K2 HS Female Reproductive System
80
Do I REALLY Need Histology to be A Doctor?
-
Upload
monika-ayuningrum -
Category
Documents
-
view
215 -
download
1
description
Slide Kuliah Reproduksi Wanita
Transcript of K2 HS Female Reproductive System

Do I REALLY Need Histology to
be A Doctor?



Female Reproductive SystemHistology Department

IntroductionSix major functions :
1. Production of female gametes, the ova2. Reception of male gametes, the spermatozoa3. Provision of a suitable environment for
fertilization of ova by spermatozoa4. Provision of an environment for development of
the fetus5. A means for expulsion of developed fetus to the
external environment6. Nutrition of the newborn

Three structural units on the basis of function:1. The ovaries2. The genital tract3. The breasts

Introduction• INTERNAL PARTS :
– OVARIES– OVIDUCT– UTERUS– VAGINA
• EXTERNAL PARTS :– OPENING OF THE VAGINA– LABIA (MAJORA & MINORA)– VESTIBULE – CLITORIS– NOTE : ALTHOUGH NOT GENITAL ORGANS, THE
MAMMARY GLANDS ARE IMPORTANT ACCESSORY ORGANS OF THE FEMALE REPRODUCTIVE TRACT.
• ANATOMICAL INTEGRATION FOR REPRODUCTION
FERTILIZATION AND DEVELOPMENT
DELIVER AND EXIT

Picture taken from Basic Histology Text & Atlas , 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.

Ovary • GROSS ANATOMY:
– PAIRED OVAL BODIES THAT LIE ON EACH SIDE OF THE UTERUS
• 2 DISTINCT ANATOMICAL REGIONS:– COVERED BY A MESOTHELIUM THAT CONTINUOUS
With MESOVARIUM SQUAMOUS CELLS BECOME CUBOIDAL AND FORM THE SURFACE EPITHELIUM OF THE OVARY = GERMINAL EPITHELIUM (OLD TERM)
– MEDULLARY-HIGHLY VASCULAR, CT, LYMPHATICS AND NERVES
– CORTEX-FOLLICLES, CT, AND SOME SMOOTH MUSCLE
– TUNICA ALBUGINEA TO SEPARATE EPITHELIUM FROM CORTEX

Histology of Ovary
Part of an ovary with cortical &
medullary regions. H&E stain.
Low magnification
Picture taken from Basic Histology Text & Atlas , 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.

ERDS & LDL
Low mag - entire ovary
CL – Corpus luteum; F – Follicles; H = Hilus; L – Ligament; M - medulla

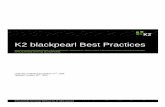
Cortical region of an ovary • Ovary surrounded by germinal
epithelium & by tunica albuginea • Groups of primordial follicles, each
formed by an oocyte surrounded by a layer of flat follicular cells, are present in the ovarian connective tissue (stroma).
• Giemsa stain. Low magnification.
Picture taken from Basic Histology Text & Atlas , 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.

Ovarian Surface epithelium Neoplasm

Follicles development

Ovarian follicle

Primordial follicles
• Located in the cortex just beneath tunica albuginea.
• One layer of flattened follicular cells surround the oocyte (about 30 µm in diameter).
• The nucleus of the oocyte is positioned eccentric in the cell. – It appears very light and contains a
prominent nucleolus.– Most organelles of the oocyte aggregate in
the centre of the cell, where they form the vitelline body (probably not visible in any of the available preparations).

Pararosaniline–toluidine blue (PT) stain. Low magnification.
Picture taken from Basic Histology Text & Atlas, 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.
Formed by: an oocyte &
one layer of cuboidal
granulosa cells
Formed by:An Oocyte & flat follicular
cells
ERDS & LDL
Primordial Follicles
Primary Follicle
Primordial Follicles
Primary Follicle

The primary follicle
• The first morphological stage that marks the onset of follicular maturation
• The previously flattened cell surrounding the oocyte now form a cuboidal or columnar epithelium surrounding the oocyte.
• Cytoplasm may have a granular appearance (granulosa cells). • The continued proliferation of these cells will result in the
formation of a stratified epithelium (with a distinct basement membrane) surrounding the oocyte.
• The zona pellucida (glycoproteins between interdigitating processes of oocyte and granulosa cells) becomes visible.
• Parenchymal cells of the ovary surrounding the growing follicle become organised in concentric sheaths, the theca folliculi.

ERDS & LDL
Late primary Follicle
Oocyte
Zona Pellucida
Stratified Follicular Epithelium
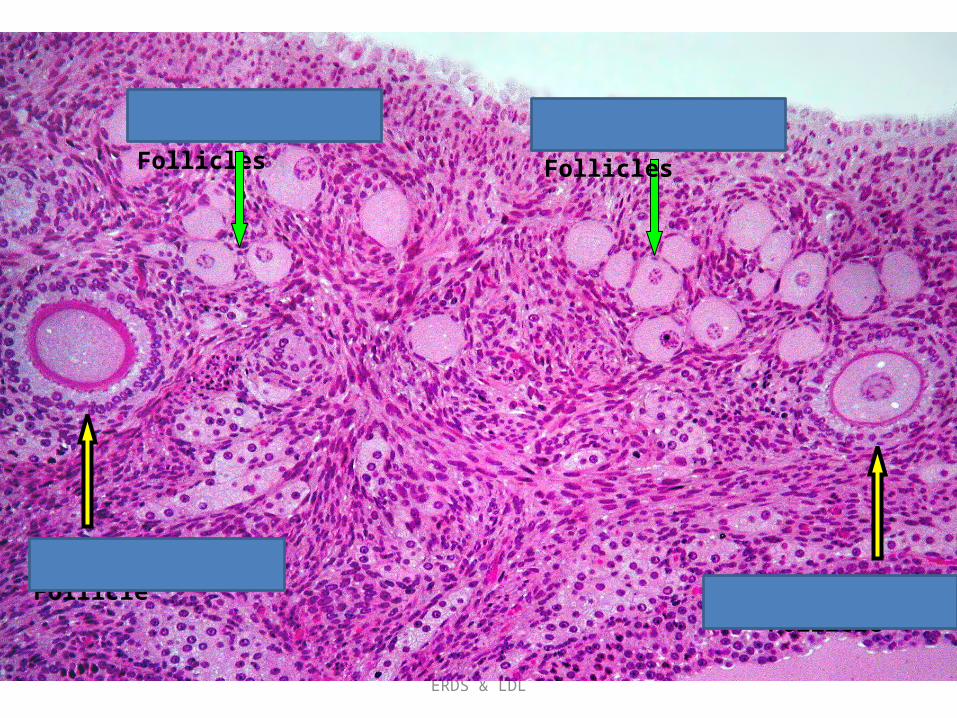
Secondary follicle • Small fluid-filled spaces become visible between the granulosa cells as the follicle
reaches a diameter of about 400 µm. • These spaces enlarge and fuse to form the follicular antrum (the defining feature
of the secondary follicle). • The oocyte is now located eccentric in the follicle in the cumulus oophorus, where
it is surrounded by granulosa cells. • The theca folliculi differentiates with the continued growth of the follicle into a
theca interna and a theca externa. – Vascularization of the theca interna improves
– The spindle-shaped or polyhedral cells in this layer start to produce oestrogens.
– The theca externa retains the characteristics of a highly cellular connective tissue with smooth muscle cells.
• The oocyte of the secondary follicle reaches a diameter of about 125 µm.• The follicle itself reaches a diameter of about 10-15 mm.

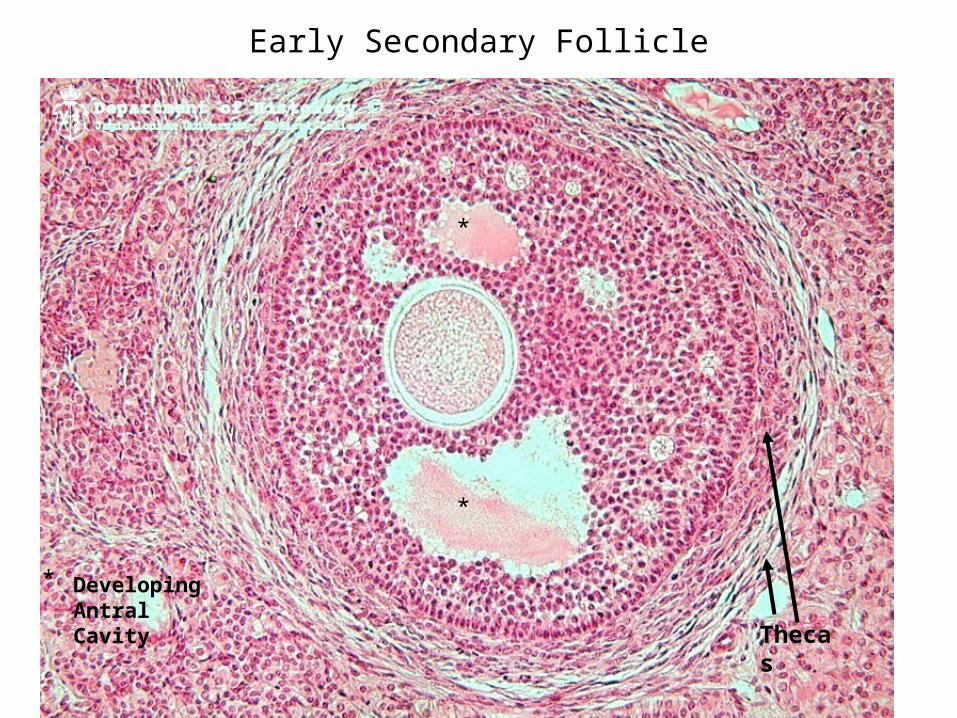
An antral follicle: • Oocyte surrounded by granulosa cells of
corona radiata & supported by cumulus oophorus.
• The remaining granulosa cells form wall of follicle & surround large antrum.
• A theca surrounds the whole follicle.
A small part of wall of antral follicle: • Antrum• Granulosa cells• Thecas interna & externa• A basement membrane
separates the granulosa layer from the theca interna.
PT stain. High magnification.
ERDS & LDL
Early Secondary Follicle
Developing Antral Cavity
*
*
*
Thecas

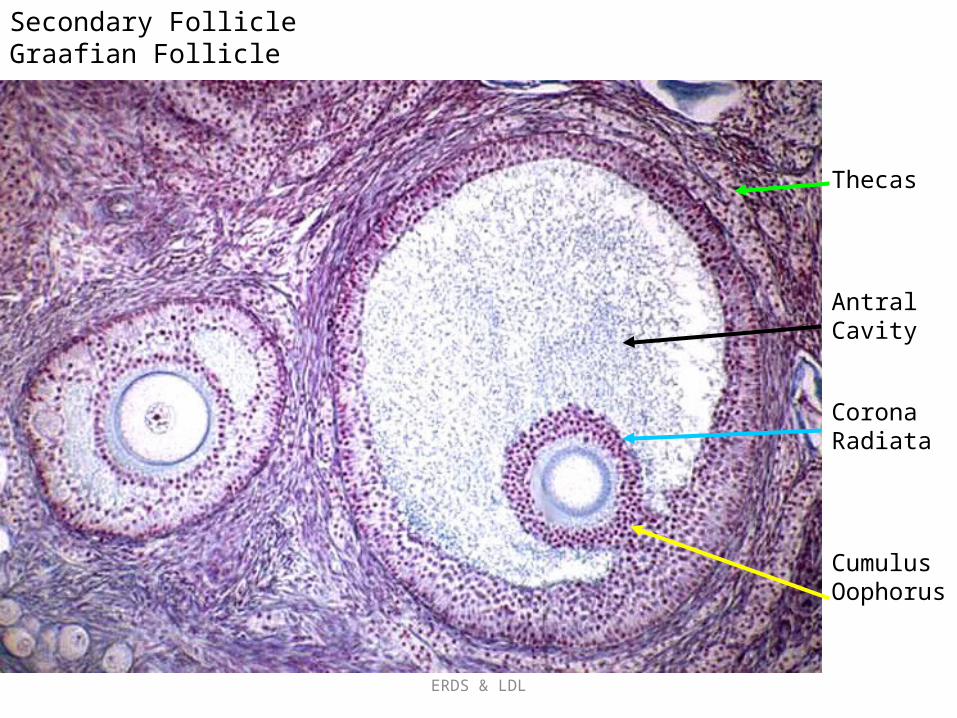
Mature or tertiary or preovulatory or Graafian follicle
• Increases further in size (in particular in the last 12h before ovulation).
• The Graafian follicle forms a small "bump" on the surface of the ovary, the stigma (or macula pellucida). – The stigma is characterised by a thinning of the
capsule and a progressive restriction of the blood flow to it.
• Prior to ovulation the cumulus oophorus separates from the follicular wall.
• The oocyte : floating freely in the follicular antrum. – It is still surrounded by granulosa cells which
form the corona radiata. • The follicle finally ruptures at the stigma and
the oocyte is released from the ovary
ERDS & LDL
Secondary Follicle Graafian Follicle
Thecas
Antral Cavity
Corona Radiata
Cumulus Oophorus

ERDS & LDL
Corona Radiata Zona Pellucida Cumulus Oophorus Theca Interna
Oocyte
High Mag –Graafian Follicle
Atresia • Atresia is the name for the degenerative process by which
oocytes (and follicles) perish without having been expelled by ovulation.
• Only about 400 oocytes ovulate - about 99.9 % of the oocytes that where present at the time of puberty undergo atresia.
• Atresia may effect oocytes at all stages of their "life" - both prenatally and postnatally.
• By the sixth month of gestation about 7 million oocytes and oogonia are present in the ovaries.
• By the time of birth this number is reduced to about 2 million. Of these only about 400.000 survive until puberty.
• Atresia is also the mode of destruction of follicles whose maturation is initiated during the cyclus (10-15) but which do not ovulate.
• Atresia is operating before puberty to remove follicles which begin to mature during this period (none of which are ovulated).
• Given that atresia affects follicles at various stages of their development it is obvious that the process may take on quite a variety of histological appearances

Characteristic of FOLLICLE ATRESIA
1. Loss of cells of corona radiata2. Oocyte floating free
within antrum
3. Death of granulosa cells, many of which are seen
loose in antrum
PT stain. Medium magnification
Picture taken from Basic Histology Text & Atlas , 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.
The Corpus luteum• The wall of the follicle collapses into a folded structure
(characteristic for the corpus luteum). • Vascularization increases • Connective tissue network is formed. • Theca interna cells and granulosa cells triple in size and
start accumulating lutein within a few hours after ovulation (granulosa lutein cells and theca lutein cells and produce progesterone and oestrogens)
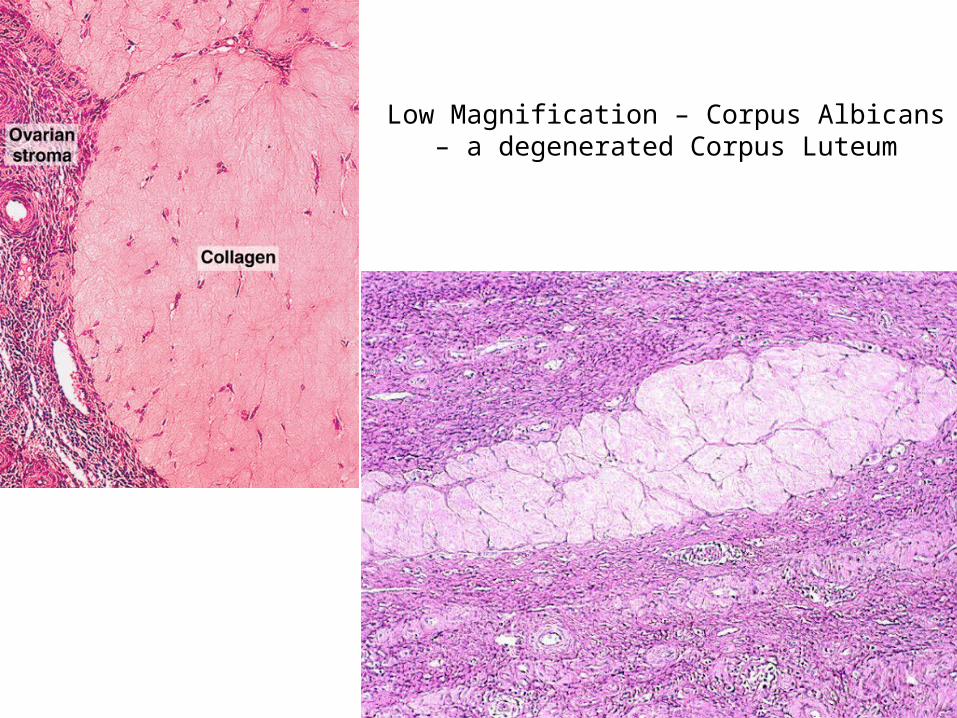
• Hormone secretion in the corpus luteum ceases within 14 days after ovulation if the oocyte is not fertilised (the corpus luteum degenerates into a corpus albicans - whitish scar tissue within the ovaries).
• Hormone secretion continues for 2-3 month after ovulation if fertilisation occurs.

ERDS & LDL
Low Magnification – Ovary with a number of Corpus Luteum (CL)
CL
CL
CL
CL
Arrow = Secondary Follicle

ERDS & LDL
Human Corpus Luteum

Corpus luteum

Corpus Luteum


Corpus Luteum Corpus albicans
ERDS & LDL
Low Magnification – Corpus Albicans – a degenerated Corpus Luteum

Oviduct • Functions : as a conduit for the oocyte, from
the ovaries to the uterus. • Histologically :
– the oviduct consists of :• a mucosa and a muscularis. • The peritoneal surface of the oviduct is lined by a
serosa and subjacent connective tissue.

Oviduct • The mucosa
– Is formed by a ciliated and secretory epithelium resting on a very cellular lamina propria.
– The number of ciliated cells and secretory cells varies along the oviduct (see below).
– Secretory activity varies during the menstrual cycle, and resting secretory cells are also referred to as peg-cells.
– Some of the secreted substances are thought to nourish the oocyte and the very early embryo.
• The muscularis – Consists of an inner circular muscle layer and an outer
longitudinal layer. • An inner longitudinal layer is present in the isthmus and the
intramural part (see below) of the oviduct. • Peristaltic muscle action seems to be more important for the
transport of sperm and oocyte than the action of the cilia.

Oviduct • Four subdivisions of the oviduct :
1. The infundibulum : funnel-shaped (up to 10 mm in diameter) end of the oviduct. • Finger-like extensions of its margins, the fimbriae, are closely applied
to the ovary. • Ciliated cells are frequent. Their cilia beat in the direction of
2. the ampulla of the oviduct. • Mucosal folds, or plicae, and secondary folds which arise from the
plicae divide the lumen of the ampulla into a very complex shape. • Fertilization usually takes place in the ampulla.
3. The isthmus is the narrowest portion (2-3 mm in diameter) of the parts of the oviduct located in the peritoneal cavity. • Mucosal folds are less complex and the muscularis is thick. An inner,
longitudinal layer of muscle is present in the isthmus and the 4. Intramural part of the oviduct, which penetrates the wall of the uterus.
• The mucosa is smooth, and the inner diameter of the duct is very small.

ERDS & LDL
Low Magnification – The Ovary
and the Oviduct (Fallopian Tube)

Uterine Tube
Three layers:
• Mucosa
• Muskularis
• Serosa

Wall of an oviduct
• Highly folded mucosa indicates that this region is close to ovary.
• PT stain• Low magnification
Oviduct Epithelial• Ciliated cells
contribute to movement of oocyte or conceptus to uterus
• PT stain. • High magnification.
Picture taken from Basic Histology Text & Atlas , 10th edition, L. Carlos Junquira MD, Jose Carneiro MD, Robert O. Kelley PhD, Lange Medical Books, Mc Graw-Hill , 2003.

Oviduct

The Uterus
• The uterus is divided into 1. Body (upper two-thirds) and 2. Cervix
• The walls of the uterus are composed of a– Mucosal layer (the endometrium)– A fibromuscular layer (the myometrium). – The peritoneal surface of the uterus is covered
by a serosa

Phases on Menstrual CycleUTERUS


The Uterus
• Endometrium – Consists of a simple columnar epithelium
(ciliated cells and secretory cells) and an underlying thick connective tissue stroma.
– The mucosa is invaginated to form many simple tubular uterine glands.
– The glands extend through the entire thickness of the stroma.
– The stromal cells of the endometrium are embedded in a network of reticular fibres.
– The endometrium is subject to cyclic changes that result in menstruation. Only the mucosa of the body of the uterus takes part in the menstrual cycle
The Uterus • Endometrium
– The endometrium can be divided into two zones based on their involvement in the changes during the menstrual cycle: the basalis and the functionalis.• The basalis is not sloughed off during menstruation
but functions as a regenerative zone for the functionalis after its rejection.
• The functionalis is the luminal part of the endometrium. It is sloughed off during every menstruation and it is the site of cyclic changes in the endometrium. These cyclic changes are divided into a number of phases: proliferative (or follicular), secretory (or luteal), and menstrual.

The Uterus
• Myometrium – The muscle fibres of the uterus form layers
with preferred orientations of fibres (actually 4), but this is very difficult to see in most preparations.
– The muscular tissue hypertrophies during pregnancy, and GAP-junctions between cells become more frequent.


The surface epithelium & uterine glands are embedded in a lamina propria made of very loose connective tissue.PT stain. Medium magnification.
Straight uterine glands in deep endometrium during proliferative phase. Smooth muscle of myometrium is also seen. H&E stain. Medium magnification

Uterine glands during luteal phaseuterine glands become tortuous and their lumen is filled with secretions. Some edema is present in the connective tissue. H&E stain. Medium magnification. Inset: High magnification.

Reproductive Changes

Cervix
• TRANTITIONAL EPITHELIUM (T zone) GOES FROM SQUAMOUS (ectocervix) TO SECRETING (UTERINE GLANDS) COLUMNAR EPITHELIUM (endocervix).
• VISCOUS OF MUCUS GLANDS CHANGES WITH MENSTRUAL CYCLE
• MULTILAYERED:– MUCOSAL
• FOLDS OF STRATIFIED EPITH• NOT KERATINIZED BUT
KERATOHYALIN GRANULES MAY BE VISIBLE
• NO GLANDS BUT CELLS ARE HIGH IN GLYCOGEN
• MUCUS COMES FROM CERVICAL GLANDS
– MUSCULARIS-SMOOTH MUSCLE– ADVENTITIAL

Cervix in Woman’s Life

The cervix of a 14-year-old sexually active female.
Colpophotograph of the cervix of a 14-year-old
nonsexually active female

Cervix
Normal endocervix: epithelium composed of one layer of mucin secreting cells with few reserve cells (arrow).
Structure of the ectocervix: CT=connective tissue, BM=basement membrane, L1=basal cells (1 layer), L2=parabasal cells (2 layers), L3=intermediate cells (around 8 layers), L4=superficial cells (5 or 6 layers) and L5=exfoliating cells

Ectocervix
Structure of the ectocervix - details of basal, parabasal & intermediate layers: connective tissue, basal cells (one layer), parabasal cells (two layers), intermediate cells (some layers) with inter-cellular bridges. The N/C ratio of basal & parabasal cells is high
Structure of the ectocervix : details of the superficial layers : superficial cells (5 or 6 layers). The N/C ratio is very low and the axis of cells is parallel to the basement membrane

Transformation Zone
Transformation zone: normal squamous epithelium (red star), squamous metaplasia (green star) with some remaining endocervical cells (blue arrow)
Transformation zone: squamous epithelium islet in the endocervix area.
All cervix pictures downloaded from : http://screening.iarc.fr/atlasglossdef.php?key=Normal+endocervix&img

Different types of squamous cells - A: superficial cells (arrows); B: intermediate cells; C: parabasal cells; D: metaplastic cells. (obj. 20x)
Cervix Cells & pap’s smear

HSIL. (obj. 20x)
There is a cervical intraepithelial neoplasia
(CIN) 3 lesion at (1), and within the stroma there are infiltrating
malignant cells (2)

Vagina • The vagina is a fibromuscular tube with a wall consisting of three
layers: – Mucosa
• The stratified squamous epithelium (deep stratum basalis, intermediate stratum spinosum, superficial layers of flat eosinophilic cells which do contain keratin but which do not normally form a true horny layer) rests on a very cellular lamina propria (many leukocytes). Towards the muscularis some vascular cavernous spaces may be seen (typical erectile tissue).
– Muscularis • Inner circular and outer longitudinal layers of smooth muscle are present.
Inferiorly, the striated, voluntary bulbospongiosus muscle forms a sphincter around the vagina.
– Adventitia • The part of the adventitia bordering the muscularis is fairly dense and
contains many elastic fibres. Loose connective tissue with a prominent venous plexus forms the outer part of the adventitia.

Stratified squamous epithelium of vagina supported by a dense connective tissue. The cytoplasm of these epithelial cells is clear because of accumulated glycogen.PSH stain. Medium magnification.
Vagina

Female Accessory Reproductive Glands - Mammary Glands
• Mammary glands modified glands of skin (resembles that of sweat glands).
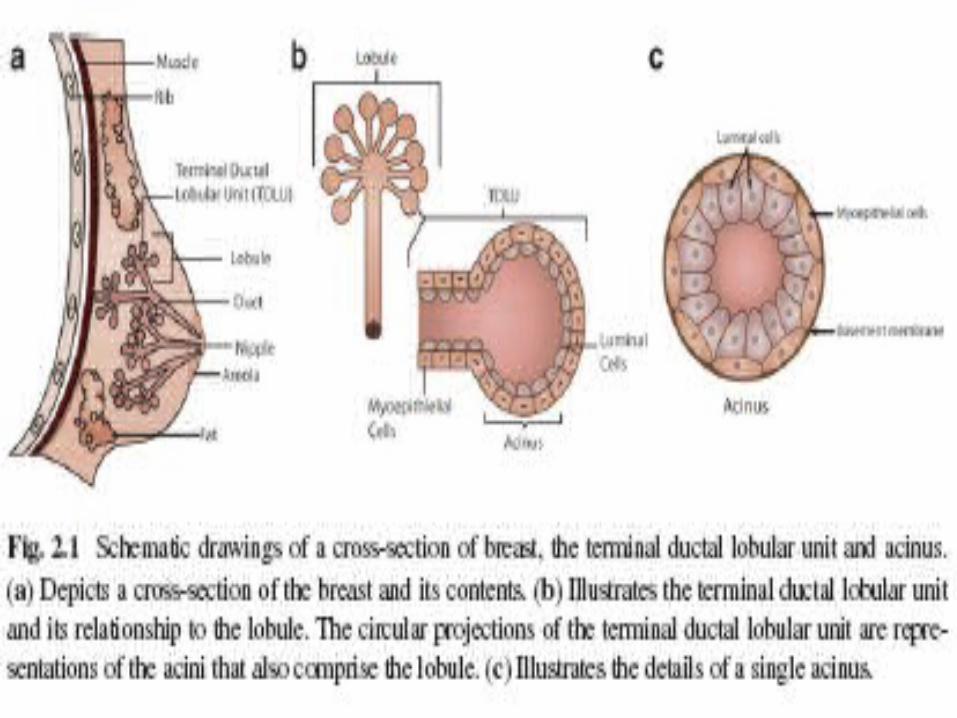
• Compound branched alveolar glands, which consist of 15-25 lobes separated by dense interlobar connective tissue and fat (Each lobe contains an individual gland)
• The excretory duct of each lobe, also called lactiferous duct, has its own opening on the nipple.
• The lactiferous duct has a two layered epithelium - basal cells are cuboidal whereas the superficial cells are columnar.
• Beneath the nipple, the dilated lactiferous duct forms a lactiferous sinus , which functions as a reservoir for the milk.
• Branches of the lactiferous duct are lined with a simple cuboidal epithelium.
• The secretory units are alveoli, which are lined by a cuboidal or columnar epithelium.
• A layer of myoepithelial cells is always present between the epithelium and the basement membrane of the branches of the lactiferous duct and the alveoli.

Breast in Woman’s Life

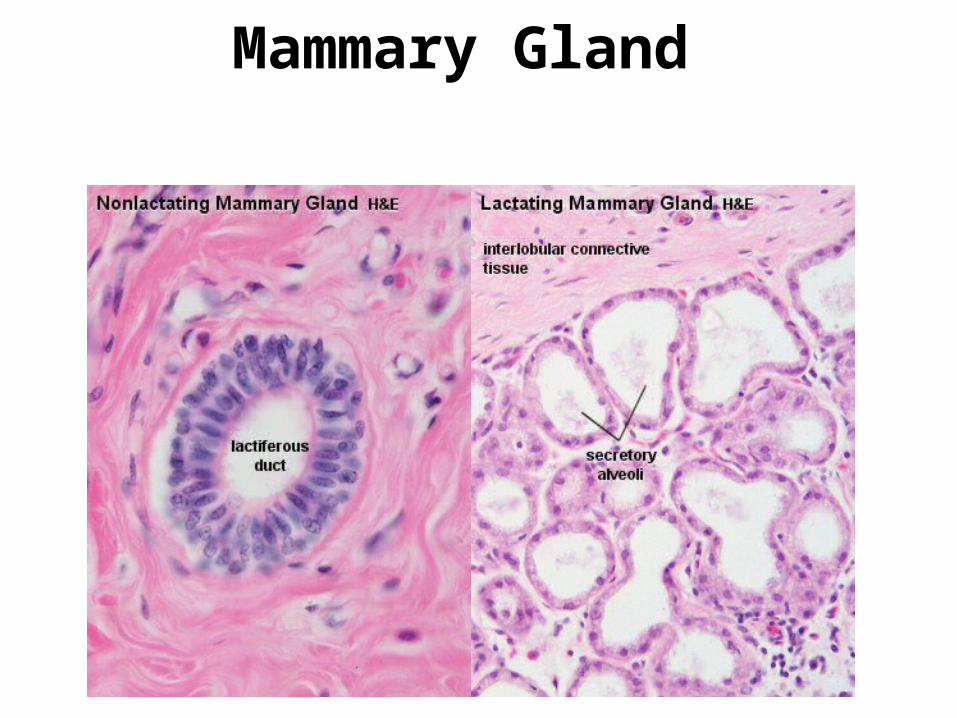
Mammary Gland

normal tdlu
Breast Cancer

Pregnancy
Fungsi Plasenta
Kata plasenta pertama kali digunakan oleh Realdus Columbus thn 1559• Transfer gas• Fungsi eksresi, keseimbangan air, pengaturan pH• Fungsi katabolisme & resorpsi• Fungsi sintesis & sekresi spt fungsi kelenjar endokrin• Sejumlah fungsi metabolik & sekresi yg dilaksanakan oleh hepar• Hematopoiesis dari sumsum tulang (pd awal kehamilan)• Fungsi penghantaran panas oleh kulit• Fungsi imunologis (masih belum dipahami seluruhnya)Mosman (1937) mendefenisikan plasenta sbg suatu penggabungan
membran fetus pd mukosa uterus yg bertujuan untuk pertukaran fisiologis
Fungsi plasenta:

Tahapan pembentuk
an plasenta:
1. Tahapan Fertilisasi
2. Tahapan Pembelahan zygot
3. Tahapan prelakunar 4. Tahapan lakunar
5. Tahapan perkembangan villi
Animasi

TAMPILAN PLASENTA NORMAL

Placenta

Potongan Tali Pusat Normal:
2 arteri & 1 Vena
Potongan T. Pusat Abnormal: single artery & single
vein

Umbilical Cord

Placenta• The placenta may be usefully understood as a
"parasite" feeding on blood from the endometrium (Imagine scooping out a portion of the endometrium).
• The resulting bowl will fill with blood from broken vessels in the endometrial stroma.
• Now lay a cover over the bowl, and imagine many "roots" extending down from the cover into the blood-filled hollow (the roots can absorb oxygen and nutrients from the blood in which they are bathed).

Placenta
• The cover is the chorionic plate of the placenta. • The "roots" are the chorionic villi.
– Both the placenta and the chorionic villi are entirely fetal tissue (orange in the diagram above).
– "Anchoring villi" attach the placenta to the endometrium. – Smaller branching villi extend out into the intervillous space. – Fetal circulation passes down the umbilical cord, though vessels in the villi, and back up
the umbilical cord. – Maternal blood "spills" from open endometrial arteries (the spiral arteries) into the
intervillous space (pink in the diagram above), and returns into endometrial veins. – The chorionic villi are surrounded and bathed by "lakes" of maternal blood. Within the
intervillous space, maternal blood is not contained by blood vessels– The surface of the chorionic villi is an epithelial layer, the fetal syncytiotrophoblast,
which has the ability to grow invasively into the maternal endometrium. The syncytiotrophoblast also has microvilli on the surface for absorbing nutrients from maternal blood.
– Beneath the syncytiotrophoblast (i.e., toward the core of the villus), is the cytotrophoblast, a layer of cuboidal cells which eventually disappear. (The cytotrophoblast also forms trophoblast columns, masses of cells filling the ends of anchoring villi.)
– Maternal endometrial stromal tissue adjacent to the placenta differentiates into large decidual cells (so named because the outer layer of the endometrium is shed at birth along with the placenta). Decidual cells may intermix with fetal cells in the cytotrophoblast. The boundary between maternal and fetal tissue is immunologically interesting.

Umbilical Cord• The umbilical cord is simply a conduit carrying fetal
blood between the fetus and the placenta. It normally contains two arteries and one vein, surrounded by extensive mesenchymal tissue ("Wharton's jelly").
• Consists of so-called "mucous" or mesenchymal connective tissue, also called Wharton's jelly (widely scattered mesenchymal fibroblasts within soft, jelly-like ground substance of hyaluronic acid and chondroitin sulfate)
• Surrounded by a thin stratified squamous epithelium and including typically two arteries and one vein. [The second vein in this image presumably represents one portion of a double U-shaped bend in this single vein.] The arteries lack internal and external elastic layers.