Juvenile Chronic Arthritis - library.up.ac.za fileXR Cartilage Primary: DIP PIP,hip,knee spine, 1...
42
Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK)
Transcript of Juvenile Chronic Arthritis - library.up.ac.za fileXR Cartilage Primary: DIP PIP,hip,knee spine, 1...

Juvenile Chronic Arthritis
Dr. Christa VisserMBChB MMed (Med Phys)
Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK)

Childhood Arthritis
• JCA/JIA/JRA
• Remember– Acute rheumatic fever– Juvenile connective tissue diseases eg SLE– Juvenile vasculitis
• Kawasaki syndrome• Henoch Schonlein purpura

XR
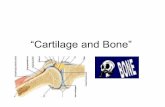
Cartilage
Primary: DIPPIP,hip,kneespine, 1 MTPSecondary:
OA
Synovial fluidXR
Urate level
CartilageSynoviumSoft tissue
Bone
GoutPseudogout
Crystal
RFXR
SynoviumJoints + C-spine
>> Systemic
RA
XRHLA B27
SynoviumEntheses
Axial + peripheraljoints>> systemic
ASPsoriatic
EnteropathicReactive
SpA
ANFENA
Organ Fx tests
SynoviumSystemic >>Synovium
SLEPSS
PM/DMMCTD
CTD
ANCAHistologyImaging
SynoviumSystemic >>Synovium
PAN,WegenersTakayasu,GCA etc
Vasculitis
Arthritis




• Example of the typical fever curve seen in systemic onset JCA.

• The rash of systemic onset JCA. Larger lesions becoming confluent are shown

• A 3-year-old with systemic onset JCA with pericardial effusion.

• Growth chart of a boy with systemic onset JCA.

• Iritis demonstrating cataract and irregular pupil secondary to posterior synechiae.

• A 6-year-old girl withpauciarticular onset JCA affecting her right knee. Her right leg is 3cm longer than her left leg.

• Pauciarticular onset JCA in the right ankle. A shorter leg length from the knee to the ankle is demonstrated.

• Pauciarticular onset JCA in the right ankle. The right foot is smaller, with underdevelopment of the right forefoot due to disuse.

• Pauciarticular JCA involving the left knee with overgrowth of the leg and widening of the epiphysis.

• An 8-year-old girl withpauciarticular onset JCA demonstrating destruction of both wrists, subluxationof the carpal bones and undergrowth of the ulnar styloids. There was a family history of psoriasis and she had a polyarticularcourse.

• An 11-year-old withseropositive JCA demonstrating the erosions at severalmetacarpophalangealjoints and carpal bone fusion in the wrist.

• An 8-year-old withpauciarticular JCA.Epiphysial destruction and undergrowth of the third MCP of the left hand are seen as well as overgrowth of the carpal bones of the right wrist compared to the left wrist. Also note the widened appearance of the third phalanges due toperiosteal new bone formation.

• A 12-year-old withseronegative polyarticularonset JCA since the age of 4 years. Note the asymmetry and obvious fusion and growth abnormalities of the right wrist compared to the left wrist.

• A 21-year-old with evidence of sacroiliitis on the left. There is left hip joint space narrowing

• Systemic onset JCA withpolyarticular course. Severe hip destruction and protrusion.

• A 19-year-old with bilateral heel pain since the age of 9 years.Sacroiliitis in the left SI joint

• Erosion in the right heel was noted 10 years after onset of heel pain (b).
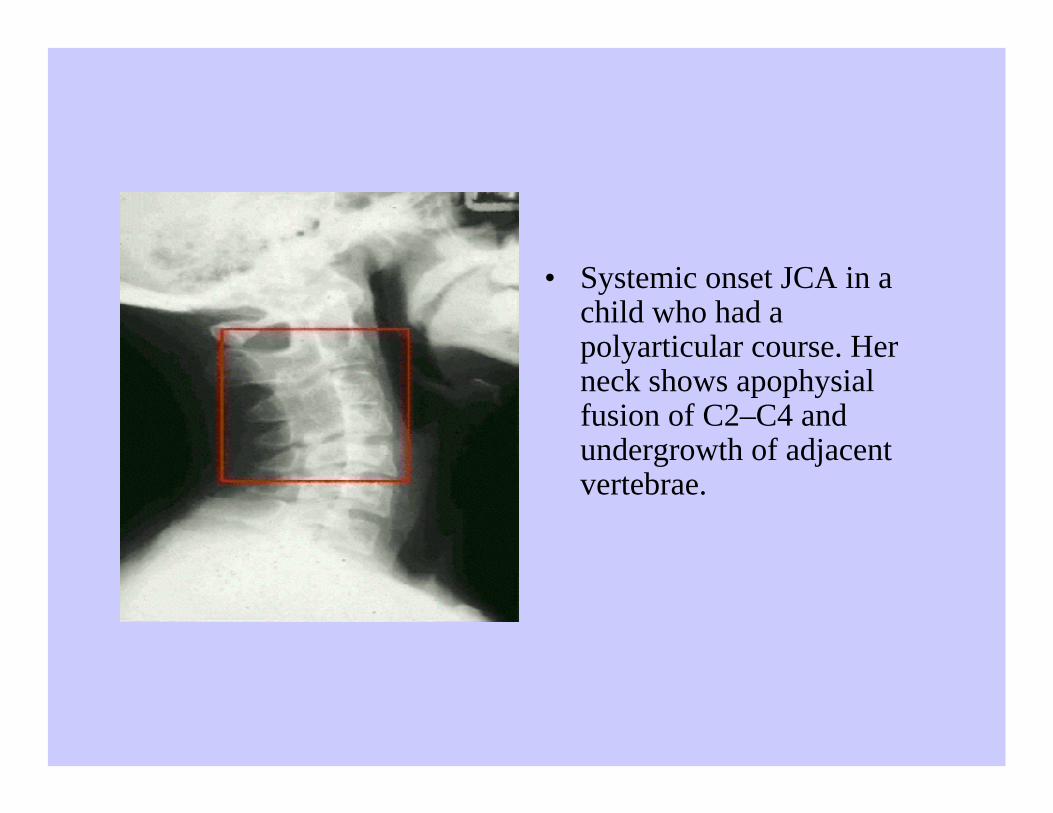
• Systemic onset JCA in a child who had apolyarticular course. Her neck shows apophysialfusion of C2–C4 and undergrowth of adjacent vertebrae.

• Severe erosions and joint space narrowing in systemic onset JCA of 10 years’ duration.




• Still’s rash. The faint salmon colored rash of Still’s disease. Moreerythematous eruptions may also be seen. Although the rash is most common on the trunk and upper extremities, it may also be seen on the face.


Acute Rheumatic fever
• An acute systemic inflammatory illness which usually occurs 2–4 weeks after group A b-hemolytic streptococcal infection of the pharynx.
• It appears to be related to a series of immunologicreactions to antigenic components of the streptococcus, which also crossreact with various human tissues, including heart muscle, valvularstructures, articular tissues and neuronal antigens.

Acute Rheumatic Fever: clinical features
• Characterized by fever, migrating arthritis, and destructive inflammatory lesions within the myocardium, endocardium, pericardium, heart valves, joints, periarticular regions, lungs, and subcutaneous tissues.
• Can be associated with chorea, when a profound functional motor disturbance of central nervous system activity may also be present transiently or persistently.


A 7-year-old girl with acute rheumatic fever and acute arthritis of the knee associated with obvious swelling and extreme pain on movement or weight-bearing. True to the usual rapid clinical evolution of such synovitis, in 2 days the knee pain was completely gone and the patient was running after her friends about the ward.

Typical rash oferythema marginatumin a child with acute rheumatic fever. The varying border and tendency to clear in the central zones of the lesions are typical.

Henoch Schonlein Purpura
• Polymorphonuclear inflammation of the vessel wall of small to medium-sized vessels which supply nutrients to the skin.
• Pathogenesis is presumed to be due to circulating immune complexes.
• It is a systemic disease process with variable manifestations in the skin, musculoskeletal, renal and gastrointestinal systems

Henoch Schonlein Purpura: Clinical Features
• Cutaneous involvement (palpable purpura) are most common.
• Systemic involvement – arthritis,glomerulonephritis, gastrointestinal hemorrhage or colic are most common.
• HSP is self-limiting.

Kawasaki Disease
• An acute febrile eruptive disease occurring most commonly in infants and children under 5 years of age.
• Vasculitis, especially involving coronary arteries, is a serious complication.
Kawasaki Disease: Clinical Features
• Fever of unknown etiology lasting 5 days or more.• Bilateral conjunctival congestion.• Dry and red lips, reddening of oral cavity.• Acute nonpurulent swelling of the cervical lymph
nodes.• Polymorphous exanthema of the trunk without
vesicles or crusts.• Red palms and soles.

Bleeding and crust formation on the lips and cervical lymphadenopathy in Kawasaki disease.

Membranous desquamation of the fingertips.

Polymorphous exanthema on the limbs and trunk of an infant with Kawasaki disease.