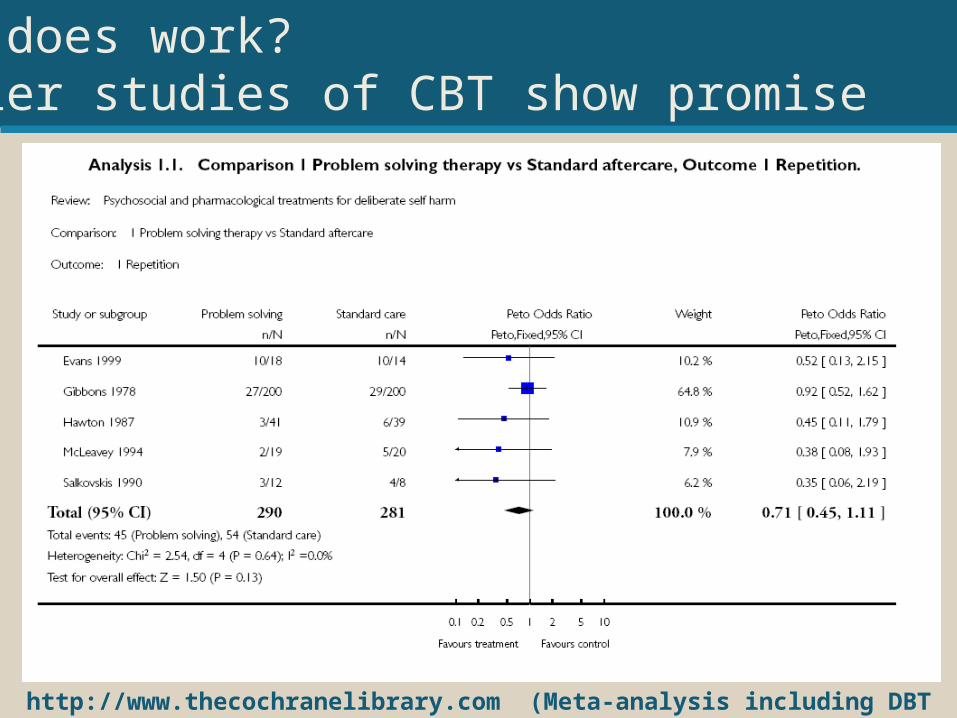
What does work?Earlier studies of CBT show promise
http://www.thecochranelibrary.com (Meta-analysis including DBT show significance for CBT)
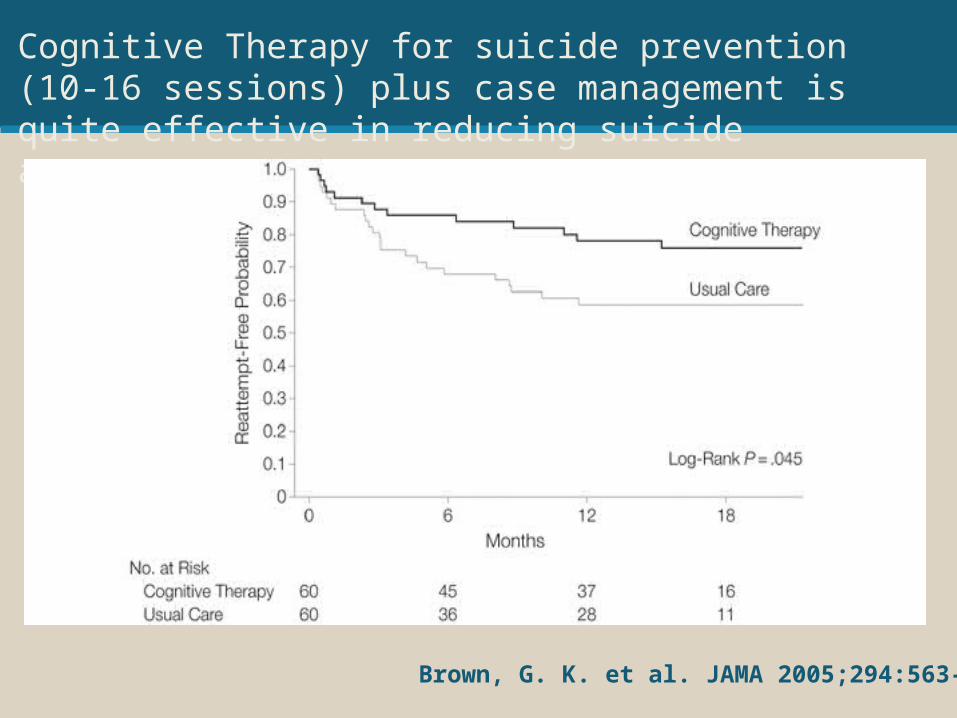
Cognitive Therapy for suicide prevention (10-16 sessions) plus case management is quite effective in reducing suicide attempts.
Brown, G. K. et al. JAMA 2005;294:563-570
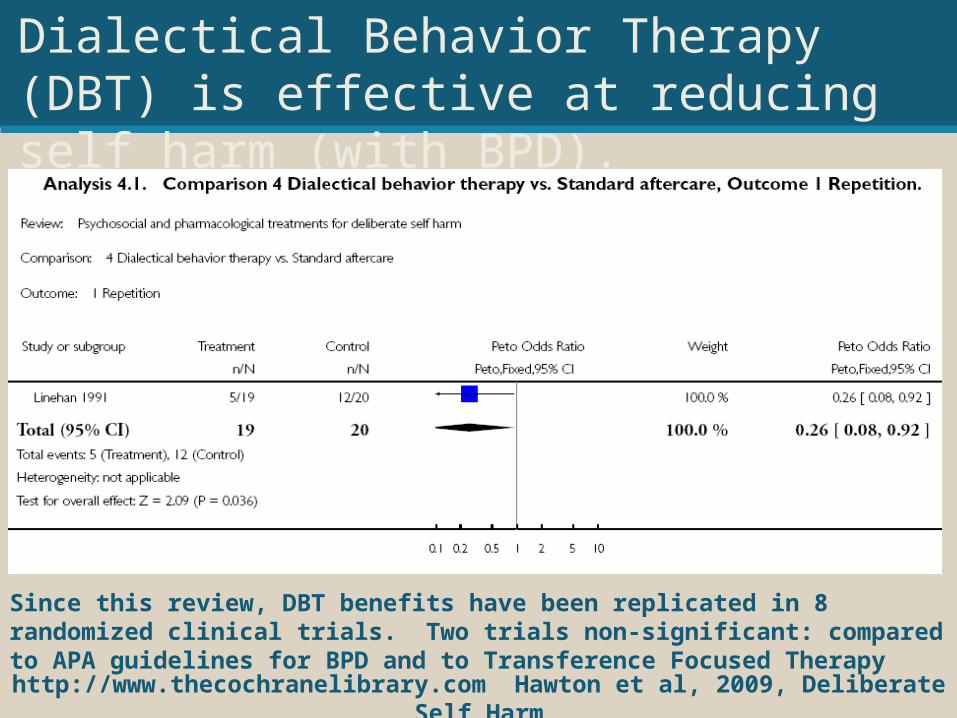
Dialectical Behavior Therapy (DBT) is effective at reducing self harm (with BPD).
http://www.thecochranelibrary.com Hawton et al, 2009, Deliberate Self Harm
Since this review, DBT benefits have been replicated in 8 randomized clinical trials. Two trials non-significant: compared to APA guidelines for BPD and to Transference Focused Therapy
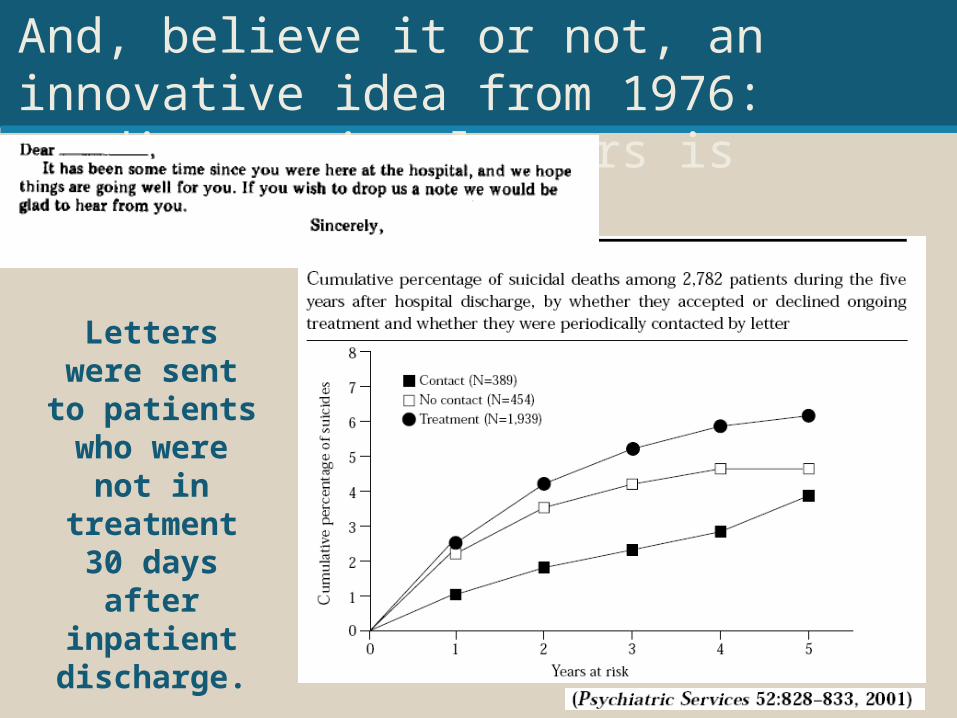
And, believe it or not, an innovative idea from 1976: sending caring letters is effective.
Letters were sent to patients who were not in
treatment 30 days after inpatient discharge.
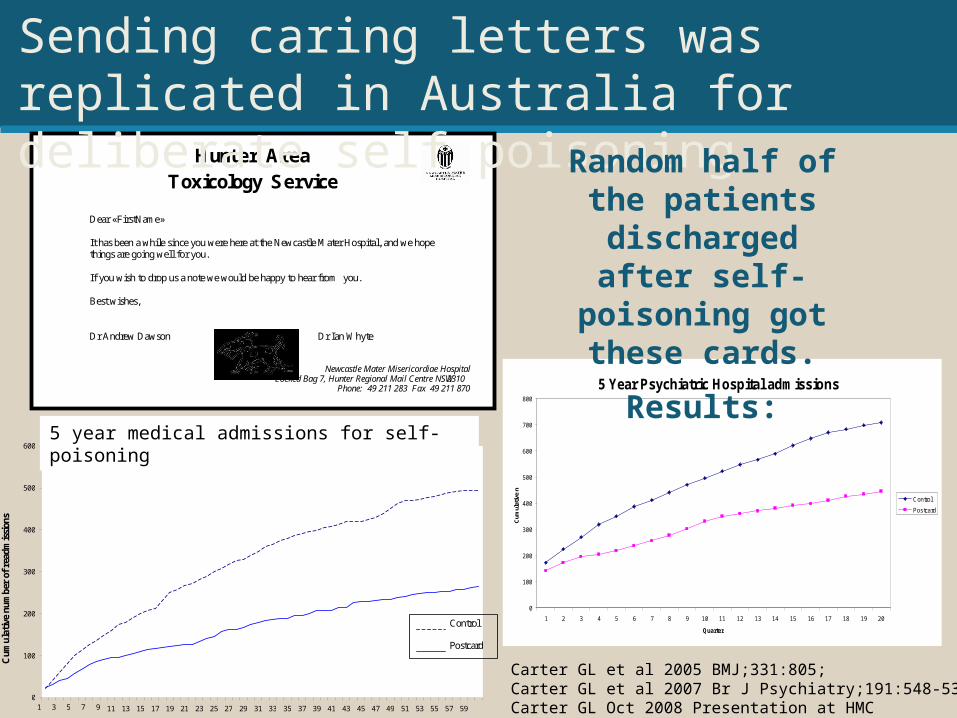
Hunter Area
Toxicology Service
Dear « FirstName » It has been a while since you were here at the Newcastle Mater Hospital, and we hope things are going well for you. If you wish to drop us a note we would be happy to hear from you. Best wishes, Dr Andrew Dawson Dr Ian Whyte
Newcastle Mater Misericordiae Hospital
Locked Bag 7, Hunter Regional Mail Centre NSW 2310 Phone: 49 211 283 Fax 49 211 870
5 Year Psychiatric Hospital admissions
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Quarter
Cum
ulat
ive
n
Control
Postcard
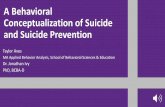
Sending caring letters was replicated in Australia for deliberate self poisoning.
Random half of the patients discharged after self-poisoning
got these cards.
Results:
0
100
200
300
400
500
600
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59
Months
Cum
ulat
ive
num
ber
of r
eadm
issi
ons
Control
Postcard
5 year medical admissions for self-poisoning
Carter GL et al 2005 BMJ;331:805; Carter GL et al 2007 Br J Psychiatry;191:548-53.Carter GL Oct 2008 Presentation at HMC
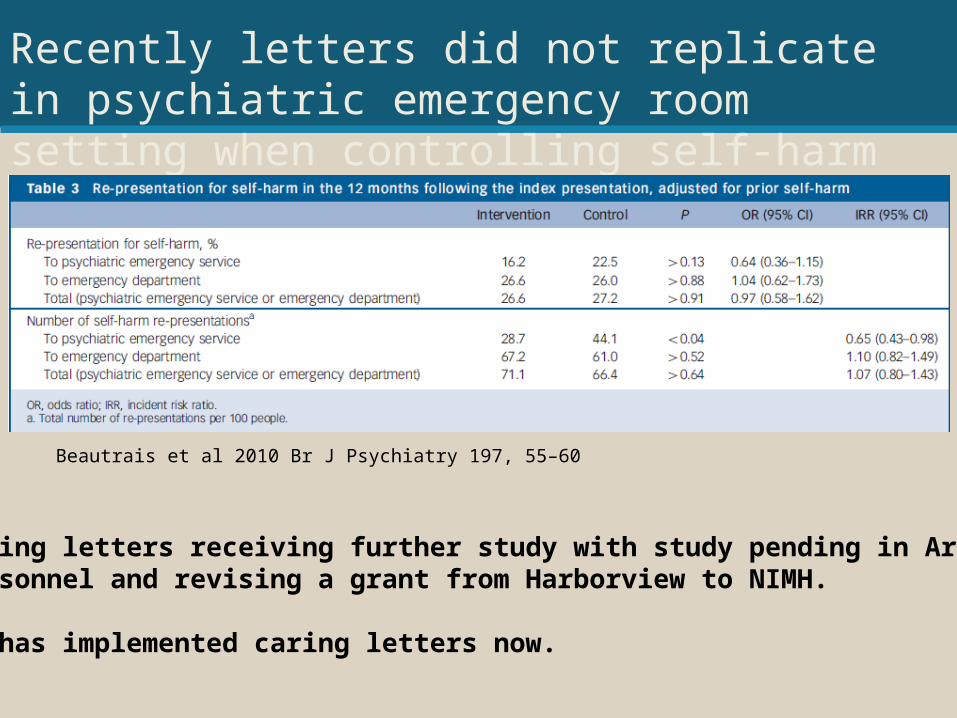
Recently letters did not replicate in psychiatric emergency room setting when controlling self-harm
Beautrais et al 2010 Br J Psychiatry 197, 55–60
Caring letters receiving further study with study pending in Army personnel and revising a grant from Harborview to NIMH.
VA has implemented caring letters now.
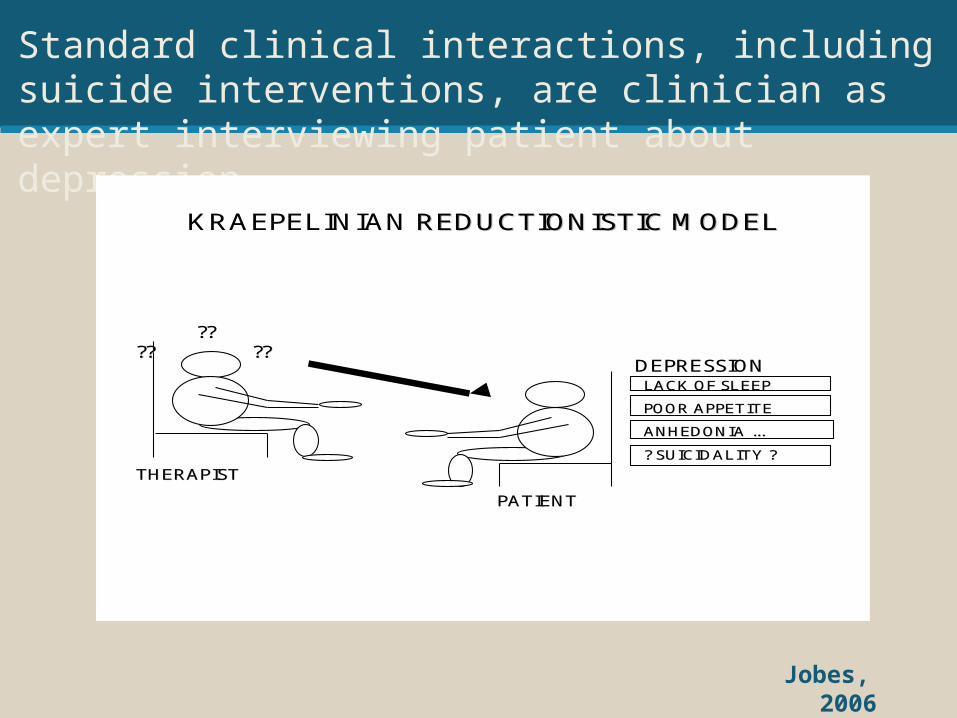
Jobes, 2006
Standard clinical interactions, including suicide interventions, are clinician as expert interviewing patient about depression.
????????
????
THERAPISTTHERAPIST
PATIENTPATIENT
KRAEPELINIAN REDUCTIONISTIC MODELREDUCTIONISTIC MODEL
DEPRESSIONDEPRESSIONLACK OF SLEEPLACK OF SLEEP
POOR APPETITEPOOR APPETITE
ANHEDONIA ...ANHEDONIA ...
? SUICIDALITY ?? SUICIDALITY ?
(1) Treating suicide directly (not just bytreating the diagnosis)
Effective psychotherapies for suicidal individuals have (at least) 2 differences.
(2) Using an overtly collaborative stance rather than psychiatric interview.
Treatment of psychiatric diagnosis does not necessarily result in reduction of suicide risk.
• Treatment associated with reduced psychiatric symptoms and suicidal behavior:– Lithium in bipolar
affective disorder (no RCT but Baldessarini et al, 1999 shows evidence in review of studies) (RCT in progress)
– Clozapine in schizophrenia (one RCT: Meltzer et al., 1998)
• Treatment not associated with reduced psychiatric symptoms and suicidal behavior:– Depression (Brent et al,
1997; Hawton et al, 2009; Khan et al., 2000; Khan et al, 2001; Lerner & Clum, 1990; Rutz, 1999)
– Psychosis (Khan et al., 2001)
– Depression in Borderline Personality Disorder (Linehan et al, 1991)
If you’re not treating diagnosis,what should you treat?
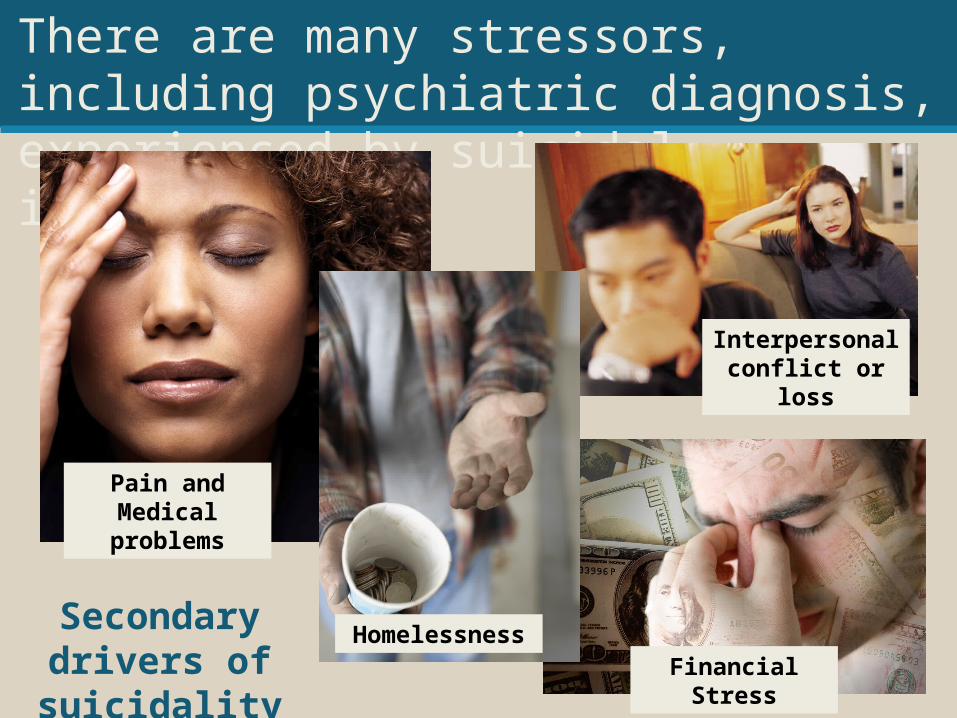
There are many stressors, including psychiatric diagnosis, experienced by suicidal individuals.
Secondary drivers of suicidality
Pain and Medical problems
HomelessnessFinancial Stress
Interpersonal conflict or loss
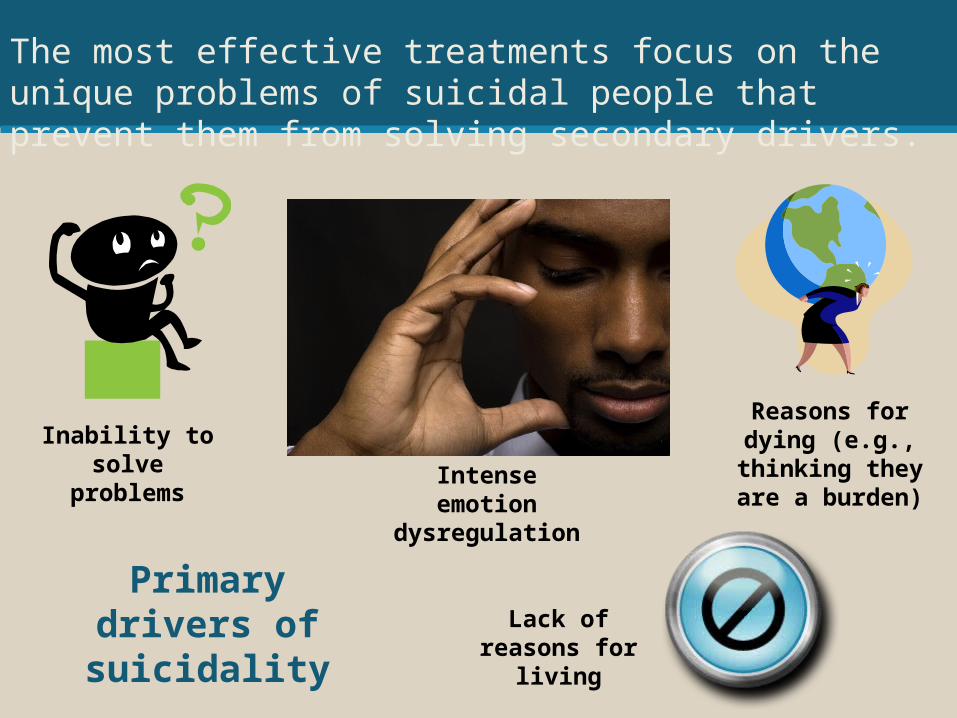
The most effective treatments focus on the unique problems of suicidal people that prevent them from solving secondary drivers.
Primary drivers of suicidality
Intense emotion dysregulation
Inability to solve problems
Reasons for dying (e.g., thinking they
are a burden)
Lack of reasons for living
Psychiatric interviews often do not create collaboration.
• Instead, the patient is more likely to feel interrogated (or even shamed if regretful).
• The patient may feel that you are only trying to run through a checklist, rather than trying to understand what is really going on.
• Patients are frequently aware that they can have their freedom taken away due to their suicide risk, so they can be leery of authority.
Jobes, 2007
Collaborative Assessment and Management of Suicidality(CAMS)
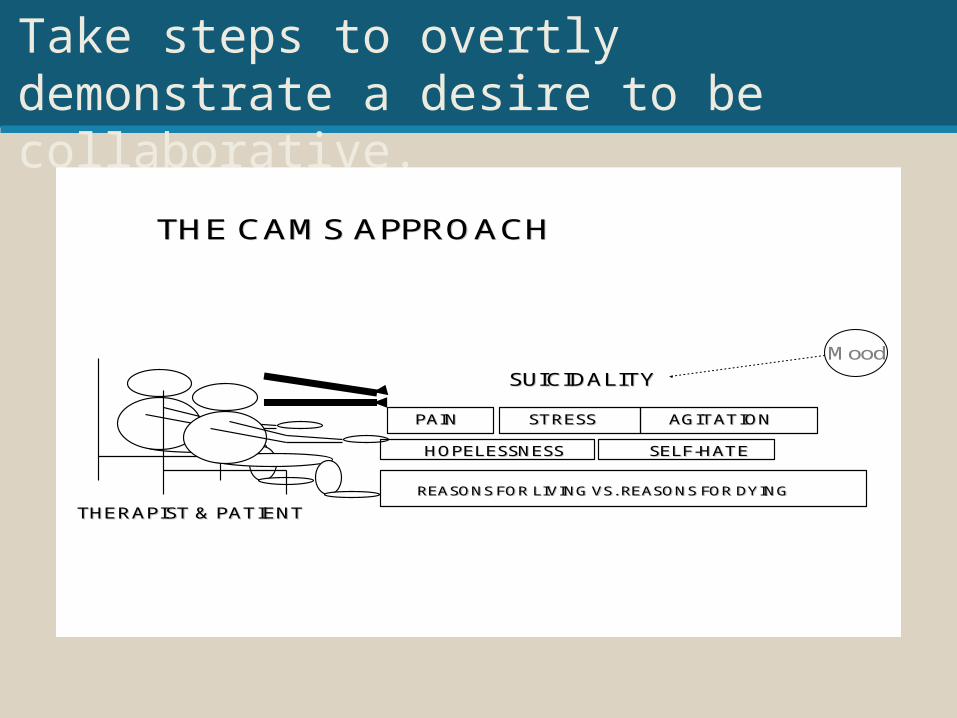
Take steps to overtly demonstrate a desire to be collaborative.
THE CAMS APPROACHTHE CAMS APPROACH
THERAPIST & PATIENTTHERAPIST & PATIENT
SUICIDALITYSUICIDALITY
PAINPAIN STRESSSTRESS AGITATIONAGITATION
HOPELESSNESSHOPELESSNESS SELFSELF--HATEHATE
REASONS FOR LIVING VS. REASONS FOR DYINGREASONS FOR LIVING VS. REASONS FOR DYING
Mood
Collaborative Stance in CAMS
• Want to directly demonstrate to client that you empathize with the patient’s suicidal wish– “You have everything to gain and nothing to lose from
participating in this potentially life-saving treatment”.– You can always kill yourself later.
• At the same time, clarify when you would have to take action that they might not choose – know your personal and clinic limits– If they won’t participate in treatment…OR– If they say they can’t control their impulses…
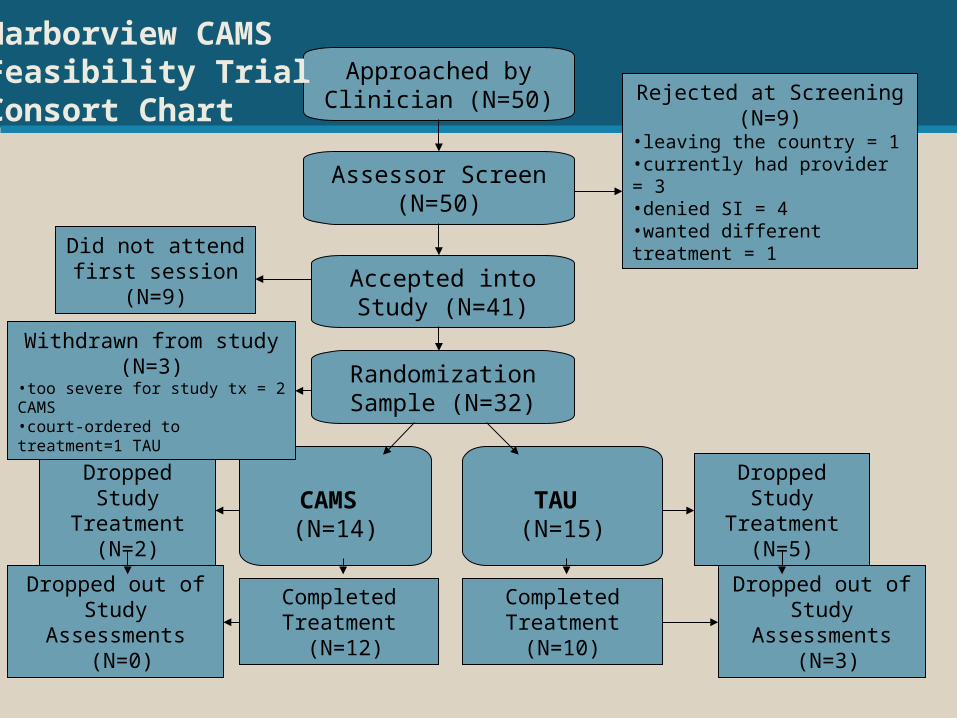
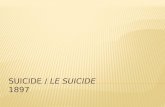
Approached by Clinician (N=50)
Assessor Screen (N=50)
Accepted into Study (N=41)
Randomization Sample (N=32)
Rejected at Screening (N=9)•leaving the country = 1 •currently had provider = 3 •denied SI = 4 •wanted different treatment = 1
CAMS (N=14)
TAU (N=15)
Completed Treatment
(N=10)
Dropped Study Treatment (N=2)
Dropped out of Study Assessments
(N=0)
Completed Treatment
(N=12)
Did not attend first session (N=9)
Dropped Study Treatment (N=5)
Dropped out of Study Assessments
(N=3)
Harborview CAMSFeasibility TrialConsort Chart
Withdrawn from study (N=3)•too severe for study tx = 2 CAMS•court-ordered to treatment=1 TAU
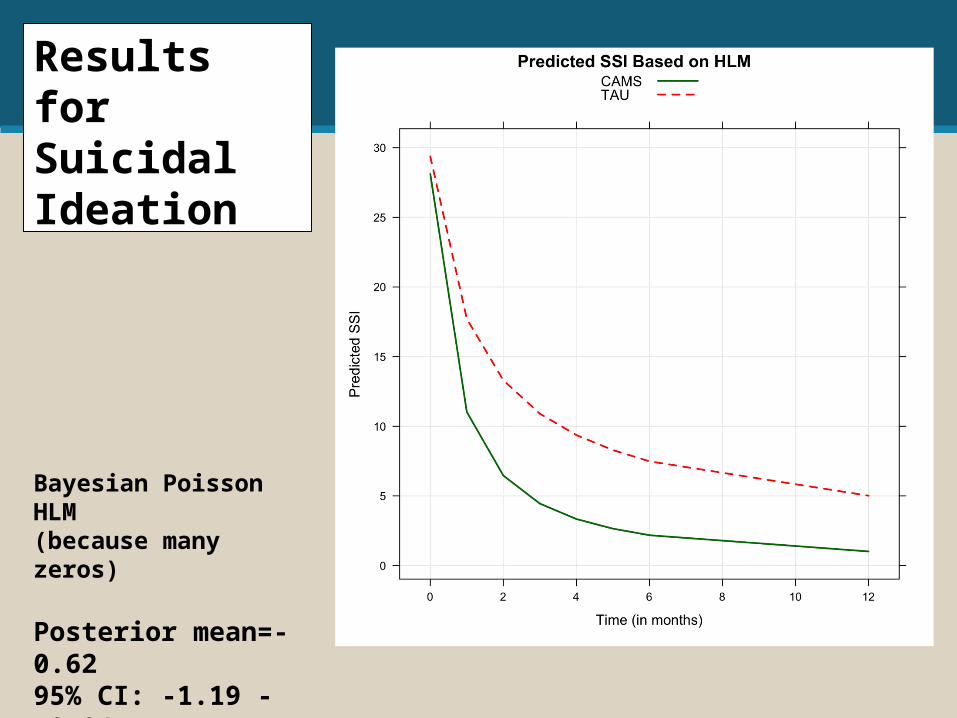
Results for Suicidal Ideation
Bayesian Poisson HLM(because many zeros)
Posterior mean=-0.6295% CI: -1.19 - -0.04
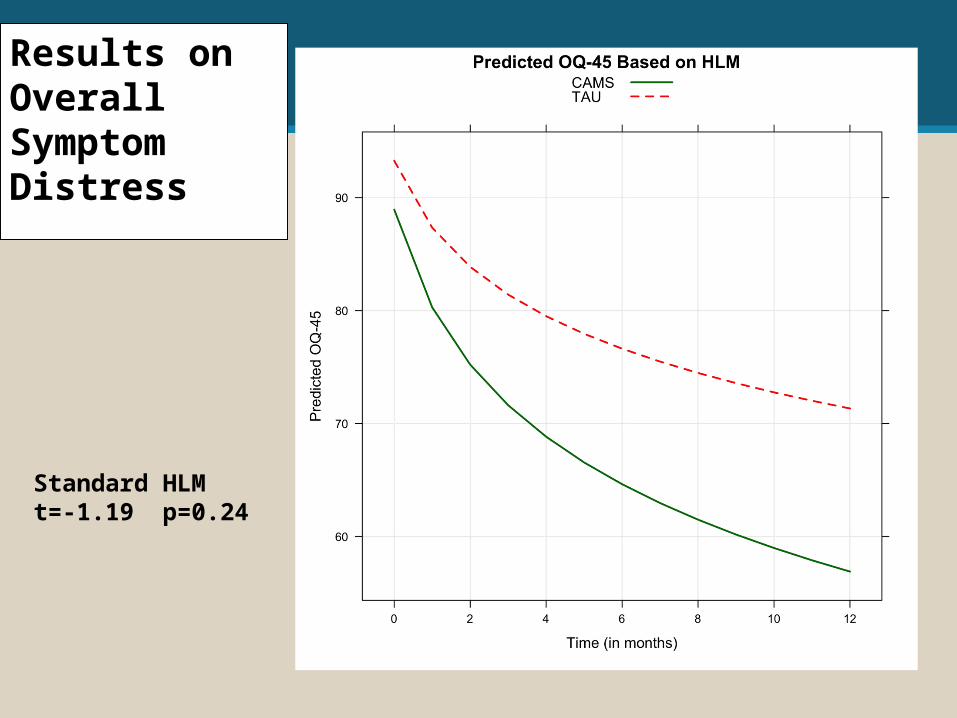
Results on Overall Symptom Distress
Standard HLMt=-1.19 p=0.24
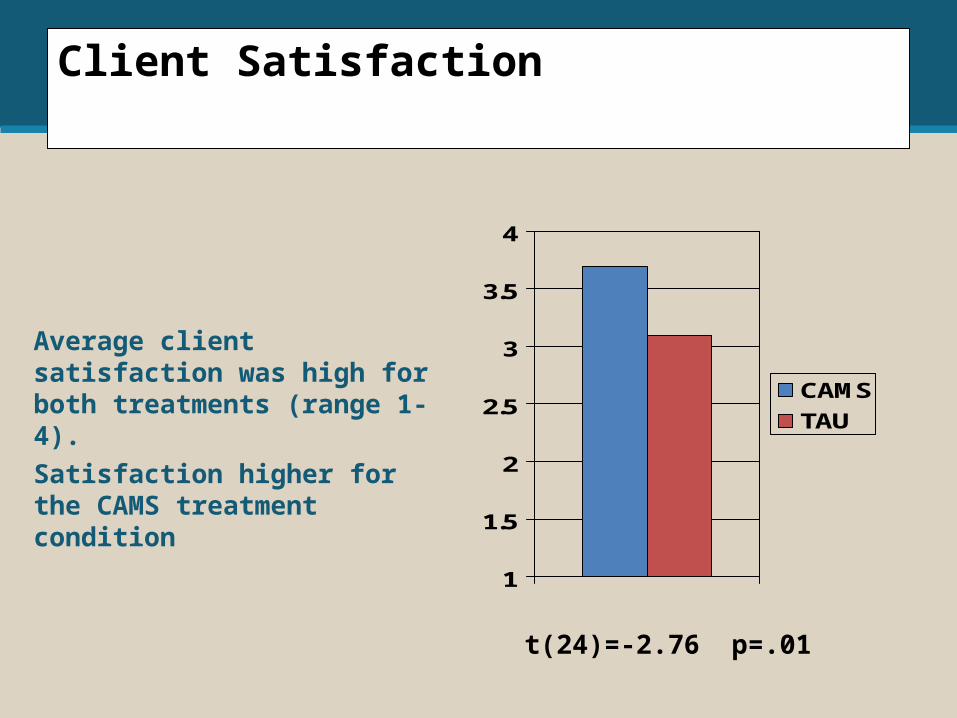
Client Satisfaction
Average client satisfaction was high for both treatments (range 1-4).Satisfaction higher for the CAMS treatment condition
1
1.5
2
2.5
3
3.5
4
CAMS
TAU
t(24)=-2.76 p=.01
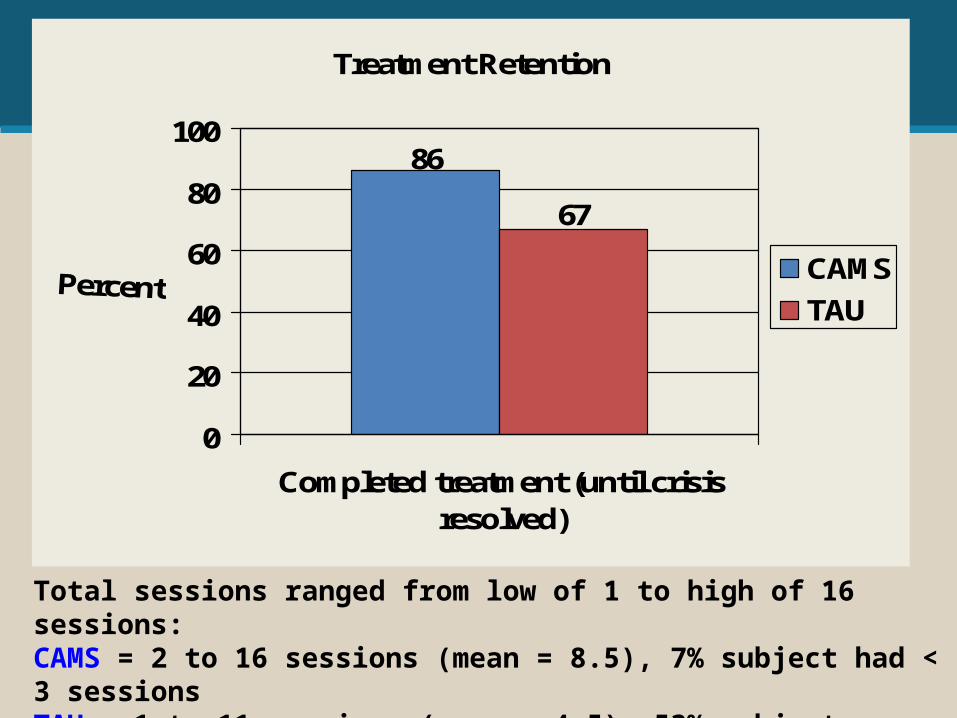
Treatment Retention
86
67
0
20
40
60
80
100
Completed treatment (until crisisresolved)
CAMS
TAU
Total sessions ranged from low of 1 to high of 16 sessions:CAMS = 2 to 16 sessions (mean = 8.5), 7% subject had < 3 sessionsTAU = 1 to 11 sessions (mean = 4.5), 53% subjects had < 3 sessions
In summary
1.There are relatively few clinical trials for treatments for suicidality.
2.Standard of care interventions such as inpatient and anti-depressants do not have strong support.
3.Psychotherapy – particularly CBT and DBT have support.
4.Caring letters alone have support.5.Psychotherapy emphasizes collaboration and
directly treating suicidality. Perhaps this makes them more effective?
Questions?