Juanita High School - jhs.lwsd.org · documentation for enrollment. ... Juanita High School...
10
Welcome to Juanita High School for the 2018-2019 school year. Please complete and return to the Juanita Counseling Office the following required documentation for enrollment. • Proof of Residency (please submit one of the following) o Utility bill o Closing papers o Rental agreement • Birth Certificate • Immunization Record • Unofficial Transcript from previous school o Unofficial transcript for incoming 10 th , 11 th and 12 th graders. Counselors must have this at the time of enrollment to help with credit check and scheduling classes. o Report card or academic history for incoming 9 th graders. • Withdrawal from previous school o Make sure you inform the school your student would have attended in 2018-19 that your student will not be attending for the 2018-2019 school year. • Proof of Guardianship (if applicable) • Special Needs (if applicable): Please provide a current copy of an IEP – Individual Education Plan, 504 Plan, or ELL – English Language Learner documentation. • Completed Juanita High School Enrollment Forms Juanita High School 10601 NE 132 nd Street Kirkland, WA 98034 (425)936-1600
Transcript of Juanita High School - jhs.lwsd.org · documentation for enrollment. ... Juanita High School...

Welcome to Juanita High School for the 2018-2019 school year. Please
complete and return to the Juanita Counseling Office the following required
documentation for enrollment.
• Proof of Residency (please submit one of the following) o Utility bill o Closing papers o Rental agreement
• Birth Certificate
• Immunization Record
• Unofficial Transcript from previous school o Unofficial transcript for incoming 10th, 11th and 12th graders.
Counselors must have this at the time of enrollment to help with credit check and scheduling classes.
o Report card or academic history for incoming 9th graders.
• Withdrawal from previous school o Make sure you inform the school your student would have
attended in 2018-19 that your student will not be attending for the 2018-2019 school year.
• Proof of Guardianship (if applicable)
• Special Needs (if applicable): Please provide a current copy of an IEP – Individual Education Plan, 504 Plan, or ELL – English Language Learner documentation.
• Completed Juanita High School Enrollment Forms
Juanita High School
10601 NE 132nd Street
Kirkland, WA 98034
(425)936-1600
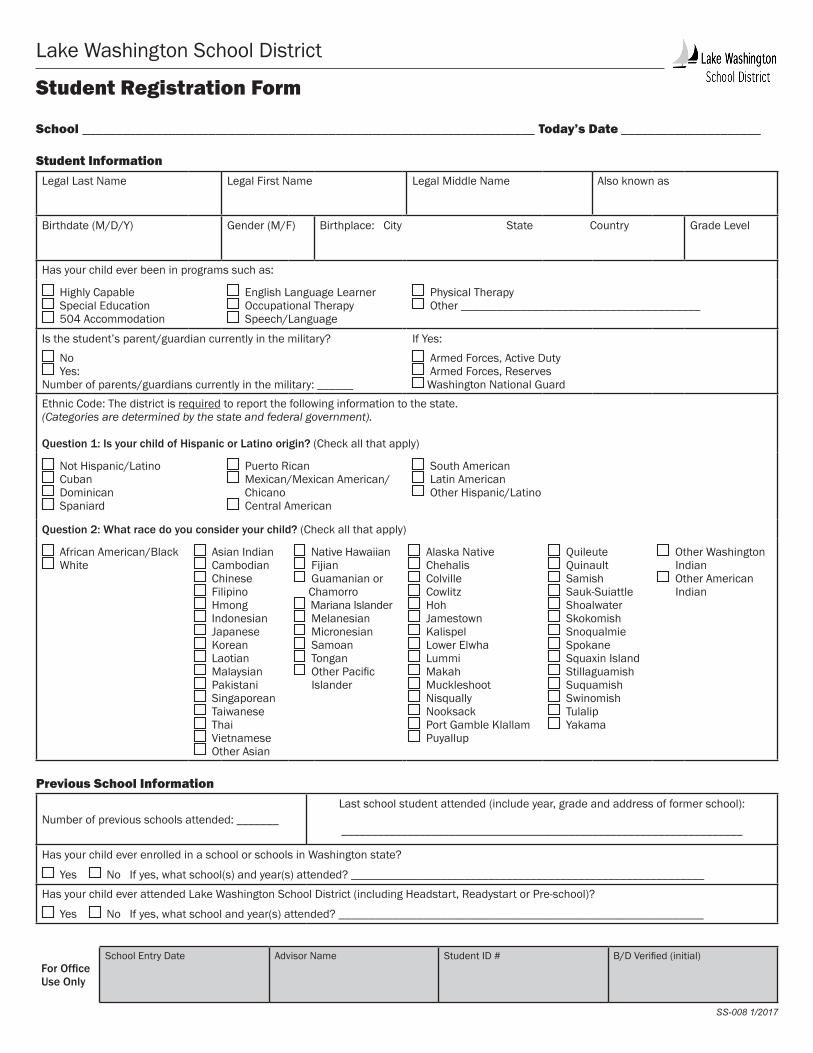
Lake Washington School District
Student Registration Form
School ____________________________________________________________________ Today’s Date _____________________
Student InformationLegal Last Name Legal First Name Legal Middle Name Also known as
Birthdate (M/D/Y) Gender (M/F) Birthplace: City State Country Grade Level
Has your child ever been in programs such as:
Highly Capable Special Education 504 Accommodation
English Language Learner Occupational Therapy Speech/Language
Physical Therapy Other ________________________________________
Is the student’s parent/guardian currently in the military?
No Yes:
Number of parents/guardians currently in the military: ______
If Yes:
Armed Forces, Active Duty Armed Forces, Reserves Washington National Guard
Ethnic Code: The district is required to report the following information to the state.(Categories are determined by the state and federal government).
Question 1: Is your child of Hispanic or Latino origin? (Check all that apply)
Not Hispanic/Latino Cuban Dominican Spaniard
Puerto Rican Mexican/Mexican American/ Chicano Central American
South American Latin American Other Hispanic/Latino
Question 2: What race do you consider your child? (Check all that apply)
African American/Black White
Asian Indian Cambodian Chinese Filipino Hmong Indonesian Japanese Korean Laotian Malaysian Pakistani Singaporean Taiwanese Thai Vietnamese Other Asian
Native Hawaiian Fijian Guamanian or
Chamorro Mariana Islander Melanesian Micronesian Samoan Tongan Other Pacific
Islander
Alaska Native Chehalis Colville Cowlitz Hoh Jamestown Kalispel Lower Elwha Lummi Makah Muckleshoot Nisqually Nooksack Port Gamble Klallam Puyallup
Quileute Quinault Samish Sauk-Suiattle Shoalwater Skokomish Snoqualmie Spokane Squaxin Island Stillaguamish Suquamish Swinomish Tulalip Yakama
Other Washington Indian
Other American Indian
Previous School Information
Number of previous schools attended: _______Last school student attended (include year, grade and address of former school):
___________________________________________________________________
Has your child ever enrolled in a school or schools in Washington state?
Yes No If yes, what school(s) and year(s) attended? ___________________________________________________________
Has your child ever attended Lake Washington School District (including Headstart, Readystart or Pre-school)?
Yes No If yes, what school and year(s) attended? _____________________________________________________________
SS-008 1/2017
For OfficeUse Only
School Entry Date Advisor Name Student ID # B/D Verified (initial)
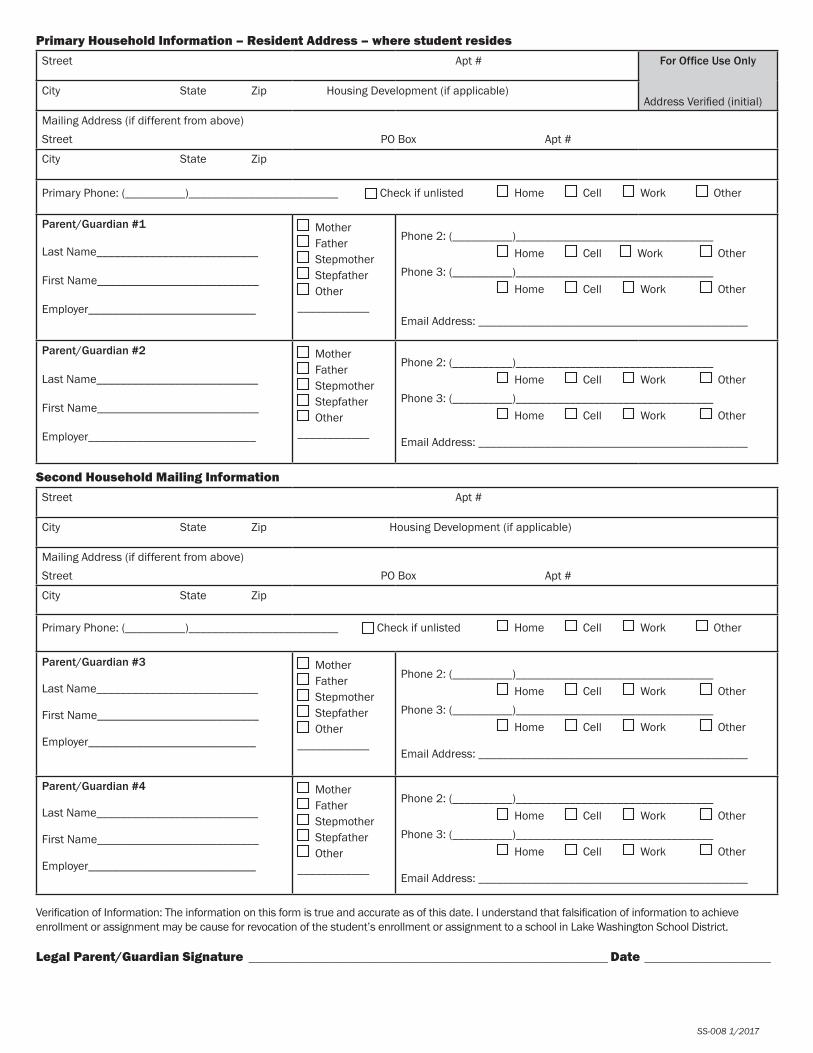
Primary Household Information – Resident Address – where student residesStreet Apt # For Office Use Only
City State Zip Housing Development (if applicable)Address Verified (initial)
Mailing Address (if different from above)Street PO Box Apt #
City State Zip
Primary Phone: (__________)_________________________ Check if unlisted Home Cell Work Other Parent/Guardian #1
Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell Work OtherPhone 3: (__________)_________________________________ Home Cell Work Other Email Address: _____________________________________________
Parent/Guardian #2
Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell Work OtherPhone 3: (__________)_________________________________ Home Cell Work Other Email Address: _____________________________________________
Second Household Mailing InformationStreet Apt #
City State Zip Housing Development (if applicable)
Mailing Address (if different from above)Street PO Box Apt #
City State Zip
Primary Phone: (__________)_________________________ Check if unlisted Home Cell Work Other
Parent/Guardian #3
Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell Work OtherPhone 3: (__________)_________________________________ Home Cell Work Other
Email Address: _____________________________________________
Parent/Guardian #4
Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell Work Other Phone 3: (__________)_________________________________ Home Cell Work Other
Email Address: _____________________________________________
Verification of Information: The information on this form is true and accurate as of this date. I understand that falsification of information to achieve enrollment or assignment may be cause for revocation of the student’s enrollment or assignment to a school in Lake Washington School District.
Legal Parent/Guardian Signature ______________________________________________________ Date ___________________
SS-008 1/2017

Lake Washington School District
Emergency Notification - SecondaryStudent Name: ____________________________________________________________________________________________ Last First Middle
Grade Level
Birthdate (MM/DD/YYYY) Gender (M/F) Teacher (Advisor/Counselor):
Primary Household Information – Resident Address – where student residesStreet Apt #
City State Zip Housing Development (if applicable)
Mailing Address (if different from above)Street PO Box Apt #
City State Zip
Primary Phone: (__________)_________________________ Check if unlisted Home Cell* Work Other
Parent/Guardian #1Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell* Work OtherPhone 3: (__________)_________________________________ Home Cell* Work OtherEmail Address: _____________________________________________
Parent/Guardian #2Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell* Work OtherPhone 3: (__________)_________________________________ Home Cell* Work OtherEmail Address: _____________________________________________
* I grant LWSD permission to use the SchoolMessenger auto-dialer system to contact me on all of the cell phones listed in the Primary Household Information section of this form. (Please note: LWSD will use SchoolMessenger to contact you with emergency messages, even if you do not check this box.)
Second Household Information (if a parent lives at an address different from primary)Street Apt #
City State Zip Housing Development (if applicable)
Mailing Address (if different from above)Street PO Box Apt #
City State Zip
Primary Phone: (__________)_________________________ Check if unlisted Home Cell** Work Other
Parent/Guardian #3Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell** Work OtherPhone 3: (__________)_________________________________ Home Cell** Work Other Email Address: _____________________________________________
Parent/Guardian #4Last Name___________________________
First Name___________________________
Employer____________________________
Mother Father Stepmother Stepfather Other
____________
Phone 2: (__________)_________________________________ Home Cell** Work Other Phone 3: (__________)_________________________________ Home Cell** Work Other Email Address: _____________________________________________
**Please note: The Second Household will use an online process through Parent Access to confirm permission to call cell phones using the SchoolMessenger auto-dialer system.
Please fill out other side →

Emergency ContactsWhen injury or illness involving your child occurs, we want to be able to quickly reach families or other responsible adults. In the event we cannot reach a parent/guardian, please list person(s) you trust who are available during the day to provide care for your child. We suggest at least one local contact and one out of state contact. Please be sure to list anyone who may need to pick your child up from school (i.e., carpool drivers).
1. Name: Relationship: Phone: (__________)_____________________2. Name: Relationship: Phone: (__________)_____________________3. Name: Relationship: Phone: (__________)_____________________Student Release Authorization: In the event the school is unable to contact the parent/guardian, I authorize the school to release my student to the person(s) listed above. For grades 6-8, in the event of an unanticipated dismissal of school we will attempt to contact parents/guardians. If we are unable to reach you, please indicate if your student has permission to:
bus home (if buses run early) walk home Siblings in DistrictName: School:Name: School:Name: School:
Verification of Information: The information on this form is true and accurate as of this date. I understand that falsification of information to achieve enrollment or assignment may be cause for revocation of the student’s enrollment or assignment to a school in Lake Washington School District.
Legal Parent/Guardian Signature ______________________________________________________ Date ___________________
Please notify your student’s school if any of the information on this form changes during the school year.
1238A | Revised 6/2016
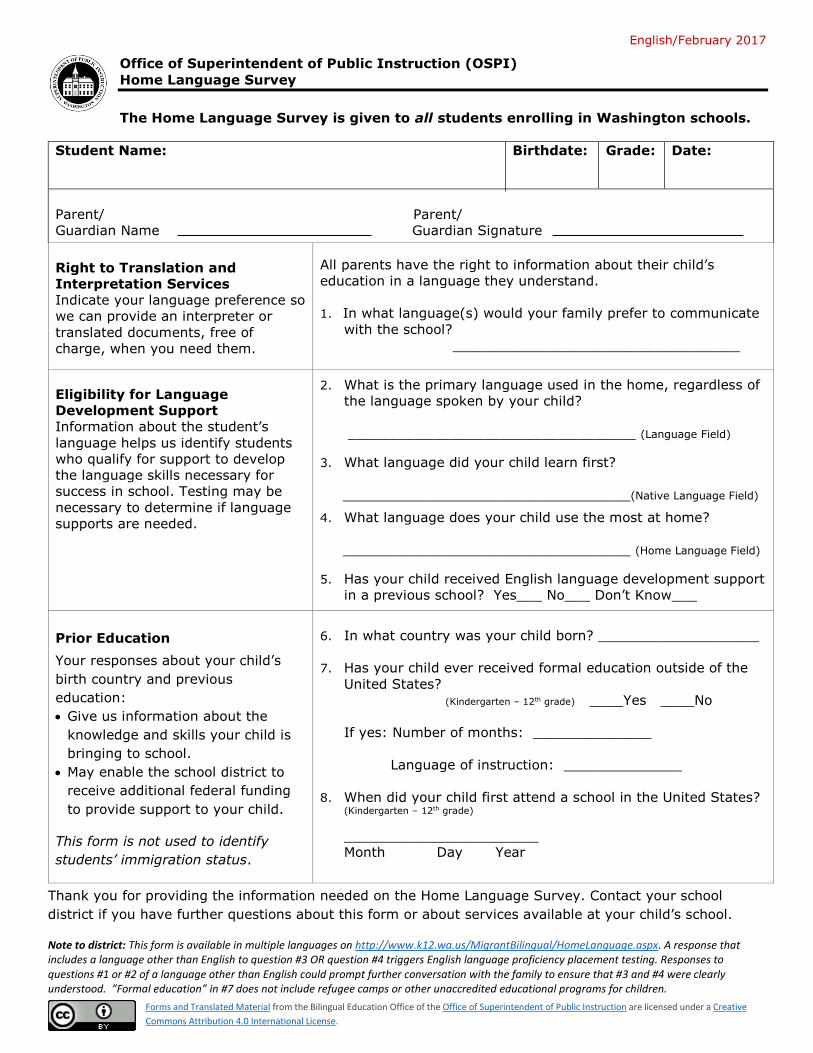
English/February 2017
Office of Superintendent of Public Instruction (OSPI)
Home Language Survey
The Home Language Survey is given to all students enrolling in Washington schools.
Student Name: Birthdate: Grade: Date:
Parent/ Parent/
Guardian Name Guardian Signature
Right to Translation and
Interpretation Services
Indicate your language preference so
we can provide an interpreter or
translated documents, free of
charge, when you need them.
All parents have the right to information about their child’s
education in a language they understand.
1. In what language(s) would your family prefer to communicate
with the school?
__________________________________
Eligibility for Language
Development Support
Information about the student’s
language helps us identify students
who qualify for support to develop
the language skills necessary for
success in school. Testing may be
necessary to determine if language
supports are needed.
2. What is the primary language used in the home, regardless of
the language spoken by your child?
__________________________________ (Language Field)
3. What language did your child learn first?
__________________________________(Native Language Field)
4. What language does your child use the most at home?
__________________________________ (Home Language Field)
5. Has your child received English language development support
in a previous school? Yes___ No___ Don’t Know___
Prior Education
Your responses about your child’s
birth country and previous
education:
Give us information about the
knowledge and skills your child is
bringing to school.
May enable the school district to
receive additional federal funding
to provide support to your child.
This form is not used to identify
students’ immigration status.
6. In what country was your child born? ___________________
7. Has your child ever received formal education outside of the
United States?
(Kindergarten – 12th grade) ____Yes ____No
If yes: Number of months: ______________
Language of instruction: ______________
8. When did your child first attend a school in the United States? (Kindergarten – 12th grade)
_______________________
Month Day Year
Thank you for providing the information needed on the Home Language Survey. Contact your school
district if you have further questions about this form or about services available at your child’s school.
Note to district: This form is available in multiple languages on http://www.k12.wa.us/MigrantBilingual/HomeLanguage.aspx. A response that includes a language other than English to question #3 OR question #4 triggers English language proficiency placement testing. Responses to questions #1 or #2 of a language other than English could prompt further conversation with the family to ensure that #3 and #4 were clearly understood. ”Formal education” in #7 does not include refugee camps or other unaccredited educational programs for children.
Forms and Translated Material from the Bilingual Education Office of the Office of Superintendent of Public Instruction are licensed under a Creative
Commons Attribution 4.0 International License.

Certificate of Immunization Status (CIS) DOH 348-013 January 2010
Please print. See back for instructions on how to fill out this form or get it printed from the Immunization Registry. Child’s Last Name: First Name: Middle Initial: Birthdate (mm/dd/yyyy): Sex:
I certify that the information provided on this form is correct and verifiable.
Parent/Guardian Signature Required Date
Symbols below: Required for School and Child Care/Preschool Required for Child Care/Preschool Only
Parent/Guardian Name (please print):
Vaccine Dose Date
Month Day Year Hepatitis B (Hep B) 1 2 3 or Hep B - 2 dose alternate schedule for teens 1 2 Rotavirus (RV1, RV5) 1 2 3 Diphtheria, Tetanus, Pertussis (DTaP, DTP, DT) 1 2 3 4 5 Tetanus, Diphtheria, Pertussis (Tdap, Td) 1 2 Haemophilus influenzae type b (Hib) 1 2 3 4 Pneumococcal (PCV, PPSV) 1 2 3 4
Vaccine Dose Date
Month Day Year Polio (IPV, OPV) 1 2 3 4
Influenza (flu, most recent)
Measles, Mumps, Rubella (MMR) 1 2
Varicella (chickenpox) or verify disease 1-4 1 2
Hepatitis A (Hep A)
1
2
Meningococcal (MCV, MPSV)
1
Human Papillomavirus (HPV) 1 2 3
Office Use Only: Immunization information updated and verified with parent/guardian permission:
Printed Staff Name Date
Printed Staff Name Date
Printed Staff Name Date
Printed Staff Name Date
If the child named on this CIS had chickenpox disease (and not the vaccine), disease history must be verified. Mark option 1, 2, 3, OR 4 below – see, back #5.
1) Chickenpox disease verified by printout
from CHILD Profile Immunization Registry
Must be marked by printout (not by hand) to be valid.
2) Chickenpox disease verified by Health
Care Provider (HCP) If you choose this box, mark 2A OR 2B below.
2A) Signed note from HCP attached OR
2B) HCP signed here and print name below: Licensed health care provider (HCP) Signature Date (MD, DO, ND, PA, ARNP)
HCP Printed Name: _______________________________
3) Chickenpox disease verified by school
staff from CHILD Profile Immunization Registry
If you choose this box, staff must initial that parent or guardian approves: __________(initial) _________(date)
4) Chickenpox disease verified by parent*
If you choose this box, fill in the date or child’s age when he or she had the disease:
Age/Date of disease:_______________________
*Can ONLY verify for some grades, see back #5 (4).
If the child can show immunity by blood test (titer) and hasn’t had the vaccine, ask your HCP to fill in this box.
Documentation of Disease Immunity
I certify that the child named on this CIS has laboratory evidence of immunity (titer) to the diseases marked. Signed lab report(s) MUST also be attached.
Diphtheria Hepatitis A Hepatitis B Hib Measles
Mumps Polio Rubella Tetanus Varicella
Other:
_______________
_______________
Licensed health care provider (HCP) Signature Date (MD, DO, ND, PA, ARNP)
HCP Printed Name: _______________________________
Office Use Only:
Reviewed by: Date:
Signed Cert. of Exemption on file? Yes No
EXAMPLE
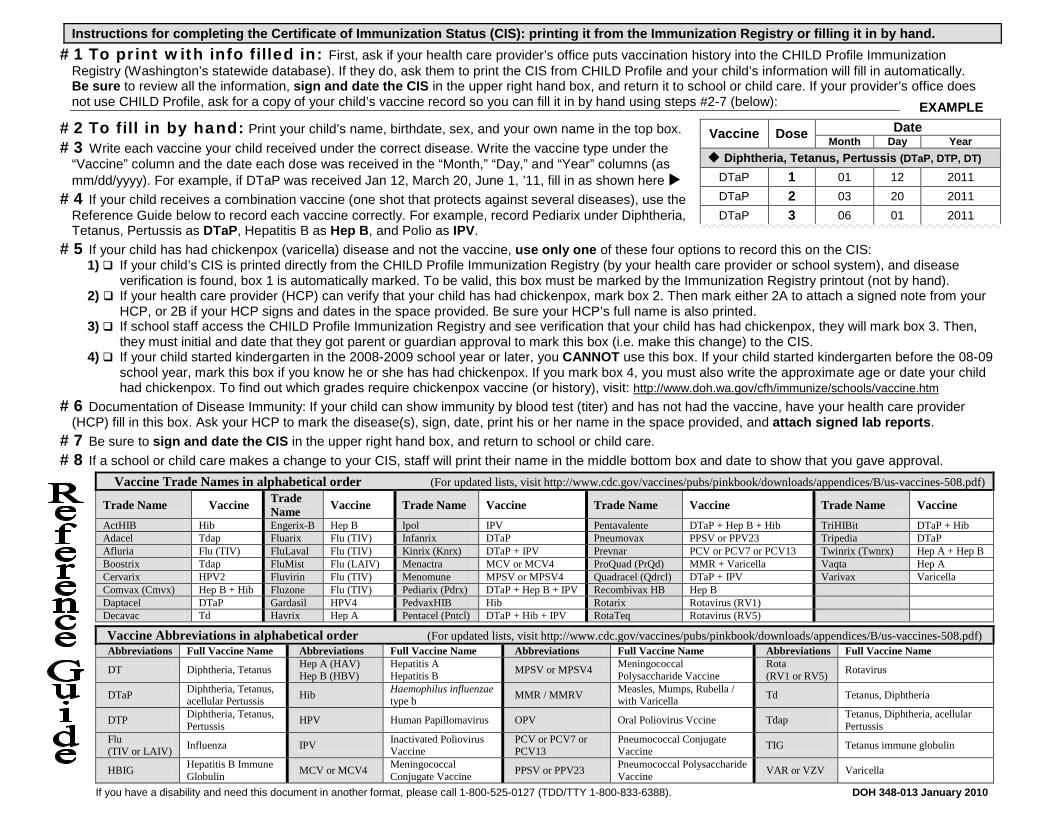
Instructions for completing the Certificate of Immunization Status (CIS): printing it from the Immunization Registry or filling it in by hand.
#1 To print with info filled in: First, ask if your health care provider’s office puts vaccination history into the CHILD Profile Immunization Registry (Washington’s statewide database). If they do, ask them to print the CIS from CHILD Profile and your child’s information will fill in automatically. Be sure to review all the information, sign and date the CIS in the upper right hand box, and return it to school or child care. If your provider’s office does not use CHILD Profile, ask for a copy of your child’s vaccine record so you can fill it in by hand using steps #2-7 (below):
#2 To fill in by hand: Print your child’s name, birthdate, sex, and your own name in the top box. #3 Write each vaccine your child received under the correct disease. Write the vaccine type under the
“Vaccine” column and the date each dose was received in the “Month,” “Day,” and “Year” columns (as mm/dd/yyyy). For example, if DTaP was received Jan 12, March 20, June 1, ’11, fill in as shown here
#4 If your child receives a combination vaccine (one shot that protects against several diseases), use the Reference Guide below to record each vaccine correctly. For example, record Pediarix under Diphtheria, Tetanus, Pertussis as DTaP, Hepatitis B as Hep B, and Polio as IPV.
#5 If your child has had chickenpox (varicella) disease and not the vaccine, use only one of these four options to record this on the CIS: 1) If your child’s CIS is printed directly from the CHILD Profile Immunization Registry (by your health care provider or school system), and disease
verification is found, box 1 is automatically marked. To be valid, this box must be marked by the Immunization Registry printout (not by hand). 2) If your health care provider (HCP) can verify that your child has had chickenpox, mark box 2. Then mark either 2A to attach a signed note from your
HCP, or 2B if your HCP signs and dates in the space provided. Be sure your HCP’s full name is also printed. 3) If school staff access the CHILD Profile Immunization Registry and see verification that your child has had chickenpox, they will mark box 3. Then,
they must initial and date that they got parent or guardian approval to mark this box (i.e. make this change) to the CIS. 4) If your child started kindergarten in the 2008-2009 school year or later, you CANNOT use this box. If your child started kindergarten before the 08-09
school year, mark this box if you know he or she has had chickenpox. If you mark box 4, you must also write the approximate age or date your child had chickenpox. To find out which grades require chickenpox vaccine (or history), visit: http://www.doh.wa.gov/cfh/immunize/schools/vaccine.htm
#6 Documentation of Disease Immunity: If your child can show immunity by blood test (titer) and has not had the vaccine, have your health care provider (HCP) fill in this box. Ask your HCP to mark the disease(s), sign, date, print his or her name in the space provided, and attach signed lab reports.
#7 Be sure to sign and date the CIS in the upper right hand box, and return to school or child care. #8 If a school or child care makes a change to your CIS, staff will print their name in the middle bottom box and date to show that you gave approval.
Vaccine Trade Names in alphabetical order (For updated lists, visit http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/B/us-vaccines-508.pdf)
Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine
ActHIB Hib Engerix-B Hep B Ipol IPV Pentavalente DTaP + Hep B + Hib TriHIBit DTaP + Hib Adacel Tdap Fluarix Flu (TIV) Infanrix DTaP Pneumovax PPSV or PPV23 Tripedia DTaP Afluria Flu (TIV) FluLaval Flu (TIV) Kinrix (Knrx) DTaP + IPV Prevnar PCV or PCV7 or PCV13 Twinrix (Twnrx) Hep A + Hep B Boostrix Tdap FluMist Flu (LAIV) Menactra MCV or MCV4 ProQuad (PrQd) MMR + Varicella Vaqta Hep A Cervarix HPV2 Fluvirin Flu (TIV) Menomune MPSV or MPSV4 Quadracel (Qdrcl) DTaP + IPV Varivax Varicella Comvax (Cmvx) Hep B + Hib Fluzone Flu (TIV) Pediarix (Pdrx) DTaP + Hep B + IPV Recombivax HB Hep B Daptacel DTaP Gardasil HPV4 PedvaxHIB Hib Rotarix Rotavirus (RV1) Decavac Td Havrix Hep A Pentacel (Pntcl) DTaP + Hib + IPV RotaTeq Rotavirus (RV5)
Vaccine Abbreviations in alphabetical order (For updated lists, visit http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/B/us-vaccines-508.pdf) Abbreviations Full Vaccine Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine Name
DT Diphtheria, Tetanus Hep A (HAV) Hep B (HBV)
Hepatitis A Hepatitis B MPSV or MPSV4 Meningococcal
Polysaccharide Vaccine Rota (RV1 or RV5) Rotavirus
DTaP Diphtheria, Tetanus, acellular Pertussis Hib Haemophilus influenzae
type b MMR / MMRV Measles, Mumps, Rubella / with Varicella Td Tetanus, Diphtheria
DTP Diphtheria, Tetanus, Pertussis HPV Human Papillomavirus OPV Oral Poliovirus Vccine Tdap Tetanus, Diphtheria, acellular
Pertussis Flu (TIV or LAIV) Influenza IPV Inactivated Poliovirus
Vaccine PCV or PCV7 or PCV13
Pneumococcal Conjugate Vaccine TIG Tetanus immune globulin
HBIG Hepatitis B Immune Globulin MCV or MCV4 Meningococcal
Conjugate Vaccine PPSV or PPV23 Pneumococcal Polysaccharide Vaccine VAR or VZV Varicella
If you have a disability and need this document in another format, please call 1-800-525-0127 (TDD/TTY 1-800-833-6388). DOH 348-013 January 2010
Vaccine Dose Date
Month Day Year Diphtheria, Tetanus, Pertussis (DTaP, DTP, DT)
DTaP 1 01 12 2011 DTaP 2 03 20 2011 DTaP 3 06 01 2011

02/18
FRESHMAN JUANITA HIGH SCHOOL COURSE SELECTION WORKSHEET
Student Name: ______________________________________________________
THIS IS THE FINAL COPY OF YOUR COURSE SELECTION WORKSHEET AND MUST BE TURNED IN FOR REGISTRATION FOR NEXT SCHOOL YEAR. PLEASE BE SURE THAT ALL SIGNATURES HAVE BEEN OBTAINED. REVIEW YOUR REQUESTS CAREFULLY AND READ THE STATEMENT IN THE BOX BELOW BEFORE SUBMITTING THIS WORKSHEET. NOTE THAT YOU MUST SIGN UP FOR 7 CLASSES EACH SEMESTER.
SEMESTER 1: SEMESTER 2:
TITLE OF COURSE
Teacher INITIAL
TITLE OF COURSE
Teacher INITIAL
*
ALTERNATES:
You must choose 6 different ELECTIVE alternates. Please note: There is no priority ranking to the alternate choices.
Title of Alternate ELECTIVE Course: Title of Alternate ELECTIVE Course:
__________________________________________ __________________________________________
__________________________________________ __________________________________________
__________________________________________ __________________________________________
Parents and Students, Please note that teachers will be assigned to specific classes at JHS based on student requests for courses. Students should select courses carefully. Requests for schedule changes that deviate from the courses selected on this Course Selection Worksheet cannot be granted.
I have reviewed my graduation requirements and request the above courses for next year.
Student Signature _______________________________________________ Date _____/_____/_____
Parent Signature ________________________________________________ Date _____/_____/_____
ELECTIVE:
ENGLISH:
Final
*** DUE ON WEDNESDAY, FEBRUARY 14, 2018 ***
MATH:
ENGLISH:
SOCIAL STUDIES:
MATH:
SCIENCE: SCIENCE:
(choose one)
(choose one)
Honors English 9 English 9 English 9
Honors English 9
World History (1 semester) Hon World History (year) Honors World History (year)
__________________ (1 semester)
Biology in the Earth System Biology in the Earth System
PE:* HEALTH:* Physical Education 1 Health
ELECTIVE:
ELECTIVE:
ELECTIVE:
ELECTIVE:
* PE 1 and Health are recommended classes for all 9th graders and fulfill specific graduation requirements.
See back of this sheet for a list of all classes available to freshmen. “ELECTIVE” above includes any class listed on the back.
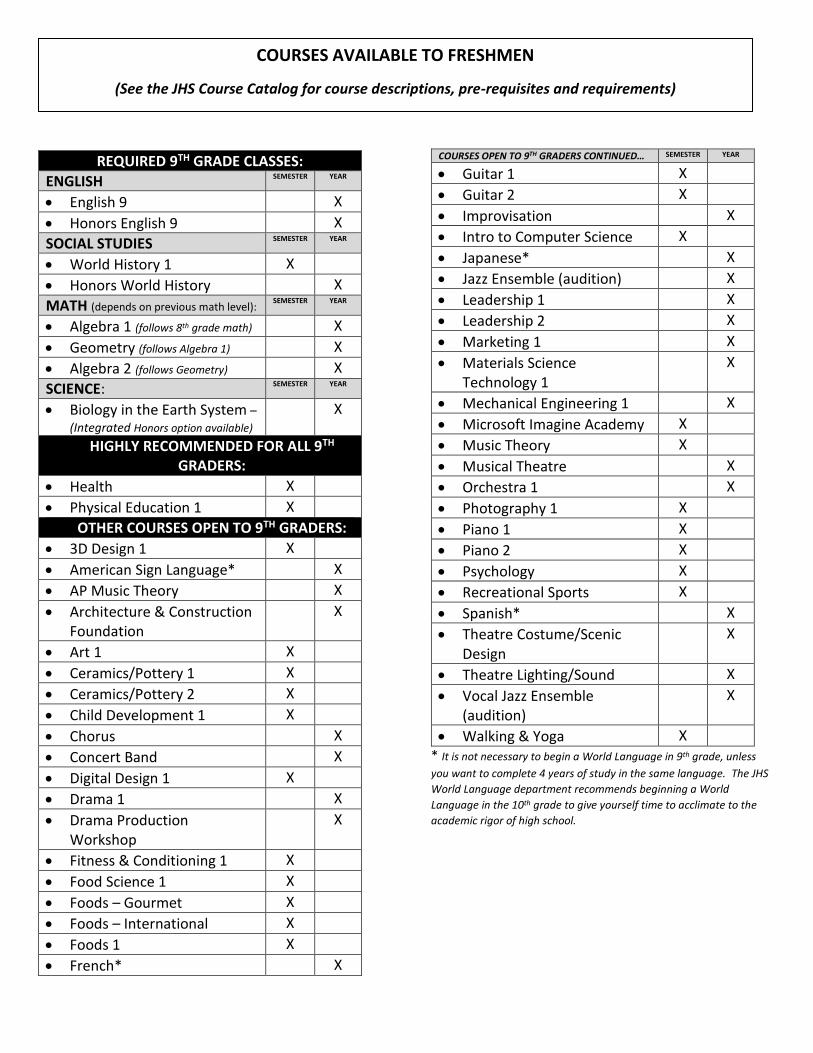
REQUIRED 9TH GRADE CLASSES:
ENGLISH SEMESTER YEAR
• English 9 X
• Honors English 9 X
SOCIAL STUDIES SEMESTER YEAR
• World History 1 X
• Honors World History X
MATH (depends on previous math level): SEMESTER YEAR
• Algebra 1 (follows 8th grade math) X
• Geometry (follows Algebra 1) X
• Algebra 2 (follows Geometry) X
SCIENCE: SEMESTER YEAR
• Biology in the Earth System –
(Integrated Honors option available) X
HIGHLY RECOMMENDED FOR ALL 9TH GRADERS:
• Health X
• Physical Education 1 X
OTHER COURSES OPEN TO 9TH GRADERS:
• 3D Design 1 X
• American Sign Language* X
• AP Music Theory X
• Architecture & Construction Foundation
X
• Art 1 X
• Ceramics/Pottery 1 X
• Ceramics/Pottery 2 X
• Child Development 1 X
• Chorus X
• Concert Band X
• Digital Design 1 X
• Drama 1 X
• Drama Production Workshop
X
• Fitness & Conditioning 1 X
• Food Science 1 X
• Foods – Gourmet X
• Foods – International X
• Foods 1 X
• French* X
COURSES OPEN TO 9TH GRADERS CONTINUED… SEMESTER YEAR
• Guitar 1 X
• Guitar 2 X
• Improvisation X
• Intro to Computer Science X
• Japanese* X
• Jazz Ensemble (audition) X
• Leadership 1 X
• Leadership 2 X
• Marketing 1 X
• Materials Science Technology 1
X
• Mechanical Engineering 1 X
• Microsoft Imagine Academy X
• Music Theory X
• Musical Theatre X
• Orchestra 1 X
• Photography 1 X
• Piano 1 X
• Piano 2 X
• Psychology X
• Recreational Sports X
• Spanish* X
• Theatre Costume/Scenic Design
X
• Theatre Lighting/Sound X
• Vocal Jazz Ensemble (audition)
X
• Walking & Yoga X * It is not necessary to begin a World Language in 9th grade, unless
you want to complete 4 years of study in the same language. The JHS
World Language department recommends beginning a World
Language in the 10th grade to give yourself time to acclimate to the
academic rigor of high school.
COURSES AVAILABLE TO FRESHMEN
(See the JHS Course Catalog for course descriptions, pre-requisites and requirements)