Journal of Medical & Advanced Clinical Case Reports · 2020. 8. 13. · Journal of Medical &...
2
1 J Med Adv Clin Case Rep https://www.jmaccr.com 1 CASE REPORT A 57-year-old female presented with a facial rash and edema (Figure 1). The rash started on the cheeks and spread to her neck and upper chest over the course of three to four days. Her past medical history was significant for dry hands with scaling and cracking of the palms and fingers. She attributed the prob- lem to contact dermatitis from frequent hand washing and the use of surgical gloves (non-latex) from her work as a physical therapist. She was seen by her physician and prescribed Clo- betasol cream which she applied to her hands twice a day for the last two weeks. Her physical examination was remarkable for facial erythema, edema, and pustular lesions all at the same stage of development; some of the lesions had honey-crusted scaling. She returned to her physician and was diagnosed with steroid-induced acne and impetigo. She was advised to dis- continue the Clobetasol and was started on a seven-day course of clindamycin for the impetigo. 2 DISCUSSION Hand eczema is an inflammation of the skin of the hands that runs a chronic, relapsing course. It is often associated with itching, social stigma, and impairment in employment. Topical steroids are commonly used to alleviate symptoms. However, their beneficial effects must be balanced with their side effect profile which varies with the duration of treatment, the chem- ical nature and strength of the medication, the vehicle, and the location of its application. Topical steroids are broken into sev- en classes based on potency from Class I (very high potency) to class VII (low potency) (Table 1) [1]. A recent Cochrane meta-analysis on hand eczema assessed various corticosteroid creams/ointments 15 days after the start of treatment. Results showed that Clobetasol propion- ate 0.05% foam improved participant-rated control of symp- toms compared to vehicle (risk ratio (RR) 2.32, 95% confi- dence interval (CI) 1.38 to 3.91; number needed to treat for an additional beneficial outcome (NNTB) 3, 95% CI 2 to 8; 1 study, 125 participants). The effect of Clobetasol compared to vehicle for investigator-rated improvement was less clear (RR 1.43, 95% CI 0.86 to 2.40) [2]. On the other hand, the most fre- quent adverse effects of topical steroids include acne, atrophy, perioral dermatitis, purpura, rosacea, and striae. Those that occur with lower frequency include hypertrichosis, pigmen- tation alterations, delayed wound healing, and exacerbation of skin infections, both bacterial and fungal. Systemic reactions such as adrenal insufficiency, diabetes mellitus glaucoma, hip and vertebral fractures, hyperglycemia, and hypertension have also been reported with long-term topical use [3,4]. Acne is a known side effect of many medications, systemic and topical, including steroids. Drug-induced acne is defined as an erup- tion of inflammatory papules and papulopustules that occurs suddenly and often at an unusual age and can be associated with the initiation of a medication with this known side effect. Drug-related eruptions are characterized by rapid resolution after discontinuation of the medication [5]. Studies on steroid use for melasma also shed light on their adverse effects. A study of 60 patients with melasma who used a triple combination of 2% hydroquinone, 0.025% tretinoin, and 1% mometasone (mid-potency steroid) for at least three weeks found that 18% developed anceiform eruptions. Other cutaneous side effects included telangiectasia, skin atrophy, and hypertrichosis. However, none of the patients who had CASE REPORT Received: 13 July 2020 Accepted: 07 August 2020 Published: 16 August 2020 Steroid-Induced Acne from Topical Treatment of Contact Dermatitis Sarah Cavenaugh | Miriam Matthews | McGovern Medical School, United States Journal of Medical & Advanced Clinical Case Reports Correspondence Dr. Lynnette Mazur McGovern Medical School United States E-mail: [email protected] Tel: +1-713-500-5668 Figure 1: Facial acne from topical application of Clobetasol. Anita D'Souza | Lynnette Mazur*
Transcript of Journal of Medical & Advanced Clinical Case Reports · 2020. 8. 13. · Journal of Medical &...

1J Med Adv Clin Case Rephttps://www.jmaccr.com
1 CASE REPORT
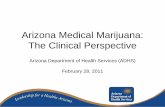
A 57-year-old female presented with a facial rash and edema (Figure 1). The rash started on the cheeks and spread to her neck and upper chest over the course of three to four days. Her past medical history was significant for dry hands with scaling and cracking of the palms and fingers. She attributed the prob-lem to contact dermatitis from frequent hand washing and the use of surgical gloves (non-latex) from her work as a physical therapist. She was seen by her physician and prescribed Clo-betasol cream which she applied to her hands twice a day for the last two weeks. Her physical examination was remarkable for facial erythema, edema, and pustular lesions all at the same stage of development; some of the lesions had honey-crusted scaling. She returned to her physician and was diagnosed with steroid-induced acne and impetigo. She was advised to dis-continue the Clobetasol and was started on a seven-day course of clindamycin for the impetigo.
2 DISCUSSION
Hand eczema is an inflammation of the skin of the hands that runs a chronic, relapsing course. It is often associated with itching, social stigma, and impairment in employment. Topical steroids are commonly used to alleviate symptoms. However, their beneficial effects must be balanced with their side effect profile which varies with the duration of treatment, the chem-ical nature and strength of the medication, the vehicle, and the location of its application. Topical steroids are broken into sev-en classes based on potency from Class I (very high potency) to class VII (low potency) (Table 1) [1].A recent Cochrane meta-analysis on hand eczema assessed various corticosteroid creams/ointments 15 days after the start of treatment. Results showed that Clobetasol propion-ate 0.05% foam improved participant-rated control of symp-toms compared to vehicle (risk ratio (RR) 2.32, 95% confi-dence interval (CI) 1.38 to 3.91; number needed to treat for an additional beneficial outcome (NNTB) 3, 95% CI 2 to 8; 1 study, 125 participants). The effect of Clobetasol compared to vehicle for investigator-rated improvement was less clear (RR 1.43, 95% CI 0.86 to 2.40) [2]. On the other hand, the most fre-quent adverse effects of topical steroids include acne, atrophy, perioral dermatitis, purpura, rosacea, and striae. Those that occur with lower frequency include hypertrichosis, pigmen-tation alterations, delayed wound healing, and exacerbation of skin infections, both bacterial and fungal. Systemic reactions such as adrenal insufficiency, diabetes mellitus glaucoma, hip and vertebral fractures, hyperglycemia, and hypertension have also been reported with long-term topical use [3,4]. Acne is a known side effect of many medications, systemic and topical, including steroids. Drug-induced acne is defined as an erup-tion of inflammatory papules and papulopustules that occurs suddenly and often at an unusual age and can be associated with the initiation of a medication with this known side effect. Drug-related eruptions are characterized by rapid resolution after discontinuation of the medication [5].Studies on steroid use for melasma also shed light on their adverse effects. A study of 60 patients with melasma who used a triple combination of 2% hydroquinone, 0.025% tretinoin, and 1% mometasone (mid-potency steroid) for at least three weeks found that 18% developed anceiform eruptions. Other cutaneous side effects included telangiectasia, skin atrophy, and hypertrichosis. However, none of the patients who had
CASE REPORT
Received: 13 July 2020 Accepted: 07 August 2020 Published: 16 August 2020
Steroid-Induced Acne from Topical Treatment of Contact Dermatitis
Sarah Cavenaugh | Miriam Matthews |
McGovern Medical School, United States
Journal of Medical & Advanced Clinical Case Reports
CorrespondenceDr. Lynnette MazurMcGovern Medical SchoolUnited StatesE-mail: [email protected]: +1-713-500-5668
Figure 1: Facial acne from topical application of Clobetasol.
Anita D'Souza | Lynnette Mazur*

2
J Med Adv Clin Case Rephttps://www.jmaccr.com
used the treatment for less than a month had an adverse effect on the face or skin [6]. Another study of 547 patients using topical steroids (89.6% using a Class I or very high potency steroid) as skin lightening agents for more than three weeks found 248 (45.3%) developed steroid-induced acne [4]. Other complications included widespread striae in 161 (28.3%), tel-angiectasia in 117 (21.3%), easy bruisability in 95 (17.4%), and hypertrichosis in 73 (13.3%). Very high potency steroids were significantly associated with the development of diabetes mellitus in 11 (2.1%) and obesity in nine (1.6%) patients. The majority of patients (81.3%) applied the products all over the body while 18.7% applied then directly to only the face [4].In conclusion, our patient’s acne and impetigo progressive-ly resolved over the course of two weeks after discontinuing the cream and completing the course of antibiotics. Like the above mentioned studies, patients who use high potency topic-al steroids are at risk of steroid-induced acne. It is important to warn patients of the potential side effects of topical steroid use and to discourage their prolonged use, and to consider lower potency agents when possible.
3 REFERENCES
1. Engorn B and Flerlage J (2015) The Harriet Lane Hand-book: A Manual for Pediatric House Officers. Philadelphia: Elsevier 0182-183.
2. Christoffers WA, Coenraads PJ, Svensson Å, Diepgen TL, Dickinson-Blok JL, et al. (2019) Interventions for hand ec-zema.Cochrane Database Syst Rev 4: CD004055.
3. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ (2006) Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol 54 :1-15.
4. Nnoruka E and Okoye O (2006) Topical Steroid Abuse: It’s Use as A Depigmenting Agent. J Nat Med Assoc 98: 934-939.
5. Kazandjieva J and Tsankov N (2017) Drug-induced acne. Clinical Dermatology 35: 156-162.
6. Majid I (2010) Mometasone-based Triple Combination Therapy in Melasma: Is It Really Safe? Indian J Dermatol 55 :359-362.
Potency Drugs
LowestDexamethasone Hydrocortisone Hydrocortisone acetate
LowAlclometasone Desonide Fluocinonide
Lower-MediumHydrocortisone butyrate Hydrocortisone probutate Hydrocortisone valerate Prednicarbate
Medium
Betamethosone valerate Clocortolone pivalate Desoximetsone Fluocinolone acetonide Fluradrenolide Fluticasone propionate (cream/ointment) Mometasone furoate Triamcinolone acetonide
High
Amcinonide Augmented betamethasone diproprionate (cream) Betamethosone proprionate Desoximetasone Diflorasone Fluocinonide Halocinonide Mometsone Triamcinolone acetonide
Very High
Augmented Betamethasone diproprionate (ointment) Clobetasol proprionate Diflorasone diacetate Halobetasol propionate
Table 1: Relative Potencies of Topical Corticosteroids.