Journey into International Health -Seminar of Public Health - Univ Miami May 2015
94
1 Totoro, Ya Hariri! A Journey to International Health Leopoldo Villegas MD, DTM&H, MSc, DrPH, AdvPHM Senior International Health Advisor
-
Upload
leopoldo-villegas-md-dtmh-msc-drph-advdphm -
Category
Documents
-
view
26 -
download
1
Transcript of Journey into International Health -Seminar of Public Health - Univ Miami May 2015

1
Totoro, Ya Hariri!A Journey to International Health
Leopoldo Villegas MD, DTM&H, MSc, DrPH, AdvPHM
Senior International Health Advisor

2
1
Content
The beginning
2 The opportunity
3 The consolidation
4 The expertise
5 The way forward

The beginning

Advantages:
• Ability to provide service and support to others
• Save lives
• Continuous learning
• Opportunity to appreciate medical science
• Teach students and patients about medicine
• Rewarding
• Decent salary
• High status occupation
Disadvantages:
• DEBT
• Long education.
• Long process to acquire a license
• Difficult
• Stressful
• Depressing when you are unable to help
• Time consuming
• Long hours
• A great deal of responsibility
• Managed care means more difficulty earning a
high salary
• Very significant student loans (hundreds of
thousands of dollars)
Studying Medicine

Yanomami
https://bluestockingbrazil.files.wordpress.com/2011/08/yanomami2peq.jpg

Health Problems
• Fever
• ARI
• Otitis
• Diarrhea
• Malnutrition
• Malaria
• Onchocerciasis
• Helminths
• Tungiasis
• Scabies

7Yanomami

8

9

Parasites Mosquitoes Human

11

Malaria 1993-1995 0135
Alto Orinoco – Ministerio de Salud - Venezuela
95%Main cause of death
64%Splenomegaly
21%Malaria Prevalence
High Anemia rate >60% (2-9 years)
associated with Hyperreactive Malarious Syndrome (HMS)

Actions
Why so many deaths after using the right treatment?
Why so many cases of severe anemia?
How to solve the problem?
Documented the malaria epidemiology Vectors
Parasites
Ecology
Human
?

14

Results
Investigated malaria response to treatment (in vitro)
Identified poor response and 100% resistance in vitro to chloroquine –
first line treatment for malaria
Disseminated the findings
No well-received by politicians at MOH
No changes in treatment policies – death rate increased over time
New treatment provided by religious missions
Rapid improvement after treatment – children < 5 y
Changed MOH staff – recognition of “resistant” of the MOH
Temporary policy change for treatment of malaria in the Yanomami area

The Opportunity

17

18
MSc 1996 – DTM&H 1996 – DrPH 2001

19

20
Umpang
B U R M A
C H I N A
I N D I A
PAKISTAN
I N D O N E S I A
S U M A T R A
T H A I L A N D
B U R M A
L A O S
M A
L A Y S I A
SINGAPORE
C A M B O D I A
V I E T N A
M
G U L F O F S I A M
G U L F
O F
T O N K I N
A N D A M A N
S E A
B A Y
O F
B E N G A L
S O
U T
H C
H I
N A
S E
A
Singapore
Phnom
Penh
Bangkok
Vientiane
Hanoi
Rangoon
Kuala Lumpur
HO CHI MINH CITY
N
Country Capital-
BURMA, THAILAND, LAOS,
CAMBODIA, VIETNAM,
SINGAPORE and MALAYSIA
0 50 100 150 200 MI
0 50 100 200 300KM
Huey Haeng
Mae Ok Hu
Pop Pra
Maela Camp Mae Ra Mat Tak
Mae Sod
Perng Klerng
Ti Po Ji
Wa Lay
UmPiem Camp
Saw-O
Myawady
Tee No Ko
Huey Plakong
No Bo
Ta song Yang
HueyMi
Huey Namkun
Nu Po Camp
Munruchai
Mae Jan
Thai-Karen villages
Mae La camp

21icfi.com |
Host
Parasite
Drug
Inmune Response Pharmacodynamics
Pharmacokinetics
Malaria Treatment

Resistance to antimalarial drugs
E %
C

23icfi.com |
C H I N A
I N D I A
PA KISTAN
I N D O N E S I A
S U M A
T R A
T H A I L A N D
B U R M A
L A O S
M A
L A Y S I A
SIN GA POR E
C A M B O D I A
V I E T N A M
G U L F O F S I A M
G U L F
O F
T O N K I N
A N D A M A N
S E A
B A Y
O F
B E N G A L
S O
U T
H
C H
I N
A
S E
A
Singapore
Phnom
Penh
Bangkok
Vientiane
Hanoi
Rangoon
Kuala Lumpur
HO CHI MINH CITY
N
Country Capital-
BURMA, THAILAND, LAOS,
CAMBODIA, VIETNAM,
SINGAPORE and MALAYSIA
0 50 100 150 200 MI
0 50 100 200 300KM
Resistance in vivo
F (SP)
MSP
Q
M
CQ
Multidrug resistant Malaria SE Asia
Art

24
50
60
70
80
90
100
M15
M25
MAS3
Efficacy (%)

25
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
PF
PV
MIX
M25
MAS3
% of patients treated with M+A combination
IBN
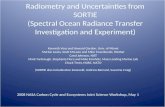
cases/person/yr
year
26
50 60 70 80 90 100
Cure rate (%)
0
0.2
0.4
0.6
0.8
1
1.2P.f. infections/ person/ year
r2 = 0.68
SHOKLO

27

28
5 lost to follow up
1 refused
1 placenta previa
1 abortion
450 completed surveillance
1 poor compliance
33 lost to follow up
4 withdrew consent
3 side effects +1 died
492 received placebo
500 assigned placebo
3 lost to follow up
1 delivery
1 cerebral malaria
3 abortions
460 completed surveillance
2 poor compliance
23 lost to follow up
6 withdrew consent
1 side effect
492 received chloroquine
500 assigned chloroquine
1000 pregnant women
randomised
2946
Pregnant women available Figure 6.4. Kaplan-Meier intent-to-treat analysis of parasite-free survival.
403020100
1.00
.90
.80
Cum
ula
tive
pro
port
ion a
par
asit
aem
ic
Log Rank test =36.82; df =1; p<0.0001
Placebo
Chloroquine
Time since started prophylaxis (weeks)
Chloroquine prophylaxis against vivax malaria among
pregnant women – CP trial

The Consolidation

Instituto de Altos Estudios
“Dr. Arnoldo Gabaldon”
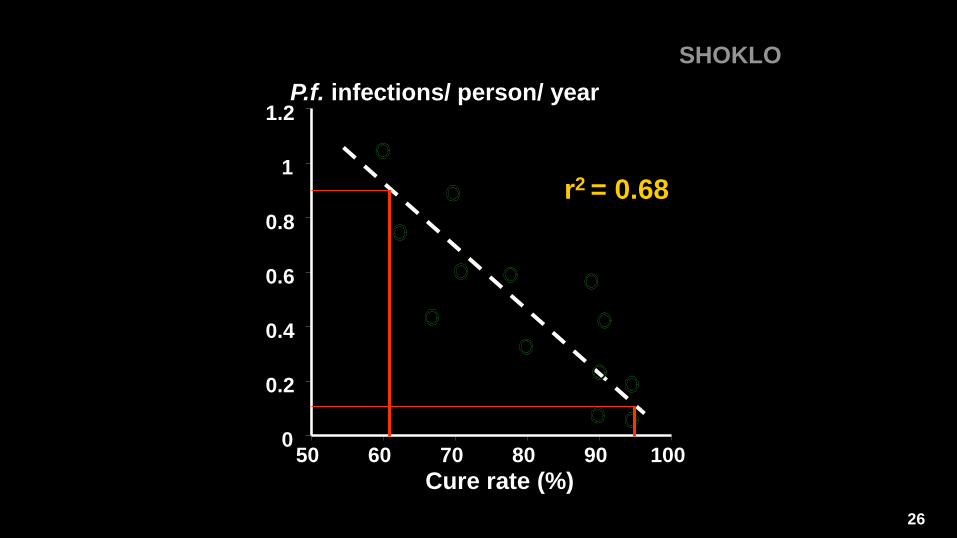
South American Network
Sentinel site
RAVREDA/AMI

25
50
75
100
Efficacy
%CQ AMO SP Q M CQSP AMOSP QDOX QCL ASSP ASDOX ASM ARTLUM
Overall Results Efficacy studies P. falciparum

33icfi.com |
Antimalarial drug resistance in the Amazon basin, 2006
CQ
SP
Q (+D, Cl)
M
AMO
MAS
P. falciparum

34
Antimalarial drug resistance profiles

35
Artesunate+Mefloquine
vs. Coartem®
Artesunate + Mefloquine
Coartem®
First line treatment for P. falciparum in the Amazon región
Artesunate + SP

The Expertise

37icfi.com |
Smallest independent country in South America
• part of the Guyanan Shield
• 163 821 km2
80% of the territory is tropical rainforest
Estimated population (2010)= 524,000 inh.
Mixed population:
• Creole, Chinese, Amerindians, Indians, Javanese,
Lebanese, Jewish, Brazilian and Dutch descendants.
Economy based mainly in bauxite, caolin, and gold.
Suriname

38icfi.com |
Malaria has been a public health problem in Suriname
Successful malaria control program eradicated malaria
from the coastal area (1968)
Malaria transmission has been mainly in communities
living in the interior
Parasites species: Pf > Pv > Pm > Mixed
Vectors: Anopheles darlingi – primary vector
Excellent environmental conditions
Malaria in Suriname
Coastal
Interior

39icfi.com |
Malaria Strategy – until 2005The country strategy for malaria control includes:
Adequate and prompt diagnosis and effective treatment
Vector control: Insecticide-treated nets, entomological surveillance
Information, Education and Communication– Behavior Change
Communication (IEC/BCC)
Intelligent surveillance, detection and respond to epidemics
• Stratification and implementation of tailored-made interventions
Monitoring and Evaluation: interventions, drug and insecticide resistance and
operational research

40icfi.com |
Malaria in Suriname, 1965-2004
0
2000
4000
6000
8000
10000
12000 Guerilla war
CQ
resistance
War
ended
41icfi.com |
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Gold miner
s
LLNs, ACD, IRS, Media, KOTAB, P
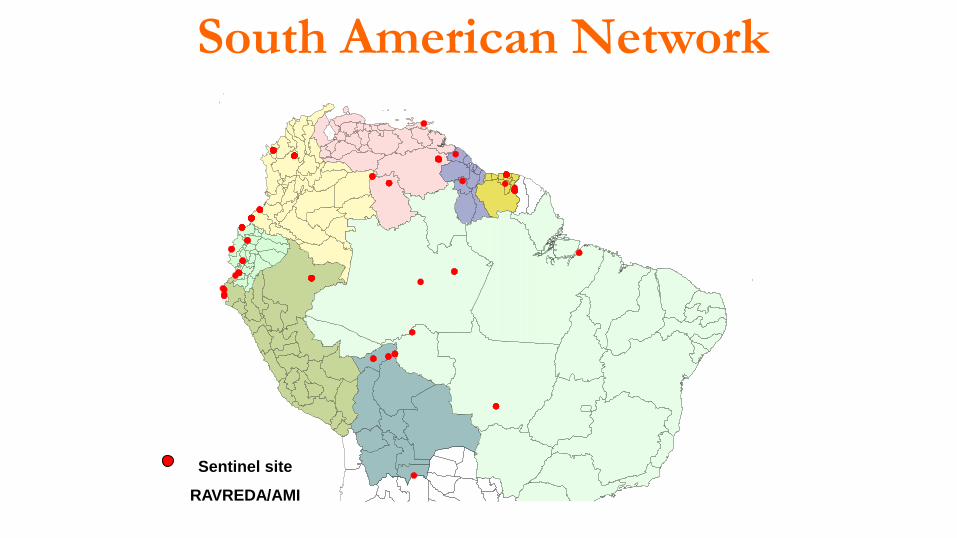
What happened between 2000-2004?
Pre ACT ACT Plus
Flooding
•Several epidemics in the interior
• Treatment failures – Quinine
•Stock out of medicines -common
•Limited funding for operational activities
•Malaria control - case management
•ACT trials in 2003
•Approved R4 GF
•No previous experience on performance-
based funding
•Malaria cases started going down
42icfi.com |
Stratification

43icfi.com |
18th Meeting of the RBM Partnership
Monitoring and Evaluation Reference Group (MERG)
cases %
STOELMANSEILAND 963 15,3
APOEMA 679 10,8
GAKABA 679 10,8
DRIETABIKI 523 8,3
BROWNSWEG 434 6,9
LANGATABIKI 319 5,1
KWAMALASAMUTU 276 4,4
Total 3873 61,6
7 Poli = 61,6% malaria
63 localities - 60% malaria
Priorities

44icfi.com |
Methodology similar to the malaria eradication program - 1950s
Interventions
• IRS
• Diagnosis
• Treatment
• Local/community participation
Important
• Good logistic system
• Adequate funding
• Knowing your population
• Adapt and implement what works
• Supervision - Monitoring
Management
• Strong leadership
• Commitment
• Political will
• Trained fully dedicated staff
• Strong surveillance system
• Stratification to the lowest ADM level
possible
• Mapping
• Priorities

45icfi.com |
ACD/PCD
IRS
ACT+P
Mobile surveys
LLINs
BCC/IEC
PCD
ACT+P
LLINs
BCC/IEC
PCD
ACT+P
LLINs
BCC/IEC
Combination of interventionsMOH Suriname, 2004

46icfi.com |
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
MSDPf/Pv RDT
LLNs, ACD, IRS, Media, KOTAB, P
LLINsReplacement
Malaria Interventions in Suriname, 2000-2013Pre ACT ACT Plus
Flooding
2013

47icfi.com |
2000
47
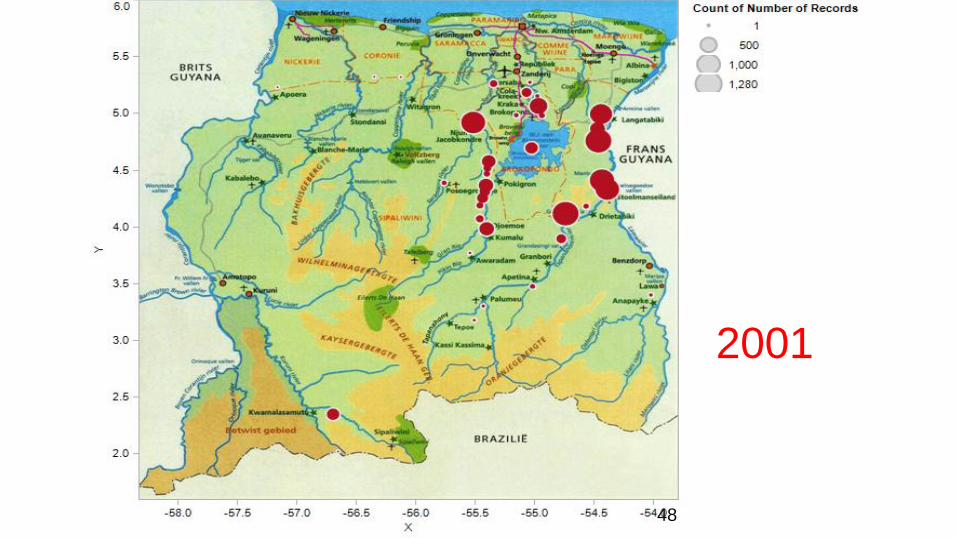
48icfi.com |
2001
48

49icfi.com |
2002
49

50icfi.com |
2003
50

51icfi.com |
2004
51
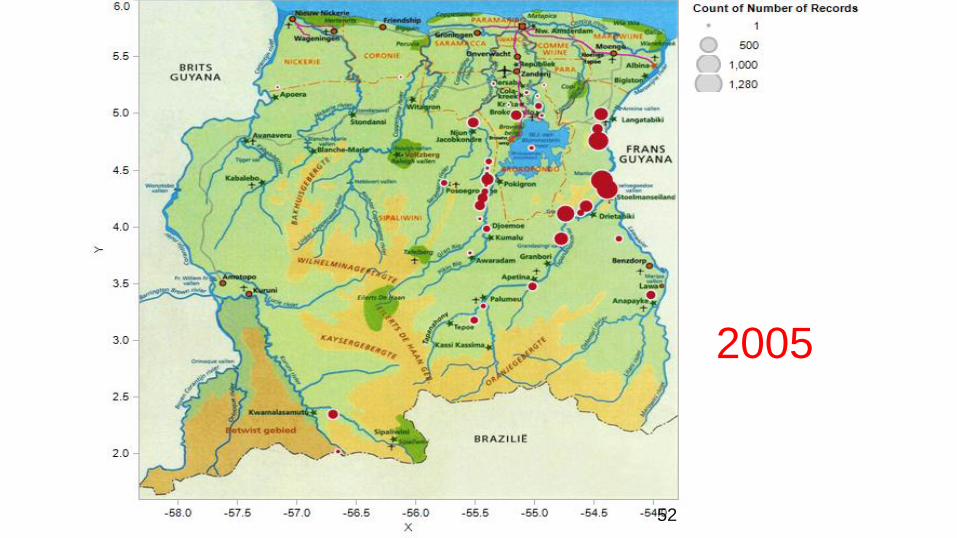
52icfi.com |
2005
52

53icfi.com |
2006
53

54icfi.com |
2007
5418th Meeting of the RBM Partnership
Monitoring and Evaluation Reference Group (MERG)

55icfi.com |
2010-2013
55

56icfi.com |
Measuring impact
0
100
200
300
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
API AFI AVI AFI AVI
API
0
10
20
30 SPR %
y = -1813x + 18347R² = 0.8807
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Malaria cases

57icfi.com |
0
2000
4000
6000
8000
10000
12000
14000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Pf/Mi…Pv
Cases by species
0
5000
10000
15000
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
PF/MIX
PV/PM
0
100
200
300
400
0.00
200.00
400.00
600.00
800.00
200020012002200320042005200620072008
Hospitalization
Deaths
Measuring impact

58icfi.com |
Changing scenarios
Malaria cases by age-groups
(%)
Malaria cases by sex (%)

59icfi.com |
Autochthonous vs. imported malaria
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Authocthonous Imported
2014
60icfi.com |
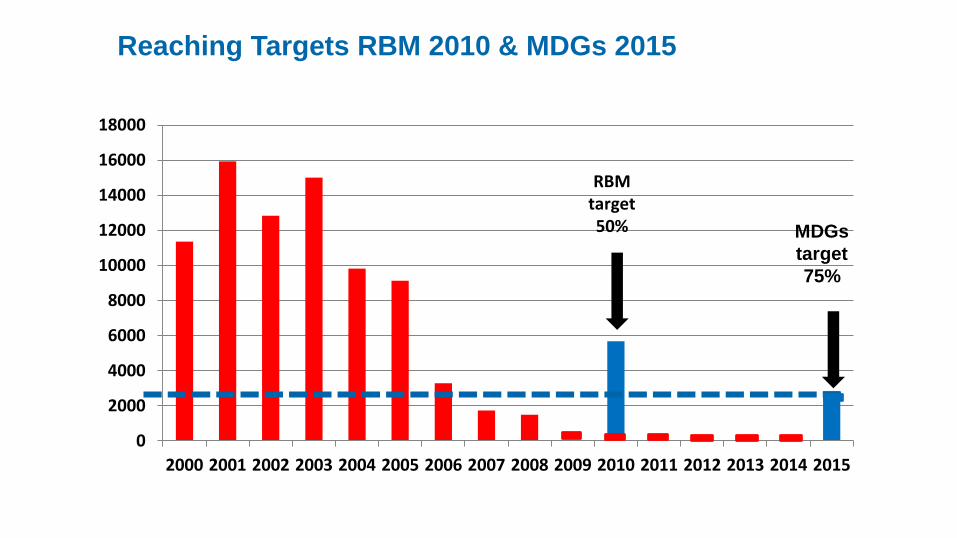
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
RBM target 50% MDGs
target
75%
Reaching Targets RBM 2010 & MDGs 2015

61icfi.com |
Cross border impactMalaria impact along the Suriname-French Guyana
border
• Cooperation between countries
• Financial and technical support
• Close collaboration with health authorities
• Malaria risk decreased along the border areas in both
countries
• Gold miners remains the challenge!
62icfi.com |
Malaria among gold miners

63icfi.com |
Road map for malaria elimination
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
MAL R4
MAL R7 Gold miners
Elimination Phase 1
CONSOLIDATION MAL ARIA EFFORTS
elimination – cross cutting research-leadership
2020
Phase 2
Suriname a malaria-free country by 2020

64icfi.com | 64
Malaria contextual factors & macro picture

65icfi.com |
Sub-Regional Picture

66icfi.com |

67icfi.com |
Similar mining
activities in the
Guyanan
Shield

68icfi.com |
http://en.wikipedia.org/wiki/Gold_reserve
World Gold reserves per capita

69icfi.com |www. maps.google.com/maps?hl=en&tab=wl
Epicenter multidrug resistance
Border areas in the Guyanan Shield: malaria transmission areas

Malaria Update

Control Pre-elimination EliminationPrevention of
reintroductionMalaria free
SPR<5% <1 case/1000 pop at risk 0 locally acquired cases 3 years
From Control to Elimination

Control Pre-elimination EliminationPrevention of
reintroductionMalaria free
National: DHS, MICS, MIS, RMIS
State: DHS, MICS, MIS, RMIS
District: RMIS
Facility/Sentinel: RMIS
Community/Individual: RMIS
No households surveys (2011-2013)
At least 1households surveys (2011-2013)
Measuring Malaria
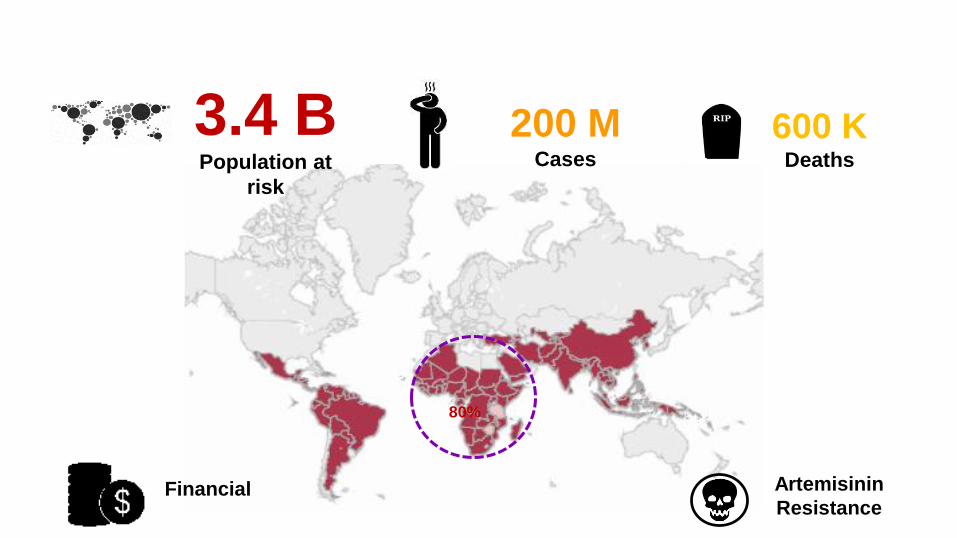
Artemisinin
Resistance
80%
3.4 BPopulation at
risk
200 MCases
600 KDeaths
Financial

>3.3 MDeaths prevented
50%# children dying
Cases
Deaths
Funding
2000 2012
Impact


NigeriaDR Congo
Madagascar
South East Asia – Mekong Subregion
Kenya

% Deaths <5 y #cases PW #cases >5 y
Democratic Republic of Congo

The Way forward

Big
Data
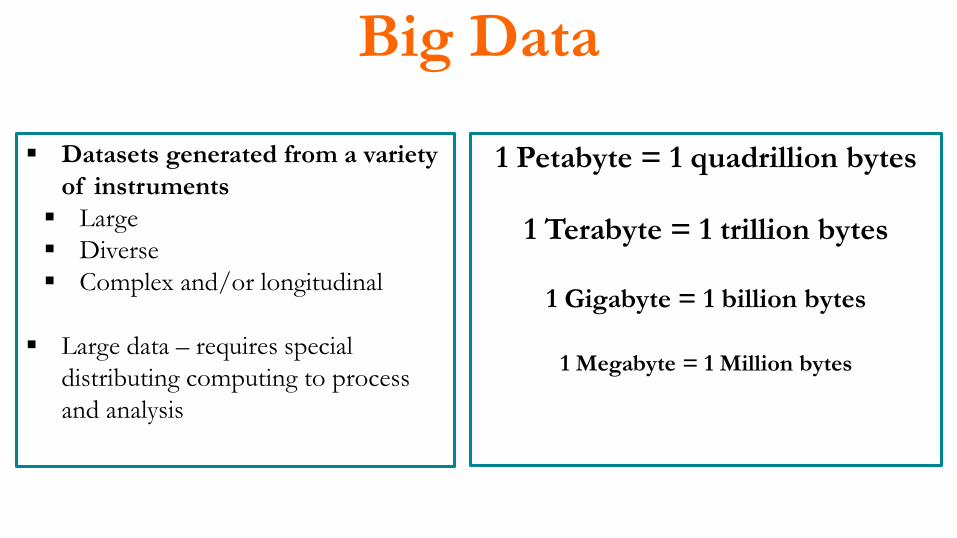
Big Data
Datasets generated from a variety
of instruments
Large
Diverse
Complex and/or longitudinal
Large data – requires special
distributing computing to process
and analysis
1 Petabyte = 1 quadrillion bytes
1 Terabyte = 1 trillion bytes
1 Gigabyte = 1 billion bytes
1 Megabyte = 1 Million bytes

Characteristics of Big Data
Volume Variety Velocity
Data at scale
TB to petabytes
Data in many forms
Text, structured, mixed
Data in motion
Analysis of streaming
data for decision
Veracity
Data uncertainty
Managing the reliability and predictability of imprecise data

Sources of Big Data
http://www.micscompiler.org/
http://www.childinfo.org/mics4_surveys.html
World Development Indicators

Sustainable Development
“Development that meets the needs of the present without
compromising the ability of future generations to meet their own
needs."
Rational use of natural resources and energy, pollution, and climate
change.
In development terms, sustainability means responsible growth—
when social and environmental concerns are aligned with people's economic needs.

EasyPol Issue 102, 2011
Sustainable Development
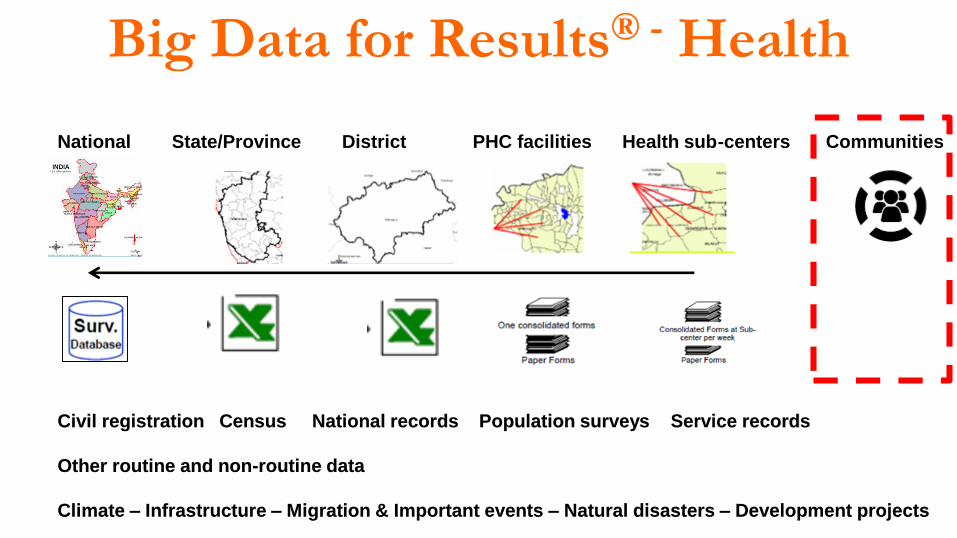
Big Data for Results® - Health
National State/Province District PHC facilities Health sub-centers Communities
Civil registration Census National records Population surveys Service records
Other routine and non-routine data
Climate – Infrastructure – Migration & Important events – Natural disasters – Development projects


Technical Review Panel
To support the Global Fund in financing effective programs, the Board relies
on an independent panel of international experts: the Technical Review
Panel (TRP).
• The TRP comprises the Chair, two Vice-Chairs and a pool of experts.
• The TRP consists of experts in HIV/AIDS, tuberculosis, malaria, health
systems, community systems and cross-cutting development issues.


Takeaways

“It’s being in the right place at the right
time and taking the advantage of your
opportunities”
Lee Majors

“Choose a job you love, and you will never
have to work a day in your life.”
Confucius

92
Leopoldo VillegasMD, DTM&H, MSc, DrPH, AdvDPHM
leopoldovillegas
@LeopoldVillega
www.linkedin.com/in/leopoldovillegas

Thank you!

Q&ACredits:Photos: several Google images (search Yanomami), Dr. Salvatore Ferraro, Dr. Leopoldo Villegas; LSHTM; SMRU; Wellcome
Trust; ICF international/MEASURE Evaluation; Global Fund; World Bank; CDC; DHS program; EasyPol Issue 102,
2011; PAHO/WHO; MOH (Venezuela, Suriname, Peru, Colombia, Ecuador, Bolivia); Google maps; Camara Andina de
Fomento; AMI/RAVREDA; bluestockingbrazil.
Infographics: Dr. Leopoldo Villegas
Icons: www.flaticom.com