Just Culture: High Impact Case Studies
84
1 © 2018 TMIT March 15, 2018 Webinar Month 112 For resource downloads go to: www.safetyleaders.org Just Culture: High Impact Case Studies
Transcript of Just Culture: High Impact Case Studies
1 © 2018 TMIT
March 15, 2018 Webinar Month 112
For resource downloads go to: www.safetyleaders.org
Just Culture: High Impact Case Studies
2 © 2018 TMIT
Charles Denham, MD Chairman, TMIT TMIT High Performer Webinar March 15, 2018
Welcome
3 © 2018 TMIT
To optimize webinar sound volume, please check: o WebEx volume o Computer volume o External speaker volume
4 © 2018 TMIT
If you are still having difficulty hearing the webinar: Please click on Participants
If you are still having difficulty hearing the webinar: Please click on Participants
Then the “Request Phone”
button to receive a toll dial-in
5 © 2018 TMIT 5
6 © 2018 TMIT 6
7 © 2018 TMIT
If you wish to follow us on Twitter, go to: http://twitter.com/TMIT1 or use #safetyleaders hashtag
Also, go to: www.facebook.com/SafetyLeaders
and related sites
8 © 2018 TMIT
TMIT Purpose Statement Our Purpose: We will measure our success by how we protect and enrich the lives of families…patients AND caregivers. Our Mission: To accelerate performance solutions that save lives, save money, and create value in the communities we serve and ventures we undertake.
9 © 2018 TMIT
Disclosure Statement The following panelists certify: that unless otherwise noted below, each presenter provided full disclosure information; does not intend to discuss an unapproved/investigative use of a commercial product/device; and has no significant financial relationship(s) to disclose. If unapproved uses of products are discussed, presenters are expected to disclose this to participants. None of the participants have any relationship medication or device companies discussed in their presentations.
Outcome Engenuity, LLC was founded in 1997 by CEO David Marx, a pioneer of the Just Culture movement. The firm originally addressed safety issues and human factors in aviation and offered expertise in post-event investigation and analysis. With the unique combination of systems engineering, human factors, and the law, Marx adopted and expanded the concepts of ‘Just Culture’ to help improve the management of human error. He has nothing to disclose. Jennifer Dingman realized, after her mother’s death in 1995 due to errors in medical diagnoses and treatment, that there is little to no help available for patients and their families in similar situations. This life-changing experience left her feeling vulnerable, and she decided to dedicate her life to help prevent medical tragedies from happening to others. She has nothing to disclose. With 37 years in municipal and campus policing, William H. Adcox serves as the Chief of Police and CSO at The University of Texas MD Anderson Cancer Center and The University of Texas Health Science Center. Chief Adcox holds an MBA degree from UTEP and is a graduate of the PERF’s Senior Management Institute for Police and the Wharton School ASIS Program for Security Executives. He is the recipient of the IACLEA’s 2013 Award for Administrative Excellence and was named by Security Magazine as one of the “Most Influential People in Security 2013.” The agency received the IHSS Foundation’s prestigious 2015 Lindberg Bell Distinguished Program Award. Nationally, Chief Adcox received the Campus Safety 2015 Director of the Year Award in Healthcare; and locally he received the Texas Police Chiefs Association’s 2015 Leadership Award. He has nothing to disclose. Gregory H. Botz, MD, FCCM, is a professor in the Department of Critical Care at the UT MD Anderson Cancer Center. He received his medical degree from George Washington University School of Medicine in Washington, DC. He completed an internship in internal medicine at Huntington Memorial Hospital and then completed a residency in anesthesiology and a fellowship in critical care medicine at Stanford University in California. He also completed a medical simulation fellowship at Stanford with Dr. David Gaba and the Laboratory for Human Performance in Healthcare. Dr. Botz is board-certified in anesthesiology and critical care medicine. He is a Fellow of the American College of Critical Care Medicine. He has nothing to disclose. John J. Nance brings a rich and varied professional background to the task of helping doctors, administrators, boards, and front-line staff alike survive and prosper during the most profoundly challenging upheaval in the history of modern medicine. Having helped pioneer the renaissance in patient safety as one of the founders of the National Patient Safety Foundation in 1997, his efforts (and healthcare publications) are dedicated to reforming American healthcare from a reactive cottage industry to an effective and safe system of prevention and wellness. A lawyer, Air Force and airline pilot, prolific internationally-published author, national broadcaster, and renowned professional speaker, John’s leadership is propelled by a deep commitment. He has nothing to disclose. Charles Denham, MD, is the Chairman of TMIT; a former TMIT education grantee of CareFusion and AORN with co-production by Discovery Channel for Chasing Zero documentary and Toolbox including models; and an education grantee of GE with co-production by Discovery Channel for Surfing the Healthcare Tsunami documentary and Toolbox, including models. HCC is a former contractor for GE and CareFusion, and a former contractor with Siemens and Nanosonics, which produces a sterilization device, Trophon. HCC is a former contractor with Senior Care Centers. HCC is a former contractor for ByoPlanet, a producer of sanitation devices for multiple industries. He does not currently work with any pharmaceutical or device company. His current area of research is in threat management to institutions and continuing professional education and consumer education. Dr. Denham is a collaborator with Professor Christensen.

10 © 2018 TMIT
Speakers and Reactors
David Marx
Charles Denham Jennifer Dingman
John Nance Greg Botz
William Adcox
11 © 2018 TMIT
Voice of Patient and Family
Jennifer Dingman Founder, Persons United Limiting Sub-standards and Errors in Healthcare (PULSE), Colorado Division Co-founder, PULSE American Division TMIT Patient Advocate Team Member Pueblo, CO TMIT High Performer Webinar March 15, 2018
12 © 2018 TMIT
Charles Denham, MD Chairman, TMIT TMIT High Performer Webinar March 15, 2018
In the News Update and February 2018 Webinar National Survey
© 2006 HCC, Inc. CD000000-0000XX 13 © 2018 TMIT
In the News: Active Shooter Events
Source: http://abcnews.go.com/US/18-school-shootings-us-year-group/story?id=53091125
© 2006 HCC, Inc. CD000000-0000XX 14 © 2018 TMIT
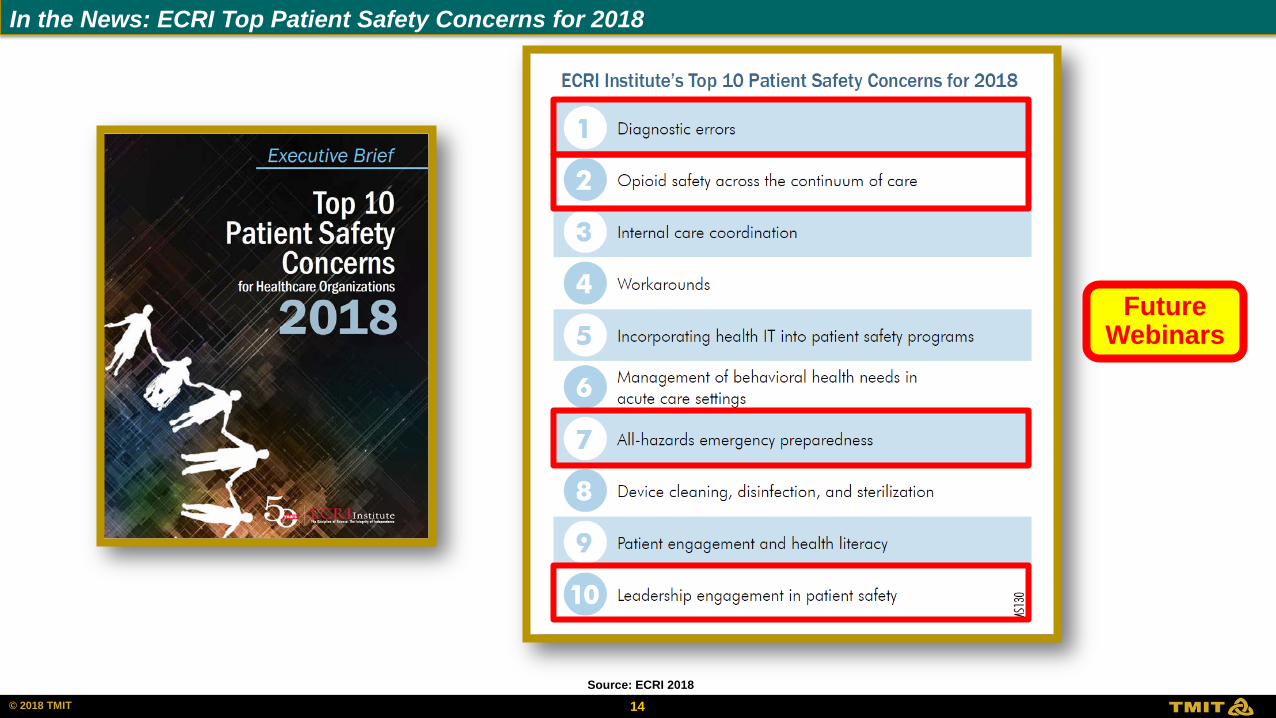
In the News: ECRI Top Patient Safety Concerns for 2018
Source: ECRI 2018
Future Webinars
© 2006 HCC, Inc. CD000000-0000XX 15 © 2018 TMIT
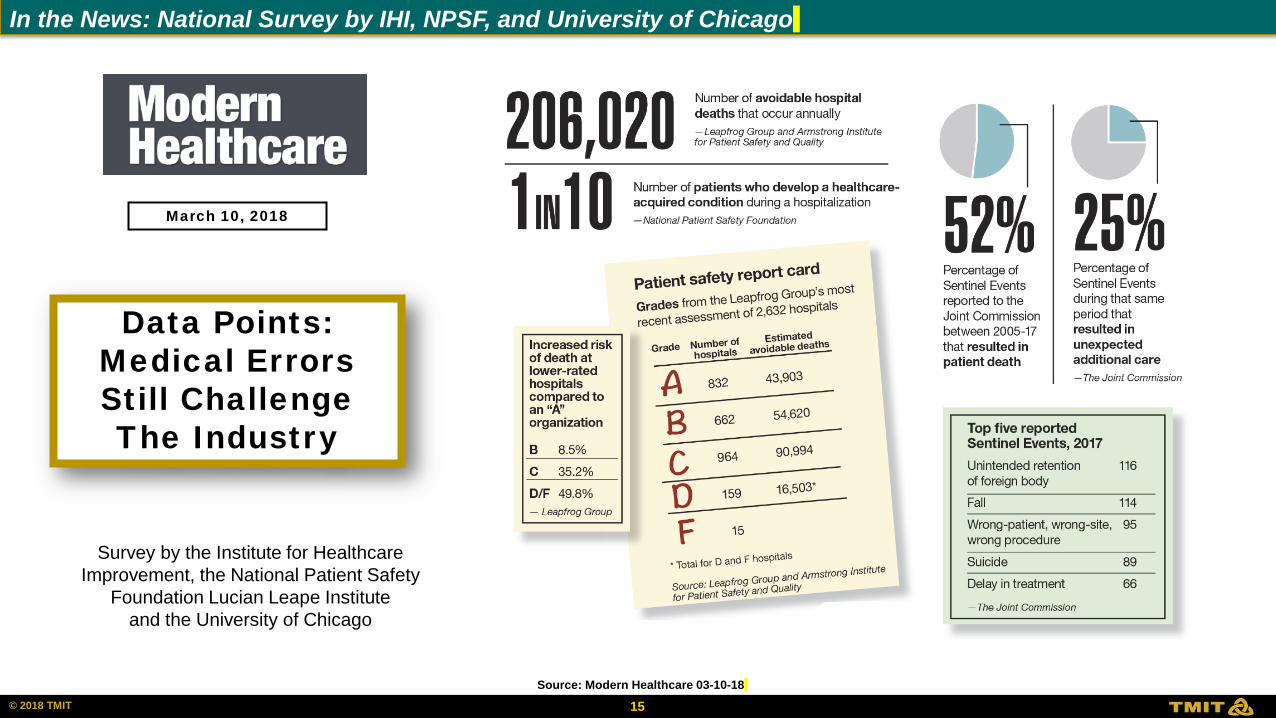
In the News: National Survey by IHI, NPSF, and University of Chicago
Source: Modern Healthcare 03-10-18
Data Points: Medical Errors Still Challenge The Industry
March 10, 2018
Survey by the Institute for Healthcare Improvement, the National Patient Safety
Foundation Lucian Leape Institute and the University of Chicago
© 2006 HCC, Inc. CD000000-0000XX 16 © 2018 TMIT
In the News: Politico Report on E.H.R. for Active Military and VA
Source: Propublica & United Press International
March 7-8, 2018
© 2006 HCC, Inc. CD000000-0000XX 17 © 2018 TMIT
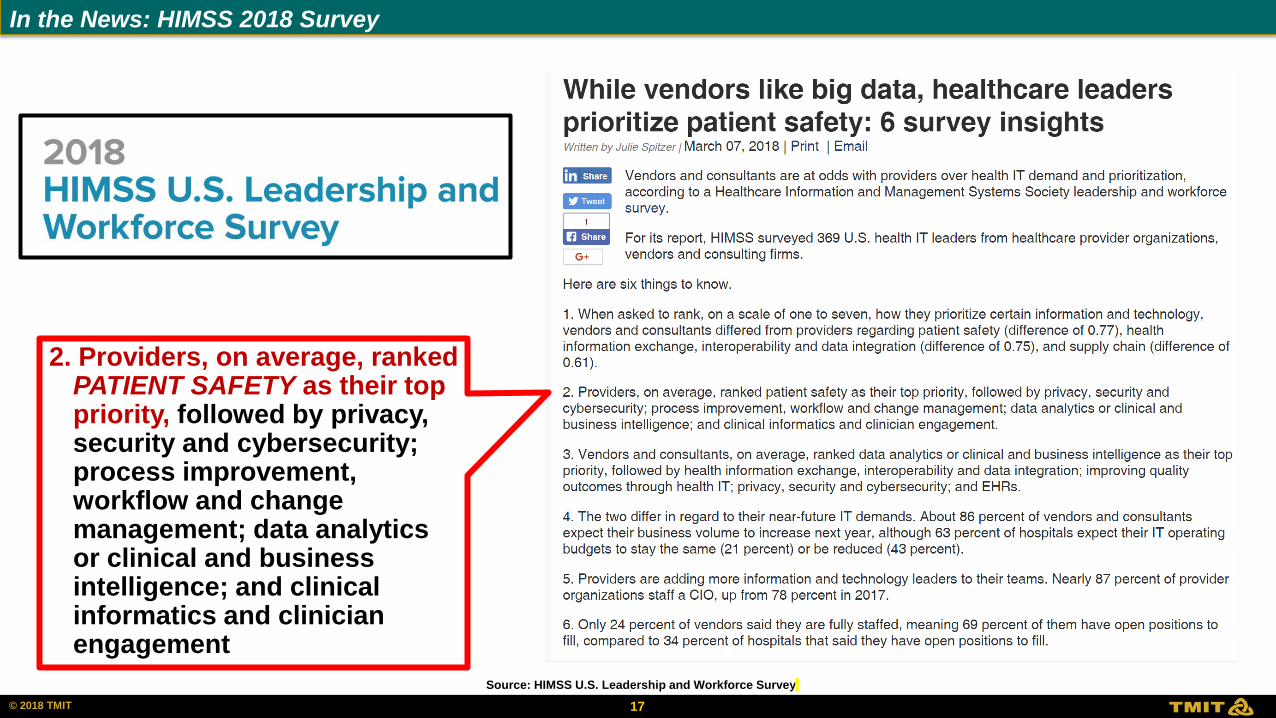
In the News: HIMSS 2018 Survey
Source: HIMSS U.S. Leadership and Workforce Survey
2. Providers, on average, ranked PATIENT SAFETY as their top priority, followed by privacy, security and cybersecurity; process improvement, workflow and change management; data analytics or clinical and business intelligence; and clinical informatics and clinician engagement
© 2006 HCC, Inc. CD000000-0000XX 18 © 2018 TMIT
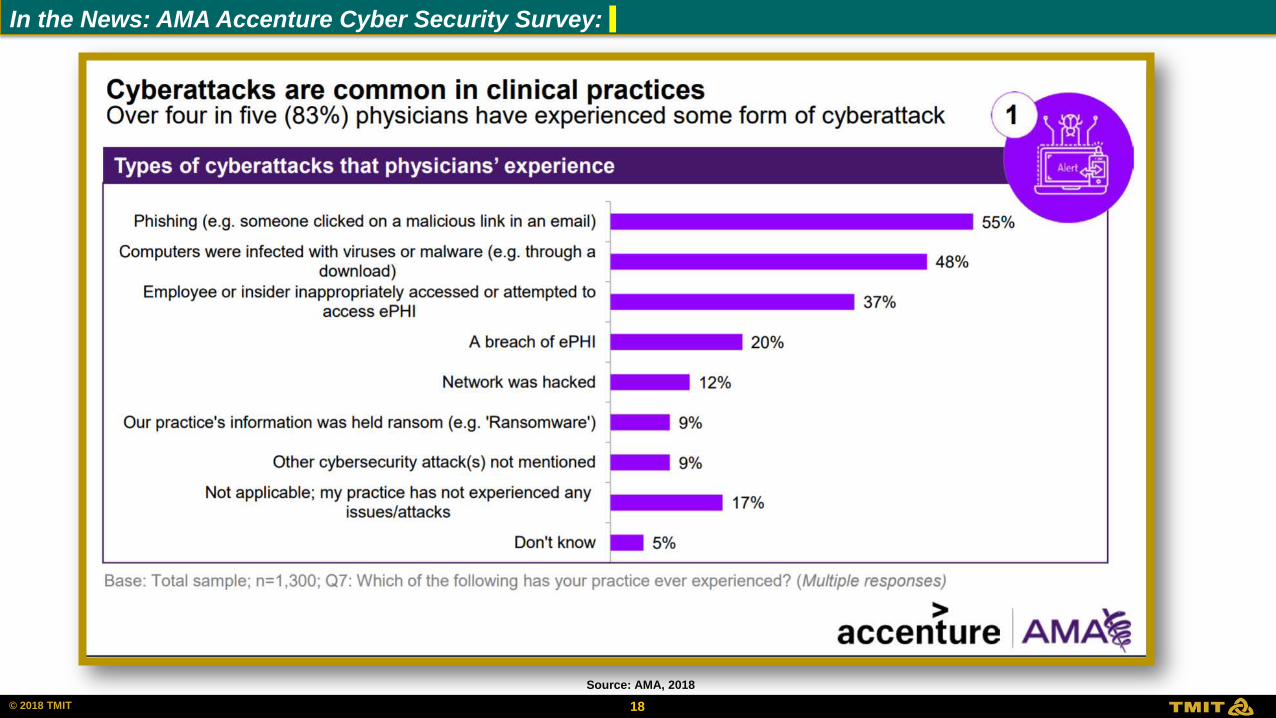
In the News: AMA Accenture Cyber Security Survey:
Source: AMA, 2018
© 2006 HCC, Inc. CD000000-0000XX 19 © 2018 TMIT
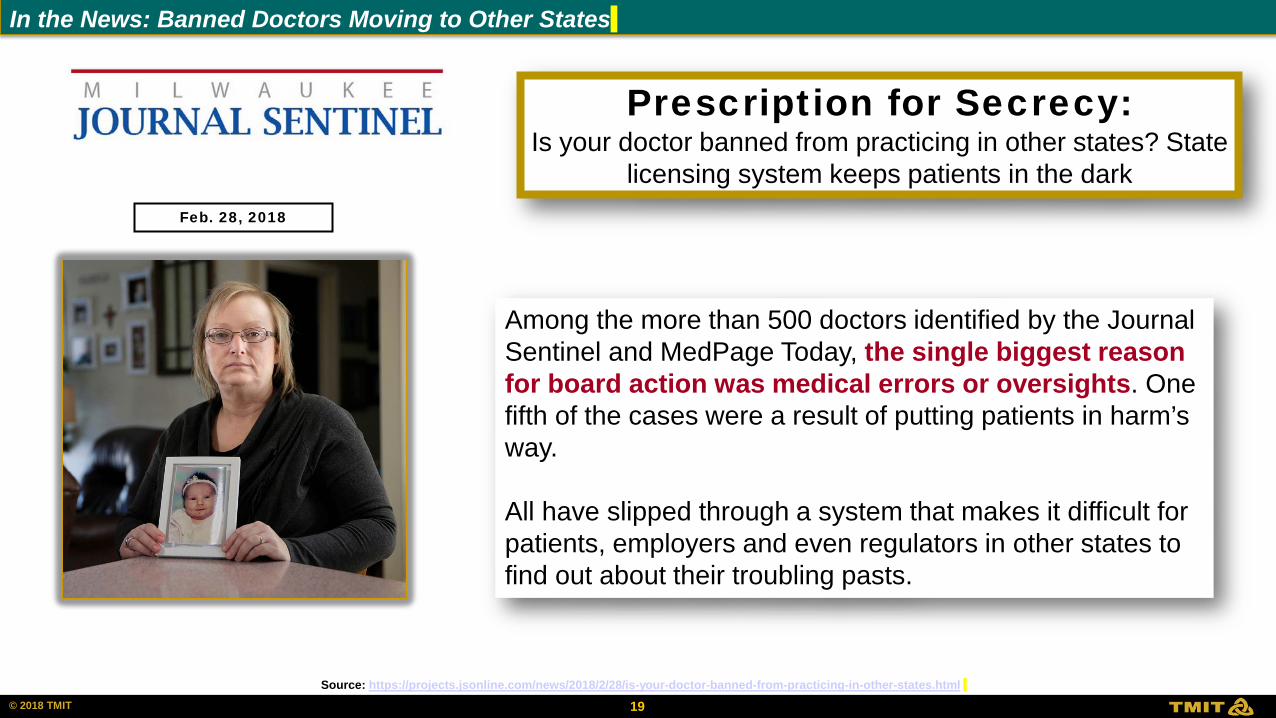
In the News: Banned Doctors Moving to Other States
Source: https://projects.jsonline.com/news/2018/2/28/is-your-doctor-banned-from-practicing-in-other-states.html
Prescription for Secrecy: Is your doctor banned from practicing in other states? State
licensing system keeps patients in the dark
Among the more than 500 doctors identified by the Journal Sentinel and MedPage Today, the single biggest reason for board action was medical errors or oversights. One fifth of the cases were a result of putting patients in harm’s way. All have slipped through a system that makes it difficult for patients, employers and even regulators in other states to find out about their troubling pasts.
Feb. 28, 2018
© 2006 HCC, Inc. CD000000-0000XX 20 © 2018 TMIT
In the News: Banned Doctors Moving to Other States
Source: https://www.chronicle.com/article/Why-Beall-s-List-Died-/241171 , Caplan, The Problem of Publication-Pollution Denialism Mayo Clinic Proceedings May 2015
Predatory Journals: Why Beall’s List Died
Nine months after a dogged academic librarian quietly deleted his carefully tended list shaming more than a thousand scientific journals as unscrupulous, the Beall’s List Murder Mystery remains unsolved. Why, after toiling so hard for five years — and creating a resource cherished by scientists wary of exploitative publishers — did the University of Colorado at Denver’s Jeffrey Beall abruptly give it all up? Who, or what, forced his hand?
Cuckoo for Cocoa Puffs? The surgical and neoplastic role of cacao extract in breakfast cereals
Pinkerton LeBrain1, Orson G. Welles2
1. Department of Statistical Research, Green Mountain Institute of Nutrition, Sharon, MA 02067, USA
2. Asuza Atlantic University, Department of Nutrition and Tomography, Westchester, NY, USA
The Problem of Publication-Pollution Denialism
Arther L. Caplan PhD
“The currency of science is fragile, and allowing counterfeiters, fraudsters, bunko artists, scammers, and cheats to continue to operate with abandon in the publishing realm is unacceptable. Talk of free speech and the power of the marketplace of ideas to sort out the wheat from the chaff is naive. When the marketplace is full of dangerous and defective goods, there is no free market because the trust requisite to support a market has evaporated.”
Regarding Cuckoo for Cocoa Puffs Article: Harvard researcher Mark Shrime submitted this fake article to 37 journals. “At last count, 17 had accepted the obviously phony, nonsensical paper..”
© 2006 HCC, Inc. CD000000-0000XX 21 © 2018 TMIT
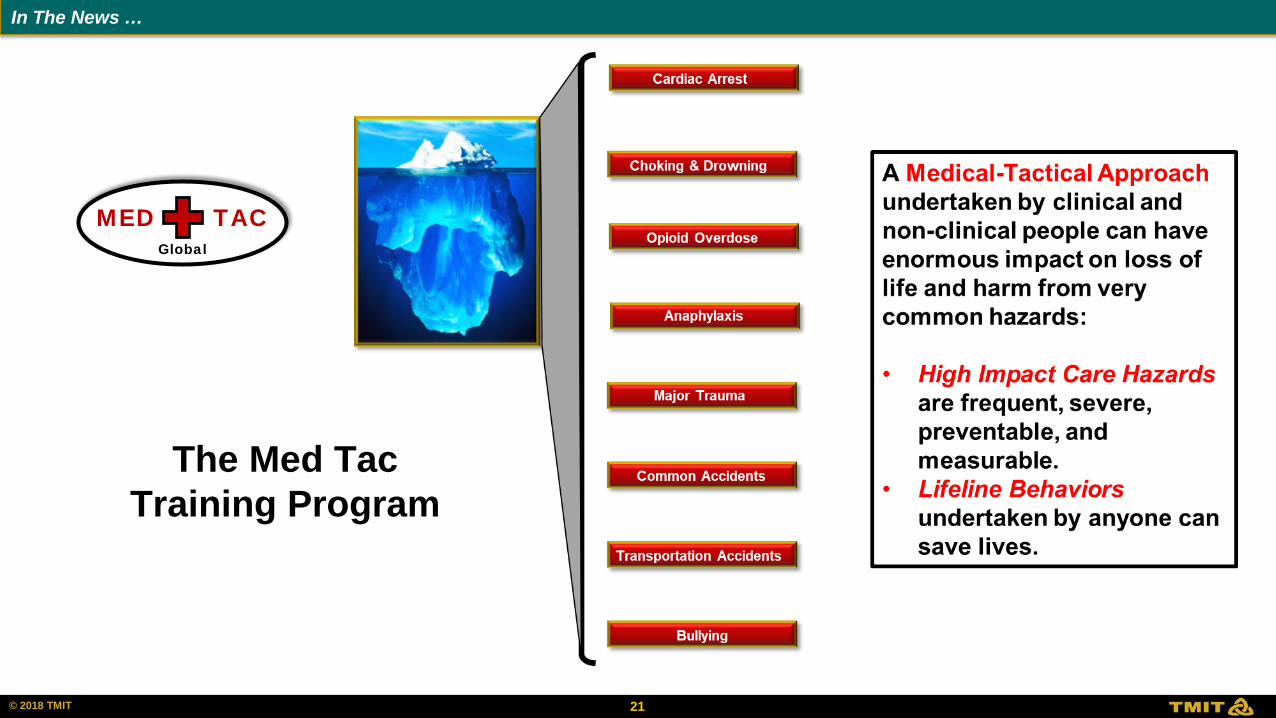
MED TAC Global
The Med Tac Training Program
In The News …
© 2006 HCC, Inc. CD000000-0000XX 22 © 2018 TMIT
Source: https://www.bleedingcontrol.org/
In The News …
Major Trauma: Stop the Bleed Program Cardiac Arrest
Opioid Overdose
Common Accidents
Bullying
Choking & Drowning
Anaphylaxis
Major Trauma
Transportation Accidents
Source: CBS. American College of Surgeons website. (also available via CBS All Access) Available at http://www.bleedingcontrol.org/about-bc/news-updates#kit
October 12, 2016
© 2006 HCC, Inc. CD000000-0000XX 23 © 2018 TMIT
Source: https://www.bleedingcontrol.org/
In The News …

© 2006 HCC, Inc. CD000000-0000XX 24 © 2018 TMIT
Source: https://www.bleedingcontrol.org/
In The News …
© 2006 HCC, Inc. CD000000-0000XX 25 © 2018 TMIT
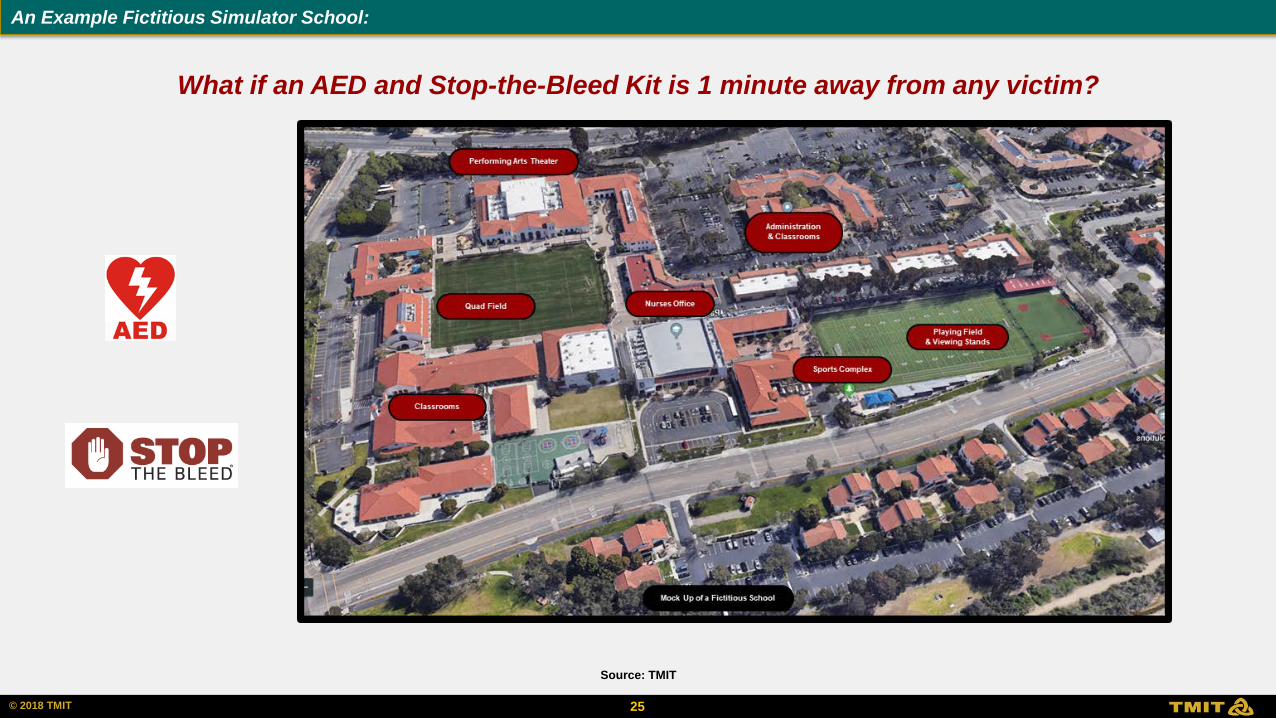
Source: TMIT
An Example Fictitious Simulator School:
What if an AED and Stop-the-Bleed Kit is 1 minute away from any victim?
26 © 2018 TMIT
25%
15% 13%
8% 13% 15%
3% 4% 1% 3%
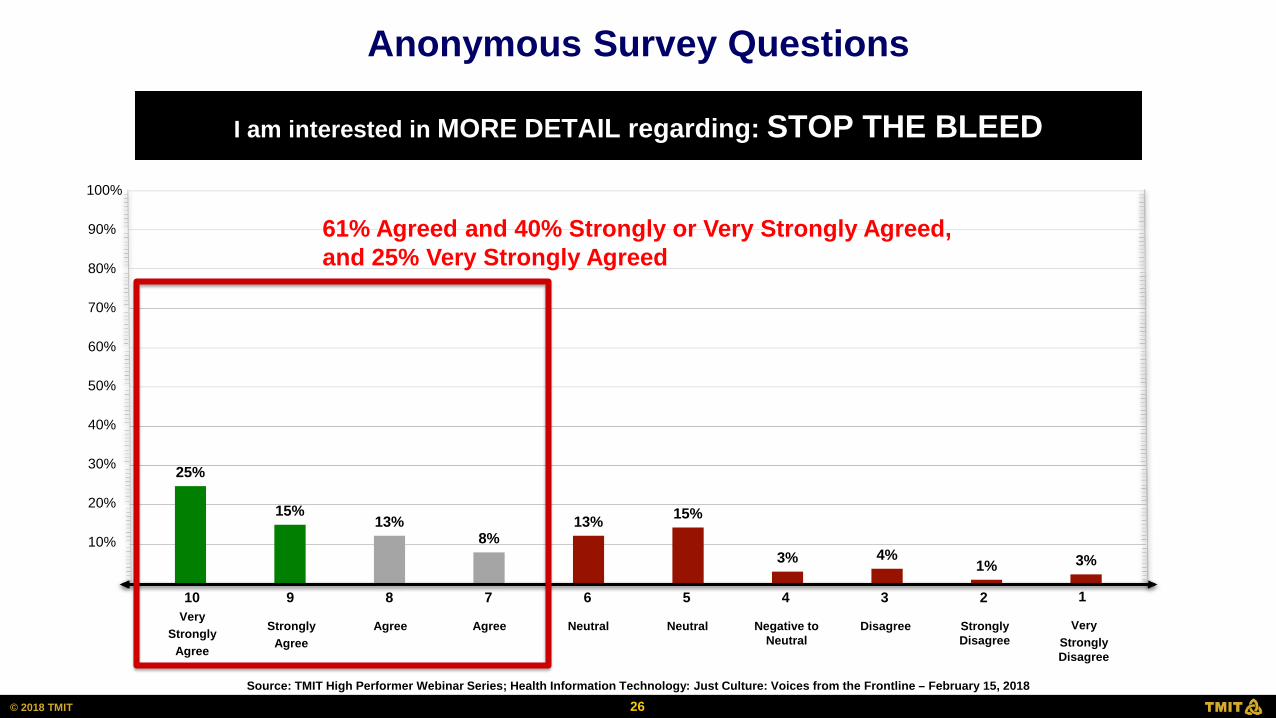
I am interested in MORE DETAIL regarding: STOP THE BLEED
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Very Strongly
Agree
10
Strongly Agree
9
Agree
8
Agree
7
Very Strongly Disagree
1
Disagree
3
Strongly Disagree
2
Neutral
6
Neutral
5
Negative to Neutral
4
61% Agreed and 40% Strongly or Very Strongly Agreed, and 25% Very Strongly Agreed
Anonymous Survey Questions
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
27 © 2018 TMIT
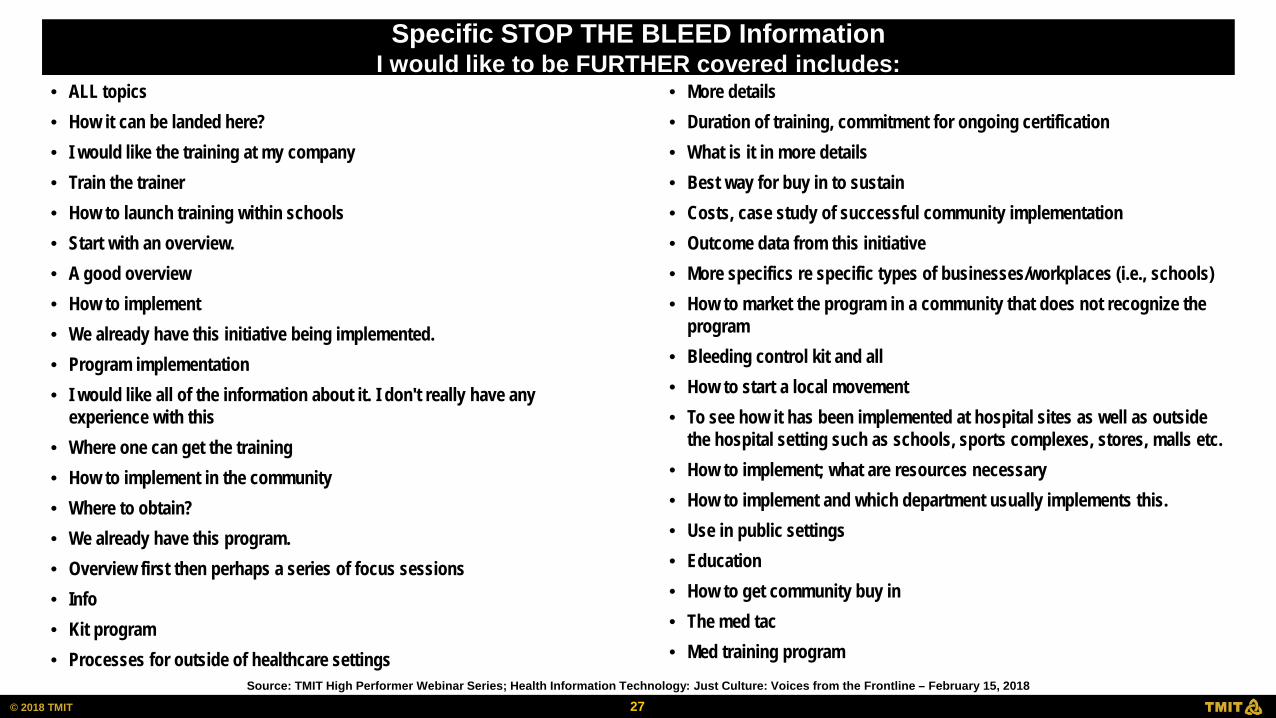
• ALL topics • How it can be landed here? • I would like the training at my company • Train the trainer • How to launch training within schools • Start with an overview. • A good overview • How to implement • We already have this initiative being implemented. • Program implementation • I would like all of the information about it. I don't really have any
experience with this • Where one can get the training • How to implement in the community • Where to obtain? • We already have this program. • Overview first then perhaps a series of focus sessions • Info • Kit program • Processes for outside of healthcare settings
• More details • Duration of training, commitment for ongoing certification • What is it in more details • Best way for buy in to sustain • Costs, case study of successful community implementation • Outcome data from this initiative • More specifics re specific types of businesses/workplaces (i.e., schools) • How to market the program in a community that does not recognize the
program • Bleeding control kit and all • How to start a local movement • To see how it has been implemented at hospital sites as well as outside
the hospital setting such as schools, sports complexes, stores, malls etc. • How to implement; what are resources necessary • How to implement and which department usually implements this. • Use in public settings • Education • How to get community buy in • The med tac • Med training program
Specific STOP THE BLEED Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
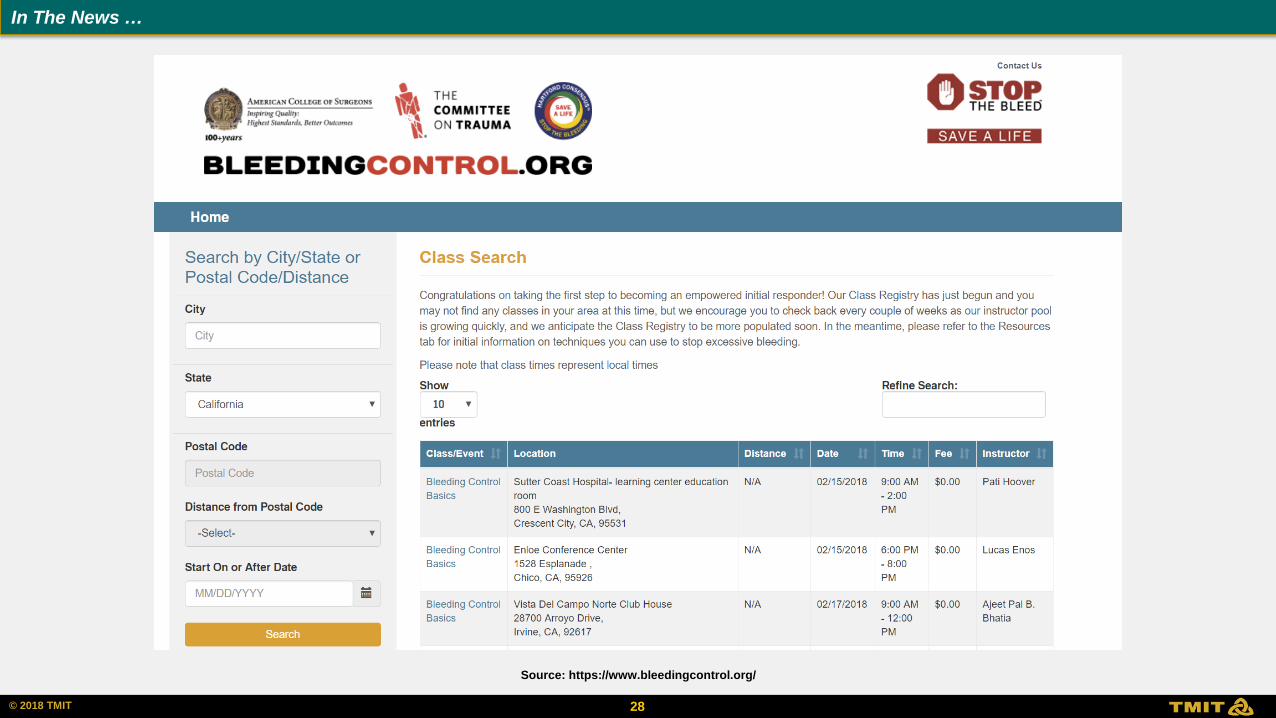
© 2006 HCC, Inc. CD000000-0000XX 28 © 2018 TMIT
Source: https://www.bleedingcontrol.org/
In The News …
29 © 2018 TMIT
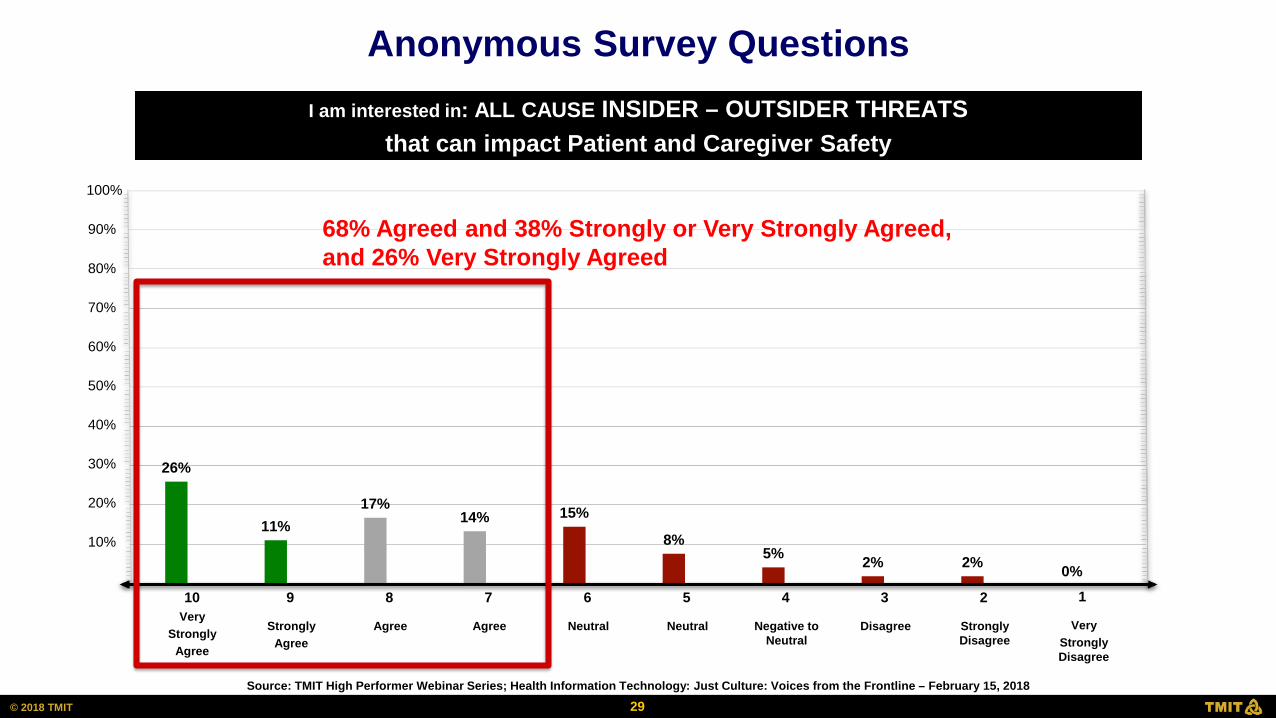
26%
11% 17%
14% 15%
8% 5% 2% 2% 0%
I am interested in: ALL CAUSE INSIDER – OUTSIDER THREATS that can impact Patient and Caregiver Safety
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Very Strongly
Agree
10
Strongly Agree
9
Agree
8
Agree
7
Very Strongly Disagree
1
Disagree
3
Strongly Disagree
2
Neutral
6
Neutral
5
Negative to Neutral
4
68% Agreed and 38% Strongly or Very Strongly Agreed, and 26% Very Strongly Agreed
Anonymous Survey Questions
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
30 © 2018 TMIT
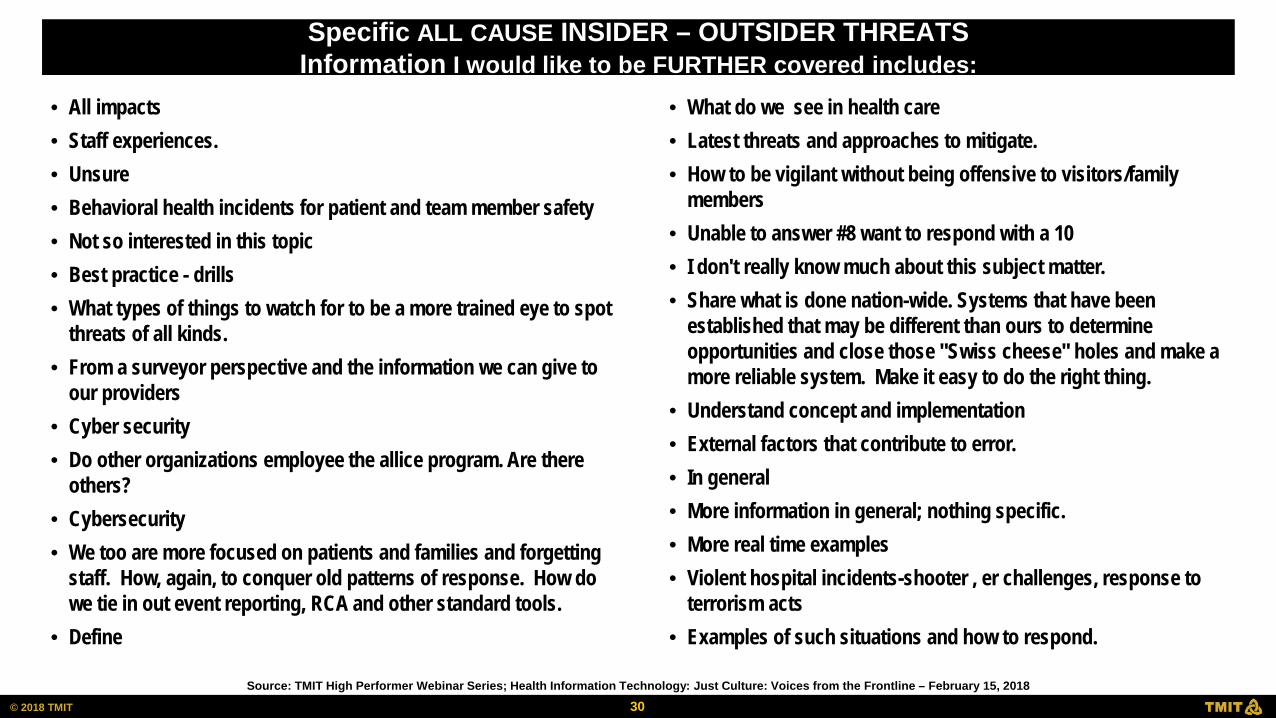
• All impacts • Staff experiences. • Unsure • Behavioral health incidents for patient and team member safety • Not so interested in this topic • Best practice - drills • What types of things to watch for to be a more trained eye to spot
threats of all kinds. • From a surveyor perspective and the information we can give to
our providers • Cyber security • Do other organizations employee the allice program. Are there
others? • Cybersecurity • We too are more focused on patients and families and forgetting
staff. How, again, to conquer old patterns of response. How do we tie in out event reporting, RCA and other standard tools.
• Define
• What do we see in health care • Latest threats and approaches to mitigate. • How to be vigilant without being offensive to visitors/family
members • Unable to answer #8 want to respond with a 10 • I don't really know much about this subject matter. • Share what is done nation-wide. Systems that have been
established that may be different than ours to determine opportunities and close those "Swiss cheese" holes and make a more reliable system. Make it easy to do the right thing.
• Understand concept and implementation • External factors that contribute to error. • In general • More information in general; nothing specific. • More real time examples • Violent hospital incidents-shooter , er challenges, response to
terrorism acts • Examples of such situations and how to respond.
Specific ALL CAUSE INSIDER – OUTSIDER THREATS Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
31 © 2018 TMIT
Implementing a Just Culture
David Marx, JD Just Culture Leader & Innovator Principle, Outcome Engenuity Center Eden Prairie, MN
Just Culture: The Ottawa Hospital Experience
Alan Forster, MD, FRCPC, MSC Vice President, Quality, Performance, and Population Health, The Ottawa Hospital Vice Chair, Quality and Clinical Services, Department of Medicine, University of Ottawa, Professor, Faculty of Medicine, University of Ottawa
Just Culture: A CEO Perspective
Sandra Coletta, FACHE Senior Executive, Author and Public Speaker Former President and CEO, Kent Hospital Saunderstown, RI
TMIT High Performer Webinar: Go to https://safetyleaders.com/webinarfebruary2018/
Just Culture Implementation
David Marx, BSE, JD CEO, Outcome Engenuity www.outcome-eng.com
February 15, 2017
JUST CULTURE IMPLEMENTATION 1. Commit to explore the idea (scouts)
2. Learn the concepts and methods (certification)
3. Commit to implement (time, resources, resolve)
4. Benchmark (survey, audits, reporting, outcomes)
5. Scrub policies and procedures (alignment?)
6. Train managers (1 day)
7. Establish the covenant (a unilateral promise)
8. Train staff (2 hours)
9. Feed the change (continuous reinforcement)
10. Measure progress (survey, audits, reporting, outcomes)

LEVEL OF COMMITMENT?
• Just Culture Light
• It’s about non-punitive reporting
• It’s only about safety
• It’s only post-event
• It’s about rules
• It’s somewhere in a policy
• It’s an “optional” tool
• Just Culture
• It’s about accountability
• It’s all conduct
• It’s duty and breach
• It’s about values
• It’s hardwired in
• It’s a covenant
35 © 2018 TMIT
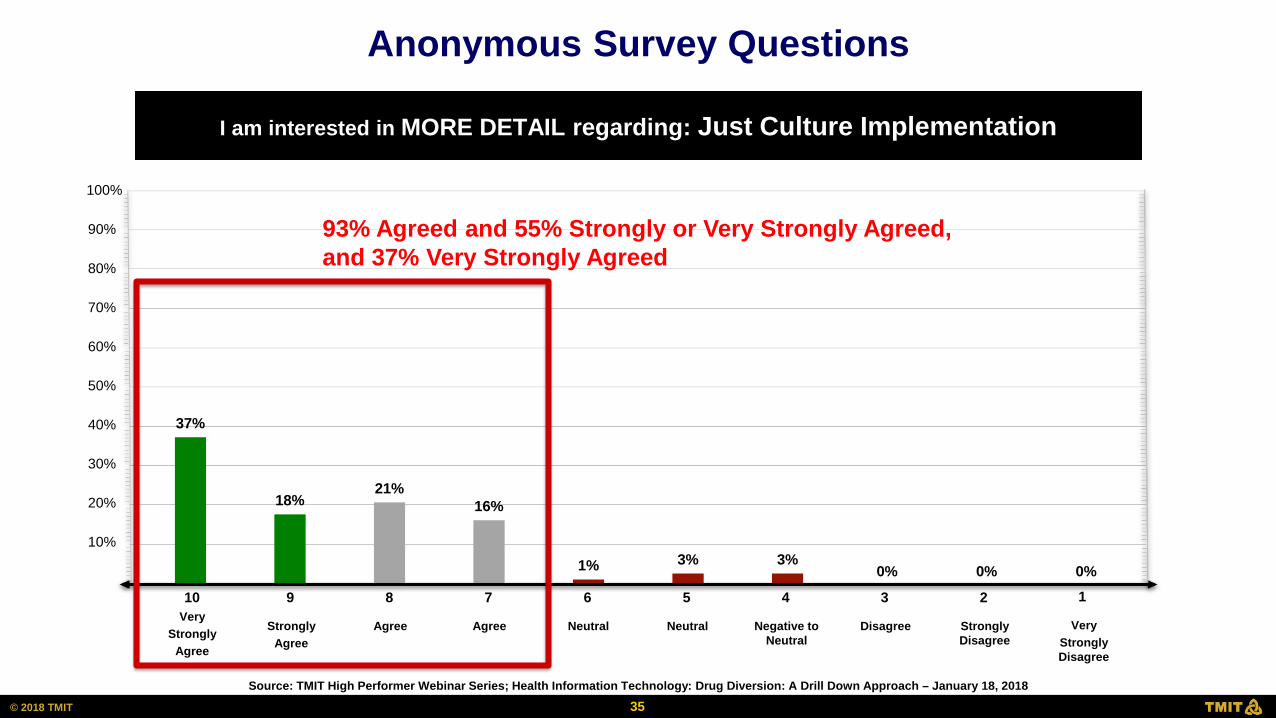
37%
18% 21%
16%
1% 3% 3% 0% 0% 0%
I am interested in MORE DETAIL regarding: Just Culture Implementation
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Very Strongly
Agree
10
Strongly Agree
9
Agree
8
Agree
7
Very Strongly Disagree
1
Disagree
3
Strongly Disagree
2
Neutral
6
Neutral
5
Negative to Neutral
4
93% Agreed and 55% Strongly or Very Strongly Agreed, and 37% Very Strongly Agreed
Anonymous Survey Questions
Source: TMIT High Performer Webinar Series; Health Information Technology: Drug Diversion: A Drill Down Approach – January 18, 2018
36 © 2018 TMIT
• Culture of safety • Becoming a HRO- developing a culture that
embraces • Case examples would • Have just cult certification - it is effective as long as
it is utilized consistently by all involved thank you, • How to make sure it is used by all managers
similarly • Culture connection to clinician burnout and
wellness/resilience • Addressing some behaviors: some type they exhibit
highs/lows, increased patient complaints • What I don't know but should
• Ambulatory care applications • Employ loyalty to co-workers/staff vs organization • How to • Need options to choose from to best answer critical
issues. • Creating a culture of "I've got your back" for staff to
be sure and witness waste rather than a culture of distrust or suspicion.
• I wasn't able to be on the webinar you mentioned at the beginning of today's program.
• How to help an individual "diverter" to rehab vs assuming "firing"
• Engagement; accountability
Specific Just Culture Implementation Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Drug Diversion: A Drill Down Approach – January 18, 2018
37 © 2018 TMIT
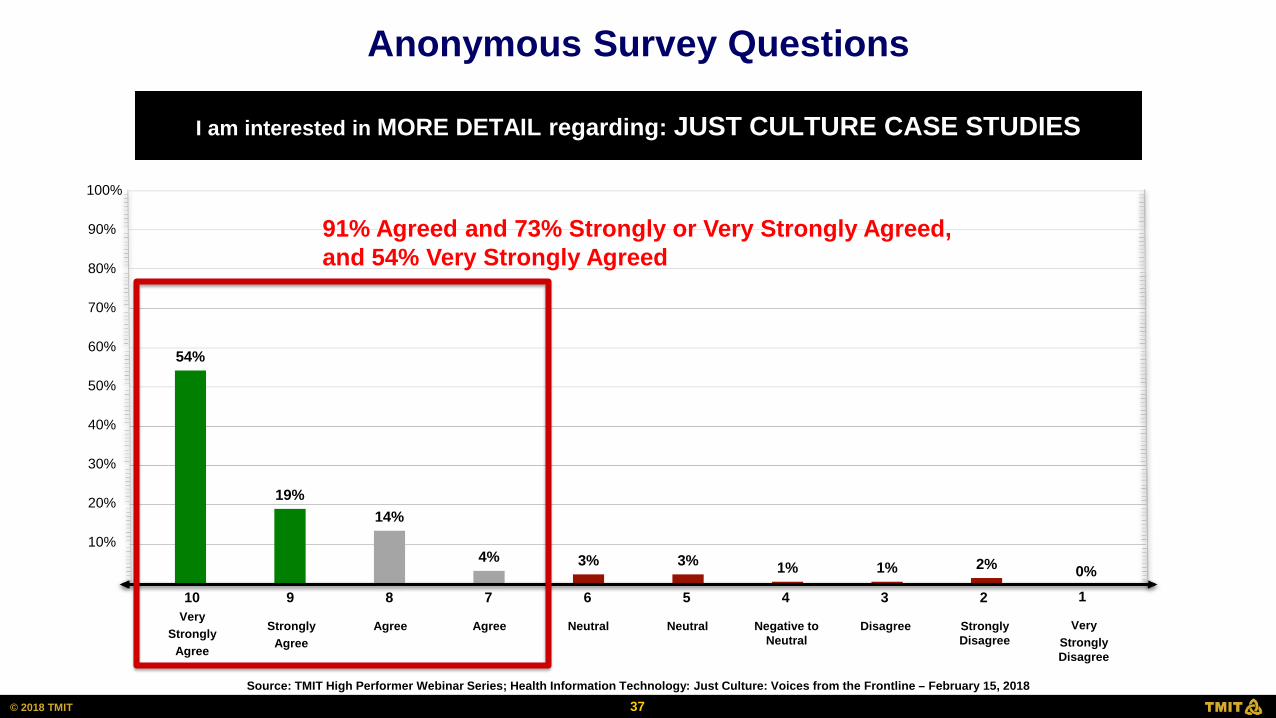
54%
19% 14%
4% 3% 3% 1% 1% 2% 0%
I am interested in MORE DETAIL regarding: JUST CULTURE CASE STUDIES
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Very Strongly
Agree
10
Strongly Agree
9
Agree
8
Agree
7
Very Strongly Disagree
1
Disagree
3
Strongly Disagree
2
Neutral
6
Neutral
5
Negative to Neutral
4
91% Agreed and 73% Strongly or Very Strongly Agreed, and 54% Very Strongly Agreed
Anonymous Survey Questions
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
38 © 2018 TMIT
• How you handle sentinel and never events • Implementation • All topics • Case studies that walk through the algorithm • Employee at risk behavior, employee reckless behavior, and medication errors • I think the case studies would provide the details needed to implement a just culture in
our organization. The actual presentation was extremely vague • Challenges with implementation in a union environment • Case studies of errors, at-risk, and reckless • Community pharmacy setting • Implementation strategies within large HMO and juncture between physician and
hospital leadership • Healthcare event involving multiple disciplines • Overview and then specific examples of implementing core key principles. • How the cases were investigated, response work, etc. • Case discussion, types of coaching • Case specific examples of the just culture model application and policy examples. • Case studies please • Case studies, implementation plan, keeping just culture momentum • How to jump start at organizational level • Examples of actual incidents and how just culture was applied • More details about implementation strategies, especially for larger systems
• More examples • N/A • Roll outs and sustainability, tools provided that were used • Updated algorithm • Different case studies where just culture was utilized and applied. • How to explain to providers from a surveyors perspective. What can the provider do to
improve their just culture. • Stories/scenarios with details to contrast how it may have been handled vs. How it was • Discussion of some of this tools used • Case studies then using the JC algorithm would further understanding and how to use
and apply principles • Leadership sustainability • Train the trainer, certification • Implementing just culture across a vast organization/system • Specific measures for maintaining • Everything. Structure the starting point • Manager training • How to deal with provider correction as no fault • Case studies are great • Just culture in the mediation/arbitration process. Case law supports old methods of
discipline. • How specifically did leader get buy in
Specific JUST CULTURE Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
39 © 2018 TMIT
• 2nd victim theory; PTSD in those involved • Barriers to implementation; can it be done without CEO leading
it, can it succeed by spread from one site to another versus all at once in a multihospital system, estimated costs (training, time, resources, etc.)
• Strategies to implement just culture, dealing with resistant push-back, data on outcomes in terms of harm reduction, impact on near misses.
• My facility utilizes and has implemented this approach already • How to sustain just culture environment once implemented and
change of upper management staff. • How to kick start just culture in my own department, information
that i can share with my fellow leaders. • Effective coaching tools/techniques • Managers trainers • Resources and case studies • The case studies would be very valuable to review. • Selling it to leadership effectively
• Best practices on how to implement, as i am having a hard time finding information on this. Specifics on training mgmt (what tools to use), and what types of focus groups should we form in our investigation of current state.
• Coaching mechanism • Would like to hear from more organizations and how they
implemented a just culture program • Case studies • Coaching, root cause analysis and investigation, do you have
staff involved participate in the RCA process investigation discussion action plan for the future. Investigating and discipline for reckless behavior. Do you believe RCAs should be discoverable in a lawsuit.
• None at this time • Specific examples, training materials • Case studies and application. How to apply to near miss cases or
where harm did not occur. Disclosure practices, and how to hardwire within the organization and medical staff. What department generally owns just culture implementation?
Specific JUST CULTURE Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
40 © 2018 TMIT
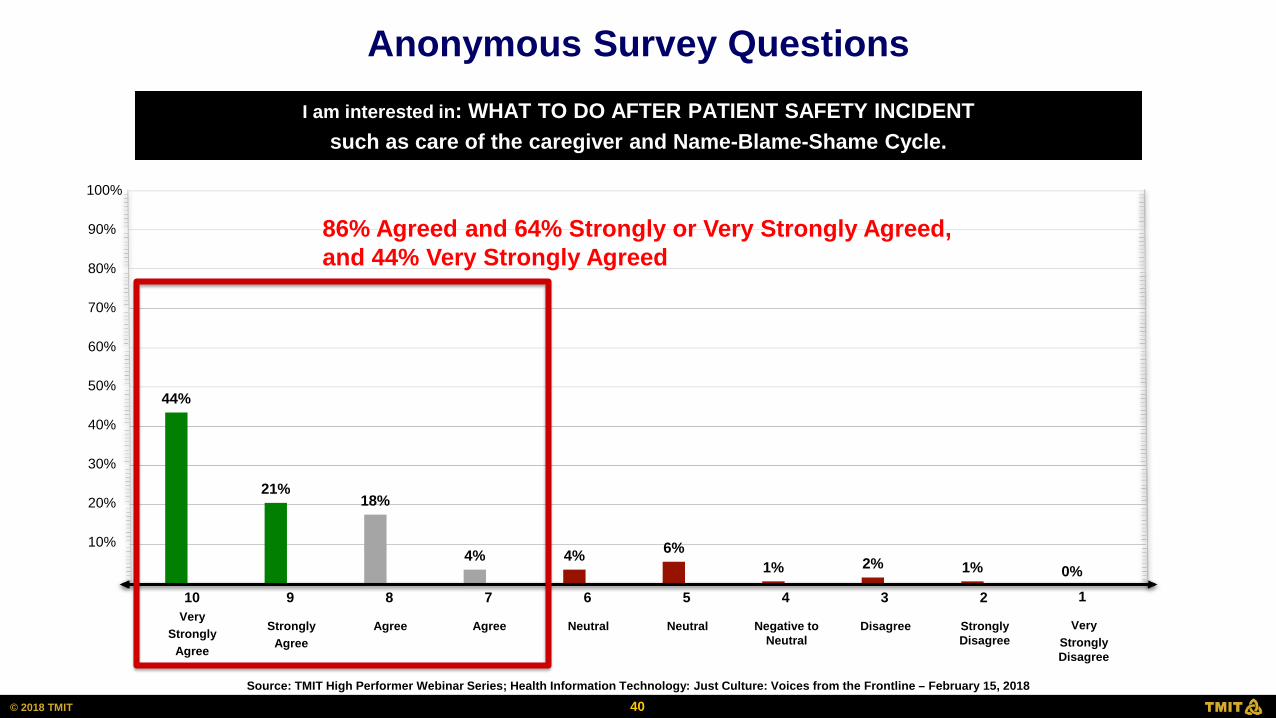
44%
21% 18%
4% 4% 6% 1% 2% 1% 0%
I am interested in: WHAT TO DO AFTER PATIENT SAFETY INCIDENT such as care of the caregiver and Name-Blame-Shame Cycle.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
Very Strongly
Agree
10
Strongly Agree
9
Agree
8
Agree
7
Very Strongly Disagree
1
Disagree
3
Strongly Disagree
2
Neutral
6
Neutral
5
Negative to Neutral
4
86% Agreed and 64% Strongly or Very Strongly Agreed, and 44% Very Strongly Agreed
Anonymous Survey Questions
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
41 © 2018 TMIT
• All interventions and preventive measures • Any • How to handle with just culture mindset, tools or scripts that were helpful • Elements of a good RCA process • Process • 2nd victims • More about human factors, 2nd and 3rd victim responses • Use for learning, improvement • Reporting systems • Any information you can provide • Timing for disclosure vs. Investigation • How to make people feel comfortable to be honest and come forward • Roadmap to use so that we don't miss anything. • How to address those who are not "on board" with just culture, as you defend your
staff. • How do the human resources policies change to cover just culture - how do we change
staff views? • Trying very hard to break old patterns of responding to issues. Structure of just
culture committees and tools for responding to incidents/issues • How to balance disciplinary action with accountability with coaching • How to collect data
• How to help someone rebuild confidence following an event. • Who are the best people to interact with the patient after an event • How to maintain communication with patient / family involved; how far to go • Second victim tools • Where does the patient come into the process after the incident occurs? What is the
practice? • We already have a care for the care giver program and trained staff to serve in this role • How to promote a protective environment for total open discussion on what has
occurred during a safety incident • How do we get other facility leaders to buy in? • How to teach practical application of 2nd victim/care of the caregiver concepts. • RCAs guidelines • Process and structure • To see what other organizations do for the 2nd victim support. • Applying just culture • Roles of both the reporter and person receiving report • Mechanism utilized to share the key learnings across the organization on a consistent
basis • Again, would like to hear from more organizations • Case studies, especially around disclosure • Apologies and disclosure to patients,
Specific WHAT TO DO AFTER PATIENT SAFETY INCIDENT Information I would like to be FURTHER covered includes:
Source: TMIT High Performer Webinar Series; Health Information Technology: Just Culture: Voices from the Frontline – February 15, 2018
42 © 2018 TMIT
Just Culture: High Impact Case Studies
David Marx, JD Just Culture Leader & Innovator Principle, Outcome Engenuity Center Eden Prairie, MN TMIT High Performer Webinar March 15, 2018

JUST CULTURE:
HIGH IMPACT CASE STUDIES
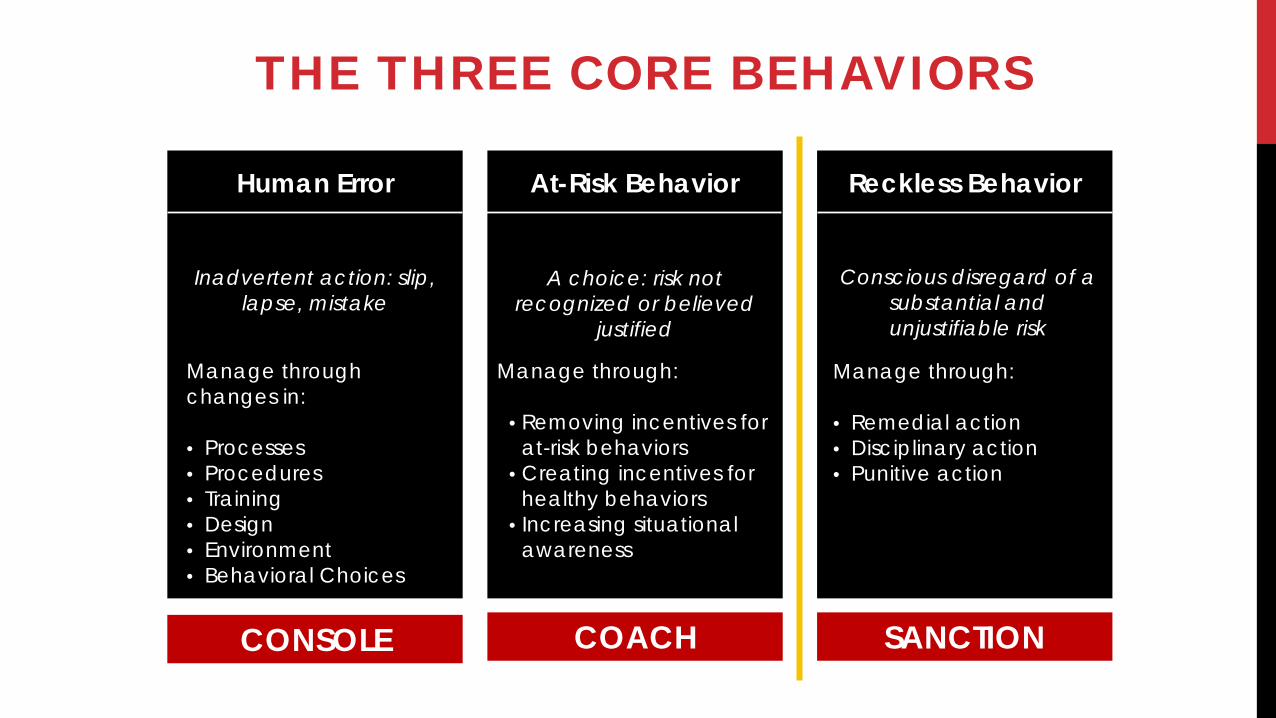
THE THREE CORE BEHAVIORS
Reckless Behavior
Conscious disregard of a
substantial and unjustifiable risk
Manage through: • Remedial action • Disciplinary action • Punitive action
At-Risk Behavior
A choice: risk not recognized or believed
justified
Manage through:
• Removing incentives for at-risk behaviors
• Creating incentives for healthy behaviors
• Increasing situational awareness
Human Error
Inadvertent action: slip,
lapse, mistake
Manage through changes in: • Processes • Procedures • Training • Design • Environment • Behavioral Choices
CONSOLE COACH SANCTION
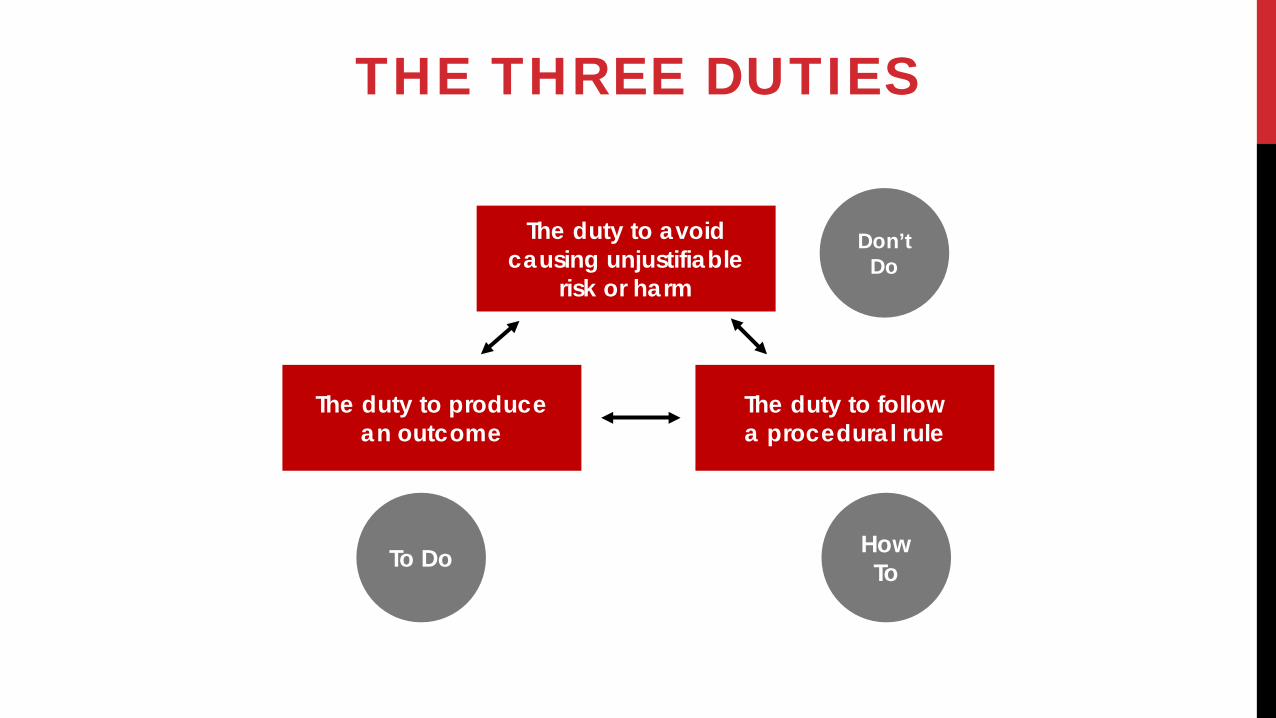
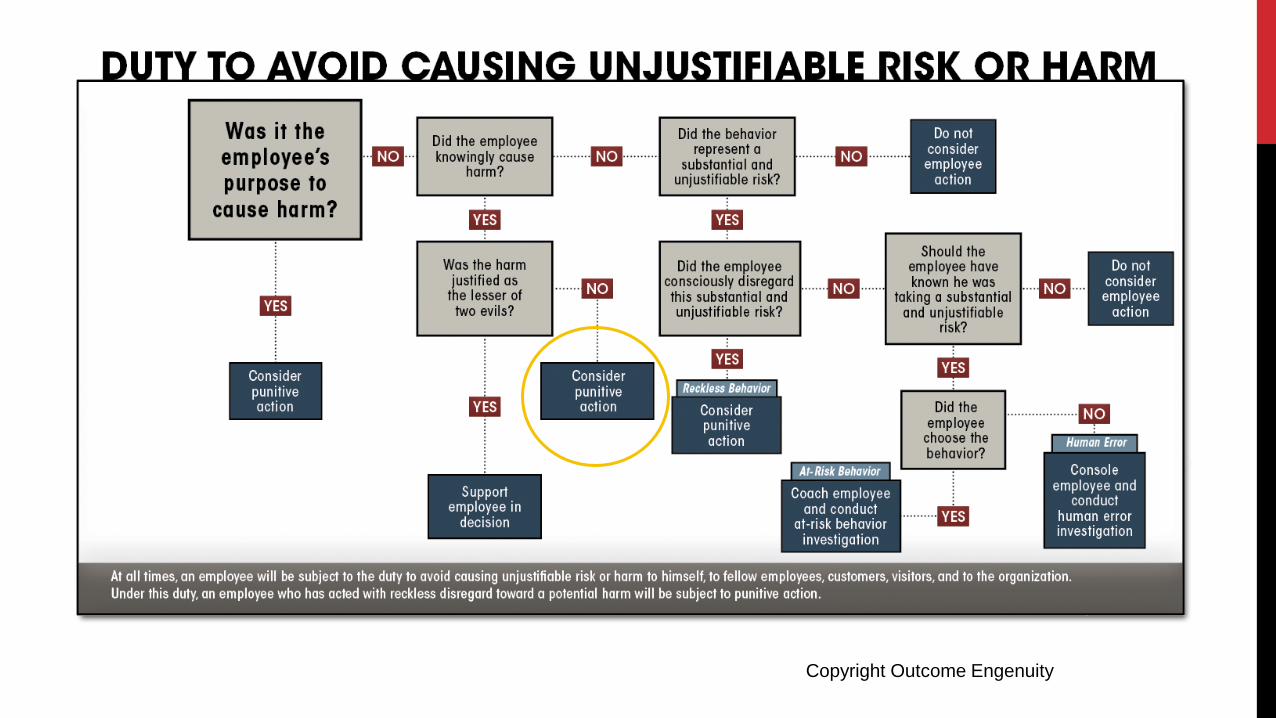
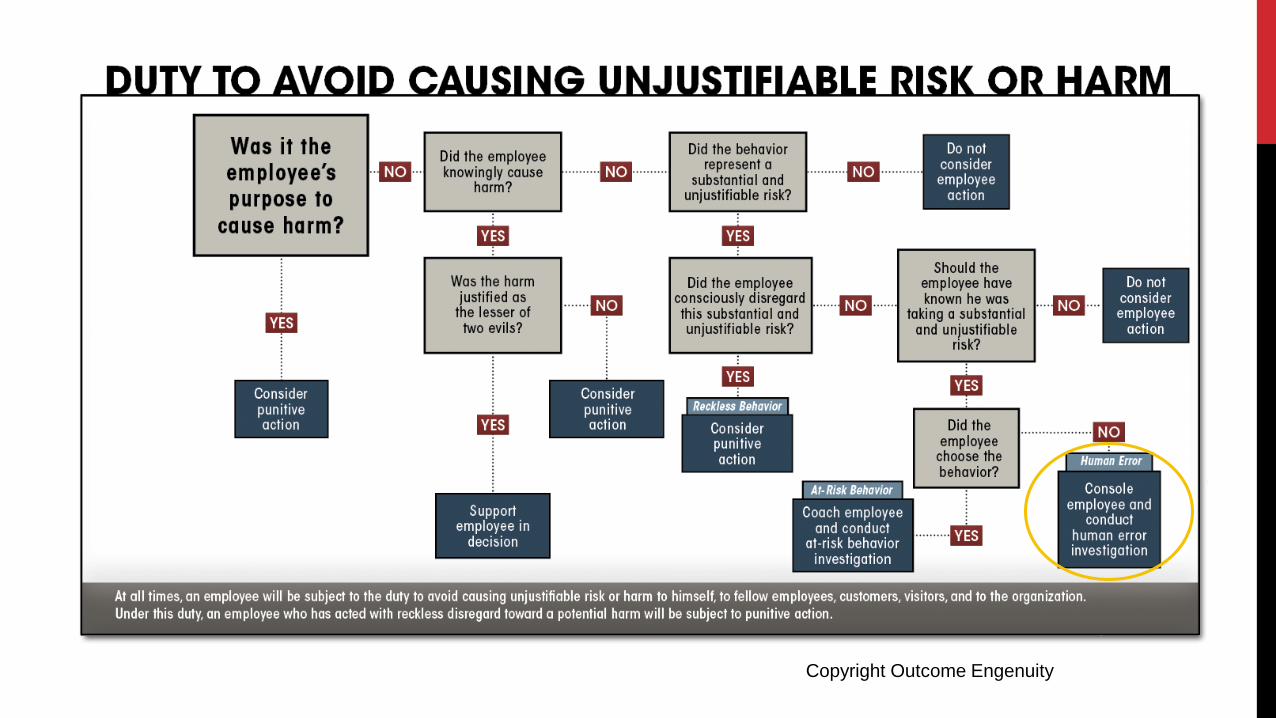
THE THREE DUTIES
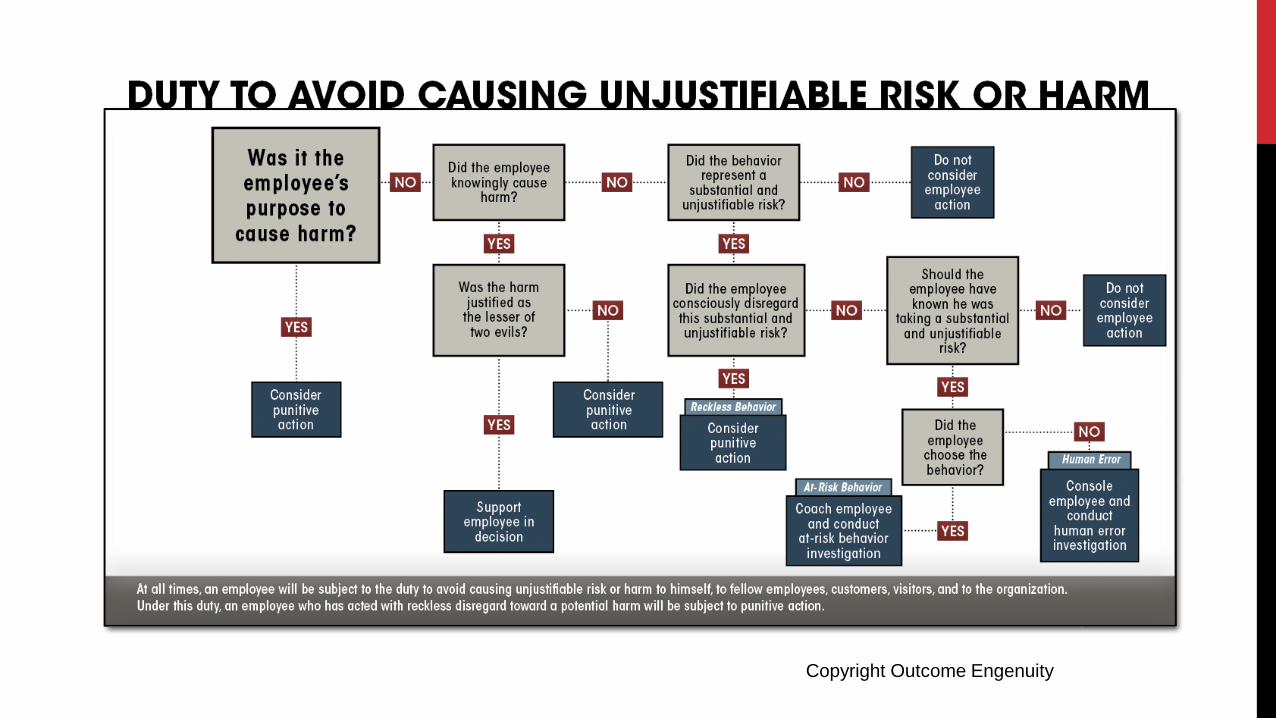
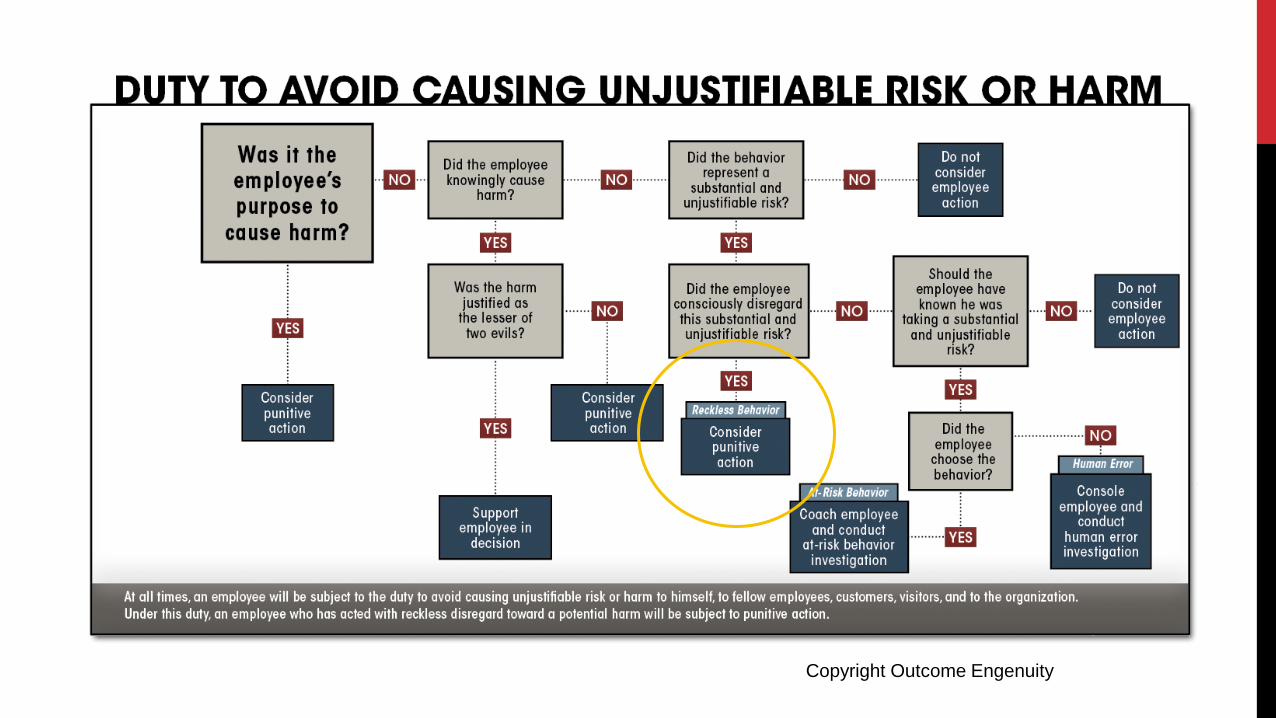
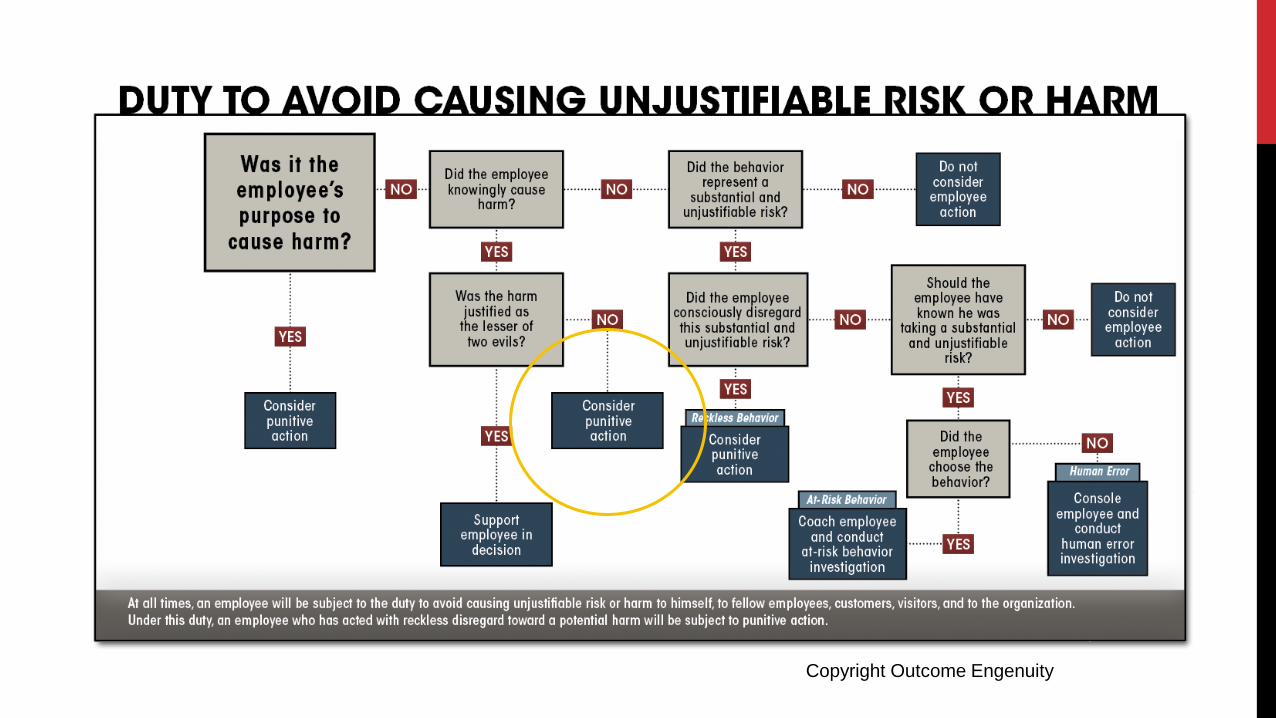
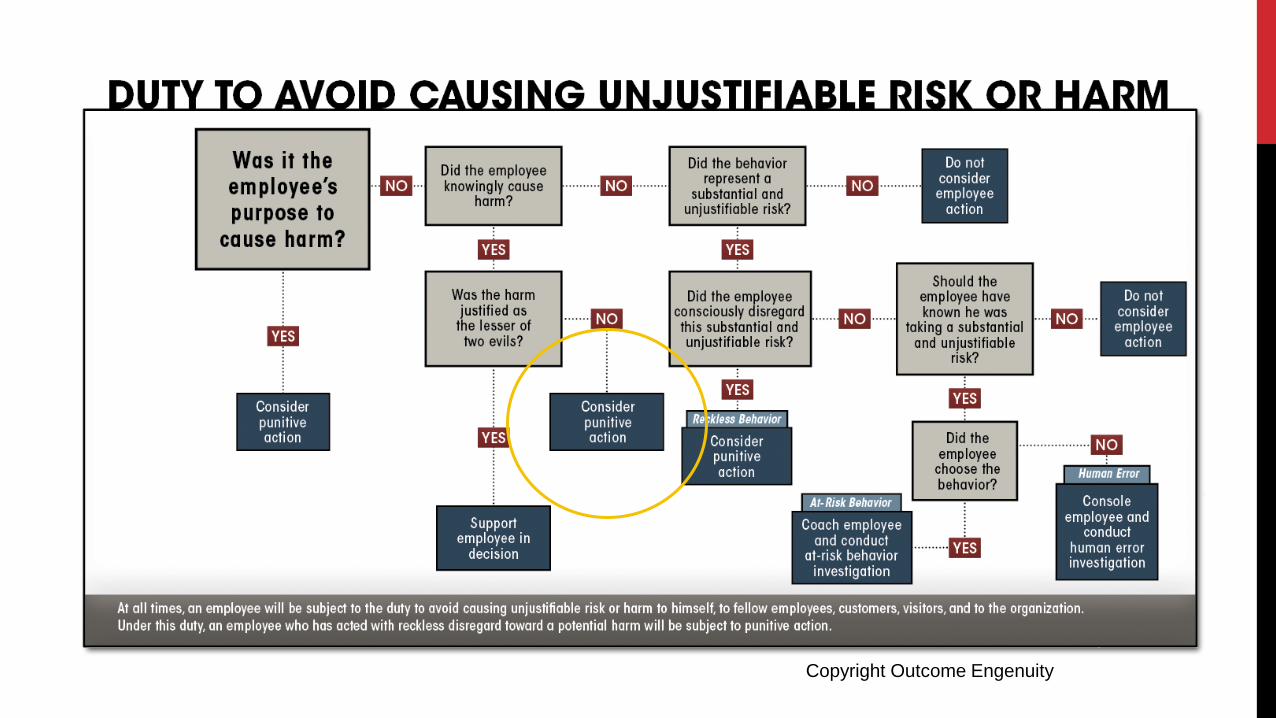
The duty to avoid causing unjustifiable
risk or harm
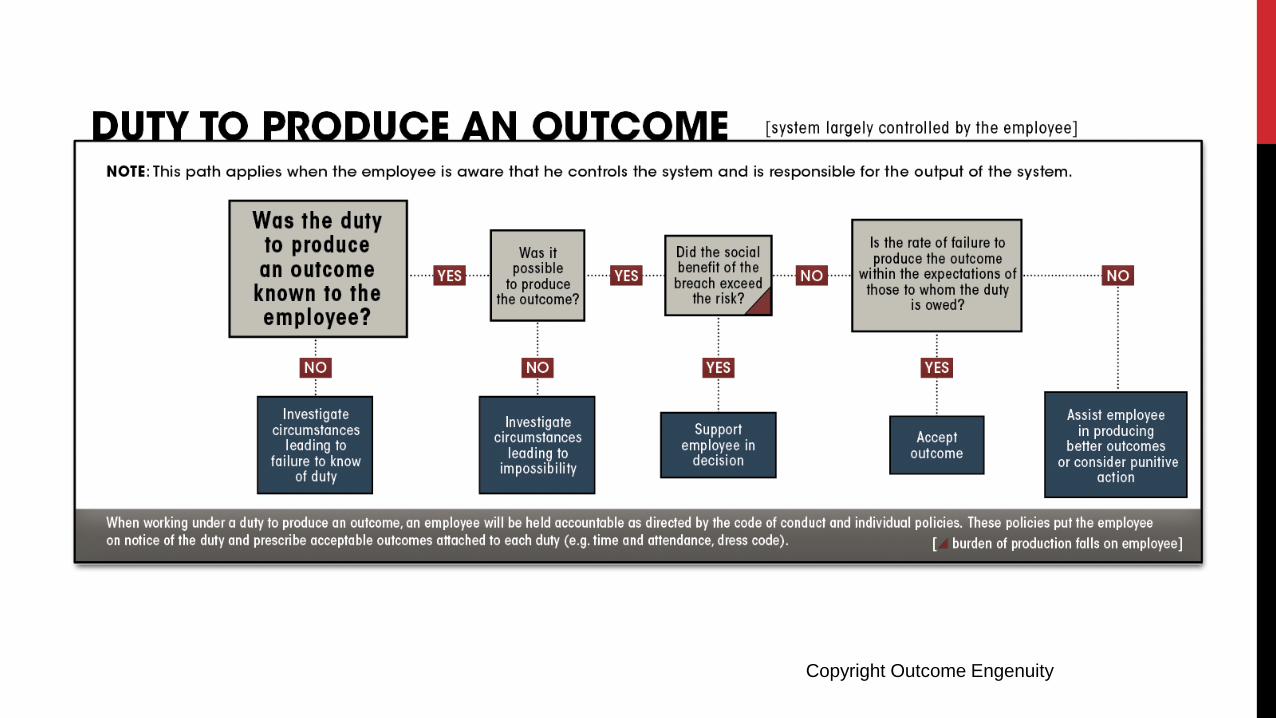
The duty to produce an outcome
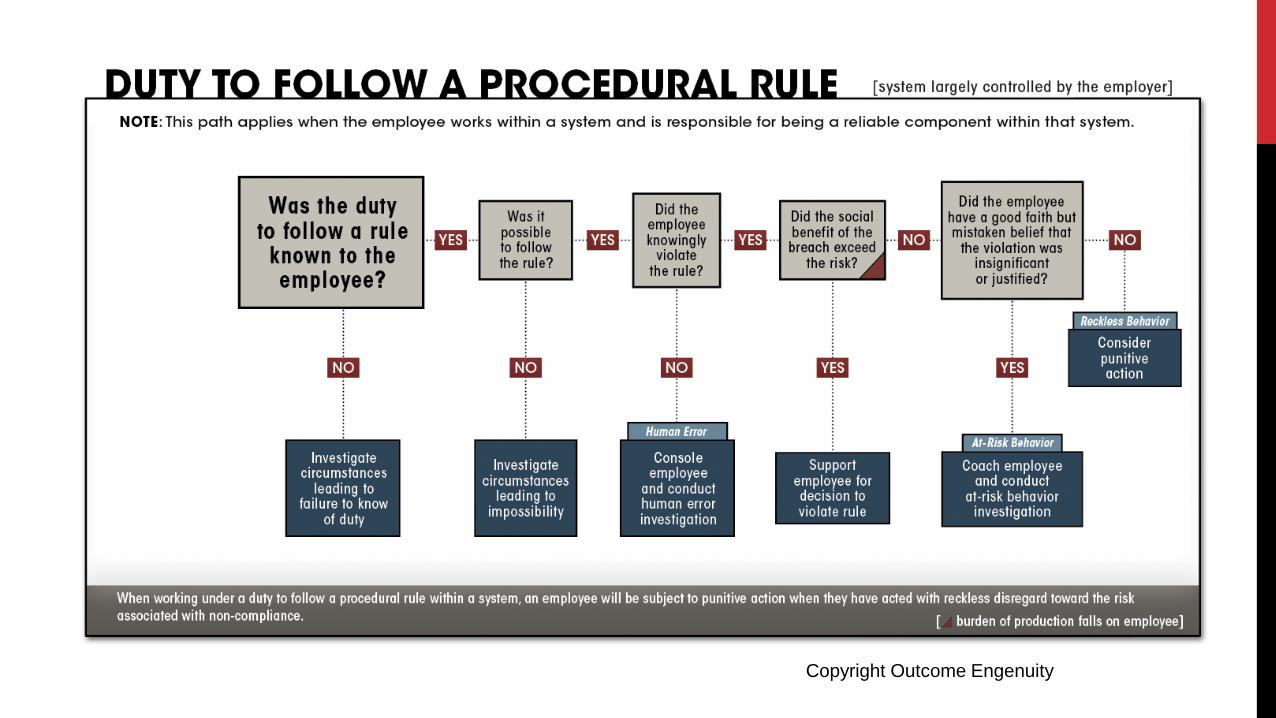
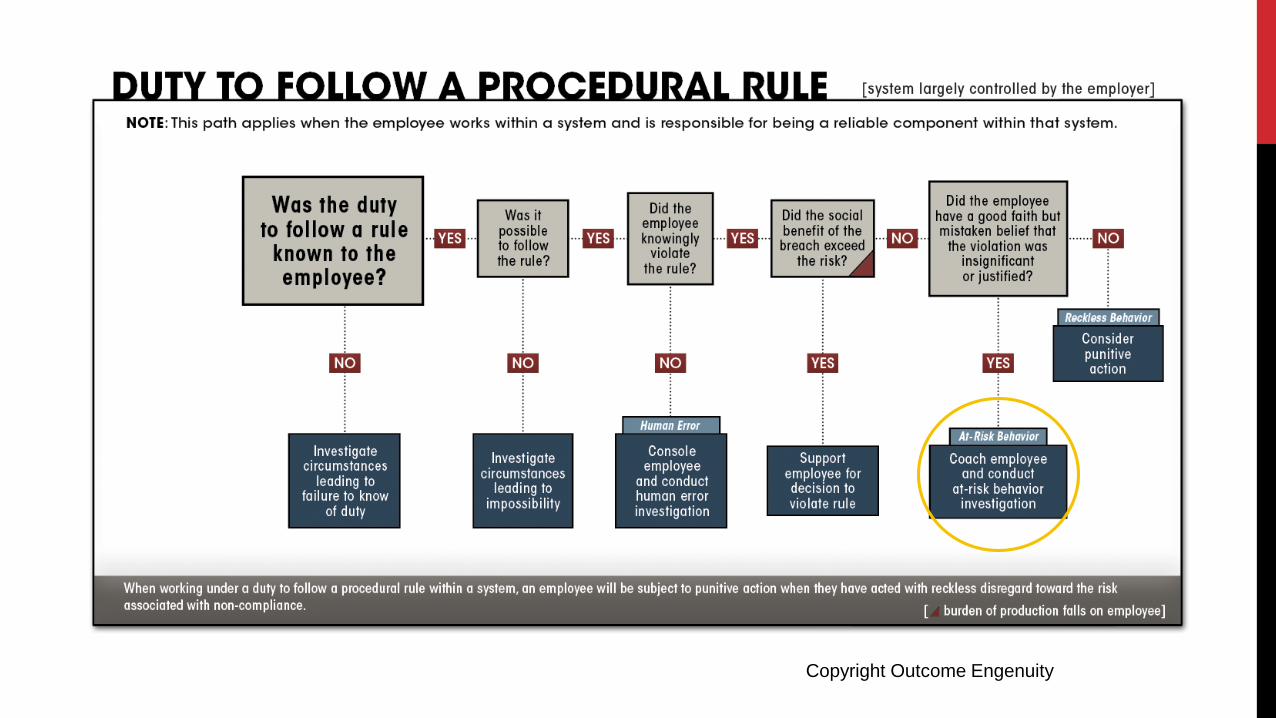
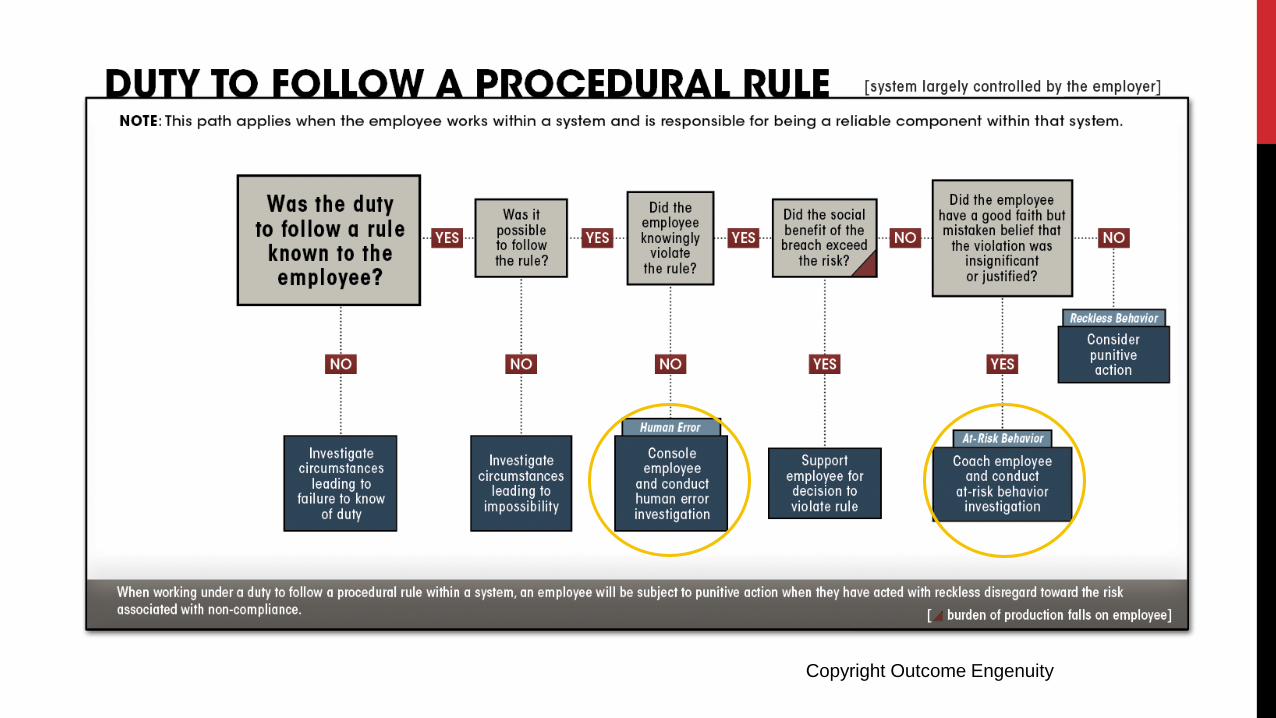
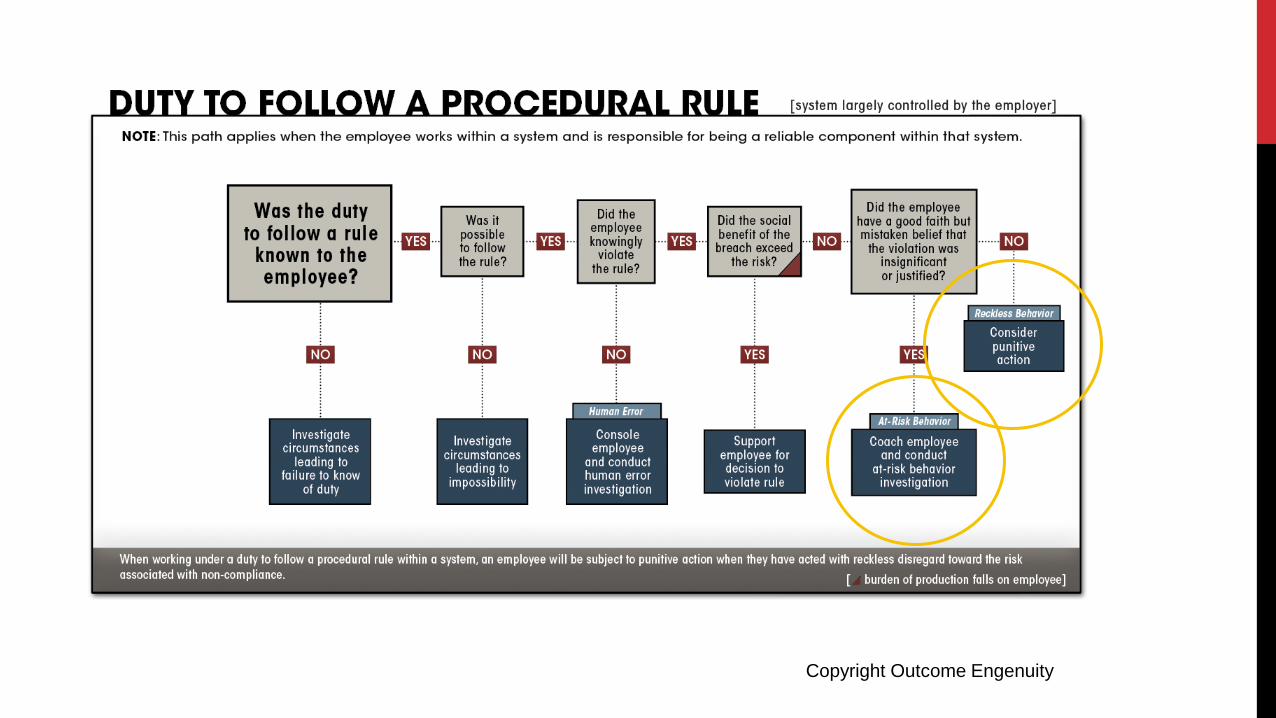
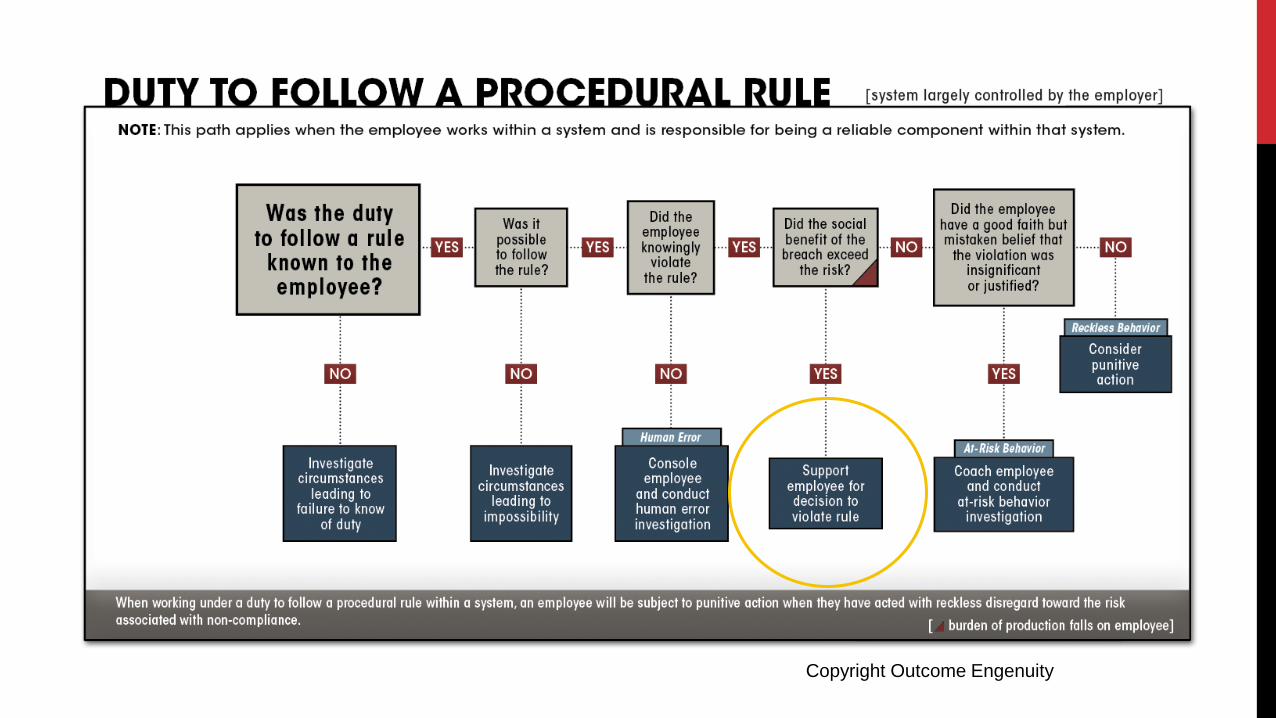
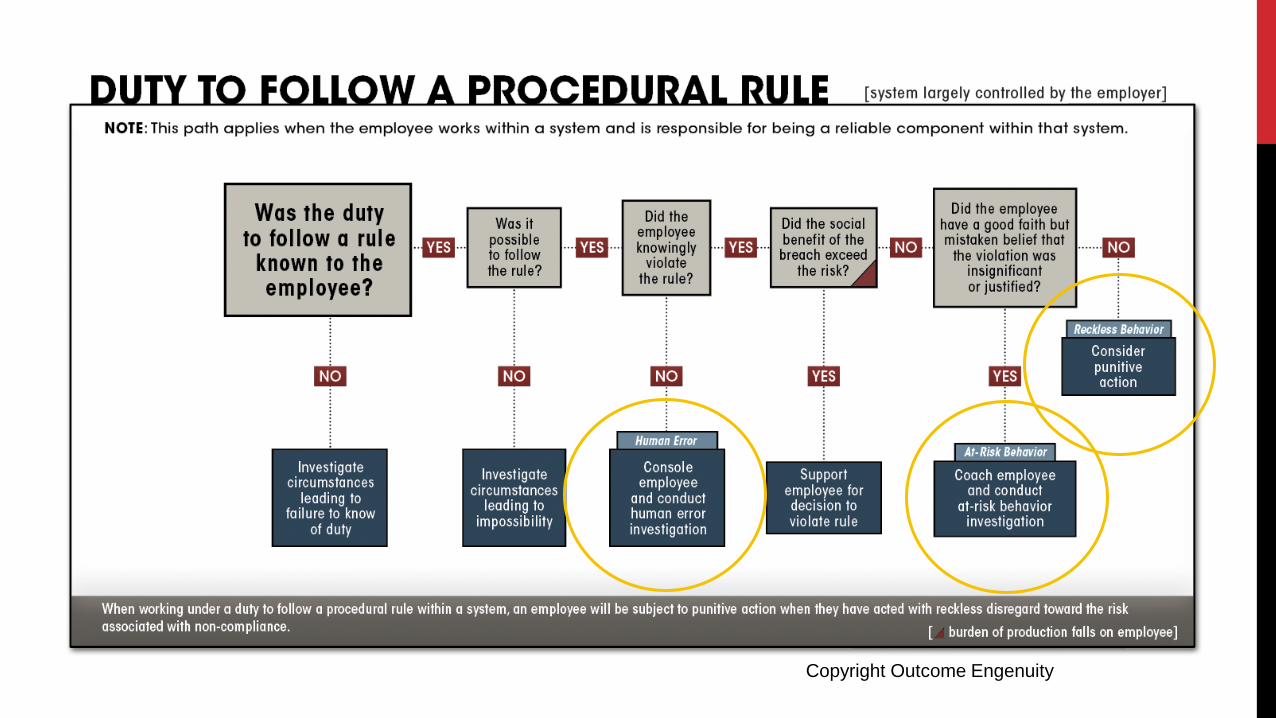
The duty to follow a procedural rule
Don’t Do
To Do How To
PROCEDURAL “HOW TO” BREACHES
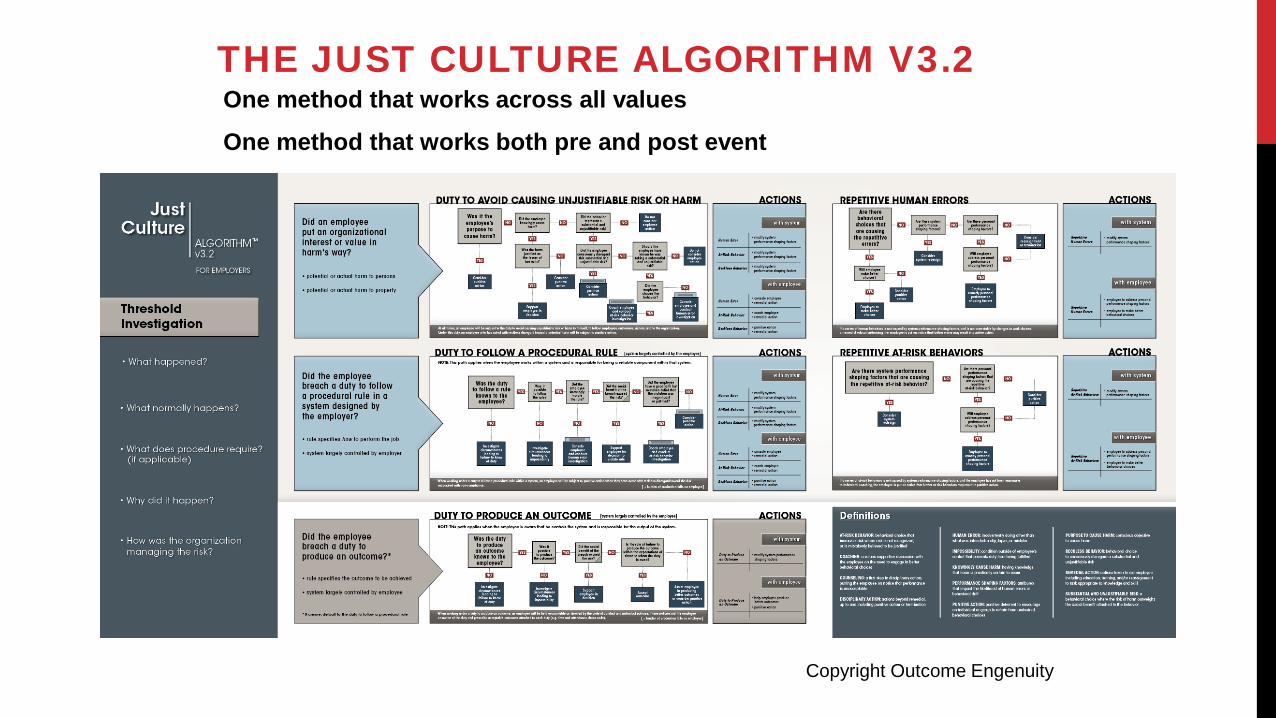
One method that works across all values One method that works both pre and post event
THE JUST CULTURE ALGORITHM V3.2
Copyright Outcome Engenuity
THE ALGORITHM IS TO BE USED AFTER THE INVESTIGATI0N IS COMPLETE, AND
BOTH SYSTEMS AND BEHAVIORAL ISSUES HAVE BEEN IDENTIFIED
PROCEDURAL “HOW TO” BREACHES
Copyright Outcome Engenuity
A housekeeping worker was waxing the floors around 10:00 pm. He could not find a wet floor sign and would have had to have go to another building to search for one. Believing he was alone in the building, he did not search for a warning sign. An accountant slipped on the wet floor and severely damaged his knee. The housekeeping staff frequently had to search for the wet floor warning signs which caused them to get behind on their work. The housekeeping manager was aware of the unavailability of signs, but did not take any action to purchase more.
SCENARIO 1
Copyright Outcome Engenuity
The Engineering department has a large book in which the instructions for repairing equipment are located. Policy requires that these instructions be followed each time that a repair was performed. Last week a technician made a mistake on the repair of an infusion pump by omitting a required check upon re-assembly of the pump (relying on his memory to perform the task). This check, called out in the manual, would have confirmed that the infusion pump would not allow the free (unregulated) flow of medication under a particular failure mode of the pump. The inoperable pump safety device was caught when a patient received a free flow of heparin, leading to the death of the patient. Investigation reveals that the technician regularly performs this specific maintenance. Investigation also reveals that other technicians were performing this task by memory, without the aid of the procedure manual.
SCENARIO 2
Copyright Outcome Engenuity
SCENARIO 3
A brand new nurse to the OR (watching and learning the processes and practices of her new employer) storms out of the safety timeout ahead of surgery and right in the Director of the OR’s office. She blurts out, “Are you kidding me? The anesthesiologist is listened to his IPod with those little things in his ears. He’s actually dancing a bit, you know, moving to the beat, nodding his lead when people look his way. I looked at everyone else in the timeout, and no one seemed to notice. They look like Zombies. Is this how we’re going to treat patients here? Do anesthesiologists get a pass? Does anyone care?”
Copyright Outcome Engenuity
A nursing manager walks by a patient’s room, seeing the patient about to fall from his bed. She quickly runs to the bedside, lifting the patient back on to the bed before the patient actually falls. In doing so, the nurse manager failed to follow hand hygiene procedures requiring that hands be washed prior to touching the patient. The event came to light when a disgruntled nurse filed a risk report on the nurse manager.
SCENARIO 4
Copyright Outcome Engenuity
A physician leader at a major medical center who had significant primary clinical duties also led an educational service. She was presented with a negative performance review regarding that service by the administrator responsible for the operation of the educational service. This was presented without adhering to the written policy of having her review it before it was sent to her clinical chairman who was her boss. This negative review was used as a rationale to shut down most of the educational services and to cut costs. It appeared to the physician leader that the negative performance review of her work was used to justify a reduction of expenses, given the organization was going through very difficult financial times. Unfortunately, the negative performance review also impacted her bonus, professional advancement, and tenure track without her having the opportunity to defend her work with the facts.
SCENARIO 5
Copyright Outcome Engenuity
VALUES-BASED “DON’T DO” BREACHES
Copyright Outcome Engenuity
SCENARIO 6
A nurse arrives at the patient’s bed with two syringes in her pocket. One was prepared by the nurse at the central nurse’s station; it had no patient name or medication label. The second syringe also did not have a label, and the nurse did not know where it came from. She guessed that she must have also picked it up by mistake from the central nurse’s station. Knowing that she just prepared a medication with 2 ml of the drug, and the second unknown syringe only had 1.5 ml filled, she decided to use the unmarked syringe having 2 ml of drug.
Copyright Outcome Engenuity
A Root Cause Analysis is undertaken after a patient dies of sepsis. When the RCA did not address the many hours lacking responsiveness of the attending physician to calls by the nursing staff regarding the deteriorating patient and the lack of action when she was reached, one of the nurses brought theses issues up for discussion in the RCA. In the weeks that followed, the nurse was presented with what appeared to be a fabricated Performance Improvement Plan by his nursing supervisor and the director of HR. It was clear that this document was fabricated with damaging and inaccurate information and post-dated for prior actions. He had never seen it before and the written policy stated that such reviews should have been reviewed with the employee. He had the clear impression that the organization was weaponizing the HR department to quiet him or get him to leave. Given that the physician was employed by the hospital, he did not know what to do.
SCENARIO 7
Copyright Outcome Engenuity
Physician A and Physician B from two different institutions are undertaking collaborative research and co-author papers together. Physician A publishes a peer reviewed article to specifically discredit Physician B. The article is fraught with verifiable fabrication and falsification of information about her. Careful scrutiny reveals the article is a public sham peer review of Physician B. Physician A did not declare his conflicts of interest, prior work with Physician B, and what funding he had gained from work with Physician B, or what he could gain from the article. Physician A is rewarded by assuming positions once held by Physician B which generate personal income him. He applies for and receives federal funding of research previously undertaken by Physician B. The federal funding is granted to Physician A’s organization. Physician A’s violation of conflict of interest disclosure guidelines of the peer review journal are clear, however the article is already published and in circulation.
SCENARIO 8
Copyright Outcome Engenuity
An OB nurse had to undertake back to back shifts during a holiday weekend when other nurses were out sick. He was very fatigued and notified his supervisor of this issue and stayed at the hospital between shifts due to concerns regarding fatigue driving home. A new bar code reader was not functional for IV bags and the data had to be entered into the system manually. A checklist had been initiated to have nurses “load the IV pumps” with epidural block medication prior to the anesthesiologists arriving on the floor to undertake the procedure. The fatigued nurse made the error of accidently beginning to administer the epidural medication I.V., believing it was an antibiotic in a look alike fluid bag that was already ordered. Although the nurse immediately took responsibility for his error, another nurse caught this near miss and wrote him up for this potential medication adverse event.
SCENARIO 9
Copyright Outcome Engenuity
The CEO of a major medical center discovers that a number of researchers, who have received federal grants, have fabricated and falsified certain information in their applications. Wanting to get to the bottom of this and assess the magnitude of such behavior, she orders an audit of all grants by an outside firm. Much to her dismay, she realizes there is a significant problem and that substantial funds will have to be returned to the government. A careful review of the behaviors reveals a number of researchers do not follow the written policies and procedures regarding budgets and grant applications. When interviewed, many state “we have always done it this way”. Although there are a small number of egregious acts that are clearly intentional acts of fraud, there has been a normalization of deviance away from clear guidelines. The CEO authorizes full reimbursement of the government, however must deal with the institutionalized non-compliance of researchers regarding accurate grant submissions.
SCENARIO 10
Copyright Outcome Engenuity
OUTCOMES
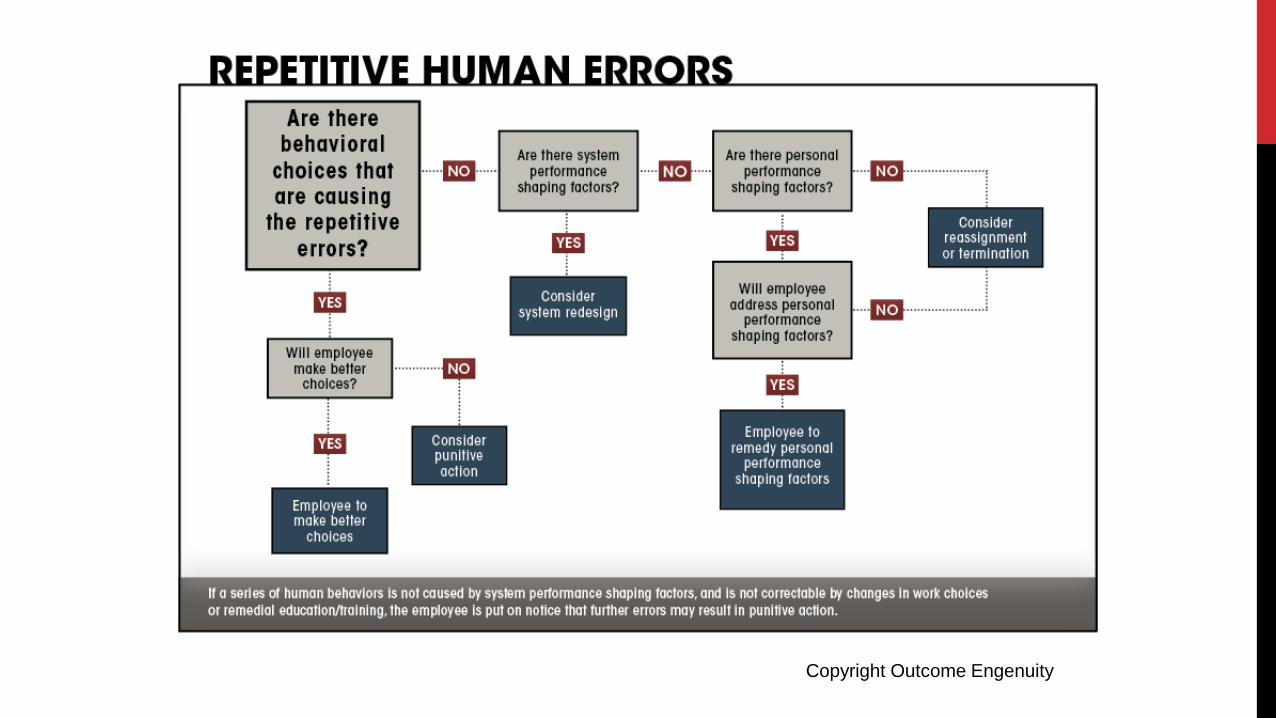
REPETITIVE ERRORS
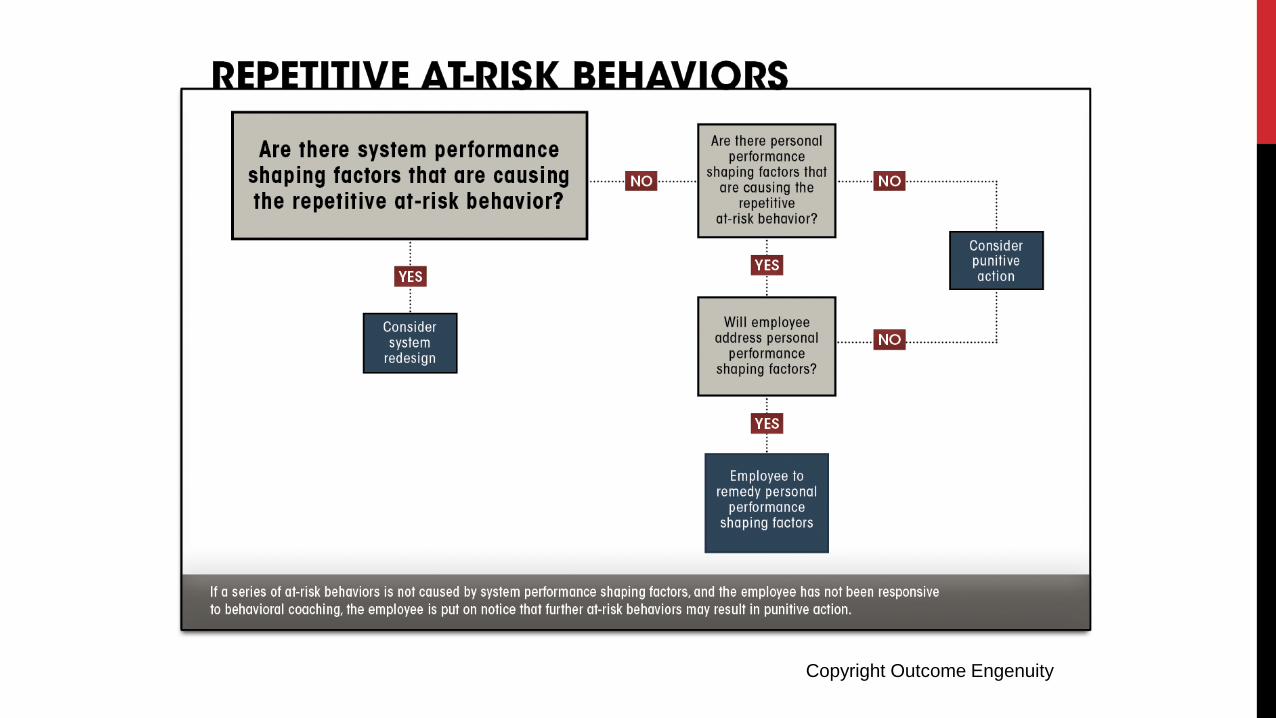
REPETITIVE AT-RISK BEHAVIORS
Copyright Outcome Engenuity
Copyright Outcome Engenuity
Copyright Outcome Engenuity

THANK YOU
© 2006 HCC, Inc. CD000000-0000XX 78 © 2018 TMIT
A New Program
The Innocence Project, founded in 1992 by Peter Neufeld and Barry Scheck at Cardozo School of Law, exonerates the wrongly convicted through DNA testing and reforms the criminal justice system to prevent future injustice.
The Healthcare Innocence Project builds on the successful model of The Innocence Project. Where it used the new technology of DNA 25 years ago, we will use the new technology of electronic records and the digital DNA in the E.H.R. and administrative records to protect the medical identity of patients and the professional identity of caregivers. Both patients and caregivers may be unjustly treated through intentional or unintentional behaviors of insiders or outsiders of healthcare organizations. They include weaponization of HR, sham peer review, discrediting patients and families after healthcare accidents, or unjust harm through outsider cybersecurity issues.
TheHealthcare Innocence Project
79 © 2018 TMIT
National Survey Questions
I am interested in MORE DETAIL regarding the: HEALTHCARE INNOCENCE PROJECT
Very Strongly
Agree
10 Strongly
Agree
9
Agree
8
Agree
7 Very
Strongly Disagree
1
Disagree
3 Strongly Disagree
2
Neutral
6
Neutral
5 Negative to Neutral
4
Specific HEALTHCARE INNOCENCE PROJECT FOCUS I would like to SEE covered includes:
80 © 2018 TMIT
National Survey Questions
I am interested in MORE DETAIL regarding: JUST CULTURE CASE STUDIES
Very Strongly
Agree
10 Strongly
Agree
9
Agree
8
Agree
7 Very
Strongly Disagree
1
Disagree
3 Strongly Disagree
2
Neutral
6
Neutral
5 Negative to Neutral
4
Specific JUST CULTURE CASE STUDY DETAIL & SCENARIOS I would like to be FURTHER covered includes:
81 © 2018 TMIT
National Survey Questions
I am interested in: END OF LIFE OPPORTUNITIES FOR IMPROVEMENT that can impact Patient and Caregiver Safety
Very Strongly
Agree
10 Strongly
Agree
9
Agree
8
Agree
7 Very
Strongly Disagree
1
Disagree
3 Strongly Disagree
2
Neutral
6
Neutral
5 Negative to Neutral
4
Specific END OF LIFE OPPORTUNITIES FOR IMPROVEMENT Information I would like to be FURTHER covered includes:

82 © 2018 TMIT
Speakers and Reactors
David Marx
Charles Denham Jennifer Dingman
John Nance Greg Botz
William Adcox
83 © 2018 TMIT
To Register or Learn More Visit: • May 2nd: sharp.com/caringmay2 • May 3rd: sharp.com/caringmay3 • Call: 858-499-4560
84 © 2018 TMIT
Voice of Patient and Family
Jennifer Dingman Founder, Persons United Limiting Sub-standards and Errors in Healthcare (PULSE), Colorado Division Co-founder, PULSE American Division TMIT Patient Advocate Team Member Pueblo, CO TMIT High Performer Webinar March 15, 2018