
kala-azar West 1. dermal leishmaniasis the outbreak 24...
6
Ten years of kala-azar in West Bengal, Part 1. Did post-kala-azar dermal leishmaniasis initiate the outbreak in 24-Parganas?* Manjulika Addy1 & A. Nandy2 Following resurgence in Bihar of epidemic kala-azar, outbreaks of the disease were identified simulta- neously in two separate foci about 500 km apart in West Bengal in 1980. While the outbreak in one of these foci, in northern West Bengal, was the result of a direct extension of the Bihar epidemic, the source of parasite in the other (in the village of Bandipur in the south of West Bengal) remained un- known until a case of nodulo-ulcerative post-kala-azar dermal leishmaniasis (PKDL) was located in the village. The continued presence of this case in the village from a time long before the outbreak aroused strong suspicion about its causal role. Laboratory-bred female Phlebotomus argentipes sandflies were allowed to feed on four cases of PKDL, including the case from Bandipur, to determine the transmission potential of these cases. Of a total of 400 flies in the experiment, 104 (26%) fed on the cases, and of these flies 44 died (31 within 48 hours of feeding). Of the surviving 60 flies, 32 developed promastigotes in the mid-gut. In view of the presence of the case of PKDL in the village prior to the outbreak and the availability of a susceptible human population and vectors, it is possible that the patient with PKDL was a source of Leishmania donovani parasites for the local focus. Furthermore, PKDL may act as a reservoir of parasites during inter-epidemic periods. Introduction Unlike other areas where kala-azar is endemic, in India it appears to be anthroponotic (1, 2) and the evidence available so far, although incomplete, is not consistent with the existence of a nonhuman reservoir for Leishmania donovani. Post-kala-azar dermal leishmaniasis (PKDL) has long been suspec- ted to have the potential of a reservoir (2-4), particu- larly in view of the occurrence of numerous parasites in the skin of individuals with nodular PKDL. Moreover, there are uncertainties about the role played by cases of PKDL in maintaining L. donovani in nature during inter-epidemic periods and also their role in the origin of fresh outbreaks. Apart from a few serological investigations (1, 5), there have been no systematic attempts to implicate animals as reser- voirs of L. donovani in India. After kala-azar had virtually disappeared from India for about 20 years, following the outbreak in Bihar State in 1970-71, the disease was identified simultaneously in epidemic form in 1980 in two dis- * From the Division of Parasitology, Calcutta School of Tropical Medicine, Chittaranjan Avenue, Calcutta 700 073, India. ' Research Officer. 2 Associate Professor. Requests for reprints should be sent to Dr. A. Nandy, 72A, Jatin Das Road, Calcutta 700 029, India. Reprint No. 5285 tinct foci about 500 km apart in West Bengal. One of these foci was in Malda district, in northern West Bengal, which shares a common border with the kala-azar-affected district of Katihar in Bihar, and the other was in the district of 24-Parganas, in southem West Bengal (Fig. 1) (6-9).a The source of infection for the focus in Malda was traced to the adjacent district of Katihar in Bihar, with the mode of entry being population movement (8). The situa- tion in 24-Parganas was more complex since here the population appeared not to have any communication with known kala-azar foci in either West Bengal or Bihar. It was therefore of importance to identify the source of L. donovani in this isolated district, into which a few Bengalis had immigrated from Bangladesh 20-30 years ago. A thorough house-to- house survey revealed a possible source of infec- tion-an individual with nodulo-ulcerative PKDL in the village of Bandipur in 24-Parganas. We therefore carried out a study to ascertain the role of this individual in initiating the kala-azar out- break in Bandipur. Three more cases of PKDL from other unrelated areas were also included in the study. a Hati, A.K. et al. An epidemic outbreak of kala-azar in a district in West Bengal, India. Unpublished document WHO/VBC/85.91 1; WHO/LEISH/85. 22. Bulletin of the World Health Organization, 70 (3): 341-346 (1992) © World Health Organization 1992 341
Transcript of kala-azar West 1. dermal leishmaniasis the outbreak 24...
Ten years of kala-azar in West Bengal, Part 1.Did post-kala-azar dermal leishmaniasis initiatethe outbreak in 24-Parganas?*Manjulika Addy1 & A. Nandy2
Following resurgence in Bihar of epidemic kala-azar, outbreaks of the disease were identified simulta-neously in two separate foci about 500 km apart in West Bengal in 1980. While the outbreak in oneof these foci, in northern West Bengal, was the result of a direct extension of the Bihar epidemic, thesource of parasite in the other (in the village of Bandipur in the south of West Bengal) remained un-known until a case of nodulo-ulcerative post-kala-azar dermal leishmaniasis (PKDL) was located in thevillage. The continued presence of this case in the village from a time long before the outbreak arousedstrong suspicion about its causal role.
Laboratory-bred female Phlebotomus argentipes sandflies were allowed to feed on four cases ofPKDL, including the case from Bandipur, to determine the transmission potential of these cases. Of atotal of 400 flies in the experiment, 104 (26%) fed on the cases, and of these flies 44 died (31 within 48hours of feeding). Of the surviving 60 flies, 32 developed promastigotes in the mid-gut. In view of thepresence of the case of PKDL in the village prior to the outbreak and the availability of a susceptiblehuman population and vectors, it is possible that the patient with PKDL was a source of Leishmaniadonovani parasites for the local focus. Furthermore, PKDL may act as a reservoir of parasites duringinter-epidemic periods.
IntroductionUnlike other areas where kala-azar is endemic, inIndia it appears to be anthroponotic (1, 2) andthe evidence available so far, although incomplete,is not consistent with the existence of a nonhumanreservoir for Leishmania donovani. Post-kala-azardermal leishmaniasis (PKDL) has long been suspec-ted to have the potential of a reservoir (2-4), particu-larly in view of the occurrence of numerous parasitesin the skin of individuals with nodular PKDL.Moreover, there are uncertainties about the roleplayed by cases of PKDL in maintaining L. donovaniin nature during inter-epidemic periods and also theirrole in the origin of fresh outbreaks. Apart from afew serological investigations (1, 5), there have beenno systematic attempts to implicate animals as reser-voirs of L. donovani in India.
After kala-azar had virtually disappeared fromIndia for about 20 years, following the outbreak inBihar State in 1970-71, the disease was identifiedsimultaneously in epidemic form in 1980 in two dis-
* From the Division of Parasitology, Calcutta School of TropicalMedicine, Chittaranjan Avenue, Calcutta 700 073, India.' Research Officer.2 Associate Professor. Requests for reprints should be sent toDr. A. Nandy, 72A, Jatin Das Road, Calcutta 700 029, India.Reprint No. 5285
tinct foci about 500 km apart in West Bengal. One ofthese foci was in Malda district, in northern WestBengal, which shares a common border with thekala-azar-affected district of Katihar in Bihar, andthe other was in the district of 24-Parganas, insouthem West Bengal (Fig. 1) (6-9).a The sourceof infection for the focus in Malda was traced to theadjacent district of Katihar in Bihar, with the modeof entry being population movement (8). The situa-tion in 24-Parganas was more complex since here thepopulation appeared not to have any communicationwith known kala-azar foci in either West Bengal orBihar. It was therefore of importance to identify thesource of L. donovani in this isolated district, intowhich a few Bengalis had immigrated fromBangladesh 20-30 years ago. A thorough house-to-house survey revealed a possible source of infec-tion-an individual with nodulo-ulcerative PKDL inthe village of Bandipur in 24-Parganas.
We therefore carried out a study to ascertain therole of this individual in initiating the kala-azar out-break in Bandipur. Three more cases of PKDL fromother unrelated areas were also included in the study.
a Hati, A.K. et al. An epidemic outbreak of kala-azar in adistrict in West Bengal, India. Unpublished documentWHO/VBC/85.91 1; WHO/LEISH/85. 22.
Bulletin of the World Health Organization, 70 (3): 341-346 (1992) © World Health Organization 1992 341
M. Addy & A. Nandy
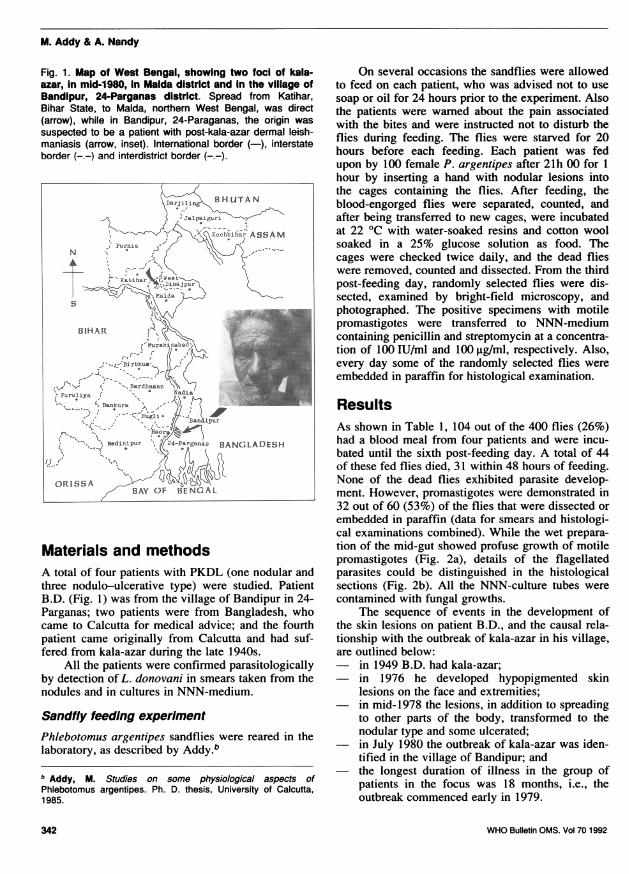
Fig. 1. Map of West Bengal, showing two foci of kala-azar, in mid-1980, In Malda district and in the village ofBandipur, 24-Parganas district. Spread from Katihar,Bihar State, to Malda, northern West Bengal, was direct(arrow), while in Bandipur, 24-Paraganas, the origin wassuspected to be a patient with post-kala-azar dermal leish-maniasis (arrow, inset). International border (-), interstateborder (-.-) and interdistrict border (-.-).
zarI DHTAN
NS S AMlKohblarASSA
OsISSA ISG L^D ES l'
BIHAR
Atfurpat
Pgsw an wfl-varomPaBANGLADESH
ORISSAAYO N L
Materials and methodsA total of four patients with PKDL (one nodular andthree nodulo-ulcerative type) were studied. PatientB.D. (Fig. 1) was from the village of Bandipur in 24-Parganas; two patients were from Bangladesh, whocame to Calcutta for medical advice; and the fourthpatient came originally from Calcutta and had suf-fered from kala-azar during the late 1940s.
All the patients were confirmed parasitologicallyby detection of L. donovani in smears taken from thenodules and in cultures in NNN-medium.
Sandfly feeding experimentPhlebotomus argentipes sandflies were reared in thelaboratory, as described by Addy.bb Addy, M. Studies on some physiological aspects ofPhlebotomus argentipes. Ph. D. thesis, University of Calcutta,1985.
On several occasions the sandflies were allowedto feed on each patient, who was advised not to usesoap or oil for 24 hours prior to the experiment. Alsothe patients were warned about the pain associatedwith the bites and were instructed not to disturb theflies during feeding. The flies were starved for 20hours before each feeding. Each patient was fedupon by 100 female P. argentipes after 21h 00 for 1hour by inserting a hand with nodular lesions intothe cages containing the flies. After feeding, theblood-engorged flies were separated, counted, andafter being transferred to new cages, were incubatedat 22 °C with water-soaked resins and cotton woolsoaked in a 25% glucose solution as food. Thecages were checked twice daily, and the dead flieswere removed, counted and dissected. From the thirdpost-feeding day, randomly selected flies were dis-sected, examined by bright-field microscopy, andphotographed. The positive specimens with motilepromastigotes were transferred to NNN-mediumcontaining penicillin and streptomycin at a concentra-tion of 100 IU/ml and 100 ,ug/ml, respectively. Also,every day some of the randomly selected flies wereembedded in paraffin for histological examination.
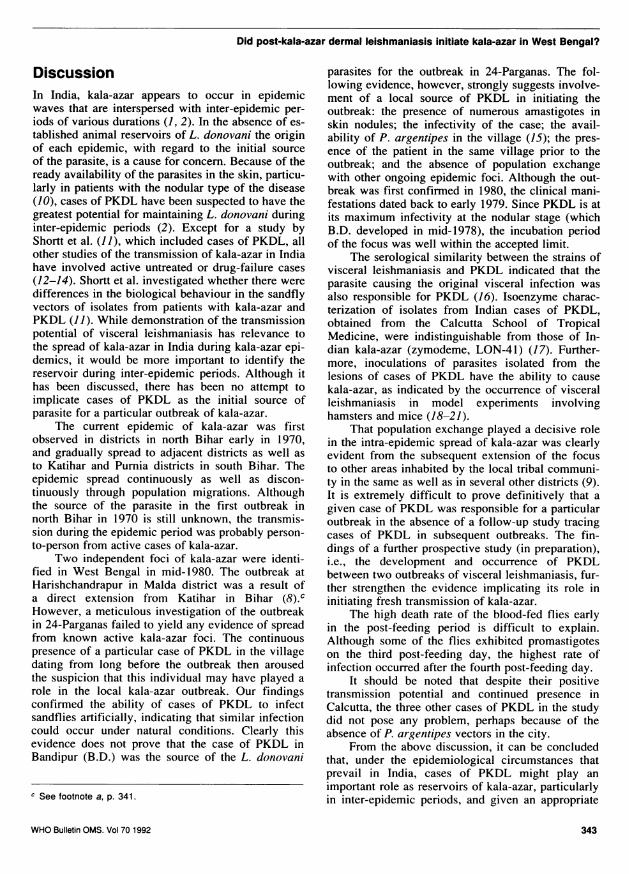
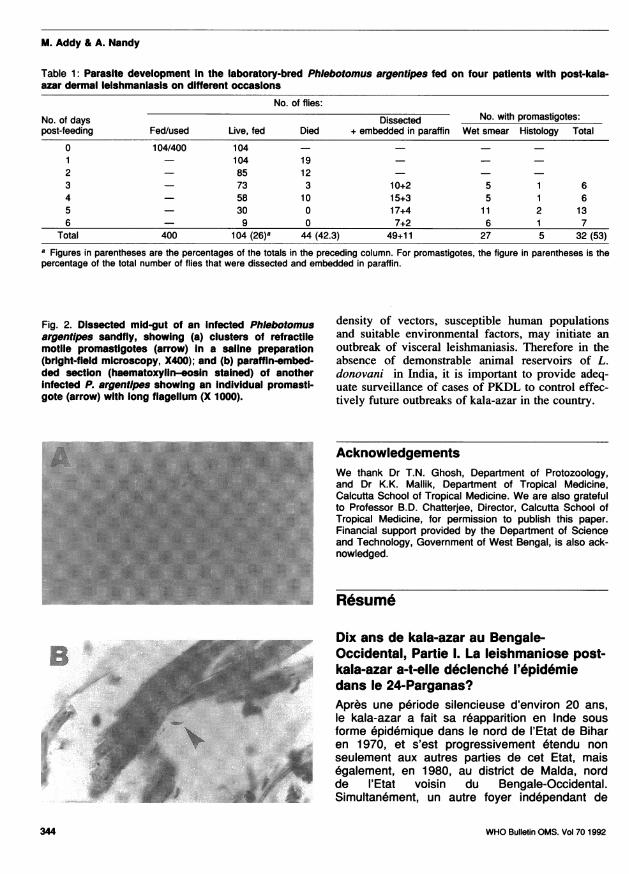
ResultsAs shown in Table 1, 104 out of the 400 flies (26%)had a blood meal from four patients and were incu-bated until the sixth post-feeding day. A total of 44of these fed flies died, 31 within 48 hours of feeding.None of the dead flies exhibited parasite develop-ment. However, promastigotes were demonstrated in32 out of 60 (53%) of the flies that were dissected orembedded in paraffin (data for smears and histologi-cal examinations combined). While the wet prepara-tion of the mid-gut showed profuse growth of motilepromastigotes (Fig. 2a), details of the flagellatedparasites could be distinguished in the histologicalsections (Fig. 2b). All the NNN-culture tubes werecontamined with fungal growths.
The sequence of events in the development ofthe skin lesions on patient B.D., and the causal rela-tionship with the outbreak of kala-azar in his village,are outlined below:- in 1949 B.D. had kala-azar;- in 1976 he developed hypopigmented skin
lesions on the face and extremities;- in mid-1978 the lesions, in addition to spreading
to other parts of the body, transformed to thenodular type and some ulcerated;
- in July 1980 the outbreak of kala-azar was iden-tified in the village of Bandipur; and
- the longest duration of illness in the group ofpatients in the focus was 18 months, i.e., theoutbreak commenced early in 1979.
342 WHO Bulletin OMS. Vol 70 1992
Did post-kala-azar dermal leishmaniasis initiate kala-azar in West Bengal?
DiscussionIn India, kala-azar appears to occur in epidemicwaves that are interspersed with inter-epidemic per-iods of various durations (1, 2). In the absence of es-tablished animal reservoirs of L. donovani the originof each epidemic, with regard to the initial sourceof the parasite, is a cause for concem. Because of theready availability of the parasites in the skin, particu-larly in patients with the nodular type of the disease(10), cases of PKDL have been suspected to have thegreatest potential for maintaining L. donovani duringinter-epidemic periods (2). Except for a study byShortt et al. (11), which included cases of PKDL, allother studies of the transmission of kala-azar in Indiahave involved active untreated or drug-failure cases(12-14). Shortt et al. investigated whether there weredifferences in the biological behaviour in the sandflyvectors of isolates from patients with kala-azar andPKDL (11). While demonstration of the transmissionpotential of visceral leishmaniasis has relevance tothe spread of kala-azar in India during kala-azar epi-demics, it would be more important to identify thereservoir during inter-epidemic periods. Although ithas been discussed, there has been no attempt toimplicate cases of PKDL as the initial source ofparasite for a particular outbreak of kala-azar.
The current epidemic of kala-azar was firstobserved in districts in north Bihar early in 1970,and gradually spread to adjacent districts as well asto Katihar and Pumia districts in south Bihar. Theepidemic spread continuously as well as discon-tinuously through population migrations. Althoughthe source of the parasite in the first outbreak innorth Bihar in 1970 is still unknown, the transmis-sion during the epidemic period was probably person-to-person from active cases of kala-azar.
Two independent foci of kala-azar were identi-fied in West Bengal in mid-1980. The outbreak atHarishchandrapur in Malda district was a result ofa direct extension from Katihar in Bihar (8).cHowever, a meticulous investigation of the outbreakin 24-Parganas failed to yield any evidence of spreadfrom known active kala-azar foci. The continuouspresence of a particular case of PKDL in the villagedating from long before the outbreak then arousedthe suspicion that this individual may have played arole in the local kala-azar outbreak. Our findingsconfirmed the ability of cases of PKDL to infectsandflies artificially, indicating that similar infectioncould occur under natural conditions. Clearly thisevidence does not prove that the case of PKDL inBandipur (B.D.) was the source of the L. donovani
c See footnote a, p. 341.
parasites for the outbreak in 24-Parganas. The fol-lowing evidence, however, strongly suggests involve-ment of a local source of PKDL in initiating theoutbreak: the presence of numerous amastigotes inskin nodules; the infectivity of the case; the avail-ability of P. argentipes in the village (15); the pres-ence of the patient in the same village prior to theoutbreak; and the absence of population exchangewith other ongoing epidemic foci. Although the out-break was first confirmed in 1980, the clinical mani-festations dated back to early 1979. Since PKDL is atits maximum infectivity at the nodular stage (whichB.D. developed in mid-1978), the incubation periodof the focus was well within the accepted limit.
The serological similarity between the strains ofvisceral leishmaniasis and PKDL indicated that theparasite causing the original visceral infection wasalso responsible for PKDL (16). Isoenzyme charac-terization of isolates from Indian cases of PKDL,obtained from the Calcutta School of TropicalMedicine, were indistinguishable from those of In-dian kala-azar (zymodeme, LON-41) (17). Further-more, inoculations of parasites isolated from thelesions of cases of PKDL have the ability to causekala-azar, as indicated by the occurrence of visceralleishmaniasis in model experiments involvinghamsters and mice (18-21).
That population exchange played a decisive rolein the intra-epidemic spread of kala-azar was clearlyevident from the subsequent extension of the focusto other areas inhabited by the local tribal communi-ty in the same as well as in several other districts (9).It is extremely difficult to prove definitively that agiven case of PKDL was responsible for a particularoutbreak in the absence of a follow-up study tracingcases of PKDL in subsequent outbreaks. The fin-dings of a further prospective study (in preparation),i.e., the development and occurrence of PKDLbetween two outbreaks of visceral leishmaniasis, fur-ther strengthen the evidence implicating its role ininitiating fresh transmission of kala-azar.
The high death rate of the blood-fed flies earlyin the post-feeding period is difficult to explain.Although some of the flies exhibited promastigoteson the third post-feeding day, the highest rate ofinfection occurred after the fourth post-feeding day.
It should be noted that despite their positivetransmission potential and continued presence inCalcutta, the three other cases of PKDL in the studydid not pose any problem, perhaps because of theabsence of P. argentipes vectors in the city.
From the above discussion, it can be concludedthat, under the epidemiological circumstances thatprevail in India, cases of PKDL might play animportant role as reservoirs of kala-azar, particularlyin inter-epidemic periods, and given an appropriate
WHO Bulletin OMS. Vol 70 1992 343
M. Addy & A. Nandy
Table 1: Parasite development In the laboratory-bred Phlebotomus argentipes fed on four patients with post-kala-azar dermal leishmaniasis on different occasions
No. of flies:
No. of days Dissected No. with promastigotes:post-feeding Fed/used Live, fed Died + embedded in paraffin Wet smear Histology Total
0 104/400 104 - - - -1 - 104 19 - - -2 - 85 12 - - -
3 - 73 3 10+2 5 1 64 - 58 10 15+3 5 1 65 - 30 0 17+4 1 1 2 136 - 9 0 7+2 6 1 7
Total 400 104 (26)8 44 (42.3) 49+11 27 5 32 (53)
8 Figures in parentheses are the percentages of the totals in the preceding column. For promastigotes, the figure in parentheses is thepercentage of the total number of flies that were dissected and embedded in paraffin.
Fig. 2. Dissected mid-gut of an infected Phlebotomusargentipes sandfly, showing (a) clusters of refractilemotile promastigotes (arrow) In a saline preparation(bright-field microscopy, X400); and (b) paraffin-embed-ded section (haematoxylin-eosin stained) of anotherInfected P. argentlpes showing an Individual promasti-gote (arrow) with long flagellum (X 1000).
density of vectors, susceptible human populationsand suitable environmental factors, may initiate anoutbreak of visceral leishmaniasis. Therefore in theabsence of demonstrable animal reservoirs of L.donovani in India, it is important to provide adeq-uate surveillance of cases of PKDL to control effec-tively future outbreaks of kala-azar in the country.
AcknowledgementsWe thank Dr T.N. Ghosh, Department of Protozoology,and Dr K.K. Mallik, Department of Tropical Medicine,Calcutta School of Tropical Medicine. We are also gratefulto Professor B.D. Chatterjee, Director, Calcutta School ofTropical Medicine, for permission to publish this paper.Financial support provided by the Department of Scienceand Technology, Government of West Bengal, is also ack-nowledged.
Resume
Dix ans de kala-azar au Bengale-Occidental, Partie 1. La leishmaniose post-kala-azar a-t-elle d6clench6 l'6pid6miedans le 24-Parganas?Apres une periode silencieuse d'environ 20 ans,le kala-azar a fait sa reapparition en Inde sousforme epidemique dans le nord de l'Etat de Biharen 1970, et s'est progressivement etendu nonseulement aux autres parties de cet Etat, mais6galement, en 1980, au district de Malda, nordde l'Etat voisin du Bengale-Occidental.Simultanement, un autre foyer independant de
B .. .:r..... ..
:SF :-yp
.s
X.:S }. j,jjj.. e ... .. 3_
j _ _. .:_Y 5 FS rF #= _= j
____a -__
S,SS :i. : _rS ll _FF |_
** _!
WHO Bulletin OMS. Vol 70 1992344
Did post-kala-azar dermal leishmaniasis initiate kala-azar in West Bengal?
kala-azar a ete reconnu en 1980 a Bandipur, vil-lage du district de 24-Parganas dans le sud duBengale-Occidental. En I'absence de tout ph6no-mene migratoire et de toute communication avecun foyer d'end6mie connu, l'origine du parasitedans l'6pidemie de Bandipur est restee obscure(de meme que dans le cas de I'epid6mie du norddu Bihar), jusqu'a la decouverte d'un sujet atteintde leishmaniose cutanee post-kala-azar (PKDL)ayant longtemps resid6 a Bandipur avant led6clenchement de I'epid6mie.
En I'absence de r6servoir animal connu deLeishmania donovani en Inde, on soupconnedepuis longtemps les cas de PKDL d'entretenir leparasite pendant les p6riodes interepid6miques etd'etre a l'origine de la reprise de la transmissiondu kala-azar. On a donc r6alis6 une 6tude afind'6valuer I'aptitude du sujet atteint de PKDL atransmettre L. donovani a des phl6botomes(Phlebotomus argentipes) elev6s en laboratoireet, ainsi, a se comporter comme source localed'infestation. L'6tude comportait 6galement troiscas de PKDL provenant d'autres regions.
Sur les 400 femelles de P. argentipes utili-s6es pour l'6tude, 104 se sont nourries sur lesmalades; elles ont ete incub6es et 44 sontmortes dans les 48 heures suivant le repas desang. Sur les 60 autres, 32 ont ete trouves infes-t6es par L. donovani (pr6sence de promastigotesdans le mesent6ron). Ces r6sultats confirmentdonc l'aptitude des cas de PKDL, notamment dela vari6t6 nodulaire, a transmettre l'infestation ades phl6botomes dans des conditions exp6rimen-tales.
Au vu de ces r6sultats, le malade atteint dePKDL a e fortement soupqonn6 d'avoir servi depoint de d6part de l'epid6mie de kala-azar aBandipur. Cette hypothese a et6 encore renfor-c6e par les faits suivants: pr6sence d'amastigotesen grand nombre dans les nodules cutanes dumalade; infectiosite considerable du malade pourles phl6botomes; s6jour continu du malade dansle village avant l'epid6mie; absence de communi-cation avec tout foyer end6mique connu de kala-azar; similitude entre les parasites responsablesdu kala-azar et de la PKDL; existence de popula-tions vectrices et humaines sensibles au momentde la transmission.
Ces r6sultats laissent a penser que dans lasituation 6pid6miologique qui pr6vaut en Inde, lescas de PKDL pourraient jouer un r6le importantdans le maintien du reservoir de L. donovani pen-dant les p6riodes interepid6miques et etre a l'ori-gine des flambees ult6rieures de kala-azar. Pour6viter de nouvelles flamb6es dans le pays, il fau-dra exercer une surveillance appropri6e afin de
diagnostiquer et traiter les cas de PKDL, defagon a 6liminer la source du parasite dans lacommunaute.
References1. Moleneux, D.H. & Ashford, R.W. Visceral leish-
maniasis. In: The biology of Trypanosoma andLeishmania parasites of man and domestic animals,1st edition. London, Taylor & Francis, 1983, pp.211-227.
2. WHO Technical Report Series, No. 701, 1984 (TheLeishmaniases: report of a WHO ExpertCommittee).
3. Sen Gupta, P.C. Post-kala-azar dermal leishmania-sis. In: Scientific reports of Instituto Superiore diSanita, vol. 2. Amsterdam, Elsevier, 1962, pp.124-130.
4. Sen Gupta, P.C. Leishmaniasis in India. Journal ofthe Indian Medical Association, 50: 34-36 (1968).
5. Bhattacharyya, A. & Ghosh, T. N. A search forLeishmania in vertebrates from kala-azar-affectedareas of Bihar, India. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 77:874-875 (1983).
6. Prasad, L.S.N. et al. Studies on kala-azar. In:Proceedings of the Indo-UK Workshop onLeishmaniasis, Patna, 6-10 December 1982. NewDelhi, Indian Council of Medical Research, 1983,pp. 119-121.
7. Ramalingaswami, V. Welcome address. In: Pro-ceedings of the Indo-UK Workshop on Leishmaniasis,Patna, 6-10 December 1982. New Delhi, IndianCouncil of Medical Research, 1983, pp. 1-2.
8. Chowdhury, A.B. Recent resurgence of kala-azarin West Bengal. In: Proceedings of the Indo-UKWorkshop on Leishmaniasis, Patna, 6-10 December1982. New Delhi, Indian Council of MedicalResearch, pp. 10-19.
9. Nandy, A. et al. Current situation of visceral leish-maniasis in India, with special reference to WestBengal. In: Proceedings of the InternationalWorkshop on Research on Control Strategies forthe Leishmaniases, Ottawa, 1-4 June 1987 Ottawa,IDRC/CRDI/CIID, 1988, pp. 8-15.
10. Sen Gupta, P.C. Observations on post-kala-azardermal leishmaniasis. Revista Brasileira de malario-logia, 8: 175-186 (1956).
11. Shortt, H.E. et al. Note on dermal leishmaniasis.Indian journal of medical research, 16: 239-240(1928).
12. Knowles, R. et al. On a Herpetomonas found in thegut of the sandfly, Phlebotomus argentipes, fed on akala-azar patient. Indian medical gazette, 59:593-597 (1924).
13. Shortt, H.E. et al. A note on a massive infection ofthe pharynx of Phlebotomus argentipes withHerpetomonas donovani. Indian medical researchmemoirs, 4: 157-160 (1926).
14. Das Gupta, B. et al. Experiments with the sandflyPhlebotomus argentipes. Bulletin of the CalcuttaSchool of Tropical Medicine, 3: 168 (1955).
WHO Bulletin OMS. Vol 70 1992 345

M. Addy & A. Nandy
15. Hati, A.K. Current status of leishmaniasis vectorbiology. In: Proceedings of the Indo-UK Workshopon Leishmaniasis, Patna, 6-10 December 1982.Indian Council of Medical Research, New Delhi,1983, pp. 84-91.
16. Bray, R.S. et al. Studies on the immunology andserology of leishmaniasis: IX. Serological investiga-tion of the parasites of Indian kala-azar and Indianpost-kala-azar dermal leishmaniasis. Transactions ofthe Royal Society of Tropical Medicine and Hygiene,67: 125-129 (1973).
17. Le Blancq, S.M. & Peters, W. Leishmania in theOld World: 4. The distribution of L.donovani sensulato zymodemes. Transactions of the Royal Society
of Tropical Medicine and Hygiene, 80: 367-377(1986).
18. Das Gupta, B.M. A note on the parasite of "dermalleishmanoid". Indian medical gazette, 62: 11-12 (1927).
19. Das Gupta, B.M. Further observations upon "dermalleishmanoid". Indian medical gazette, 62: 199(1927).
20. Das Gupta, B.M. On the differentiation ofLeishmania tropica from the parasite of dermalleishmanoid. Indian journal of medical research, 18:105-108 (1930).
21. Acton, H.W. & Napier, L.E. Post-kala-azar dermalleishmaniasis. Indian journal of medical research,15: 97-106 (1927).
346 WHO Bulletin OMS. Vol 70 1992


















